
A Systematic Review of Compensation and Technology-Mediated Strategies to Maintain Older Adults’ Medication Adherence
 , ,
, ,
Abstract
:1. Introduction
- (1)
- What compensation strategies could the elderly utilize to maintain or improve their medication adherence?
- (2)
- What technology-mediated strategies could the elderly utilize to maintain or improve their medication adherence?
2. Methods
2.1. Search Strategy
2.2. Eligibility Criteria
2.3. Risk of Bias Assessment
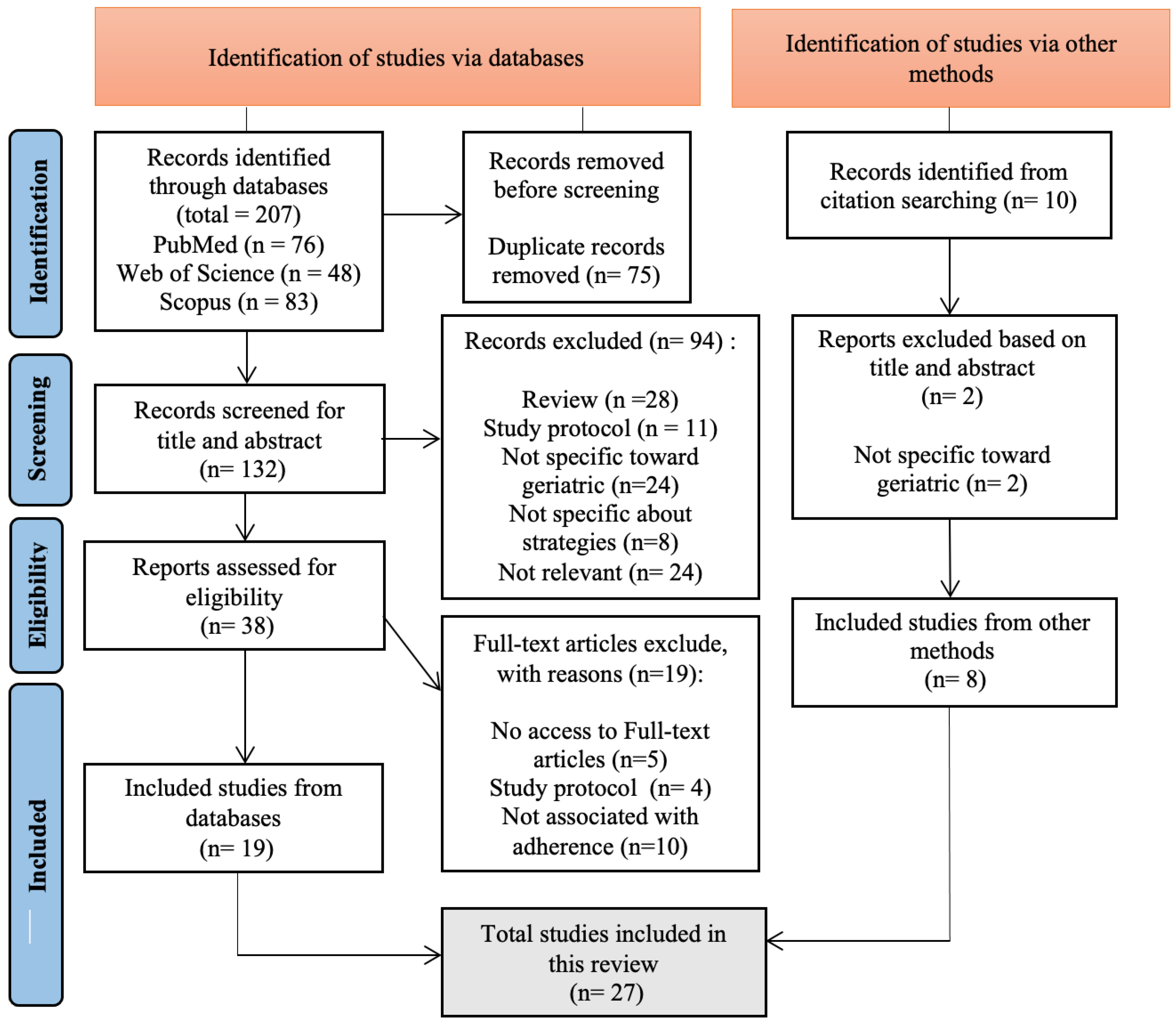
3. Results
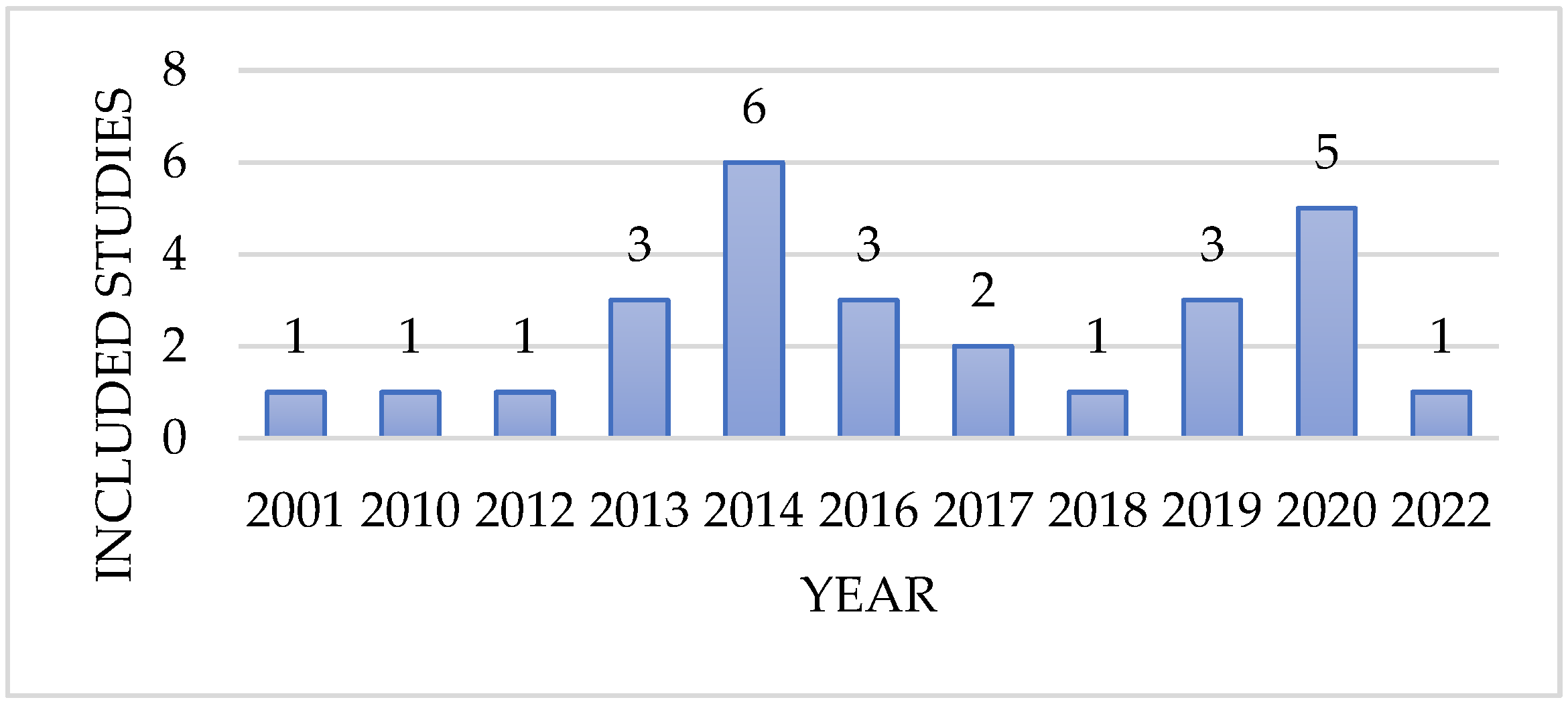
3.1. Characteristics of Included Studies
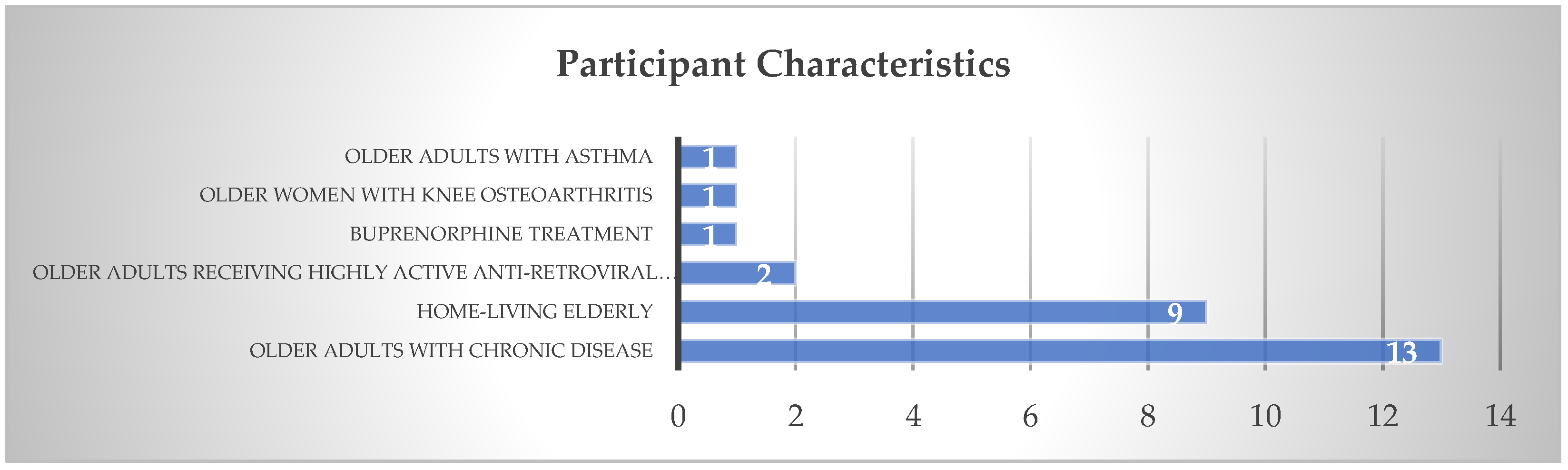
3.2. Participant Characteristics
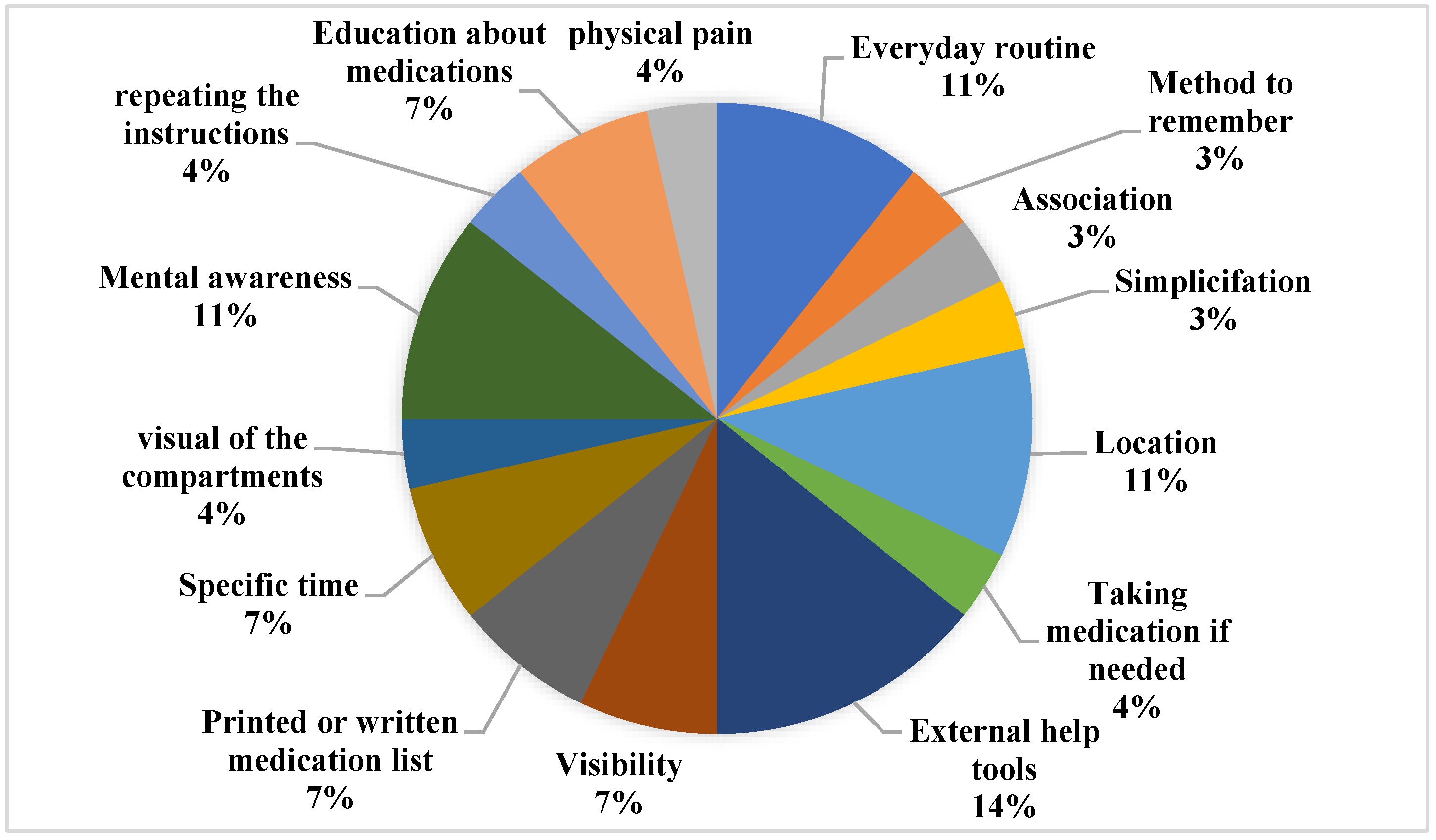
3.3. Types of Strategies
3.4. Outcome and Measurement
4. Discussion
4.1. Compensation Strategies
4.2. Technology-Based Strategies
4.2.1. Text Message Reminders
4.2.2. Electronic Pillbox
4.2.3. Smartphone Mobile Applications
4.2.4. Limitations of This Review
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Jimmy, B.; Jose, J. Patient Medication Adherence: Measures in Daily Practice. Oman Med. J. 2011, 26, 155–159. [Google Scholar] [CrossRef]
- Dobbels, F.; van Damme-Lombaert, R.; Vanhaecke, J.; de Geest, S. Growing pains: Non-adherence with the immunosuppressive regimen in adolescent transplant recipients. Pediatr. Transpl. 2005, 9, 381–390. Available online: https://pubmed.ncbi.nlm.nih.gov/15910397/ (accessed on 21 December 2022). [CrossRef] [PubMed]
- Turcu-Stiolica, A.; Taerel, A.E.; Turcu-Stiolica, R. Identifying and Measuring Compliance and Adherence in Antidepressants Taking. Procedia Econ. Financ. 2014, 15, 836–839. [Google Scholar] [CrossRef]
- Lehane, E.; McCarthy, G. Intentional and unintentional medication non-adherence: A comprehensive framework for clinical research and practice? A discussion paper. Int. J. Nurs. Stud. 2007, 44, 1468–1477. [Google Scholar] [CrossRef] [PubMed]
- Gellad, W.F.; Grenard, J.L.; Marcum, Z.A. A Systematic Review of Barriers to Medication Adherence in the Elderly: Looking Beyond Cost and Regimen Complexity. Am. J. Geriatr. Pharm. 2011, 9, 11–23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dagli, R.J.; Sharma, A. Polypharmacy: A Global Risk Factor for Elderly People. J. Int. Oral Health 2014, 6, i–ii. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4295469/ (accessed on 25 November 2021).
- Jin, H.K.; Kim, Y.H.; Rhie, S.J. Factors affecting medication adherence in elderly people. Patient Prefer. Adherence 2016, 10, 2117. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5077271/ (accessed on 7 October 2022). [CrossRef] [Green Version]
- Chisholm-Burns, M.A.; Spivey, C.A. The “cost” of medication nonadherence: Consequences we cannot afford to accept. J. Am. Pharm. Assoc. 2012, 52, 823–826. [Google Scholar] [CrossRef]
- Atreja, A.; Bellam, N.; Levy, S.R. Strategies to Enhance Patient Adherence: Making it Simple. Medscape Gen. Med. 2005, 7, 4. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1681370/ (accessed on 25 November 2021).
- Hughes, C.M. Medication non-adherence in the elderly: How big is the problem? Drugs Aging 2004, 21, 793–811. Available online: https://pubmed.ncbi.nlm.nih.gov/15382959/ (accessed on 19 December 2022). [CrossRef]
- Yap, A.F.; Thirumoorthy, T.; Kwan, Y.H. Medication adherence in the elderly. J. Clin. Gerontol. Geriatr. 2016, 7, 64–67. [Google Scholar] [CrossRef] [Green Version]
- Ozaki, A.F.; Choi, A.S.; Le, Q.T.; Ko, D.T.; Han, J.K.; Park, S.S.; Jackevicius, C.A. Real-World Adherence and Persistence to Direct Oral Anticoagulants in Patients with Atrial Fibrillation: A Systematic Review and Meta-Analysis. Circ. Cardiovasc. Qual. Outcomes 2020, 13, e005969. Available online: https://pubmed.ncbi.nlm.nih.gov/32148102/ (accessed on 19 December 2022). [CrossRef] [PubMed]
- Nieuwlaat, R.; Wilczynski, N.; Navarro, T.; Hobson, N.; Jeffery, R.; Keepanasseril, A.; Agoritsas, T.; Mistry, N.; Iorio, A.; Jack, S.; et al. Interventions for enhancing medication adherence. Cochrane Database Syst. Rev. 2014, 2014, CD000011. Available online: https://pubmed.ncbi.nlm.nih.gov/25412402/ (accessed on 25 November 2021). [CrossRef] [PubMed]
- Tomaszewski Farias, S.; Schmitter-Edgecombe, M.; Weakley, A.; Harvey, D.; Denny, K.G.; Barba, C.; Gravano, J.T.; Giovannetti, T.; Willis, S. Compensation Strategies in Older Adults: Association with Cognition and Everyday Function. Am. J. Alzheimer’s Dis. Other Dement. 2018, 33, 184–191. [Google Scholar] [CrossRef] [PubMed]
- Badawy, S.M.; Thompson, A.A.; Kuhns, L.M. Medication Adherence and Technology-Based Interventions for Adolescents with Chronic Health Conditions: A Few Key Considerations. JMIR mHealth uHealth 2017, 5, e202. Available online: https://pubmed.ncbi.nlm.nih.gov/29273573/ (accessed on 13 January 2022). [CrossRef] [Green Version]
- Thakkar, J.; Kurup, R.; Laba, T.L.; Santo, K.; Thiagalingam, A.; Rodgers, A.; Woodward, M.; Redfern, J.; Chow, C.K. Mobile Telephone Text Messaging for Medication Adherence in Chronic Disease: A Meta-analysis. JAMA Int. Med. 2016, 176, 340–349. Available online: https://pubmed.ncbi.nlm.nih.gov/26831740/ (accessed on 25 November 2021). [CrossRef] [Green Version]
- Boron, J.B.; Rogers, W.A.; Fisk, A.D. Everyday Memory Strategies for Medication Adherence. Geriatr. Nurs. 2013, 34, 395. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3788075/ (accessed on 25 November 2021). [CrossRef] [Green Version]
- Elizabeth, S.; Lisa Marie, B.; Linda, A.O. Optimizing Medication Adherence in Older Patients: A Systematic Review SHURP (Swiss Nursing Homes Human Resources Project) View project. J. Clin. Outcomes Manag. 2008, 15, 595–606. Available online: https://www.researchgate.net/publication/24410351 (accessed on 7 October 2022).
- Chun-Yun Kang, G. Technology-based interventions to improve adherence to antihypertensive medications—An evidence-based review. Digit. Health 2022, 8, 1–16. Available online: https://us.sagepub.com/en-us/nam/ (accessed on 23 December 2022). [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8005924/ (accessed on 15 November 2021). [CrossRef]
- Branin, J.J. The role of memory strategies in medication adherence among the elderly. Home Health Care Serv. Q. 2001, 20, 1–16. Available online: https://pubmed.ncbi.nlm.nih.gov/11987652/ (accessed on 15 October 2022). [CrossRef] [PubMed]
- Brooks, T.L.; Leventhal, H.; Wolf, M.S.; O’Conor, R.; Morillo, J.; Martynenko, M.; Wisnivesky, J.P.; Federman, A.D. Strategies used by older adults with asthma for adherence to inhaled corticosteroids. J. Gen. Intern. Med. 2014, 29, 1506–1512. Available online: https://pubmed.ncbi.nlm.nih.gov/25092003/ (accessed on 26 November 2021). [CrossRef] [PubMed] [Green Version]
- Goldstein, C.M.; Gathright, E.C.; Dolansky, M.A.; Gunstad, J.; Sterns, A.; Redle, J.D.; Josephson, R.; Hughes, J.W. Randomized controlled feasibility trial of two telemedicine medication reminder systems for older adults with heart failure. J. Telemed. Telecare 2014, 20, 293. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6957063/ (accessed on 25 November 2021). [CrossRef]
- Ligons, F.M.; Mello-Thoms, C.; Handler, S.M.; Romagnoli, K.M.; Hochheiser, H. Assessing the impact of cognitive impairment on the usability of an electronic medication delivery unit in an assisted living population. Int. J. Med. Inform. 2014, 83, 841–848. Available online: https://pubmed.ncbi.nlm.nih.gov/25153770/ (accessed on 15 October 2022). [CrossRef] [Green Version]
- Park, L.G.; Ng, F.K.; Shim, J.; Elnaggar, A.; Villero, O. Perceptions and experiences of using mobile technology for medication adherence among older adults with coronary heart disease: A qualitative study. Digit. Health 2020, 6, 2055207620926844. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7241207/ (accessed on 25 November 2021). [CrossRef]
- Swanlund, S.L. Successful cardiovascular medication management processes as perceived by community-dwelling adults over age 74. Appl. Nurs. Res. 2010, 23, 22–29. Available online: https://pubmed.ncbi.nlm.nih.gov/20122507/ (accessed on 15 October 2022). [CrossRef]
- Tofighi, B.; Grazioli, F.; Bereket, S.; Grossman, E.; Aphinyanaphongs, Y.; Lee, J.D. Text message reminders for improving patient appointment adherence in an office-based buprenorphine program: A feasibility study. Am. J. Addict. 2017, 26, 581–586. Available online: https://pubmed.ncbi.nlm.nih.gov/28799677/ (accessed on 15 October 2022). [CrossRef]
- Vollmer, W.M.; Owen-Smith, A.A.; Tom, J.O.; Laws, R.; Ditmer, D.G.; Smith, D.H.; Waterbury, A.C.; Schneider, J.L.; Yonehara, C.H.; Williams, A.; et al. Improving Adherence to Cardiovascular Disease Medications with Information Technology. Am. J. Manag. Care 2014, 20, SP502. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6358176/ (accessed on 15 October 2022).
- Pagan-Ortiz, M.E.; Goulet, P.; Kogelman, L.; Levkoff, S.E.; Weitzman, P.F. Feasibility of a Texting Intervention to Improve Medication Adherence Among Older HIV+ African Americans: A Mixed-Method Pilot Study. Gerontol. Geriatr. Med. 2019, 5, 233372141985566. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6598320/ (accessed on 23 December 2022). [CrossRef] [Green Version]
- Dasgupta, D.; Johnson, R.; Chaudry, B.; Reeves, K.; Willaert, P.; Chawla, N. Design and Evaluation of a Medication Adherence Application with Communication for Seniors in Independent Living Communities. In Amia Annual Symposium Proceedings; American Medical Informatics Association: Rockville, MD, USA, 2016; p. 480. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5333254/ (accessed on 23 December 2022).
- Grindrod, K.A.; Li, M.; Gates, A. Evaluating User Perceptions of Mobile Medication Management Applications with Older Adults: A Usability Study. JMIR mHealth uHealth 2014, 2, e11. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4114457/ (accessed on 23 December 2022). [CrossRef]
- Siu, H.Y.H.; Delleman, B.; Langevin, J.; Mangin, D.; Howard, M.; Fang, Q.; Price, D.; Chan, D. Demonstrating a Technology-Mediated Intervention to Support Medication Adherence in Community-Dwelling Older Adults in Primary Care: A Feasibility Study. Gerontol. Geriatr. Med. 2019, 5, 233372141984517. Available online: https://pubmed.ncbi.nlm.nih.gov/31106241/ (accessed on 26 January 2022). [CrossRef]
- Patel, T.; Ivo, J.; Faisal, S.; McDougall, A.; Carducci, J.; Pritchard, S.; Chang, F. A Prospective Study of Usability and Workload of Electronic Medication Adherence Products by Older Adults, Caregivers, and Health Care Providers. J. Med. Internet Res. 2020, 22, e18073. Available online: https://pubmed.ncbi.nlm.nih.gov/32348292/ (accessed on 23 December 2022). [CrossRef]
- Shen, Y.; Wang, T.; Gao, M.; Zhu, X.; Zhang, X.; He, C.; Li, Y.; Sun, X. Effectiveness of low-cost reminder package combined with case-based health education to improve hypertensive patients’ medication adherence: A clustered randomized controlled trial. Patient Prefer. Adherence 2019, 13, 1083–1092. Available online: https://pubmed.ncbi.nlm.nih.gov/31371926/ (accessed on 15 October 2022). [CrossRef] [Green Version]
- Mao, J.; Xie, L.; Zhao, Q.; Xiao, M.; Tu, S.; Sun, W.; Zhou, T. Demand analysis of an intelligent medication administration system for older adults with chronic diseases based on the Kano model. Int. J. Nurs. Sci. 2022, 9, 63–70. [Google Scholar] [CrossRef]
- Harbig, P.; Barat, I.; Damsgaard, E.M. Suitability of an electronic reminder device for measuring drug adherence in elderly patients with complex medication. J. Telemed. Telecare 2012, 18, 352–356. Available online: https://journals.sagepub.com/doi/10.1258/jtt.2012.120120?url_ver=Z39.88-2003&rfr_id=ori%3Arid%3Acros-ref.org&rfr_dat=cr_pub++0pubmed (accessed on 26 January 2022). [CrossRef]
- Kinyua, F.; Kiptoo, M.; Kikuvi, G.; Mutai, J.; Meyers, A.F.; Muiruri, P.; Songok, E. Perceptions of HIV infected patients on the use of cell phone as a tool to support their antiretroviral adherence; a cross-sectional study in a large referral hospital in Kenya. BMC Public Health 2013, 13, 987. Available online: https://pubmed.ncbi.nlm.nih.gov/24143931/ (accessed on 15 October 2022). [CrossRef] [Green Version]
- Wang, C.J.; Fetzer, S.J.; Yang, Y.C.; Wang, J.J. The impacts of using community health volunteers to coach medication safety behaviors among rural elders with chronic illnesses. Geriatr. Nurs. 2013, 34, 138–145. Available online: https://pubmed.ncbi.nlm.nih.gov/23414637/ (accessed on 15 October 2022). [CrossRef]
- Varleta, P.; Acevedo, M.; Akel, C.; Salinas, C.; Navarrete, C.; García, A.; Echegoyen, C.; Rodriguez, D.; Gramusset, L.; Leon, S.; et al. Mobile phone text messaging improves antihypertensive drug adherence in the community. J. Clin. Hypertens. 2017, 19, 1276–1284. Available online: https://pubmed.ncbi.nlm.nih.gov/28941056/ (accessed on 15 October 2022). [CrossRef] [Green Version]
- Adler, A.J.; Laar, A.; Prieto-Merino, D.; Der, R.M.; Mangortey, D.; Dirks, R.; Lamptey, P.; Perel, P. Can a nurse-led community-based model of hypertension care improve hypertension control in Ghana? Results from the ComHIP cohort study. BMJ Open 2019, 9, e026799. Available online: https://pubmed.ncbi.nlm.nih.gov/30944139/ (accessed on 15 October 2022). [CrossRef] [Green Version]
- Raj, J.P.; Mathews, B. Effect of behavioral intervention on medication adherence among elderly with select non-communicable diseases (ENDORSE): Pilot randomized controlled trial. Geriatr. Gerontol. Int. 2020, 20, 1079–1084. Available online: https://onlinelibrary.wiley.com/doi/full/10.1111/ggi.14032 (accessed on 15 October 2022). [CrossRef]
- Vieira, L.B.; Reis, A.M.M.; Ramos, C. de Á.; Reis TM dos, Cassiani SH de B. The use of an electronic medication organizer device with alarm to improve medication adherence of older adults with hypertension. Einstein 2021, 19, eAO6011. Available online: https://pubmed.ncbi.nlm.nih.gov/34586158/ (accessed on 15 October 2022). [CrossRef]
- Stawarz, K.; Rodríguez, M.D.; Cox, A.L.; Blandford, A. Understanding the use of contextual cues: Design implications for medication adherence technologies that support remembering. Digit. Health 2016, 2, 2055207616678707. Available online: http://www.ncbi.nlm.nih.gov/pubmed/29942574 (accessed on 26 January 2022). [CrossRef] [Green Version]
- Mira, J.J.; Navarro, I.; Botella, F.; Borrás, F.; Nuño-Solinís, R.; Orozco, D.; Iglesias-Alonso, F.; Pérez-Pérez, P.; Lorenzo, S.; Toro, N. A Spanish pillbox app for elderly patients taking multiple medications: Randomized controlled trial. J. Med. Internet Res. 2014, 16, e99. Available online: https://pubmed.ncbi.nlm.nih.gov/24705022/ (accessed on 23 December 2022). [CrossRef] [Green Version]
- Mertens, A.; Brandl, C.; Miron-Shatz, T.; Schlick, C.; Neumann, T.; Kribben, A.; Meister, S.; Diamantidis, C.J.; Albrecht, U.V.; Horn, P.; et al. A mobile application improves therapy-adherence rates in elderly patients undergoing rehabilitation: A crossover design study comparing documentation via iPad with paper-based control. Medicine 2016, 95, e4446. Available online: https://pubmed.ncbi.nlm.nih.gov/27603339/ (accessed on 23 December 2022). [CrossRef]
- Alasfour, M.; Almarwani, M. The effect of innovative smartphone application on adherence to a home-based exercise programs for female older adults with knee osteoarthritis in Saudi Arabia: A randomized controlled trial. Disabil. Rehabil. 2022, 44, 2420–2427. Available online: https://pubmed.ncbi.nlm.nih.gov/33103499/ (accessed on 23 December 2022). [CrossRef]
- Farias, S.T.; Schmitter-Edgecombe, M.; Weakley, A.; Harvey, D.; Denny, K.G.; Barba, C.; Gravano, J.T.; Giovannetti, T.; Willis, S. Compensation Strategies in Older Adults: Association with Cognition and Everyday Function. Curr. Top. Res. 2017, 33, 184–191. [Google Scholar]
- Furniss, D.; Barber, N.; Lyons, I.; Eliasson, L.; Blandford, A. Unintentional non-adherence: Can a spoon full of resilience help the medicine go down? BMJ Qual. Saf. 2014, 23, 95–98. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3913113/ (accessed on 10 February 2022). [CrossRef] [Green Version]
- O’Quin, K.E.; Semalulu, T.; Orom, H. Elder and caregiver solutions to improve medication adherence. Health Educ. Res. 2015, 30, 323–335. Available online: https://pubmed.ncbi.nlm.nih.gov/25725500/ (accessed on 10 February 2022). [CrossRef] [Green Version]
- Hall, A.K.; Cole-Lewis, H.; Bernhardt, J.M. Mobile Text Messaging for Health: A Systematic Review of Reviews. Annu. Rev. Public Health 2015, 36, 393. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4406229/ (accessed on 26 November 2021). [CrossRef] [Green Version]
- Schwebel, F.J.; Larimer, M.E. Using text message reminders in health care services: A narrative literature review. Internet Interv. 2018, 13, 82. Available online: https://pubmed.ncbi.nlm.nih.gov/30206523/ (accessed on 26 November 2021). [CrossRef]
- Chen, S.; Gong, E.; Kazi, D.S.; Gates, A.B.; Bai, R.; Fu, H.; Peng, W.; De La Cruz, G.; Chen, L.; Liu, X.; et al. Using Mobile Health Intervention to Improve Secondary Prevention of Coronary Heart Diseases in China: Mixed-Methods Feasibility Study. JMIR mHealth uHealth 2018, 6, e9. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5806005/ (accessed on 26 November 2021). [CrossRef]
- Maharani, L.; Pratiwi, H.; Mustikaningtias, I. The Impact of Short Message Service (SMS) Reminder and Home Monitoring on Blood Pressure Control in Hypertension Patients: A Case Study of Two Primary Health Care Facilities in Banyumas Regency. In Proceedings of the Muhammadiyah International Conference on Health and Pharmaceutical Development, Jakarta, Indonesia, 10–11 August 2018. [Google Scholar]
- Schwartz, J.K. Pillbox use, satisfaction, and effectiveness among persons with chronic health conditions. Assist. Technol. J. 2016, 29, 181–187. Available online: https://www.tandfonline.com/doi/abs/10.1080/10400435.2016.1219884 (accessed on 11 February 2022). [CrossRef] [PubMed]
- Billingsley, L.; Carruth, A. Use of Technology to Promote Effective Medication Adherence. J. Contin. Educ. Nurs. 2015, 46, 340–342. Available online: https://pubmed.ncbi.nlm.nih.gov/26247653/ (accessed on 25 November 2021). [CrossRef] [PubMed]
- Pérez-Jover, V.; Sala-González, M.; Guilabert, M.; Mira, J.J. Mobile Apps for Increasing Treatment Adherence: Systematic Review. J. Med. Internet Res. 2019, 21, e12505. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6604503/ (accessed on 10 February 2022). [CrossRef] [PubMed] [Green Version]
- Abdul Minaam, D.S.; Abd-ELfattah, M. Smart drugs:Improving healthcare using Smart Pill Box for Medicine Reminder and Monitoring System. Future Comput. Inform. J. 2018, 3, 443–456. [Google Scholar] [CrossRef]
- Hayes, T.L.; Hunt, J.M.; Adami, A.; Kaye, J.A. An Electronic Pillbox for Continuous Monitoring of Medication Adherence. Conf. Proc. IEEE Eng. Med. Biol. Soc. 2006, 1, 6400. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2911441/ (accessed on 26 November 2021).
- Hayakawa, M.; Uchimura, Y.; Omae, K.; Waki, K.; Fujita, H.; Ohe, K. A smartphone-based medication self-management system with realtime medication monitoring. Appl. Clin. Inf. 2013, 4, 37–52. Available online: https://pubmed.ncbi.nlm.nih.gov/23650486/ (accessed on 25 November 2021).






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Included | Excluded |
|---|---|
| Original article | Review articles |
| Full-text available | Commentary articles |
| Study design: Randomized control trial Cross-sectional, case–control, cohort Qualitative study Mixed-method | Handbooks or guidelines |
| Associated with older adults’ medication adherence | Study protocol |
| Focused on strategies (compensation or technology-mediated strategies) used by older adults to manage their medications. |
| Strategy | Branin et al. | Swanlund et al. | Harbig et al. | Boron et al. | Kinyua et al. | Wang et al. | Brooks et al. | Vollmer et al. | Goldstein et al. | Ligons et al. | Stawarz et al. | Varleta et al. | Tofighi et al. | Adler et al. |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Compensation | ||||||||||||||
| 1. Everyday routine | ✓ | ✓ | ✓ | |||||||||||
| 2. Method to remember | ✓ | |||||||||||||
| 3. Association | ✓ | |||||||||||||
| 4. Simplification | ✓ | |||||||||||||
| 5. Location | ✓ | ✓ | ✓ | |||||||||||
| 6. Taking medication if needed | ✓ | |||||||||||||
| 7. External help tools (i.e., pillbox, alarm clocks) | ✓ | ✓ | ✓ | ✓ | ||||||||||
| 8. Visibility | ✓ | ✓ | ||||||||||||
| 9. Printed or written medication list | ✓ | ✓ | ||||||||||||
| 10. Specific time of day | ✓ | ✓ | ||||||||||||
| 11. Visual of the compartments by color, shape, and size. | ✓ | |||||||||||||
| 12. Mental awareness | ✓ | ✓ | ✓ | |||||||||||
| 13. Repeating the instructions to oneself more than one time | ✓ | |||||||||||||
| 14. Education about medications | ✓ | |||||||||||||
| 15. Physical pain | ✓ | |||||||||||||
| Technology-mediated strategy | ||||||||||||||
| 1. Electronic reminder (i.e., device) | ✓ | ✓ | ||||||||||||
| 2. Electronic pillbox | ✓ | |||||||||||||
| 3. Application on smartphone/tablet | ✓ | |||||||||||||
| 4. Text-message reminder or phone call reminder | ✓ | ✓ | ✓ | ✓ | ||||||||||
| Other strategies | ||||||||||||||
| 1. Community-offered help | ✓ | ✓ | ||||||||||||
| Strategy | Shen et al. | Siu et al. | Park et al. | Raj et al. | Vieira et al. | Mao et al. | Mira et al. | Grindrod et al. | Mertens et al. | Dasgupta et al. | Pagan et al. | Patel et al. | Alasfour et al. | |
| Compensation | ||||||||||||||
| 1. Everyday routine | ||||||||||||||
| 2. Method to remember | ||||||||||||||
| 3. Association | ||||||||||||||
| 4. Simplification | ||||||||||||||
| 5. Location | ||||||||||||||
| 6. Taking medication if needed | ||||||||||||||
| 7. External help tools (i.e., pillbox, alarm clocks) | ||||||||||||||
| 8. Visibility | ||||||||||||||
| 9. Printed or written medication list | ||||||||||||||
| 10. Specific time of day | ||||||||||||||
| 11. Visual of the compartments by color, shape, and size. | ||||||||||||||
| 12. Mental awareness | ||||||||||||||
| 13. Repeating the instructions to oneself more than one time | ||||||||||||||
| 14. Education about medications | ✓ | |||||||||||||
| 15. Physical pain | ||||||||||||||
| Technology-mediated strategy | ||||||||||||||
| 1. Electronic reminder (i.e., device) | ✓ | ✓ | ✓ | ✓ | ||||||||||
| 2. Electronic pillbox | ✓ | ✓ | ||||||||||||
| 3. Application on smartphone/tablet | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ||||||||
| 4. Text-messages reminder or phone call reminder | ✓ | ✓ | ✓ | |||||||||||
| Other strategies | ||||||||||||||
| 1. Community-offered help | ||||||||||||||
| 2. Caregivers | ||||||||||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pratiwi, H.; Kristina, S.A.; Widayanti, A.W.; Prabandari, Y.S.; Kusuma, I.Y. A Systematic Review of Compensation and Technology-Mediated Strategies to Maintain Older Adults’ Medication Adherence. Int. J. Environ. Res. Public Health 2023, 20, 803. https://doi.org/10.3390/ijerph20010803
Pratiwi H, Kristina SA, Widayanti AW, Prabandari YS, Kusuma IY. A Systematic Review of Compensation and Technology-Mediated Strategies to Maintain Older Adults’ Medication Adherence. International Journal of Environmental Research and Public Health. 2023; 20(1):803. https://doi.org/10.3390/ijerph20010803
Chicago/Turabian StylePratiwi, Hening, Susi Ari Kristina, Anna Wahyuni Widayanti, Yayi Suryo Prabandari, and Ikhwan Yuda Kusuma. 2023. "A Systematic Review of Compensation and Technology-Mediated Strategies to Maintain Older Adults’ Medication Adherence" International Journal of Environmental Research and Public Health 20, no. 1: 803. https://doi.org/10.3390/ijerph20010803