
Associations of Dietary Intakes with Gynecological Cancers: Findings from a Cross-Sectional Study
 ,
,
Abstract
:1. Introduction
2. Methods
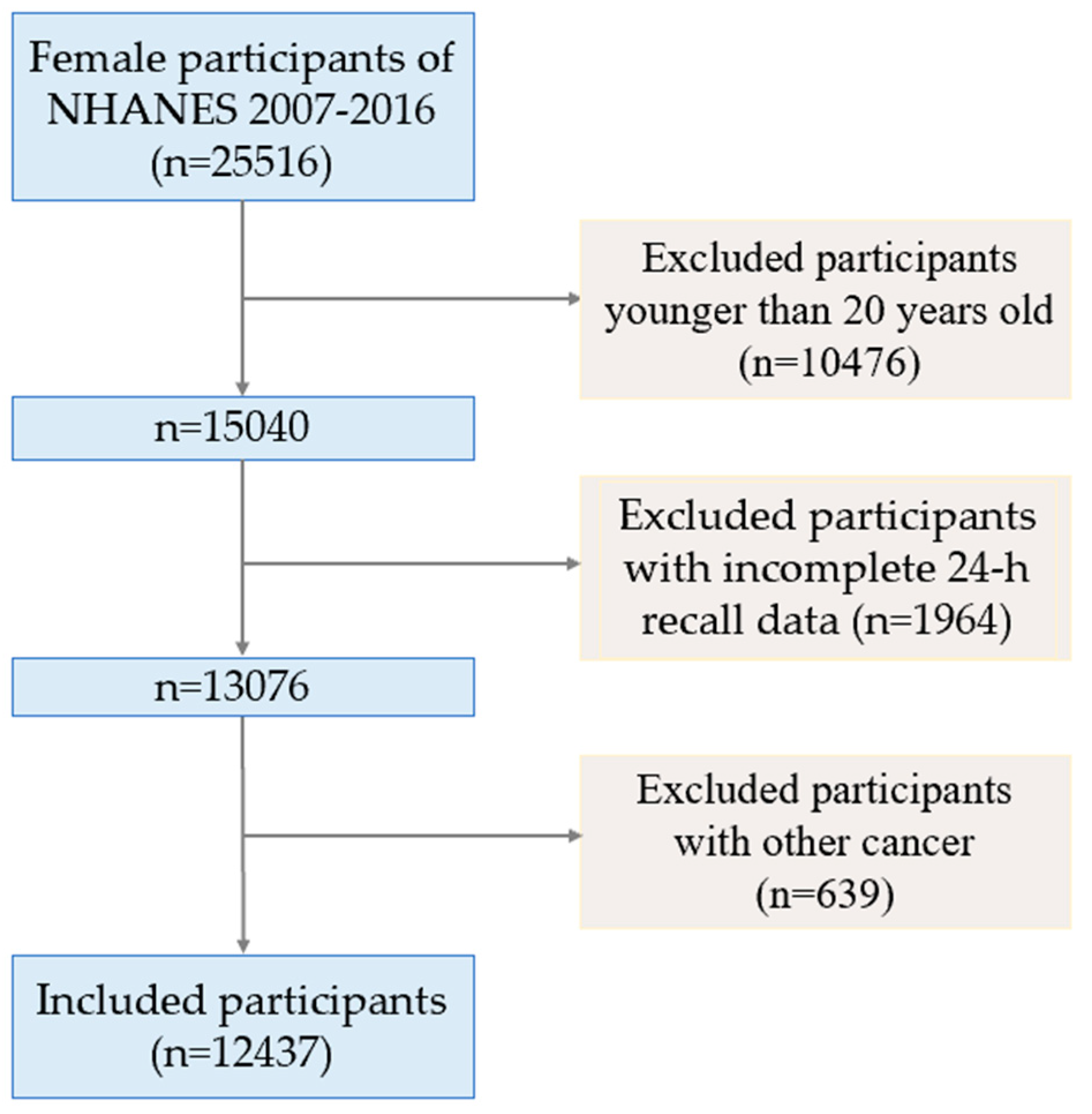
2.1. Study Design and Population
2.2. Outcomes
2.3. Dietary Intakes
2.4. Covariates
2.5. Statistical Analysis
3. Results
3.1. Characteristics of Included Participants
3.2. Dietary Intakes and Gynecological Cancer Risk
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferlay, J.; Colombet, M.; Soerjomataram, I.; Parkin, D.M.; Piñeros, M.; Znaor, A.; Bray, F. Cancer statistics for the year 2020: An overview. Int. J. Cancer 2021, 149, 778–789. [Google Scholar] [CrossRef] [PubMed]
- Siegel, R.L.; Miller, K.D.; Fuchs, H.E.; Jemal, A. Cancer statistics. CA Cancer J. Clin. 2022, 72, 7–33. [Google Scholar] [CrossRef] [PubMed]
- Doubeni, C.A.; Doubeni, A.R.; Myers, A.E. Diagnosis and Management of Ovarian Cancer. Am. Fam. Physician 2016, 93, 937–944. [Google Scholar] [PubMed]
- Wang, Q.; Peng, H.; Qi, X.; Wu, M.; Zhao, X. Targeted therapies in gynecological cancers: A comprehensive review of clinical evidence. Signal Transduct. Target. Ther. 2020, 5, 137. [Google Scholar] [CrossRef]
- Doll, R. The lessons of life: Keynote address to the nutrition and cancer conference. Cancer Res. 1992, 52, 2024s–2029s. [Google Scholar] [PubMed]
- Thanikachalam, K.; Khan, G. Colorectal Cancer and Nutrition. Nutrients 2019, 11, 164. [Google Scholar] [CrossRef] [Green Version]
- Cicco, P.D.; Catani, M.V.; Gasperi, V.; Sibilano, M.; Quaglietta, M.; Savini, I. Nutrition and Breast Cancer: A Literature Review on Prevention, Treatment and Recurrence. Nutrients 2019, 11, 1514. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oczkowski, M.; Dziendzikowska, K.; Pasternak-Winiarska, A.; Włodarek, D.; Gromadzka-Ostrowska, J. Dietary Factors and Prostate Cancer Development, Progression, and Reduction. Nutrients 2021, 13, 496. [Google Scholar] [CrossRef]
- Sun, Y.; Li, Z.; Li, J.; Li, Z.; Han, J. A Healthy Dietary Pattern Reduces Lung Cancer Risk: A Systematic Review and Meta-Analysis. Nutrients 2016, 8, 134. [Google Scholar] [CrossRef] [PubMed]
- Rieck, G.; Fiander, A. The effect of lifestyle factors on gynaecological cancer. Best Pract. Res. Clin. Obstet. Gynaecol. 2006, 20, 227–251. [Google Scholar] [CrossRef]
- Ciebiera, M.; Esfandyari, S.; Siblini, H.; Prince, L.; Elkafas, H.; Wojtyla, C.; Al-Hendy, A.; Ali, M. Nutrition in Gynecological Diseases: Current Perspectives. Nutrients 2021, 13, 1178. [Google Scholar] [CrossRef] [PubMed]
- Barchitta, M.; Maugeri, A.; Quattrocchi, A.; Agrifoglio, O.; Scalisi, A.; Agodi, A. The Association of Dietary Patterns with High-Risk Human Papillomavirus Infection and Cervical Cancer: A Cross-Sectional Study in Italy. Nutrients 2018, 10, 469. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cohen, C.W.; Fontaine, K.R.; Arend, R.C.; Soleymani, T.; Gower, B.A. Favorable Effects of a Ketogenic Diet on Physical Function, Perceived Energy, and Food Cravings in Women with Ovarian or Endometrial Cancer: A Randomized, Controlled Trial. Nutrients 2018, 10, 1187. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barchitta, M.; Maugeri, A.; La Mastra, C.; Rosa, M.C.; Favara, G.; Lio, R.M.S.; Agodi, A. Dietary Antioxidant Intake and Human Papillomavirus Infection: Evidence from a Cross-Sectional Study in Italy. Nutrients 2020, 12, 1384. [Google Scholar] [CrossRef]
- Markowska, A.; Antoszczak, M.; Markowska, J.; Huczyński, A. Role of Vitamin C in Selected Malignant Neoplasms in Women. Nutrients 2022, 14, 882. [Google Scholar] [CrossRef] [PubMed]
- Ricceri, F.; Giraudo, M.T.; Fasanelli, F.; Milanese, D.; Sciannameo, V.; Fiorini, L.; Sacerdote, C. Diet and endometrial cancer: A focus on the role of fruit and vegetable intake, Mediterranean diet and dietary inflammatory index in the endometrial cancer risk. BMC Cancer 2017, 17, 757. [Google Scholar] [CrossRef] [Green Version]
- Sun, H.; Gong, T.-T.; Xia, Y.; Wen, Z.-Y.; Zhao, L.-G.; Zhao, Y.-H.; Wu, Q.-J. Diet and ovarian cancer risk: An umbrella review of systematic reviews and meta-analyses of cohort studies. Clin. Nutr. 2021, 40, 1682–1690. [Google Scholar] [CrossRef]
- Ghosh, C.; Baker, J.A.; Moysich, K.B.; Rivera, R.; Brasure, J.R.; McCann, S.E. Dietary intakes of selected nutrients and food groups and risk of cervical cancer. Nutr. Cancer 2008, 60, 331–341. [Google Scholar] [CrossRef]
- Salazar-Martinez, E.; Lazcano-Ponce, E.; Sanchez-Zamorano, L.M.; Gonzalez-Lira, G.; Rios, P.E.-D.L.; Hernandez-Avila, M. Dietary factors and endometrial cancer risk. Results of a case-control study in Mexico. Int. J. Gynecol. Cancer 2005, 15, 938–945. [Google Scholar] [CrossRef]
- Parazzini, F.; Vecchia, C.L.; D’Avanzo, B.; Moroni, S.; Chatenoud, L.; Ricci, E. Alcohol and endometrial cancer risk: Findings from an Italian case-control study. Nutr. Cancer 1995, 23, 55–62. [Google Scholar] [CrossRef] [PubMed]
- Je, Y.; Vivo, I.D.; Giovannucci, E. Long-term alcohol intake and risk of endometrial cancer in the Nurses’ Health Study. Br. J. Cancer 2014, 111, 186–194. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Q.; Guo, P.; Li, H.; Chen, X.-D. Does alcohol consumption modify the risk of endometrial cancer? A dose-response meta-analysis of prospective studies. Arch. Gynecol. Obstet. 2017, 295, 467–479. [Google Scholar] [CrossRef] [PubMed]
- Sreeja, S.R.; Seo, S.S.; Kim, M.K. Associations of Dietary Glycemic Index, Glycemic Load and Carbohydrate with the Risk of Cervical Intraepithelial Neoplasia and Cervical Cancer: A Case-Control Study. Nutrients 2020, 12, 3742. [Google Scholar] [CrossRef] [PubMed]
- Coleman, H.G.; Kitahara, C.M.; Murray, L.J.; Dodd, K.W.; Black, A.; Stolzenberg-Solomon, R.Z.; Cantwell, M.M. Dietary carbohydrate intake, glycemic index, and glycemic load and endometrial cancer risk: A prospective cohort study. Am. J. Epidemiol. 2014, 179, 75–84. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hou, R.; Wu, Q.J.; Gong, T.T.; Jiang, L. Dietary fat and fatty acid intake and epithelial ovarian cancer risk: Evidence from epidemiological studies. Oncotarget 2015, 6, 43099–43119. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kotsopoulos, J.; Hankinson, S.E.; Tworoger, S.S. Dietary betaine and choline intake are not associated with risk of epithelial ovarian cancer. Eur. J. Clin. Nutr. 2010, 64, 111–114. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fung, T.T.; Brown, L.S. Dietary Patterns and the Risk of Colorectal Cancer. Curr. Nutr. Rep. 2013, 2, 48–55. [Google Scholar] [CrossRef] [PubMed]
- Willett, W. Nutritional Epidemiology; Oxford University Press: Oxford, UK, 2012. [Google Scholar]
- Hayden, K.M.; Beavers, D.P.; Steck, S.E.; Hebert, J.R.; Tabung, F.K.; Shivappa, N.; Casanova, R.; Manson, J.E.; Padula, C.B.; Salmoirago-Blotcher, E.; et al. The association between an inflammatory diet and global cognitive function and incident dementia in older women: The Women’s Health Initiative Memory Study. Alzheimers Dement. 2017, 13, 1187–1196. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention; National Center for Health Statistics. National Health and Nutrition Examination Survey [Internet]; Centers for Disease Control and Prevention: Atlanta, GA, USA, 2001.
- Arli, S.K.; Bakan, A.B.; Aslan, G. Distribution of cervical and breast cancer risk factors in women and their screening behaviours. Eur. J. Cancer Care 2019, 28, e12960. [Google Scholar] [CrossRef]
- Fortner, R.T.; Poole, E.M.; Wentzensen, N.A.; Trabert, B.; White, E.; Arslan, A.A.; Patel, A.V.; Setiawan, V.W.; Visvanathan, K.; Weiderpass, E.; et al. Ovarian cancer risk factors by tumor aggressiveness: An analysis from the Ovarian Cancer Cohort Consortium. Int. J. Cancer 2019, 145, 58–69. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Raglan, O.; Kalliala, I.; Markozannes, G.; Cividini, S.; Gunter, M.J.; Nautiyal, J.; Gabra, H.; Paraskevaidis, E.; Martin-Hirsch, P.; Tsilidis, K.K.; et al. Risk factors for endometrial cancer: An umbrella review of the literature. Int. J. Cancer 2019, 145, 1719–1730. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cramer, D.W. The epidemiology of endometrial and ovarian cancer. Hematol. Oncol. Clin. N. Am. 2012, 26, 1–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Charoenngam, N.; Ponvilawan, B.; Ungprasert, P. Higher zinc intake is associated with decreased risk of lung cancer. J. Evid. Based Med. 2021, 14, 185–187. [Google Scholar] [CrossRef] [PubMed]
- Lunardon, N.; Menardi, G.; Torelli, N. ROSE: A Package for Binary Imbalanced Learning. R J. 2014, 6, 79–89. [Google Scholar] [CrossRef] [Green Version]
- Muñoz, A.; Grant, W.B. Vitamin D and Cancer: An Historical Overview of the Epidemiology and Mechanisms. Nutrients 2022, 14, 1448. [Google Scholar] [CrossRef] [PubMed]
- Venturelli, S.; Leischner, C.; Helling, T.; Burkard, M.; Marongiu, L. Vitamins as Possible Cancer Biomarkers: Significance and Limitations. Nutrients 2021, 13, 3914. [Google Scholar] [CrossRef] [PubMed]
- Markowska, A.; Antoszczak, M.; Markowska, J.; Huczyński, A. Role of Vitamin K in Selected Malignant Neoplasms in Women. Nutrients 2022, 14, 3401. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.J.; Hazra, A.; Giovannucci, E.; Hankinson, S.E.; Rosner, B.; Vivo, I.D. One-carbon metabolism factors and endometrial cancer risk. Br. J. Cancer 2013, 108, 183–187. [Google Scholar] [CrossRef] [Green Version]
- Lu, J.; Trabert, B.; Liao, L.M.; Pfeiffer, R.M.; Michels, K.A. Dietary intake of nutrients involved in folate-mediated one-carbon metabolism and risk for endometrial cancer. Int. J. Epidemiol. 2019, 48, 474–488. [Google Scholar] [CrossRef] [PubMed]
- Choi, S.W.; Mason, J.B. Folate and carcinogenesis: An integrated scheme. J. Nutr. 2000, 130, 129–132. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spina, A.; Sapio, L.; Esposito, A.; Maiolo, F.D.; Sorvillo, L.; Naviglio, S. Inorganic Phosphate as a Novel Signaling Molecule with Antiproliferative Action in MDA-MB-231 Breast Cancer Cells. Biores. Open Access 2013, 2, 47–54. [Google Scholar] [CrossRef] [PubMed]
- Kesse, E.; Boutron-Ruault, M.-C.; Norat, T.; Riboli, E.; Clavel-Chapelon, F.; Group, E.N. Dietary calcium, phosphorus, vitamin D, dairy products and the risk of colorectal adenoma and cancer among French women of the E3N-EPIC prospective study. Int. J. Cancer 2005, 117, 137–144. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, L.v.; Heyworth, J.; McNaughton, S.; Iacopetta, B.; Clayforth, C.; Fritschi, L. Selected dietary micronutrients and the risk of right- and left-sided colorectal cancers: A case-control study in Western Australia. Ann. Epidemiol. 2011, 21, 170–177. [Google Scholar] [PubMed]
- Wang, Z.; Wang, W.; Yang, A.; Zhao, W.; Yang, J.; Wang, Z.; Wang, W.; Su, X.; Wang, J.; Song, J.; et al. Lower dietary mineral intake is significantly associated with cervical cancer risk in a population-based cross-sectional study. J. Cancer 2021, 12, 111–123. [Google Scholar] [CrossRef] [PubMed]
- Takata, Y.; Shu, X.-O.; Yang, G.; Li, H.; Dai, Q.; Gao, J.; Cai, Q.; Gao, Y.-T.; Zheng, W. Calcium intake and lung cancer risk among female nonsmokers: A report from the Shanghai Women’s Health Study. Cancer Epidemiol. Biomark. Prev. 2013, 22, 50–57. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, T.; Soong, S.J.; Alvarez, R.D.; Jr, C.E.B. A longitudinal analysis of human papillomavirus 16 infection, nutritional status, and cervical dysplasia progression. Cancer Epidemiol. Biomark. Prev. 1995, 4, 373–380. [Google Scholar]
- Margalioth, E.J.; Schenker, J.G.; Chevion, M. Copper and zinc levels in normal and malignant tissues. Cancer. 1983, 52, 868–872. [Google Scholar] [CrossRef] [PubMed]
- Adeoti, M.; Oguntola, A.; Akanni, E.; Agodirin, O.; Oyeyemi, G. Trace elements; copper, zinc and selenium, in breast cancer afflicted female patients in LAUTECH Osogbo, Nigeria. Indian J. Cancer 2015, 52, 106–109. [Google Scholar] [CrossRef] [PubMed]
- Jin, Y.; Zhang, C.; Xu, H.; Xue, S.; Wang, Y.; Hou, Y.; Kong, Y.; Xu, Y. Combined effects of serum trace metals and polymorphisms of CYP1A1 or GSTM1 on non-small cell lung cancer: A hospital based case-control study in China. Cancer Epidemiol. 2011, 35, 182–187. [Google Scholar] [CrossRef] [PubMed]
- Sohrabi, M.; Gholami, A.; Azar, M.H.; Yaghoobi, M.; Shahi, M.M.; Shirmardi, S.; Nikkhah, M.; Kohi, Z.; Salehpour, D.; Khoonsari, M.R.; et al. Trace Element and Heavy Metal Levels in Colorectal Cancer: Comparison Between Cancerous and Non-cancerous Tissues. Biol. Trace Elem. Res. 2018, 183, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Lopez, J.; Ramchandani, D.; Vahdat, L. Copper Depletion as a Therapeutic Strategy in Cancer. Met. Ions Life Sci. 2019, 19, 303–330. [Google Scholar]
- Martin, M.B.; Reiter, R.; Pham, T.; Avellanet, Y.R.; Camara, J.; Lahm, M.; Pentecost, E.; Pratap, K.; Gilmore, B.A.; Divekar, S.; et al. Estrogen-like activity of metals in MCF-7 breast cancer cells. Endocrinology 2003, 144, 2425–2436. [Google Scholar] [CrossRef] [Green Version]
- Zhang, X.; Wang, Y.; Zhao, Y.; Chen, X. Experimental study on the estrogen-like effect of mercuric chloride. Biometals 2008, 21, 143–150. [Google Scholar] [CrossRef]
- Choe, S.-Y.; Kim, S.-J.; Kim, H.-G.; Lee, J.H.; Choi, Y.; Lee, H.; Kim, Y. Evaluation of estrogenicity of major heavy metals. Sci. Total Environ. 2003, 312, 15–21. [Google Scholar] [CrossRef] [PubMed]
- Kambhampati, S.; Tieu, A.H.; Luber, B.; Wang, H.; Meltzer, S.J. Risk Factors for Progression of Barrett’s Esophagus to High Grade Dysplasia and Esophageal Adenocarcinoma. Sci. Rep. 2020, 10, 4899. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sturgeon, S.R.; Ziegler, R.G.; Brinton, L.A.; Nasca, P.C.; Mallin, K.; Gridley, G. Diet and the risk of vulvar cancer. Ann. Epidemiol. 1991, 1, 427–437. [Google Scholar] [CrossRef] [PubMed]
- Nour, A.; Joury, E.; Naja, F.; Hatahet, W.; Almanadili, A. Diet and the risk of head and neck squamous cell carcinomas in a Syrian population: A case-control study. East Mediterr. Health J. 2015, 21, 629–634. [Google Scholar] [CrossRef] [PubMed]
- VanderPloeg, L.C.; Wolfrom, D.M.; Welsch, C.W. Influence of caffeine on development of benign and carcinomatous mammary gland tumors in female rats treated with the carcinogens 7,12-dimethylbenz(a)anthracene and N-methyl-N-nitrosourea. Cancer Res. 1991, 51, 3399–3404. [Google Scholar] [PubMed]
- Rumgay, H.; Shield, K.; Charvat, H.; Ferrari, P.; Sornpaisarn, B.; Obot, I.; Islami, F.; Lemmens, V.E.P.P.; Rehm, J.; Soerjomataram, I. Global burden of cancer in 2020 attributable to alcohol consumption: A population-based study. Lancet Oncol. 2021, 22, 1071–1080. [Google Scholar] [CrossRef] [PubMed]
- Setiawan, V.W.; Monroe, K.R.; Goodman, M.T.; Kolonel, L.N.; Pike, M.C.; Henderson, B.E. Alcohol consumption and endometrial cancer risk: The multiethnic cohort. Int. J. Cancer 2008, 122, 634–638. [Google Scholar] [CrossRef] [Green Version]
- Webster, L.A.; Weiss, N.S. Alcoholic beverage consumption and the risk of endometrial cancer. Cancer and Steroid Hormone Study Group. Int. J. Epidemiol. 1989, 18, 786–791. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Y.-X.; Zhu, F.-F.; Chen, C.; Zhang, Y.-X.; Lv, X.-L.; Li, J.-W.; Luo, S.-P.; Gao, J. Association of Thiamine Intake with Human Papillomavirus (HPV) Infection in American Women: A Secondary Data Analysis Based on the National Health and Nutrition Examination Survey from 2003 to 2016. Med. Sci. Monit. 2020, 26, e924932. [Google Scholar] [CrossRef] [PubMed]
- Fernandez-Lazaro, C.I.; Martínez-González, M.Á.; Aguilera-Buenosvinos, I.; Gea, A.; Ruiz-Canela, M.; Romanos-Nanclares, A.; Toledo, E. Dietary Antioxidant Vitamins and Minerals and Breast Cancer Risk: Prospective Results from the SUN Cohort. Antioxidants 2021, 10, 340. [Google Scholar] [CrossRef]
- Levi, F.; Pasche, C.; Lucchini, F.; Vecchia, C.L. Dietary intake of selected micronutrients and breast-cancer risk. Int. J. Cancer 2001, 91, 260–263. [Google Scholar] [CrossRef] [PubMed]
- You, D.; Zhang, M.; He, W.; Wang, D.; Yu, Y.; Yu, Z.; Lange, T.; Yang, S.; Wei, Y.; Ma, H.; et al. Association between dietary sodium, potassium intake and lung cancer risk: Evidence from the prostate, lung, colorectal and ovarian cancer screening trial and the Women’s Health Initiative. Transl. Lung Cancer Res. 2021, 10, 45–56. [Google Scholar] [CrossRef]
- Papadimitriou, N.; Bouras, E.; Brandt, P.A.v.d.; Muller, D.C.; Papadopoulou, A.; Heath, A.K.; Critselis, E.; Gunter, M.J.; Vineis, P.; Ferrari, P.; et al. A Prospective Diet-Wide Association Study for Risk of Colorectal Cancer in EPIC. Clin. Gastroenterol. Hepatol. 2022, 20, 864–873. [Google Scholar] [CrossRef] [PubMed]
- Li, P.; Xu, J.; Shi, Y.; Ye, Y.; Chen, K.; Yang, J.; Wu, Y. Association between zinc intake and risk of digestive tract cancers: A systematic review and meta-analysis. Clin. Nutr. 2014, 33, 415–420. [Google Scholar] [CrossRef] [PubMed]
- Lin, S.; Yang, H. Ovarian cancer risk according to circulating zinc and copper concentrations: A meta-analysis and Mendelian randomization study. Clin. Nutr. 2021, 40, 2464–2468. [Google Scholar] [CrossRef] [PubMed]
- Batai, K.; Murphy, A.B.; Ruden, M.; Newsome, J.; Shah, E.; Dixon, M.A.; Jacobs, E.T.; Hollowell, C.M.; Ahaghotu, C.; Kittles, R.A. Race and BMI modify associations of calcium and vitamin D intake with prostate cancer. BMC Cancer 2017, 17, 64. [Google Scholar] [CrossRef] [Green Version]
- Jansson, B. Potassium, sodium, and cancer: A review. J. Environ. Pathol. Toxicol. Oncol. 1996, 15, 65–73. [Google Scholar] [PubMed]
- Deckers, I.A.G.; Brandt, P.A.v.d.; Engeland, M.V.; Soetekouw, P.M.M.B.; Baldewijns, M.M.L.L.; Goldbohm, R.A.; Schouten, L.J. Long-term dietary sodium, potassium and fluid intake; exploring potential novel risk factors for renal cell cancer in the Netherlands Cohort Study on diet and cancer. Br. J. Cancer 2014, 110, 797–801. [Google Scholar] [CrossRef] [PubMed]
- Pelucchi, C.; Tramacere, I.; Bertuccio, P.; Tavani, A.; Negri, E.; Vecchia, C.L. Dietary intake of selected micronutrients and gastric cancer risk: An Italian case-control study. Ann. Oncol. 2009, 20, 160–165. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Michalak, M.; Agellon, L.B. Importance of Nutrients and Nutrient Metabolism on Human Health. Yale J. Biol. Med. 2018, 91, 95–103. [Google Scholar] [PubMed]


{kind=link}
| Variables | Women with Cervical Cancer (n = 162) | Women without Cervical Cancer (n = 12,275) | p-Value | Women with Ovarian Cancer (n = 66) | Women without Ovarian Cancer (n = 12,371) | p-Value | Women with Endometrial Cancer (n = 104) | Women without Endometrial Cancer (n = 12,333) | p-Value |
|---|---|---|---|---|---|---|---|---|---|
| Age (years), median (IQR) a | 46.50 (35.00, 58.25) | 48.00 (34.00, 63.00) | 0.401 | 62.50 (48.00, 71.00) | 48.00 (34.00, 63.00) | <0.001 *** | 60.00 (48.25, 69.00) | 48.00 (34.00, 63.00) | <0.001 *** |
| Family Poverty-Income-Ratio, median (IQR) a | 1.63 (0.77, 2.69) | 2.19 (1.08, 3.57) | <0.001 *** | 1.73 (1.09, 3.33) | 2.19 (1.08, 3.55) | 0.584 | 2.05 (0.79, 2.57) | 2.19 (1.08, 3.57) | 0.047 * |
| BMI (kg/m3), median (IQR) a | 29.26 (24.20, 34.15) | 28.60 (24.19, 33.70) | 0.521 | 29.39 (26.50, 35.06) | 28.60 (24.17, 33.70) | 0.079 | 31.24 (26.08, 37.18) | 28.60 (24.16, 33.70) | <0.001 *** |
| Energy (kcal), median (IQR) a | 1722.00 (1278.50, 2136.50) | 1681.00 (1263.00, 2169.00) | 0.658 | 1549.50 (1041.25, 2292.75) | 1682.00 (1264.00, 2167.00) | 0.325 | 1631.50 (1144.75, 1999.50) | 1683.00 (1264.00, 2169.00) | 0.153 |
| Education, n (%) b | - | - | 0.009 ** | - | - | 0.010 * | - | - | <0.001 *** |
| Less than 9th grade | 12 (7.4%) | 1306 (10.6%) | - | 14 (21.2%) | 1304 (10.5%) | - | 24 (23.1%) | 1294 (10.5%) | - |
| 9th−11th grade | 36 (22.2%) | 1731 (14.1%) | - | 5 (7.6%) | 1762 (14.2%) | - | 19 (18.3%) | 1748 (14.2%) | - |
| More than 12th grade | 114 (70.4%) | 9238 (75.3%) | - | 47 (71.2%) | 9305 (75.2%) | - | 61 (58.7%) | 9291 (75.3%) | - |
| Race, n (%) b | - | - | <0.001*** | - | - | 0.791 | - | - | 0.012 * |
| Mexican American | 15 (9.3%) | 1960 (16.0%) | - | 14 (21.2%) | 1961 (15.9%) | - | 16 (15.4%) | 1959 (15.9%) | - |
| Other Hispanic | 13 (8.0%) | 1450 (11.8%) | - | 7 (10.6%) | 1456 (11.8%) | - | 19 (18.3%) | 1444 (11.7%) | - |
| Non-Hispanic White | 114 (70.4%) | 4909 (40.0%) | - | 26 (39.4%) | 4997 (40.4%) | - | 51 (49.0%) | 4972 (40.3%) | - |
| Non-Hispanic Black | 12 (7.4%) | 2713 (22.1%) | - | 14 (21.2%) | 2711 (21.9%) | - | 12 (11.5%) | 2713 (22.0%) | - |
| Other Race—including Multi-Racial | 8 (4.9%) | 1243 (10.1%) | - | 5 (7.6%) | 1246 (10.1%) | - | 6 (5.8%) | 1245 (10.1%) | - |
| Work activity, n (%) b | - | - | 0.005 ** | - | - | 0.950 | - | - | 0.145 |
| Vigorous | 30 (18.5%) | 1347 (11.0%) | - | 8 (12.1%) | 1369 (11.1%) | - | 7 (6.7%) | 1370 (11.1%) | - |
| Moderate | 39 (24.1%) | 2736 (22.3%) | - | 14 (21.2%) | 2761 (22.3%) | - | 30 (28.8%) | 2745 (22.3%) | - |
| Other | 93 (57.4%) | 8192 (66.7%) | - | 44 (66.7%) | 8241 (66.6%) | - | 67 (64.4%) | 8218 (66.6%) | - |
| Recreational activity, n (%) b | - | - | 0.076 | - | - | 0.025 * | - | - | 0.004 ** |
| Vigorous | 18 (11.1%) | 2092 (17.0%) | - | 5 (7.6%) | 2105 (17.0%) | - | 6 (5.8%) | 2104 (17.1%) | - |
| Moderate | 42 (25.9%) | 3390 (27.6%) | - | 14 (21.2%) | 3418 (27.6%) | - | 27 (26.0%) | 3405 (27.6%) | - |
| Other | 102 (63.0%) | 6793 (55.3%) | - | 47 (71.2%) | 6848 (55.4%) | - | 71 (68.3%) | 6824 (55.3%) | - |
| Variables Median (IQR) | Women with Cervical Cancer (n = 162) | Women without Cervical Cancer (n = 12,275) | p-Value | Women with Ovarian Cancer (n = 66) | Women without Ovarian Cancer (n = 12,371) | p-Value | Women with Endometrial Cancer (n = 104) | Women without Endometrial Cancer (n = 12,333) | p-Value |
|---|---|---|---|---|---|---|---|---|---|
| Protein (g) | 58.53 (39.76, 79.42) | 63.16 (45.76, 84.87) | 0.048 * | 56.77 (41.53, 79.73) | 63.12 (45.76, 84.88) | 0.086 | 62.50 (46.05, 82.96) | 63.10 (45.72, 84.87) | 0.708 |
| Total sugars (g) | 93.95 (52.88, 148.83) | 86.85 (56.02,127.72) | 0.166 | 77.21 (56.50, 143.16) | 86.94 (55.97, 127.87) | 0.807 | 84.36 (49.52, 129.05) | 86.92 (56.03, 127.96) | 0.601 |
| Total fat (g) | 62.00 (38.65, 87.61) | 61.37 (41.07, 87.05) | 0.888 | 56.65 (35.14, 84.04) | 61.41 (41.08, 87.06) | 0.166 | 56.41 (37.26, 82.12) | 61.41 (41.09, 87.10) | 0.144 |
| Cholesterol (mg) | 183.00 (97.00, 328.00) | 187.00 (109.00, 323.00) | 0.871 | 160.50 (100.75, 283.75) | 187.00 (109.00, 324.00) | 0.138 | 169.50 (93.25, 312.50) | 187.00 (109.00, 323.00) | 0.396 |
| Vitamin A (μg) | 362.00 (198.00, 612.25) | 435.00 (240.00, 717.00) | 0.018 * | 464.00 (190.75, 690.25) | 435.00 (239.00, 717.00) | 0.719 | 490.00 (259.75, 819.25) | 434.00 (239.00, 716.00) | 0.203 |
| Alpha-carotene (μg) | 20.50 (1.00, 166.25) | 48.00 (11.00, 270.00) | <0.001 *** | 43.00 (10.75, 319.75) | 47.00 (11.00, 269.00) | 0.877 | 68.00 (18.25, 538.50) | 47.00 (11.00, 267.00) | 0.101 |
| Beta-carotene (μg) | 448.00 (137.75, 1294.50) | 733.00 (267.00, 2376.00) | <0.001 *** | 904.00 (148.00, 3051.00) | 727.00 (264.00, 2351.00) | 0.874 | 1061.50 (386.00, 2777.00) | 726.00 (263.00, 2349.00) | 0.089 |
| Beta-cryptoxanthin (μg) | 16.50 (3.75, 54.50) | 27.00 (7.00, 90.00) | 0.001 ** | 45.50 (15.50, 150.50) | 26.00 (7.00, 90.00) | 0.011 * | 26.00 (10.00, 108.75) | 26.00 (7.00, 90.00) | 0.440 |
| Lycopene (μg) | 921.00 (0.00, 4612.75) | 1422.00 (1.00, 4591.00) | 0.153 | 1482.00 (0.00, 6221.25) | 1417.00 (1.00, 4583.00) | 0.796 | 1317.50 (5.25, 3957.75) | 1418.00 (1.00, 4595.00) | 0.844 |
| Vitamin B1 (mg) | 1.13 (0.80, 1.44) | 1.24 (0.86, 1.68) | 0.003 ** | 1.19 (0.76, 1.61) | 1.24 (0.86, 1.68) | 0.153 | 1.25 (0.86, 1.54) | 1.24 (0.86, 1.68) | 0.751 |
| Vitamin B2 (mg) | 1.61 (1.12, 2.34) | 1.59 (1.12, 2.20) | 0.429 | 1.52 (1.06, 2.04) | 1.59 (1.12, 2.20) | 0.270 | 1.55 (1.08, 2.11) | 1.59 (1.12, 2.20) | 0.517 |
| Niacin (mg) | 16.95 (12.34, 22.38) | 18.70 (13.16, 25.71) | 0.009 ** | 17.14 (12.45, 26.28) | 18.67 (13.16, 25.66) | 0.326 | 16.55 (12.52, 23.64) | 18.68 (13.16, 25.69) | 0.119 |
| Vitamin B6 (mg) | 1.25 (0.79, 1.88) | 1.48 (1.00, 2.11) | 0.001 ** | 1.27 (0.97, 2.01) | 1.48 (1.00, 2.10) | 0.303 | 1.38 (0.94, 1.90) | 1.48 (1.00, 2.10) | 0.230 |
| Food folate (μg) | 154.00 (92.50, 213.25) | 165.00 (110.00, 240.00) | 0.007 ** | 172.00 (115.00, 233.25) | 165.00 (110.00, 240.00) | 0.981 | 151.50 (104.50, 244.75) | 165.00 (110.00, 240.00) | 0.801 |
| Vitamin B12 (μg) | 3.05 (1.63, 5.02) | 3.17 (1.78, 5.14) | 0.586 | 2.59 (1.76, 4.08) | 3.17 (1.78, 5.14) | 0.185 | 3.24 (1.76, 5.07) | 3.16 (1.78, 5.14) | 0.914 |
| Vitamin C (μg) | 24.70 (9.15, 83.58) | 51.30 (20.90, 107.50) | <0.001 *** | 64.40 (24.93, 122.58) | 51.00 (20.60, 107.30) | 0.220 | 59.65 (25.73, 101.45) | 50.90 (20.70, 107.40) | 0.493 |
| Vitamin D (μg) | 2.70 (0.80, 4.73) | 2.80 (1.10, 5.40) | 0.240 | 3.05 (1.55, 5.23) | 2.80 (1.10, 5.40) | 0.623 | 3.10 (1.53, 5.45) | 2.80 (1.10, 5.40) | 0.485 |
| Vitamin E (mg) | 5.21 (3.14, 8.31) | 5.96 (3.80, 9.00) | 0.015 * | 5.20 (3.20, 9.31) | 5.95 (3.80, 9.00) | 0.407 | 5.45 (3.70, 8.04) | 5.96 (3.79, 9.00) | 0.216 |
| Vitamin K (μg) | 51.50 (25.43, 88.73) | 58.60 (32.50, 112.80) | 0.003 ** | 60.35 (25.30, 115.55) | 58.60 (32.40, 112.30) | 0.518 | 54.80 (34.03, 106.63) | 58.60 (32.30, 112.40) | 0.563 |
| Calcium (mg) | 671.50 (412.75, 1111.25) | 732.00 (479.00, 1054.00) | 0.257 | 653.00 (459.75, 982.75) | 732.00 (477.00, 1055.00) | 0.332 | 742.50 (477.00, 1004.75) | 731.00 (477.00, 1055.00) | 0.946 |
| Phosphorus (mg) | 1022.00 (703.50, 1391.00) | 1075.00 (783.00, 1429.00) | 0.075 | 947.50 (660.50, 1313.25) | 1075.00 (782.00, 1429.00) | 0.140 | 968.50 (789.75, 1406.00) | 1075.00 (782.00, 1429.00) | 0.205 |
| Magnesium (mg) | 224.00 (145.75, 306.25) | 239.00 (175.00, 320.00) | 0.093 | 229.50 (162.75, 323.00) | 239.00 (175.00, 320.00) | 0.447 | 230.00 (189.25, 303.25) | 239.00 (175.00, 320.00) | 0.800 |
| Iron (mg) | 10.04 (7.12, 13.62) | 11.22 (7.83, 15.60) | 0.003 ** | 9.84 (6.77, 13.83) | 11.20 (7.83, 15.60) | 0.064 | 10.58 (7.77, 15.25) | 11.20 (7.82, 15.59) | 0.745 |
| Zinc (mg) | 7.70 (5.39, 11.27) | 8.29 (5.76, 11.63) | 0.221 | 7.43 (5.15, 9.38) | 8.29 (5.76, 11.63) | 0.030 * | 8.47 (5.64, 11.39) | 8.28 (5.76, 11.62) | 0.820 |
| Copper (mg) | 0.95 (0.60, 1.30) | 0.99 (0.71, 1.35) | 0.048 * | 0.90 (0.61, 1.33) | 0.99 (0.71, 1.35) | 0.153 | 1.03 (0.72, 1.39) | 0.99 (0.71, 1.35) | 0.638 |
| Sodium (mg) | 2579.00 (1807.50, 3561.75) | 2729.00 (1955.00, 3676.00) | 0.172 | 2359.00 (1701.50, 3648.25) | 2726.00 (1954.00, 3674.00) | 0.164 | 2735.50 (1836.75, 3607.75) | 2725.00 (1952.50, 3675.50) | 0.576 |
| Potassium (mg) | 2063.50 (1370.75, 2881.00) | 2151.00 (1567.00, 2851.00) | 0.125 | 2303.50 (1454.50, 2996.00) | 2150.00 (1565.00, 2850.00) | 0.773 | 2163.00 (1604.75, 2905.00) | 2150.00 (1564.50, 2851.00) | 0.866 |
| Selenium (μg) | 80.95 (51.45, 111.60) | 86.50 (60.80, 118.90) | 0.057 | 75.65 (51.35, 112.70) | 86.50 (60.80, 118.90) | 0.038 * | 80.30 (56.63, 120.68) | 86.50 (60.70, 118.80) | 0.341 |
| Caffeine (mg) | 185.00 (44.50, 329.75) | 83.00 (9.00, 180.00) | <0.001 *** | 105.50 (22.50, 201.00) | 83.00 (9.00, 183.00) | 0.229 | 76.00 (6.50, 169.25) | 84.00 (9.00, 183.00) | 0.458 |
| Alcohol (g) | 0.00 (0.00, 0.00) | 0.00 (0.00, 0.00) | 0.711 | 0.00 (0.00, 0.00) | 0.00 (0.00, 0.00) | 0.894 | 0.00 (0.00, 0.00) | 0.00 (0.00, 0.00) | 0.005 ** |
| Variables | Cervical Cancer OR (CI) | p-Value | Ovarian Cancer OR (CI) | p-Value | Endometrial Cancer OR (CI) | p-Value |
|---|---|---|---|---|---|---|
| Protein (g) | 1.013 (0.990, 1.037) | 0.266 | 1.012 (0.986, 1.039) | 0.367 | 1.026 (0.998, 1.053) | 0.064 |
| Total sugars (g) | 1.003 (0.995, 1.010) | 0.468 | 1.005 (0.995, 1.015) | 0.332 | 1.005 (0.993, 1.017) | 0.386 |
| Total fat (g) | 1.010 (0.992, 1.028) | 0.293 | 1.009 (0.985, 1.033) | 0.469 | 0.987 (0.968, 1.006) | 0.160 |
| Cholesterol (mg) | 0.999 (0.998, 1.001) | 0.533 | 0.999 (0.997,1.001) | 0.313 | 1.001 (0.999, 1.002) | 0.477 |
| Vitamin A (μg) | 0.999 (0.998, 1.000) | 0.123 | 0.999 (0.998, 1.000) | 0.151 | 1.000 (0.999, 1.001) | 0.450 |
| Alpha-carotene (μg) | 1.000 (1.000, 1.000) | 0.981 | 1.000 (1.000, 1.000) | 0.214 | 1.000 (1.000, 1.000) | 0.253 |
| Beta-carotene (μg) | 1.000 (1.000, 1.000) | 0.213 | 1.000 (1.000, 1.000) | 0.072 | 1.000 (1.000, 1.000) | 0.460 |
| Beta-cryptoxanthin (μg) | 1.001 (0.999, 1.002) | 0.356 | 1.000 (0.999, 1.001) | 0.505 | 1.000 (0.999, 1.001) | 0.705 |
| Lycopene (μg) | 1.000 (1.000, 1.000) | 0.905 | 1.000 (1.000, 1.000) | 0.194 | 1.000 (1.000, 1.000) | 0.775 |
| Vitamin B1 (mg) | 0.518 (0.293, 0.916) | 0.025 * | 1.099 (0.678, 1.780) | 0.695 | 0.565 (0.276, 1.155) | 0.115 |
| Vitamin B2 (mg) | 1.362 (0.861, 2.154) | 0.182 | 0.775 (0.378, 1.586) | 0.476 | 1.465 (0.770, 2.785) | 0.237 |
| Niacin (mg) | 0.965 (0.921, 1.012) | 0.134 | 0.990 (0.930, 1.054) | 0.749 | 1.011 (0.950, 1.075) | 0.731 |
| Vitamin B6 (mg) | 1.408 (0.883, 2.246) | 0.146 | 1.170 (0.726, 1.885) | 0.510 | 1.232 (0.884, 1.717) | 0.212 |
| Food folate (μg) | 0.999 (0.996, 1.002) | 0.597 | 0.999 (0.996, 1.002) | 0.484 | 1.001 (0.998, 1.003) | 0.509 |
| Vitamin B12 (μg) | 1.067 (0.968, 1.177) | 0.186 | 1.031 (0.942,1.129) | 0.494 | 0.812 (0.714, 0.925) | 0.002 ** |
| Vitamin C (μg) | 0.999 (0.995, 1.003) | 0.639 | 1.001 (0.995, 1.006) | 0.837 | 1.000 (0.996, 1.004) | 0.993 |
| Vitamin D (μg) | 1.032 (0.966, 1.102) | 0.349 | 1.015 (0.959, 1.075) | 0.595 | 1.026 (0.949, 1.110) | 0.504 |
| Vitamin E (mg) | 0.979 (0.932, 1.029) | 0.392 | 0.979 (0.922, 1.039) | 0.471 | 0.990 (0.938, 1.045) | 0.715 |
| Vitamin K (μg) | 0.999 (0.997, 1.001) | 0.210 | 0.999 (0.997, 1.001) | 0.455 | 0.999 (0.997, 1.001) | 0.277 |
| Calcium (mg) | 1.001 (1.000, 1.002) | 0.026 * | 1.001 (1.000, 1.002) | 0.102 | 1.001 (1.000, 1.002) | 0.034 * |
| Phosphorus (mg) | 0.998 (0.996, 0.999) | 0.002 ** | 0.999 (0.997, 1.000) | 0.144 | 0.997 (0.996, 0.999) | <0.001 *** |
| Magnesium (mg) | 0.999 (0.995, 1.003) | 0.619 | 1.000 (0.996, 1.005) | 0.832 | 1.000 (0.995, 1.005) | 0.894 |
| Iron (mg) | 0.972 (0.913, 1.036) | 0.372 | 1.014 (0.947, 1.085) | 0.683 | 0.969 (0.893, 1.053) | 0.451 |
| Zinc (mg) | 1.015 (0.995, 1.079) | 0.624 | 0.886 (0.787, 0.999) | 0.048 * | 1.099 (0.990, 1.220) | 0.074 |
| Copper (mg) | 1.450 (0.796, 2.642) | 0.218 | 1.042 (0.404, 2.687) | 0.931 | 2.754 (1.313, 5.778) | 0.009 ** |
| Sodium (mg) | 1.000 (1.000, 1.000) | 0.194 | 1.000 (1.000, 1.001) | 0.487 | 1.000 (1.000, 1.001) | 0.042 * |
| Potassium (mg) | 1.000 (0.999, 1.000) | 0.607 | 1.000 (1.000, 1.001) | 0.516 | 0.999 (0.999, 1.000) | 0.032 * |
| Selenium (μg) | 1.002 (0.993, 1.012) | 0.625 | 0.997 (0.985, 1.010) | 0.674 | 1.000 (0.989, 1.011) | 0.969 |
| Caffeine (mg) | 1.002 (1.001, 1.003) | 0.003 ** | 1.000 (0.998, 1.002) | 0.861 | 0.999 (0.996, 1.001) | 0.297 |
| Alcohol (g) | 1.011 (0.996, 1.027) | 0.146 | 1.013 (0.994, 1.031) | 0.170 | 0.971 (0.950, 0.992) | 0.009 ** |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhu, G.; Li, Z.; Tang, L.; Shen, M.; Zhou, Z.; Wei, Y.; Zhao, Y.; Bai, S.; Song, L. Associations of Dietary Intakes with Gynecological Cancers: Findings from a Cross-Sectional Study. Nutrients 2022, 14, 5026. https://doi.org/10.3390/nu14235026
Zhu G, Li Z, Tang L, Shen M, Zhou Z, Wei Y, Zhao Y, Bai S, Song L. Associations of Dietary Intakes with Gynecological Cancers: Findings from a Cross-Sectional Study. Nutrients. 2022; 14(23):5026. https://doi.org/10.3390/nu14235026
Chicago/Turabian StyleZhu, Guixian, Zengbin Li, Liqiong Tang, Mingwang Shen, Zhangjian Zhou, Yuhang Wei, Yang Zhao, Shuheng Bai, and Lingqin Song. 2022. "Associations of Dietary Intakes with Gynecological Cancers: Findings from a Cross-Sectional Study" Nutrients 14, no. 23: 5026. https://doi.org/10.3390/nu14235026