
The Impact of Surgical Waiting Time on Oncological Outcomes in Patients with Upper Tract Urothelial Carcinoma Undergoing Radical Nephroureterectomy: A Systematic Review

 , ,
, ,  ,
,  , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Inclusion and Exclusion Criteria
- (P)opulation: Patients with UTUC who underwent RNU.
- (I)ntervention: Patients who underwent deferred RNU. Only studies reporting a specific cut-off defining the delay in RNU were included.
- (C)omparison: Patients who underwent RNU without delay.
- (O)utcome: The primary outcomes were cancer-specific survival (CSS) and overall survival (OS). The secondary outcome was recurrence-free survival (RFS).
2.3. Data Extraction
2.4. Quality Assessment and Risk of Bias
3. Results
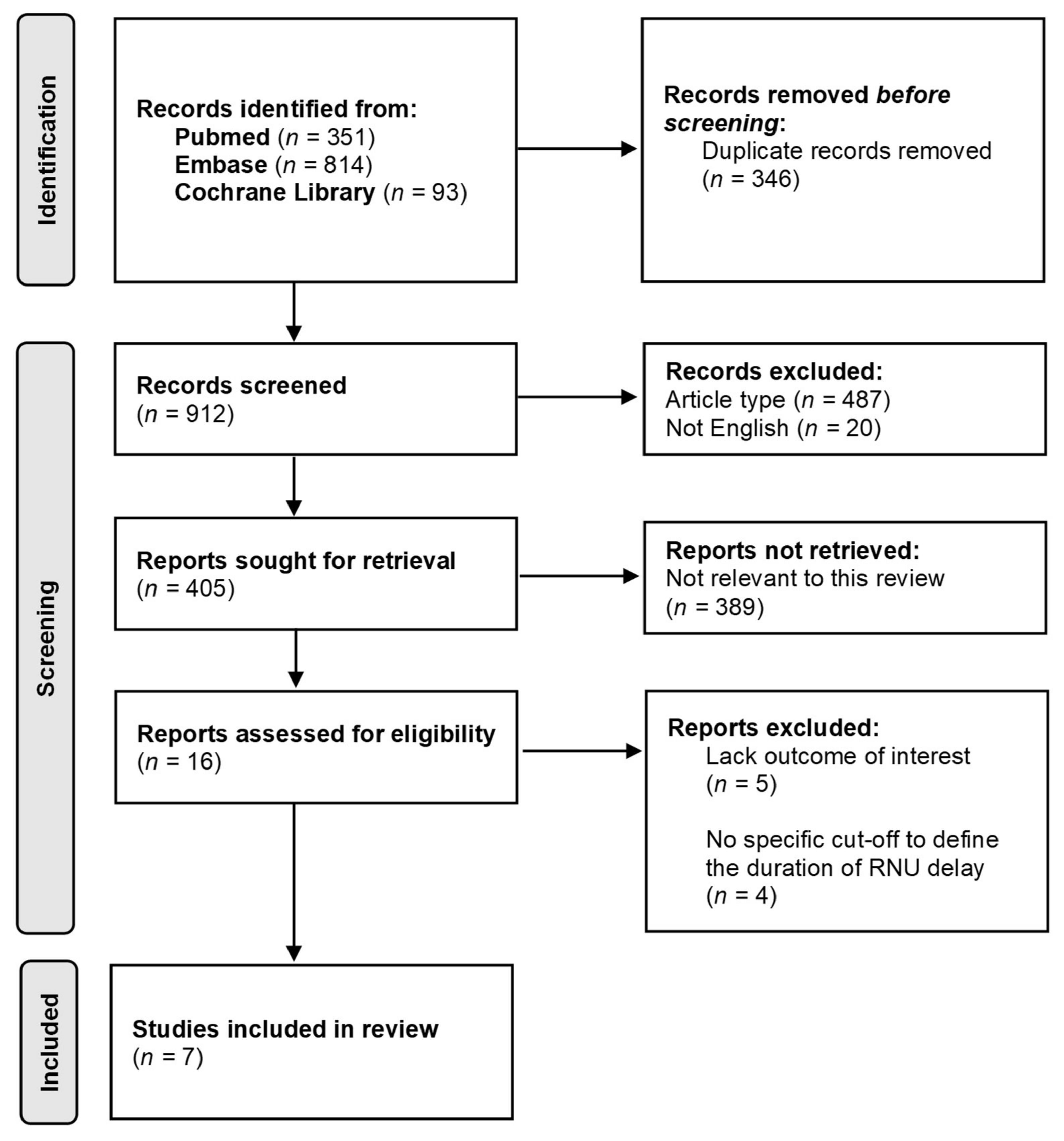
3.1. Literature Search Results
3.2. Features of Included Studies
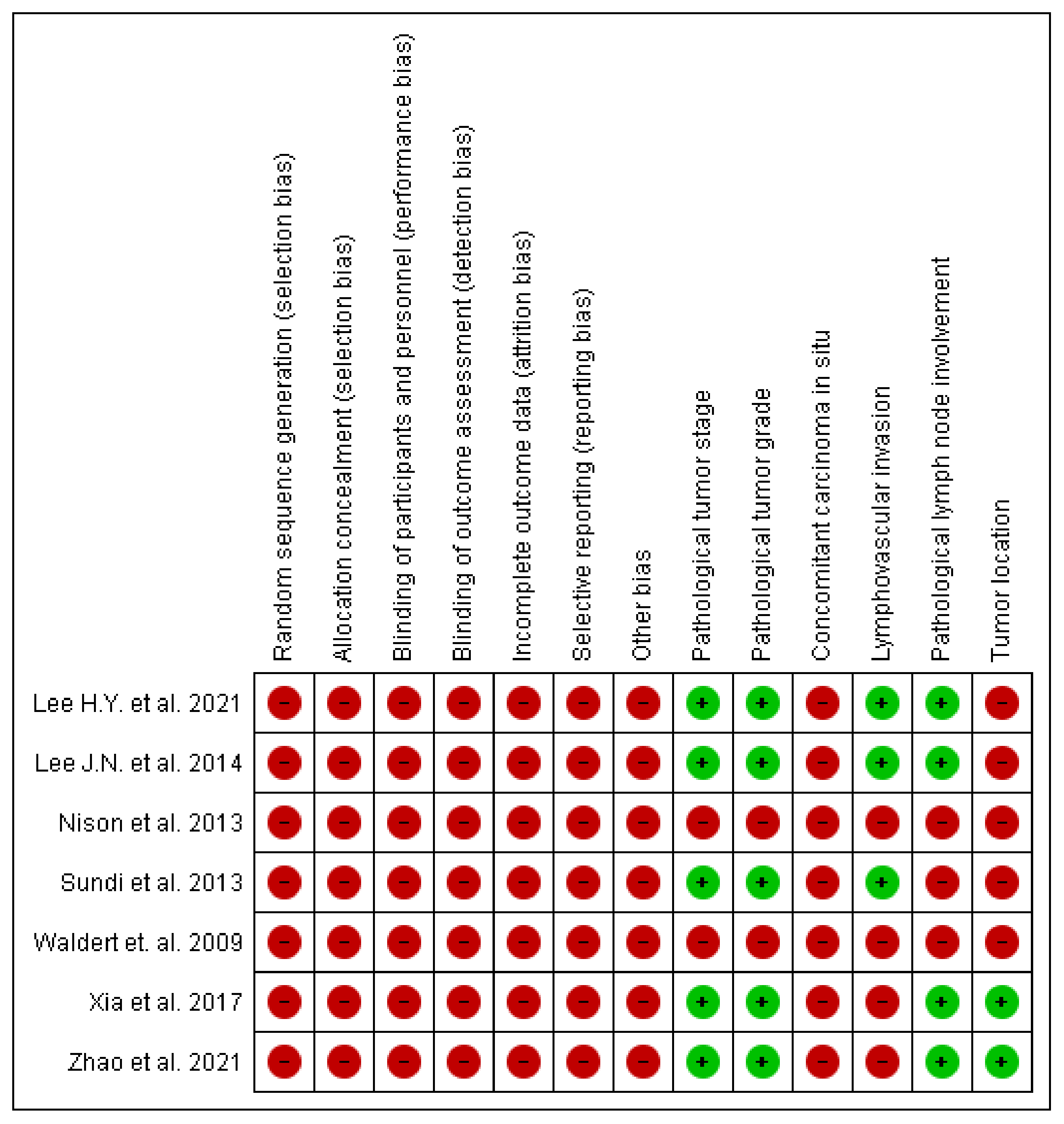
3.3. Risk of Bias (RoB) and Quality Assessment of Included Studies
3.4. Definition of Deferred Radical Nephroureterectomy
3.5. Results of Systematic Review (Qualitative Synthesis)
3.5.1. Cancer-Specific Survival (CSS)
3.5.2. Overall Survival (OS)
3.5.3. Recurrence-Free Survival (RFS)
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Fuchs, H.E.; Jemal, A. Cancer Statistics, 2021. CA Cancer J. Clin. 2021, 71, 7–33. [Google Scholar] [CrossRef] [PubMed]
- Rouprêt, M.; Babjuk, M.; Burger, M.; Capoun, O.; Cohen, D.; Compérat, E.M.; Cowan, N.C.; Dominguez-Escrig, J.L.; Gontero, P.; Hugh Mostafid, A.; et al. European Association of Urology Guidelines on Upper Urinary Tract Urothelial Carcinoma: 2020 Update. Eur. Urol. 2021, 79, 62–79. [Google Scholar] [CrossRef] [PubMed]
- Ribal, M.J.; Cornford, P.; Briganti, A.; Knoll, T.; Gravas, S.; Babjuk, M.; Harding, C.; Breda, A.; Bex, A.; Rassweiler, J.J.; et al. European Association of Urology Guidelines Office Rapid Reaction Group: An Organisation-wide Collaborative Effort to Adapt the European Association of Urology Guidelines Recommendations to the Coronavirus Disease 2019 Era. Eur. Urol. 2020, 78, 21–28. [Google Scholar] [CrossRef] [PubMed]
- Stensland, K.D.; Morgan, T.M.; Moinzadeh, A.; Lee, C.T.; Briganti, A.; Catto, J.W.F.; Canes, D. Considerations in the Triage of Urologic Surgeries During the COVID-19 Pandemic. Eur. Urol. 2020, 77, 663–666. [Google Scholar] [CrossRef] [PubMed]
- Guerrieri, R.; Rovati, L.; Dell’Oglio, P.; Galfano, A.; Ragazzoni, L.; Aseni, P. Impact of the COVID-19 Pandemic on Urologic Oncology Surgery: Implications for Moving Forward. J. Clin. Med. 2021, 11, 171. [Google Scholar] [CrossRef]
- Soualhi, A.; Rammant, E.; George, G.; Russell, B.; Enting, D.; Nair, R.; Van Hemelrijck, M.; Bosco, C. The incidence and prevalence of upper tract urothelial carcinoma: A systematic review. BMC Urol. 2021, 21, 110. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions Version 6.1 (Updated September 2020); John Wiley & Sons: Chichester, UK, 2020; Available online: www.training.cochrane.org/handbook (accessed on 15 April 2022).
- Lee, H.Y.; Chan, E.O.; Li, C.C.; Leung, D.; Li, W.M.; Yeh, H.C.; Chiu, P.K.; Ke, H.L.; Yee, C.H.; Wong, J.H.; et al. How to manage patients with suspected upper tract urothelial carcinoma in the pandemic of COVID-19? Urol. Oncol. 2021, 39, 733.e11–733.e16. [Google Scholar] [CrossRef]
- Lee, J.N.; Kwon, S.Y.; Choi, G.S.; Kim, H.T.; Kim, T.H.; Kwon, T.G.; Kim, B.W. Impact of surgical wait time on oncologic outcomes in upper urinary tract urothelial carcinoma. J. Surg. Oncol. 2014, 110, 468–475. [Google Scholar] [CrossRef]
- Nison, L.; Rouprêt, M.; Bozzini, G.; Ouzzane, A.; Audenet, F.; Pignot, G.; Ruffion, A.; Cornu, J.N.; Hurel, S.; Valeri, A.; et al. The oncologic impact of a delay between diagnosis and radical nephroureterectomy due to diagnostic ureteroscopy in upper urinary tract urothelial carcinomas: Results from a large collaborative database. World J. Urol. 2013, 31, 69–76. [Google Scholar] [CrossRef]
- Sundi, D.; Svatek, R.S.; Margulis, V.; Wood, C.G.; Matin, S.F.; Dinney, C.P.; Kamat, A.M. Upper tract urothelial carcinoma: Impact of time to surgery. Urol. Oncol. 2012, 30, 266–272. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Waldert, M.; Karakiewicz, P.I.; Raman, J.D.; Remzi, M.; Isbarn, H.; Lotan, Y.; Capitanio, U.; Bensalah, K.; Marberger, M.J.; Shariat, S.F. A delay in radical nephroureterectomy can lead to upstaging. BJU Int. 2010, 105, 812–817. [Google Scholar] [CrossRef] [PubMed]
- Xia, L.; Taylor, B.L.; Pulido, J.E.; Guzzo, T.J. Impact of surgical waiting time on survival in patients with upper tract urothelial carcinoma: A national cancer database study. Urol. Oncol. 2018, 36, 10.e15–10.e22. [Google Scholar] [CrossRef] [PubMed]
- Zhao, F.; Qi, N.; Zhang, C.; Xue, N.; Li, S.; Zhou, R.; Chen, Z.; Yao, R.; Zhu, H. Impact of Surgical Wait Time on Survival in Patients With Upper Urinary Tract Urothelial Carcinoma With Hydronephrosis. Front. Oncol. 2021, 11, 698594. [Google Scholar] [CrossRef] [PubMed]
- Nowak, Ł.; Krajewski, W.; Chorbińska, J.; Kiełb, P.; Sut, M.; Moschini, M.; Teoh, J.Y.; Mori, K.; Del Giudice, F.; Laukhtina, E.; et al. The Impact of Diagnostic Ureteroscopy Prior to Radical Nephroureterectomy on Oncological Outcomes in Patients with Upper Tract Urothelial Carcinoma: A Comprehensive Systematic Review and Meta-Analysis. J. Clin. Med. 2021, 10, 4197. [Google Scholar] [CrossRef]
- Gadzinski, A.J.; Roberts, W.W.; Faerber, G.J.; Wolf, J.S., Jr. Long-term outcomes of immediate versus delayed nephroureterectomy for upper tract urothelial carcinoma. J. Endourol. 2012, 26, 566–573. [Google Scholar] [CrossRef] [Green Version]
- Gurbuz, C.; Youssef, R.F.; Shariat, S.F.; Lotan, Y.; Wood, C.G.; Sagalowsky, A.I.; Zigeuner, R.; Kikuchi, E.; Weizer, A.; Raman, J.D.; et al. The impact of previous ureteroscopic tumor ablation on oncologic outcomes after radical nephrouretectomy for upper urinary tract urothelial carcinoma. J. Endourol. 2011, 25, 775–779. [Google Scholar] [CrossRef] [Green Version]
- Krajewski, W.; Nowak, Ł.; Małkiewicz, B.; Chorbińska, J.; Kiełb, P.; Poterek, A.; Sporniak, B.; Sut, M.; Moschini, M.; Lonati, C.; et al. The Impact of Primary Tumor Location on Long-Term Oncological Outcomes in Patients with Upper Tract Urothelial Carcinoma Treated with Radical Nephroureterectomy: A Systematic Review and Meta-Analysis. J. Pers. Med. 2021, 11, 1363. [Google Scholar] [CrossRef]
- Leow, J.J.; Chong, Y.L.; Chang, S.L.; Valderrama, B.P.; Powles, T.; Bellmunt, J. Neoadjuvant and Adjuvant Chemotherapy for Upper Tract Urothelial Carcinoma: A 2020 Systematic Review and Meta-analysis, and Future Perspectives on Systemic Therapy. Eur. Urol. 2021, 79, 635–654. [Google Scholar] [CrossRef]
- Kim, D.K.; Cho, K.S. Neoadjuvant chemotherapy for upper tract urothelial carcinoma. Transl. Cancer Res. 2020, 9, 6576–6582. [Google Scholar] [CrossRef]
- Seklehner, S.; Hladschik-Kermer, B.; Lusuardi, L.; Schabauer, C.; Riedl, C.; Engelhardt, P.F. Psychological stress assessment of patients suffering from prostate cancer. Scand. J. Urol. 2013, 47, 101–107. [Google Scholar] [CrossRef] [PubMed]
- Bourgade, V.; Drouin, S.J.; Yates, D.R.; Parra, J.; Bitker, M.O.; Cussenot, O.; Rouprêt, M. Impact of the length of time between diagnosis and surgical removal of urologic neoplasms on survival. World J. Urol 2014, 32, 475–479. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| First Author, Year [Reference] | Journal | Geographical Region | Study Type | Study Duration | Number of Patients | Definition of RNU Delay | Median Time to RNU, Days | Follow up, Months | Reported Outcomes |
|---|---|---|---|---|---|---|---|---|---|
| Lee H.Y. et al., 2021 [9] | Urologic Oncology: Seminars and Original Investigations | Asia | Retrospective Multi-center | 2000–2019 | 665 | Group 1: ≤90 days Group 2: >90 days | NR | Group 1: mean 52.3 Group 2: mean 34.2 | OS |
| Lee J.N. et al., 2014 [10] | Journal of Surgical Oncology | Asia | Retrospective Single-center | 2001–2010 | 138 | Group 1: ≤30 days Group 2: >30 days | Mean: 16.6 Mean: 70.1 | All patients: median 40 | CSS, RFS |
| Nison et al., 2013 [11] | World Journal of Urology | Europe | Retrospective Multi-center | 1995–2011 | 512 | Group 1: ≤30 days Group 2: 31–60 days Group 3: 61–90 days Group 4: >90 days | NR | All patients: median 23.6 | CSS, RFS |
| Sundi et al., 2013 [12] | Urological Oncology | North America | Retrospective Single-center | 1990–2007 | 240 | Group 1: ≤90 days Group 2: >90 days | Mean: 24 Mean: 432 | All patients: median 29 | CSS, OS |
| Waldert et al., 2009 [13] | BJU International | Multinational | Retrospective Multi-center | 2000–2007 | 187 | Group 1: ≤90 days Group 2: >90 days | Median: 33 Median: 110 | All patients: median 47.5 | CSS, RFS |
| Xia et al., 2017 [14] | Urologic Oncology: Seminars and Original Investigations | North America | Retrospective Population-based registry | 2004–2013 | 3581 | Group 1: 8–30 days Group 2: 1–7 days Group 3: 31–60 days Group 4: 61–90 days Group 5: 91–120 days Group 6: 121–180 days | NR | All patients: median 40.4 | OS |
| Zhao et al., 2021 [15] | Frontiers in Oncology | Asia | Retrospective Single-center | 2008–2019 | 316 | Group 1: ≤30 days Group 2: 31–90 days Group 3: >90 days | Median: 12 Median: 42 Median 191 | All patients: median 43 | OS, CSS |
| First Author, Year [Reference] | Gender, n (%) | Preoperative Hydronephrosis, n (%) | URS, n (%) | Tumor Location, n (%) | RNU Approach, n (%) | Pathological Tumor stage, n (%) | Pathological Tumor grade, n (%) | LNI, n (%) | Concomitant CIS, n (%) | LVI, n (%) | AC, n (%) |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Lee H.Y. et al., 2021 [9] | Male: 297 (49.5) Female: 303 (50.5) | NR | Yes: 491 (74.0) No: 174 (26.0) | NR | NR | <T2: 198 (33.0) ≥T2: 361 (67.0) | G1: 77 (14.8) G2: 62 (11.9) G3: 381 (73.3) | Yes: 44 (7.3) No a: 556 (92.7) | Yes: 20 (3.3) No: 580 (96.7) | Yes: 133 (22.2) No: 467 (77.8) | Yes: 89 (14.8) No: 511 (85.2) |
| Lee J.N. et al., 2014 [10] | Male: 96 (69.6) Female: 42 (30.4) | Yes: 100 (72.5) No: 38 (27.5) | NR | RPT: 58 (42.0) UT: 80 (58.0) | Open: 36 (26.1) Laparoscopic: 102 (73.9) | <T2: 50 (36.2) ≥T2: 88 (63.8) | LG: 46 (33.3) HG: 92 (66.7) | Yes: 10 (7.2) No a: 128 (92.8) | Yes: 7 (5.1) No: 131 (94.9) | Yes: 27 (19.6) No: 111 (80.4) | Yes: 43 (31.2) No: 95 (68.8) |
| Nison et al., 2013 [11] | Male: 348 (68.0) Female: 164 (32.0) | NR | Yes: 170 (33.2) No: 342 (66.8) | RPT: 277 (54.1) UT: 172 (33.6) Multifocal: 63 (12.3) | NR | <T2: 252 (49.2) ≥T2: 260 (50.8) | G1: 62 (12.1) G2: 154 (30.1) G3: 296 (57.8) | Yes: 39 (7.6) No a: 473 (92.4) | NR | Yes: 126 (24.6) No: 368 (75.4) | NR |
| Sundi et al., 2013 [12] | Male: 157 (65.4) Female: 83 (34.6) | NR | NR | RPT: 140 (58.3) UT: 100 (41.7) | NR | <T2: 120 (50.0) ≥T2: 120 (50.0) | LG: 51 (21.2) HG: 189 (78.8) | Yes: 30 (12.5) No a: 210 (87.5) | Yes: 101 (42.1) No: 139 (57.9) | Yes: 74 (30.8) No: 166 (69.2) | Yes: 38 (15.8) No: 202 (84.2) |
| Waldert et al., 2009 [13] | Male: 150 (80.2) Female: 37 (19.8) | NR | Yes: 49 (26.2) No: 138 (73.8) | RPT: 88 (47.1) UT: 99 (52.9) | Open: 151 (80.7) Laparoscopic: 36 (19.3) | <T2: 97 (51.9) ≥T2: 90 (48.1) | LG: 62 (33.2) HG: 125 (66.8) | Yes: 17 (9.1) No a: 170 (90.9) | Yes: 78 (41.7) No: 109 (58.3) | Yes: 54 (28.9) No: 133 (71.1) | Yes: 30 (16.0) No: 157 (84.0) |
| Xia et al., 2017 [14] | Male: 2038 (56.9) Female: 1543 (43.1) | NR | NR | RPT: 2428 (67.8) UT: 1153 (32.2) | NR | <T2: 1865 (52.1) ≥T2: 1429 (41.7) | G1-2: 1273 (35.6) G3-4: 2308 (64.4) | Yes: 147 (4.1) No a: 3434 (95.9) | NR | NR | Yes: 357 (10.0) No: 3224 (90.0) |
| Zhao et al., 2021 [15] | Male: 205 (64.9) Female: 111 (35.1) | Yes: 158 (50.0) No: 158 (50.0) | NR | RPT: 173 (54.7) UT: 143 (45.3) | Open: 67 (21.2) Laparoscopic: 249 (78.8) | <T2: 87 (27.5) ≥T2: 229 (72.5) | LG: 81 (25.6) HG: 234 (74.4) | Yes: 34 (10.8) No a: 282 (89.2) | NR | Yes: 38 (12.0) No: 278 (88.0) | Yes: 32 (10.1) No: 284 (89.9) |
| First Author, Year [Reference] | Subgroup | 5-Year CSS | p-Value | 5-Year OS | p-Value | Multivariable Cox Regression Analysis—CSS HR [95% CI] | p-Value | Multivariable Cox Regression Analysis—OS HR [95% CI] | p-Value |
|---|---|---|---|---|---|---|---|---|---|
| Lee H.Y. et al., 2021 [9] | NA | NR | NR | Delay ≤ 90 days: 72.9% Delay > 90 days: 63.5% | 0.015 * | NR | NR | Delay ≤ 90 days: Ref Delay > 90 days: 1.55 [1.03–2.33] | 0.035 * |
| Lee J.N. et al., 2014 [10] | All patients | Delay ≤ 30 days: 77.3% Delay > 30 days: 69.1% | 0.087 | NR | NR | NR | Univariable 0.089 | NR | NR |
| Renal pelvis tumors | Delay ≤ 30 days: 63.9% Delay > 30 days: 90.1% | 0.084 | NR | NR | NR | Univariable 0.085 | NR | NR | |
| Ureteral tumors | Delay ≤ 30 days: 87.9% Delay > 30 days: 54.5% | <0.001 * | NR | NR | Delay ≤ 30 days: ref Delay > 30 days: 6.26 [1.90–20.62] | 0.003 * | NR | NR | |
| Nison et al., 2013 [11] | NA | NR | NR | NR | NR | Univariable Delay ≤ 30 days: ref Delay 31–60 days: 1.00 [0.50–1.98] Delay 61–90 days: 0.84 [0.37–1.91] Delay > 90 days: 0.92 [0.45–1.89] | - 0.99 0.68 0.68 | NR | NR |
| Sundi et al., 2013 [12] | All patients | Delay ≤ 90 days: 71.6% Delay > 90 days: 70.6% | NS | Delay ≤ 90 days: 61.3% Delay > 90 days: 77.0% | NS | NR | NR | Delay ≤ 90 days: ref Delay > 90 days: 1.54 [0.73–3.25] | 0.25 |
| Patients not receiving NAC | Delay ≤ 90 days: 71.6% Delay > 90 days: 81.5% | NS | Delay ≤ 90 days: 61.3% Delay > 90 days: 77% | NS | NR | NR | Delay ≤ 90 days: ref Delay > 90 days: 0.94 [0.28–3.08] | 0.92 | |
| Waldert et al., 2009 [13] | All patients | Delay ≤ 90 days: 72% Delay > 90 days: 63% | NS | NR | NR | Univariable Time as continuous variable: 1.00 [0.99–1.01] | 0.658 | NR | NR |
| ≥pT2 on RNU | Delay ≤ 90 days: 49% Delay > 90 days: 45% | NS | NR | NR | Time as continuous variable: 1.005 [1.001–1.010] | 0.03 | NR | NR | |
| Xia et al., 2017 [14] | All patients | NR | NR | Delay 8–30 days: 64.2% Delay 1–7 days: 58.5% Delay 31–60 days: 61.8% Delay 61–90 days: 60.6% Delay 91–120 days: 61.5% Delay 121–180 days: 36.6% | * | NR | NR | Delay 8–30 days: ref Delay 1–7 days: 1.32 [1.06–1.67] Delay 31–60 days: 1.11 [0.97–1.27] Delay 61–90 days: 1.09 [0.91–1.30] Delay 91–120 days: 1.00 [0.74–1.35] Delay 121–180 days: 1.61 [1.19–2.19] | - 0.016 * 0.126 0.360 0.976 0.002 * |
| ≥pT2 and/or ≥G3 on RNU | NR | NR | Delay 8–30 days: 57.2% Delay 1–7 days: 55.8% Delay 31–60 days: 53.5% Delay 61–90 days: 51.6% Delay 91–120 days: 51.6% Delay 121–180 days: 26.5% | * | NR | NR | Delay 8–30 days: ref Delay 1–7 days: 1.24 [0.95–1.61] Delay 31–60 days: 1.10 [0.94–1.27] Delay 61–90 days: 1.07 [0.88–1.31] Delay 91–120 days: 0.94 [0.66–1.34] Delay 121–180 days: 1.56 [1.11–2.20] | - 0.114 0.231 0.510 0.744 0.010 * | |
| Zhao et al., 2021 [15] | All patients | Delay ≤ 30 days: 65.8% Delay 31–90 days: 70.9% Delay > 90 days: 39.6% | 0.032 * | Delay ≤ 30 days: 56.4% Delay 31–90 days: 59.3% Delay > 90 days: 35.1% | 0.045 * | NR | NR | NR | NR |
| Patients with hydronephrosis | Delay ≤ 60 days: 61.7% Delay > 60 days: 49.1% | 0.041 * | Delay ≤ 60 days: 55.1% Delay > 60 days: 44.2% | 0.023 * | Delay ≤ 60 days: ref Delay > 60 days: 1.74 [1.07–2.82] | 0.026 * | Delay ≤ 60 days: ref Delay > 60 days: 2.05 [1.20–3.50] | 0.009 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nowak, Ł.; Krajewski, W.; Łaszkiewicz, J.; Małkiewicz, B.; Chorbińska, J.; Del Giudice, F.; Mori, K.; Moschini, M.; Kaliszewski, K.; Rajwa, P.; et al. The Impact of Surgical Waiting Time on Oncological Outcomes in Patients with Upper Tract Urothelial Carcinoma Undergoing Radical Nephroureterectomy: A Systematic Review. J. Clin. Med. 2022, 11, 4007. https://doi.org/10.3390/jcm11144007
Nowak Ł, Krajewski W, Łaszkiewicz J, Małkiewicz B, Chorbińska J, Del Giudice F, Mori K, Moschini M, Kaliszewski K, Rajwa P, et al. The Impact of Surgical Waiting Time on Oncological Outcomes in Patients with Upper Tract Urothelial Carcinoma Undergoing Radical Nephroureterectomy: A Systematic Review. Journal of Clinical Medicine. 2022; 11(14):4007. https://doi.org/10.3390/jcm11144007
Chicago/Turabian StyleNowak, Łukasz, Wojciech Krajewski, Jan Łaszkiewicz, Bartosz Małkiewicz, Joanna Chorbińska, Francesco Del Giudice, Keiichiro Mori, Marco Moschini, Krzysztof Kaliszewski, Paweł Rajwa, and et al. 2022. "The Impact of Surgical Waiting Time on Oncological Outcomes in Patients with Upper Tract Urothelial Carcinoma Undergoing Radical Nephroureterectomy: A Systematic Review" Journal of Clinical Medicine 11, no. 14: 4007. https://doi.org/10.3390/jcm11144007