Weight Gain in a Sample of Patients Affected by Overweight/Obesity with and without a Psychiatric Diagnosis during the Covid-19 Lockdown

 ,
,  , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Procedures
2.2. Participants
2.3. Survey Measures
2.4. The General Health Questionnaire-12
2.5. The Depression, Anxiety, and Stress Scale—21 Items
2.6. Risk Perception
2.7. The Social Connections (SC) Subscale
2.8. The Binge Eating Scale
2.9. The Difficulties in Emotion Regulation Scale
2.10. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Brooks, S.K.; Webster, R.K.; Smith, L.E.; Woodland, L.; Wessely, S.; Greenberg, N.; Rubin, G.J. The psychological impact of quarantine and how to reduce it: Rapid review of the evidence. Lancet 2020, 395, 912–920. [Google Scholar] [CrossRef] [Green Version]
- Fiorillo, A.; Gorwood, P. The consequences of the COVID-19 pandemic on mental health and implications for clinical practice. Eur. Psychiatry 2020, 63, e32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kang, L.; Ma, S.; Chen, M.; Yang, J.; Wang, Y.; Li, R.; Yao, L.; Bai, H.; Cai, Z.; Xiang Yang, B.; et al. Impact on mental health and perceptions of psychological care among medical and nursing staff in Wuhan during the 2019 novel coronavirus disease outbreak: A cross-sectional study. Brain Behav. Immun. 2020, 87, 11–17. [Google Scholar] [CrossRef] [PubMed]
- Hao, F.; Tan, W.; Jiang, L.; Zhang, L.; Zhao, X.; Zou, Y.; Hu, Y.; Luo, X.; Jiang, X.; McIntyre, R.S.; et al. Do psychiatric patients experience more psychiatric symptoms during COVID-19 pandemic and lockdown? A case-control study with service and research implications for immunopsychiatry. Brain Behav. Immun. 2020, 87, 100–106. [Google Scholar] [CrossRef] [PubMed]
- Ahorsu, D.K.; Lin, C.-Y.; Imani, V.; Saffari, M.; Griffiths, M.D.; Pakpour, A.H. The Fear of COVID-19 Scale: Development and Initial Validation. Int. J. Ment. Health Addict. 2020. [Google Scholar] [CrossRef] [Green Version]
- Mazza, C.; Ricci, E.; Biondi, S.; Colasanti, M.; Ferracuti, S.; Napoli, C.; Roma, P. A Nationwide Survey of Psychological Distress among Italian People during the COVID-19 Pandemic: Immediate Psychological Responses and Associated Factors. Int. J. Environ. Res. Public Health 2020, 17, 3165. [Google Scholar] [CrossRef]
- Roma, P.; Monaro, M.; Colasanti, M.; Ricci, E.; Biondi, S.; Di Domenico, A.; Verrocchio, M.C.; Napoli, C.; Ferracuti, S.; Mazza, C. A 2-Month Follow-Up Study of Psychological Distress among Italian People during the COVID-19 Lockdown. Int. J. Environ. Res. Public Health 2020, 17, 8180. [Google Scholar] [CrossRef]
- Katsoulis, M.; Pasea, L.; Lai, A.; Dobson, R.J.; Denaxas, S.; Hemingway, H.; Banerjee, A. Obesity during the COVID-19 pandemic: Cause of high risk or an effect of lockdown? A population-based electronic health record analysis in 1 958 184 individuals. Health Policy 2020. [Google Scholar] [CrossRef]
- World Health Organization. Obesity and Overweight; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- Van Hout, G.; van Heck, G. Bariatric Psychology, Psychological Aspects of Weight Loss Surgery. Obes. Facts 2009, 2, 10–15. [Google Scholar] [CrossRef]
- Malik, S.; Mitchell, J.E.; Engel, S.; Crosby, R.; Wonderlich, S. Psychopathology in bariatric surgery candidates: A review of studies using structured diagnostic interviews. Compr. Psychiatry 2014, 55, 248–259. [Google Scholar] [CrossRef] [Green Version]
- Sarwer, D.B.; Wadden, T.A.; Fabricatore, A.N. Psychosocial and Behavioral Aspects of Bariatric Surgery. Obes. Res. 2005, 13, 639–648. [Google Scholar] [CrossRef] [PubMed]
- Branley-Bell, D.; Talbot, C.V. Exploring the impact of the COVID-19 pandemic and UK lockdown on individuals with experience of eating disorders. J. Eat. Disord. 2020, 8, 44. [Google Scholar] [CrossRef] [PubMed]
- Castellini, G.; Cassioli, E.; Rossi, E.; Innocenti, M.; Gironi, V.; Sanfilippo, G.; Felciai, F.; Monteleone, A.M.; Ricca, V. The impact of COVID-19 epidemic on eating disorders: A longitudinal observation of pre versus post psychopathological features in a sample of patients with eating disorders and a group of healthy controls. Int. J. Eat. Disord. 2020, 53, 1855–1862. [Google Scholar] [CrossRef] [PubMed]
- Goldberg, D.P.; Williams, P. A user’s Guide to the General Health Questionnaire; GL Assessment: London, UK, 2006; ISBN 9780700511822. [Google Scholar]
- Giorgi, G.; Leon Perez, J.M.; Castiello, D.; Antonio, A.; Fiz Perez, F.J.; Arcangeli, G. The General Health Questionaire (GHQ-12) in a Sample of Italian Workers: Mental Health at Individual and Organizational Level. World J. Med. Sci. 2014. [Google Scholar] [CrossRef]
- Piccinelli, M.; Bisoffi, G.; Bon, M.G.; Cunico, L.; Tansella, M. Validity and test–retest reliability of the Italian version of the 12-item General Health Questionnaire in general practice: A comparison between three scoring methods. Compr. Psychiatry 1993, 34, 198–205. [Google Scholar] [CrossRef]
- Piccinelli, M.; Politi, P. Struttura fattoriale della versione a 12 domande del General Health Questionnaire in un campione di giovani maschi adulti. Epidemiol. Psichiatr. Soc. 1993, 2, 173–181. [Google Scholar] [CrossRef]
- Bottesi, G.; Ghisi, M.; Altoè, G.; Conforti, E.; Melli, G.; Sica, C. The Italian version of the Depression Anxiety Stress Scales-21: Factor structure and psychometric properties on community and clinical samples. Compr. Psychiatry 2015, 60, 170–181. [Google Scholar] [CrossRef]
- Cho, H.; Lee, J.-S. The influence of self-efficacy, subjective norms, and risk perception on behavioral intentions related to the H1N1 flu pandemic: A comparison between Korea and the US: Cross-national comparison of behavioral intention. Asian J. Soc. Psychol. 2015, 18, 311–324. [Google Scholar] [CrossRef]
- Liao, Q.; Cowling, B.J.; Lam, W.W.; Ng, D.M.; Fielding, R. Anxiety, worry and cognitive risk estimate in relation to protective behaviors during the 2009 influenza A/H1N1 pandemic in Hong Kong: Ten cross-sectional surveys. BMC Infect. Dis. 2014, 14, 169. [Google Scholar] [CrossRef] [Green Version]
- Kiplinger, V.L.; Browne, C.H. Parents’ Assessment of Protective Factors: User’s Guide and Technical Report; Center for the Study of Social Policy: Washington, DC, USA, 2014. [Google Scholar]
- Gormally, J.; Black, S.; Daston, S.; Rardin, D. The assessment of binge eating severity among obese persons. Addict. Behav. 1982, 7, 47–55. [Google Scholar] [CrossRef]
- Ricca, V.; Mannucci, E.; Moretti, S.; Di Bernardo, M.; Zucchi, T.; Cabras, P.L.; Rotella, C.M. Screening for binge eating disorder in obese outpatients. Compr. Psychiatry 2000, 41, 111–115. [Google Scholar] [CrossRef]
- Marcus, M.D.; Wing, R.R.; Hopkins, J. Obese binge eaters: Affect, cognitions, and response to behavioral weight control. J. Consult. Clin. Psychol. 1988, 56, 433–439. [Google Scholar] [CrossRef] [PubMed]
- Gratz, K.L.; Roemer, L. Multidimensional Assessment of Emotion Regulation and Dysregulation: Development, Factor Structure, and Initial Validation of the Difficulties in Emotion Regulation Scale. J. Psychopathol. Behav. Assess. 2004, 26, 41–54. [Google Scholar] [CrossRef]
- Sighinolfi, C.; Norcini, P.A.; Chiri, L.R.; Marchetti, I.; Sica, C. Difficulties in emotion regulation scale (DERS): The Italian translation and adaptation. Psicoter. Cogn. Comport. 2010, 16, 141–170. [Google Scholar]
- Pierce, C.A.; Block, R.A.; Aguinis, H. Cautionary Note on Reporting Eta-Squared Values from Multifactor ANOVA Designs. Educ. Psychol. Meas. 2004, 64, 916–924. [Google Scholar] [CrossRef]
- Faul, F.; Erdfelder, E.; Lang, A.-G.; Buchner, A. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef]
- Hosmer, D.W.; Lemeshow, S. Applied Logistic Regression: Hosmer/Applied Logistic Regression; John Wiley and Sons, Inc.: Hoboken, NJ, USA, 2000; ISBN 9780471722144. [Google Scholar]
- Muzi, L.; Tieghi, L.; Rugo, M.A.; Lingiardi, V. Evaluating empirically valid and clinically meaningful change in intensive residential treatment for severe eating disorders at discharge and at a 6-month follow-up. Eat. Weight Disord. 2019. [Google Scholar] [CrossRef]
- Muzi, L.; Tieghi, L.; Rugo, M.A.; Lingiardi, V. Personality as a Predictor of Symptomatic Change in a Residential Treatment Setting for Anorexia Nervosa and Bulimia Nervosa. Eat. Weight Disord. 2020. [Google Scholar] [CrossRef]
- Fontanesi, L.; Marchetti, D.; Mazza, C.; Di Giandomenico, S.; Roma, P.; Verrocchio, M.C. The effect of the COVID-19 lockdown on parents: A call to adopt urgent measures. Psychol. Trauma Theory Res. Pract. Policy 2020, 12, S79–S81. [Google Scholar] [CrossRef]
- Mazza, C.; Ricci, E.; Marchetti, D.; Fontanesi, L.; Di Giandomenico, S.; Verrocchio, M.C.; Roma, P. How Personality Relates to Distress in Parents during the Covid-19 Lockdown: The Mediating Role of Child’s Emotional and Behavioral Difficulties and the Moderating Effect of Living with Other People. Int. J. Environ. Res. Public Health 2020, 17, 6236. [Google Scholar] [CrossRef]
- Marchetti, D.; Fontanesi, L.; Mazza, C.; Di Giandomenico, S.; Roma, P.; Verrocchio, M.C. Parenting-related exhaustion during the italian COVID-19 lockdown. J. Pediatric Psychol. 2020, 45. [Google Scholar] [CrossRef]
- Flesia, L.; Monaro, M.; Mazza, C.; Fietta, V.; Colicino, E.; Segatto, B.; Roma, P. Predicting Perceived Stress Related to the Covid-19 Outbreak through Stable Psychological Traits and Machine Learning Models. J. Clin. Med. 2020, 9, 3350. [Google Scholar] [CrossRef] [PubMed]
- Roma, P.; Monaro, M.; Muzi, L.; Colasanti, M.; Ricci, E.; Biondi, S.; Napoli, C.; Ferracuti, S.; Mazza, C. How to Improve Compliance with Protective Health Measures during the COVID-19 Outbreak: Testing a Moderated Mediation Model and Machine Learning Algorithms. Int. J. Environ. Res. Public Health 2020, 17, 7252. [Google Scholar] [CrossRef] [PubMed]
- Di Crosta, A.; Palumbo, R.; Marchetti, D.; Ceccato, I.; La Malva, P.; Maiella, R.; Cipi, M.; Roma, P.; Mammarella, N.; Verrocchio, M.C.; et al. Individual Differences, Economic Stability, and Fear of Contagion as Risk Factors for PTSD Symptoms in the COVID-19 Emergency. Front. Psychol. 2020, 11. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; APA Publishing: Washington, DC, USA, 2013. [Google Scholar]
- Simon, G.E.; Von Korff, M.; Saunders, K.; Miglioretti, D.L.; Crane, P.K.; van Belle, G.; Kessler, R.C. Association Between Obesity and Psychiatric Disorders in the US Adult Population. Arch. Gen. Psychiatry 2006, 63, 824. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pagoto, S.; Bodenlos, J.S.; Kantor, L.; Gitkind, M.; Curtin, C.; Ma, Y. Association of Major Depression and Binge Eating Disorder with Weight Loss in a Clinical Setting. Obesity 2007, 15, 2557–2559. [Google Scholar] [CrossRef] [PubMed]
- Amianto, F.; Lavagnino, L.; Leombruni, P.; Gastaldi, F.; Daga, G.A.; Fassino, S. Hypomania across the binge eating spectrum. A study on hypomanic symptoms in full criteria and sub-threshold binge eating subjects. J. Affect. Disord. 2011, 133, 580–583. [Google Scholar] [CrossRef] [PubMed]
- Roma, P.; Pompili, M.; Lester, D.; Girardi, P.; Ferracuti, S. Incremental conditions of isolation as a predictor of suicide in prisoners. Forensic Sci. Int. 2013, 233, e1–e2. [Google Scholar] [CrossRef] [PubMed]



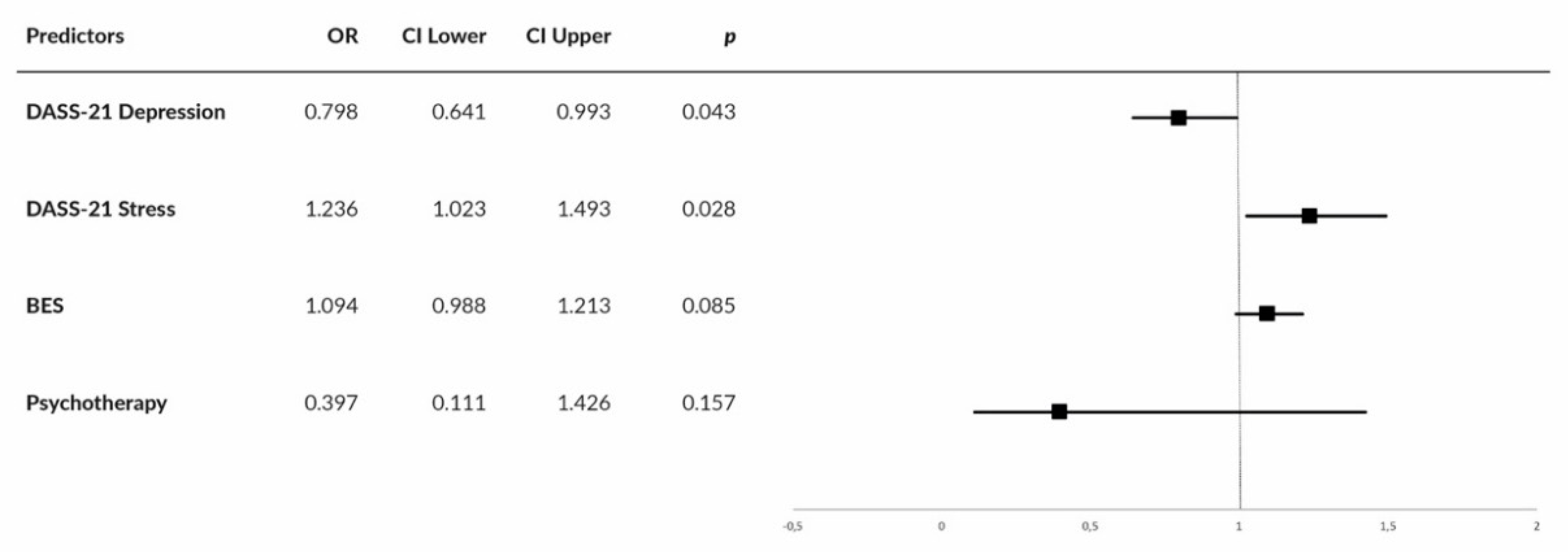{kind=link}
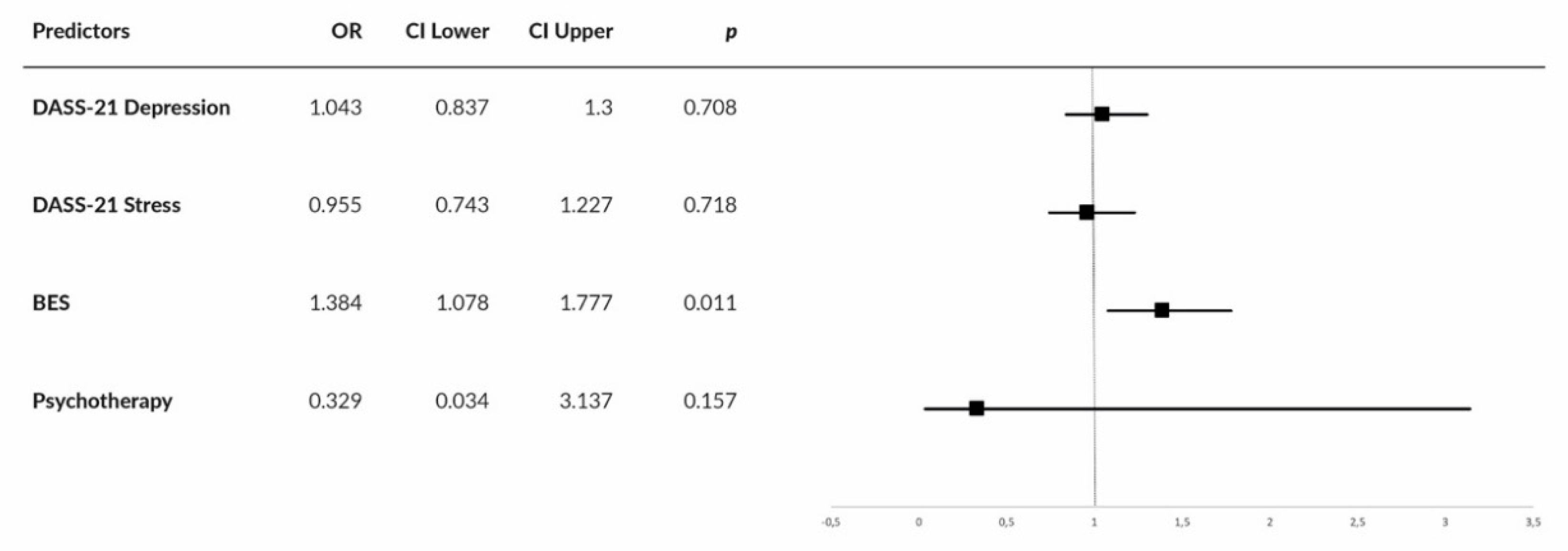{kind=link}
| Characteristic | Group | without a Psychiatric Diagnosis (n = 63) n (%) | with a Psychiatric Diagnosis (n = 47) n (%) |
|---|---|---|---|
| Citizenship | Italian | 60 (95.2) | 45 (95.7) |
| Foreign | 3 (4.8) | 2 (4.3) | |
| Region of residence | Center | 61 (96.8) | 43 (91.5) |
| South/islands | 2 (3.2) | 4 (8.5) | |
| Education | Middle school diploma | 16 (25.4) | 11 (23.4) |
| High school diploma | 24 (38.1) | 23 (48.9) | |
| Graduate | 14 (22.2) | 7 (14.9) | |
| Postgraduate | 9 (14.3) | 6 (12.8) | |
| Marital status | Unmarried | 18 (28.6) | 14 (29.8) |
| Married | 30 (47.6) | 22 (46.8) | |
| Cohabitant | 5 (7.9) | 5 (10.6) | |
| Divorced | 1 (1.6) | 3 (6.4) | |
| Separated | 5 (7.9) | 1 (2.1) | |
| Widower | 4 (6.3) | 2 (4.3) | |
| Occupation | Employee | 34 (54) | 19 (40.4) |
| Freelancer | 7 (11.1) | 6 (12.8) | |
| Unemployed | 14 (22.2) | 13 (27.7) | |
| Student | 2 (3.2) | 4 (8.5) | |
| Retired | 6 (9.5) | 5 (10.6) | |
| Spending social distancing period with | Alone | 8 (12.7) | 7 (14.9) |
| Family | 36 (57.1) | 29 (61.7) | |
| Partner | 13 (20.6) | 11 (23.4) | |
| Roommate(s) | 3 (4.8) | ||
| Child(ren) | 2 (3.2) | ||
| Other(s) | 1 (1.6) | ||
| Use of psychotherapy | Never | 42 (66.7) | 19 (40.4) |
| Previously/currently | 21 (33.3) | 28 (59.6) | |
| Use of psychopharmacology | Never | 53 (84.1) | 33 (70.2) |
| Previously/currently | 10 (15.9) | 14 (29.8) | |
| Infected acquaintances or loved ones | No | 57 (90.5) | 41 (87.2) |
| Yes | 6 (9.5) | 6 (12.8) | |
| Deaths among infected | No | 60 (95.2) | 46 (97.9) |
| acquaintances or loved ones | Yes | 3 (4.8) | 1 (2.1) |
| Patients without a Psychiatric Diagnosis (n = 63) n (%) | Patients with a Psychiatric Diagnosis (n = 47) n (%) | p | ||
|---|---|---|---|---|
| Increased compulsive binge eating | I have never practiced compulsive binge eating | 9 (14.3%) | 5 (10.6%) | 0.276 |
| Not at all | 29 (46%) | 17 (36.2%) | ||
| Rarely | 16 (25.4%) | 11 (23.4%) | ||
| Often | 7 (11.1%) | 13 (27.7%) | ||
| Very often | 2 (3.2%) | 1 (2.1%) | ||
| Increased food intake at meals | Not at all | 25 (39.7%) | 14 (29.8%) | 0.553 |
| Rarely | 28 (44.4%) | 22 (46.8%) | ||
| Often | 8 (12.7%) | 10 (21.3%) | ||
| Very often | 2 (3.2%) | 1 (2.1%) | ||
| Increased food intake between meals | I have never eaten between meals | 7 (11.1%) | 2 (4.3%) | 0.297 |
| Less frequent | 11 (17.5%) | 7 (14.9%) | ||
| Equal | 22 (34.9%) | 12 (25.5%) | ||
| More frequent | 20 (31.7%) | 21 (44.7%) | ||
| Much more frequent | 3 (4.8%) | 5 (10.6%) | ||
| Increased intake of snacks and junk food | I have never eaten snacks or junk food | 13 (20.6%) | 7 (14.9%) | 0.373 |
| Less frequent | 15 (23.8%) | 10 (21.3%) | ||
| Equal | 18 (28.6%) | 11 (23.4%) | ||
| More frequent | 17 (27%) | 17 (36.2%) | ||
| Much more frequent | 0 | 2 (4.3%) | ||
| Increased night eating episodes | I have never got up at night to eat | 12 (19%) | 5 (10.6%) | 0.085 |
| Less frequent | 11 (17.5%) | 17 (36.2%) | ||
| Equal | 2 (3.2%) | 0 | ||
| More frequent | 0 | 1 (2.1%) | ||
| Much more frequent | 38 (60.3%) | 24 (51.1%) |
| Scale | Cronbach’s Alpha | without a Psychiatric Diagnosis (n = 63) M (SD) | with a Psychiatric Diagnosis (n = 47) M (SD) | p | parn2 |
|---|---|---|---|---|---|
| GHQ-12 total score | 0.86 | 17.83 (5.7) | 19.49 (6.4) | 0.154 | 0.019 |
| DASS-21 Depression | 0.89 | 4.16 (4.6) | 6.4 (5.3) | 0.019 | 0.050 |
| DASS-21 Anxiety | 0.86 | 2.81 (3.5) | 4.06 (4.7) | 0.113 | 0.023 |
| DASS-21 Stress | 0.92 | 5.67 (4.9) | 7.98 (6) | 0.028 | 0.044 |
| Risk Perception | 0.78 | 19.48 (4.2) | 19.96 (4.4) | 0.565 | 0.003 |
| BES | 0.90 | 7.89 (6.9) | 14.4 (11.2) | <0.001 | 0.116 |
| none-to-minimal level | 55 (87.3%) | 32 (68.1%) | |||
| moderate level | 7 (11.1%) | 8 (17%) | |||
| severe level | 1 (1.6%) | 7 (14.9%) | |||
| SC subscale | 0.95 | 2.8 (1.2) | 2.67 (1.1) | 0.564 | 0.003 |
| DERS total score | 0.92 | 71.92 (20.9) | 78.32 (23.8) | 0.138 | 0.020 |
| Non-acceptance of emotional responses | 0.91 | 10.51 (5.1) | 12.70 (6.5) | 0.051 | 0.035 |
| Difficulties engaging in goal-directed behavior | 0.89 | 10.56 (4.9) | 12.49 (5.8) | 0.062 | 0.032 |
| Lack of trust in one’s own emotional regulation skills | 0.84 | 15.89 (6.5) | 17.30 (7.4) | 0.293 | 0.010 |
| Difficulties in controlling behavior | 0.83 | 9.73 (3.8) | 10.43 (5) | 0.410 | 0.006 |
| Difficulties in emotion recognition | 0.74 | 10.41 (4.3) | 9.85 (4.1) | 0.490 | 0.004 |
| Reduced emotional awareness | 0.80 | 7.19 (3.6) | 6.85 (3.1) | 0.606 | 0.002 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marchitelli, S.; Mazza, C.; Lenzi, A.; Ricci, E.; Gnessi, L.; Roma, P. Weight Gain in a Sample of Patients Affected by Overweight/Obesity with and without a Psychiatric Diagnosis during the Covid-19 Lockdown. Nutrients 2020, 12, 3525. https://doi.org/10.3390/nu12113525
Marchitelli S, Mazza C, Lenzi A, Ricci E, Gnessi L, Roma P. Weight Gain in a Sample of Patients Affected by Overweight/Obesity with and without a Psychiatric Diagnosis during the Covid-19 Lockdown. Nutrients. 2020; 12(11):3525. https://doi.org/10.3390/nu12113525
Chicago/Turabian StyleMarchitelli, Serena, Cristina Mazza, Andrea Lenzi, Eleonora Ricci, Lucio Gnessi, and Paolo Roma. 2020. "Weight Gain in a Sample of Patients Affected by Overweight/Obesity with and without a Psychiatric Diagnosis during the Covid-19 Lockdown" Nutrients 12, no. 11: 3525. https://doi.org/10.3390/nu12113525