
Acute Lung Injury Biomarkers in the Prediction of COVID-19 Severity: Total Thiol, Ferritin and Lactate Dehydrogenase

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Patients
2.2. Sample Preparation and Marker Measurements
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rothan, H.A.; Byrareddy, S.N. The epidemiology and pathogenesis of coronavirus disease (COVID-19) outbreak. J. Autoimmun. 2020, 109, 102433. [Google Scholar] [CrossRef]
- Chen, N.; Zhou, M.; Dong, X.; Qu, J.; Gong, F.; Han, Y.; Qiu, Y.; Wang, J.; Liu, M.; Wei, Y.; et al. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: A descriptive study. Lancet 2020, 395, 507–513. [Google Scholar] [CrossRef] [Green Version]
- Zhou, M.; Zhang, X.; Qu, J. Coronavirus disease 2019 (COVID-19): A clinical update. Front. Med. 2020, 14, 126–135. [Google Scholar] [CrossRef] [Green Version]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Wu, C.; Chen, X.; Cai, Y.; Xia, J.; Zhou, X.; Xu, S.; Huang, H.; Zhang, L.; Zhou, X.; Du, C.; et al. Risk Factors Associated With Acute Respiratory Distress Syndrome and Death in Patients With Coronavirus Disease 2019 Pneumonia in Wuhan, China. JAMA Intern. Med. 2020, 180, 934. [Google Scholar] [CrossRef] [Green Version]
- Meftahi, G.H.; Jangravi, Z.; Sahraei, H.; Bahari, Z. The possible pathophysiology mechanism of cytokine storm in elderly adults with COVID-19 infection: The contribution of “inflame-aging”. Inflamm. Res. 2020, 69, 825–839. [Google Scholar] [CrossRef]
- Wang, H.; Ma, S. The cytokine storm and factors determining the sequence and severity of organ dysfunction in multiple organ dysfunction syndrome. Am. J. Emerg. Med. 2008, 26, 711–715. [Google Scholar] [CrossRef] [PubMed]
- George, P.M.; Wells, A.U.; Jenkins, R.G. Pulmonary fibrosis and COVID-19: The potential role for antifibrotic therapy. Lancet Respir. Med. 2020, 8, 807–815. [Google Scholar] [CrossRef]
- Henry, B.M.; Oliveira, M.H.; Benoit, S.; Plebani, M.; Lippi, G. Hematologic, biochemical and immune biomarker abnormalities associated with severe illness and mortality in coronavirus disease 2019 (COVID-19): A meta-analysis. Clin. Chem. Lab. Med. 2020, 58, 1021–1028. [Google Scholar] [CrossRef] [Green Version]
- Lippi, G.; Plebani, M. Laboratory abnormalities in patients with COVID-2019 infection. Clin. Chem. Lab. Med. 2020, 58, 1131–1134. [Google Scholar] [CrossRef] [Green Version]
- Al-Samkari, H.; Karp Leaf, R.S.; Dzik, W.H.; Carlson, J.C.T.; Fogerty, A.E.; Waheed, A.; Goodarzi, K.; Bendapudi, P.K.; Bornikova, L.; Gupta, S.; et al. COVID-19 and coagulation: Bleeding and thrombotic manifestations of SARS-CoV-2 infection. Blood 2020, 136, 489–500. [Google Scholar] [CrossRef] [PubMed]
- Chan, N.C.; Weitz, J.I. COVID-19 coagulopathy, thrombosis, and bleeding. Blood 2020, 136, 381–383. [Google Scholar] [CrossRef]
- Silvagno, F.; Vernone, A.; Pescarmona, G.P. The Role of Glutathione in Protecting against the Severe Inflammatory Response Triggered by COVID-19. Antioxidants 2020, 9, 624. [Google Scholar] [CrossRef]
- Kalem, A.K.; Kayaaslan, B.; Neselioglu, S.; Eser, F.; Hasanoglu, I.; Aypak, A.; Akinci, E.; Akca, H.N.; Erel, O.; Guner, R. A useful and sensitive marker in the prediction of COVID-19 and disease severity: Thiol. Free. Radic. Biol. Med. 2021, 166, 11–17. [Google Scholar] [CrossRef] [PubMed]
- Sies, H. Oxidative stress: A concept in redox biology and medicine. Redox Biol. 2015, 4, 180–183. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, Q.; Zennadi, R. Oxidative Stress and Thrombosis during Aging: The Roles of Oxidative Stress in RBCs in Venous Thrombosis. Int. J. Mol. Sci. 2020, 21, 4259. [Google Scholar] [CrossRef]
- Bernard, G.R.; Artigas, A.; Brigham, K.L.; Carlet, J.; Falke, K.; Hudson, L.; Lamy, M.; Legall, J.R.; Morris, A.; Spragg, R.; et al. The American-European Consensus Conference on ARDS. Definitions, mechanisms, relevant outcomes, and clinical trial coordination. Am. J. Respir. Crit. Care Med. 1994, 149, 818–824. [Google Scholar] [CrossRef]
- Montañez, E.M.; Millón, C.; Boraldi, F.; Garcia-Guirado, F.; Pedraza, C.; Lara, E.; Santin, L.; Pavia, J.; Garcia-Fernandez, M. IGF-II promotes neuroprotection and neuroplasticity recovery in a long-lasting model of oxidative damage induced by glucocorticoids. Redox Biol. 2017, 13, 69–81. [Google Scholar] [CrossRef] [Green Version]
- Fernández, M.I.G.; Gheduzzi, D.; Boraldi, F.; Paolinelli, C.D.; Sánchez, P.S.; Valdivielso, P.; Morilla, M.J.; Quaglino, D.; Guerra, D.; Casolari, S.; et al. Parameters of oxidative stress are present in the circulation of PXE patients. Biochim. et Biophys. Acta Mol. Basis Dis. 2008, 1782, 474–481. [Google Scholar] [CrossRef] [Green Version]
- Tan, C.; Huang, Y.; Shi, F.; Tan, K.; Ma, Q.; Chen, Y.; Jiang, X.; Li, X. C-reactive protein correlates with computed tomographic findings and predicts severe COVID-19 early. J. Med. Virol. 2020, 92, 856–862. [Google Scholar] [CrossRef] [Green Version]
- Feldmann, M.; Maini, R.N.; Woody, J.N.; Holgate, S.T.; Winter, G.; Rowland, M.; Richards, D.; Hussell, T. Trials of anti-tumour necrosis factor therapy for COVID-19 are urgently needed. Lancet 2020, 395, 1407–1409. [Google Scholar] [CrossRef]
- Pascarella, G.; Strumia, A.; Piliego, C.; Bruno, F.; Del Buono, R.; Costa, F.; Scarlata, S.; Agrò, F.E. COVID-19 diagnosis and management: A comprehensive review. J. Intern. Med. 2020, 288, 192–206. [Google Scholar] [CrossRef] [PubMed]
- Guo, Y.-R.; Cao, Q.-D.; Hong, Z.-S.; Tan, Y.-Y.; Chen, S.-D.; Jin, H.-J.; Tan, K.-S.; Wang, D.-Y.; Yan, Y. The origin, transmission and clinical therapies on coronavirus disease 2019 (COVID-19) outbreak—An update on the status. Mil. Med. Res. 2020, 7, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Rabaan, A.; Al-Ahmed, S.; Garout, M.; Al-Qaaneh, A.; Sule, A.; Tirupathi, R.; Mutair, A.; Alhumaid, S.; Hasan, A.; Dhawan, M.; et al. Diverse Immunological Factors Influencing Pathogenesis in Patients with COVID-19: A Review on Viral Dissemination, Immunotherapeutic Options to Counter Cytokine Storm and Inflammatory Responses. Pathogens 2021, 10, 565. [Google Scholar] [CrossRef]
- Guzik, T.J.; West, N.E.J.; Black, E.; McDonald, D.; Ratnatunga, C.; Pillai, R.; Channon, K. Vascular Superoxide Production by NAD(P)H Oxidase. Circ. Res. 2000, 86, E85–E90. [Google Scholar] [CrossRef] [Green Version]
- Dong, T.; Cheng, Y.-W.; Yang, F.; Sun, P.-W.; Zhu, C.-J.; Zhu, L.; Zhang, G.-X. Chronic Stress Facilitates the Development of Deep Venous Thrombosis. Oxidative Med. Cell. Longev. 2015, 2015, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Del Valle, D.M.; Kim-Schulze, S.; Huang, H.-H.; Beckmann, N.D.; Nirenberg, S.; Wang, B.; Lavin, Y.; Swartz, T.H.; Madduri, D.; Gnjatic, S.; et al. An inflammatory cytokine signature predicts COVID-19 severity and survival. Nat. Med. 2020, 26, 1636–1643. [Google Scholar] [CrossRef] [PubMed]
- Meduri, G.U.; Headley, S.; Kohler, G.; Stentz, F.; Tolley, E.; Umberger, R.; Leeper, K. Persistent Elevation of Inflammatory Cytokines Predicts a Poor Outcome in ARDS. Chest 1995, 107, 1062–1073. [Google Scholar] [CrossRef]
- Zhang, C.; Wu, Z.; Li, J.-W.; Zhao, H.; Wang, G.-Q. Cytokine release syndrome in severe COVID-19: Interleukin-6 receptor antagonist tocilizumab may be the key to reduce mortality. Int. J. Antimicrob. Agents 2020, 55, 105954. [Google Scholar] [CrossRef] [PubMed]
- Soy, M.; Keser, G.; Atagündüz, P.; Tabak, F.; Atagündüz, I.; Kayhan, S. Cytokine storm in COVID-19: Pathogenesis and overview of anti-inflammatory agents used in treatment. Clin. Rheumatol. 2020, 39, 2085–2094. [Google Scholar] [CrossRef]
- Guzik, T.J.; A Mohiddin, S.; DiMarco, A.; Patel, V.; Savvatis, K.; Marelli-Berg, F.M.; Madhur, M.S.; Tomaszewski, M.; Maffia, P.; D’Acquisto, F.; et al. COVID-19 and the cardiovascular system: Implications for risk assessment, diagnosis, and treatment options. Cardiovasc. Res. 2020, 116, 1666–1687. [Google Scholar] [CrossRef]
- McGonagle, D.; O’Donnell, J.S.; Sharif, K.; Emery, P.; Bridgewood, C. Immune mechanisms of pulmonary intravascular coagulopathy in COVID-19 pneumonia. Lancet Rheumatol. 2020, 2, e437–e445. [Google Scholar] [CrossRef]
- Ruan, Q.; Yang, K.; Wang, W.; Jiang, L.; Song, J. Clinical predictors of mortality due to COVID-19 based on an analysis of data of 150 patients from Wuhan, China. Intensive Care Med. 2020, 46, 846–848. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, W. A potential treatment of COVID-19 with TGF-β blockade. Int. J. Biol. Sci. 2020, 16, 1954–1955. [Google Scholar] [CrossRef] [PubMed]
- Hsu, A.T.; Barrett, C.D.; DeBusk, G.M.; Ellson, C.D.; Gautam, S.; Talmor, D.S.; Gallagher, D.C.; Yaffe, M.B. Kinetics and Role of Plasma Matrix Metalloproteinase-9 Expression in Acute Lung Injury and the Acute Respiratory Distress Syndrome. Shock 2015, 44, 128–136. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abers, M.S.; Delmonte, O.M.; Ricotta, E.E.; Fintzi, J.; Fink, D.L.; de Jesus, A.A.A.; Zarember, K.A.; Alehashemi, S.; Oikonomou, V.; Desai, J.V.; et al. An immune-based biomarker signature is associated with mortality in COVID-19 patients. JCI Insight 2021, 6. [Google Scholar] [CrossRef] [PubMed]
- Davey, A.; McAuley, D.; O’Kane, C. Matrix metalloproteinases in acute lung injury: Mediators of injury and drivers of repair. Eur. Respir. J. 2011, 38, 959–970. [Google Scholar] [CrossRef] [Green Version]
- Kinnula, V.L.; Fattman, C.L.; Tan, R.J.; Oury, T.D. Oxidative Stress in Pulmonary Fibrosis. Am. J. Respir. Crit. Care Med. 2005, 172, 417–422. [Google Scholar] [CrossRef] [Green Version]
- Loffredo, L.; Violi, F. COVID-19 and cardiovascular injury: A role for oxidative stress and antioxidant treatment? Int. J. Cardiol. 2020, 312, 136. [Google Scholar] [CrossRef]
- Slominski, R.M.; Stefan, J.; Athar, M.; Holick, M.F.; Jetten, A.M.; Raman, C.; Slominski, A.T. COVID-19 and Vitamin D: A lesson from the skin. Exp. Dermatol. 2020, 29, 885–890. [Google Scholar] [CrossRef]
- Wang, J.-Z.; Zhang, R.-Y.; Bai, J. An anti-oxidative therapy for ameliorating cardiac injuries of critically ill COVID-19-infected patients. Int. J. Cardiol. 2020, 312, 137–138. [Google Scholar] [CrossRef]
- Shneider, A.; Kudriavtsev, A.; Vakhrusheva, A. Can melatonin reduce the severity of COVID-19 pandemic? Int. Rev. Immunol. 2020, 39, 153–162. [Google Scholar] [CrossRef]
- Shi, Z.; A Puyo, C. N-Acetylcysteine to Combat COVID-19: An Evidence Review. Ther. Clin. Risk Manag. 2020, 16, 1047–1055. [Google Scholar] [CrossRef]
- Violi, F.; Oliva, A.; Cangemi, R.; Ceccarelli, G.; Pignatelli, P.; Carnevale, R.; Cammisotto, V.; Lichtner, M.; Alessandri, F.; De Angelis, M.; et al. Nox2 activation in Covid-19. Redox Biol. 2020, 36, 101655. [Google Scholar] [CrossRef]
- Pincemail, J.; Cavalier, E.; Charlier, C.; Cheramy–Bien, J.-P.; Brevers, E.; Courtois, A.; Fadeur, M.; Meziane, S.; Goff, C.L.; Misset, B.; et al. Oxidative Stress Status in COVID-19 Patients Hospitalized in Intensive Care Unit for Severe Pneumonia. A Pilot Study. Antioxidants 2021, 10, 257. [Google Scholar] [CrossRef]
- Suhail, S.; Zajac, J.; Fossum, C.; Lowater, H.; McCracken, C.; Severson, N.; Laatsch, B.; Narkiewicz-Jodko, A.; Johnson, B.; Liebau, J.; et al. Role of Oxidative Stress on SARS-CoV (SARS) and SARS-CoV-2 (COVID-19) Infection: A Review. Protein J. 2020, 39, 644–656. [Google Scholar] [CrossRef]
- Giardino, I.; Edelstein, D.; Brownlee, M. Nonenzymatic glycosylation in vitro and in bovine endothelial cells alters basic fibroblast growth factor activity. A model for intracellular glycosylation in diabetes. J. Clin. Investig. 1994, 94, 110–117. [Google Scholar] [CrossRef]
- Matsuse, T.; Ohga, E.; Teramoto, S.; Fukayama, M.; Nagai, R.; Horiuchi, S.; Ouchi, Y. Immunohistochemical localisation of advanced glycation end products in pulmonary fibrosis. J. Clin. Pathol. 1998, 51, 515–519. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blondonnet, R.; Audard, J.; Belville, C.; Clairefond, G.; Lutz, J.; Bouvier, D.; Roszyk, L.; Gross, C.; Lavergne, M.; Fournet, M.; et al. RAGE inhibition reduces acute lung injury in mice. Sci. Rep. 2017, 7, 1–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jabaudon, M.; Berthelin, P.; Pranal, T.; Roszyk, L.; Godet, T.; Faure, J.-S.; Chabanne, R.; Eisenmann, N.; Lautrette, A.; Belville, C.; et al. Receptor for advanced glycation end-products and ARDS prediction: A multicentre observational study. Sci. Rep. 2018, 8, 2603. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Audard, J.; Godet, T.; Blondonnet, R.; Joffredo, J.-B.; Paquette, B.; Belville, C.; Lavergne, M.; Gross, C.; Pasteur, J.; Bouvier, D.; et al. Inhibition of the Receptor for Advanced Glycation End-Products in Acute Respiratory Distress Syndrome: A Randomised Laboratory Trial in Piglets. Sci. Rep. 2019, 9, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, H.; Wang, T.; Yuan, Z.; Cao, Y.; Zhou, Y.; He, J.; Shen, Y.; Zeng, N.; Dai, L.; Wen, F.; et al. Role of Receptor for Advanced Glycation End Products in Regulating Lung Fluid Balance in Lipopolysaccharide-induced Acute Lung Injury and Infection-Related Acute Respiratory Distress Syndrome. Shock 2018, 50, 472–482. [Google Scholar] [CrossRef]
- Spadaro, S.; Fogagnolo, A.; Campo, G.; Zucchetti, O.; Verri, M.; Ottaviani, I.; Tunstall, T.; Grasso, S.; Scaramuzzo, V.; Murgolo, F.; et al. Markers of endothelial and epithelial pulmonary injury in mechanically ventilated COVID-19 ICU patients. Crit. Care 2021, 25, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Reynolds, P.R.; Schmitt, R.E.; Kasteler, S.D.; Sturrock, A.; Sanders, K.; Bierhaus, A.; Nawroth, P.P.; Paine, R.; Hoidal, J.R. Receptors for Advanced Glycation End-Products Targeting Protect against Hyperoxia-Induced Lung Injury in Mice. Am. J. Respir. Cell Mol. Biol. 2010, 42, 545–551. [Google Scholar] [CrossRef] [PubMed]
- Yalcin Kehribar, D.; Cihangiroglu, M.; Sehmen, E.; Avci, B.; Capraz, A.; Bilgin, A.Y.; Gunaydin, C.; Ozgen, M. The receptor for advanced glycation end product (RAGE) pathway in COVID-19. Biomarkers 2021, 26, 114–118. [Google Scholar] [CrossRef]


{kind=link}
| Characteristics | ARDS | Non-ARDS | p Value |
|---|---|---|---|
| Patients n | 29 | 31 | |
| Age, years | 67 ± 13 | 64 ± 9 | NS |
| Male | 23 (79.3) | 15 (48.4) | 0.01 |
| Female | 6(20.7) | 16 (51.6) | 0.01 |
| Smoking status | |||
| Active or former smokers | 15 (51.7) | 7 (11.6) | 0.019 |
| Comorbidities | |||
| Arterial hypertension | 16 (55.2) | 15 (48.4) | NS |
| Diabetes mellitus | 11 (37.9) | 10 (32.3) | NS |
| Dyslipidaemia | 12 (41.4) | 12 (38.7) | NS |
| Heart disease | 4 (13.8) | 2 (6.4) | NS |
| Pulmonary disease | 3 (10.3) | 4 (12.9) | NS |
| Previous treatment | |||
| ACE blocker drugs | 14 (48.3) | 13 (31.9) | NS |
| Inhaled corticoids | 1 (3.4) | 4 (12.9) | NS |
| SOFA score | 3.7 ± 2.5 | 1.1 ± 1.2 | 0.000 |
| Respiratory support | |||
| Invasive mechanical ventilation | 23 (79.3) | 0 (0.0) | 0.000 |
| High Flow Nasal Cannula | 8 (27.6) | 2(6.9) | 0.028 |
| Length of IMV | 22.9 ± 13.9 | - | - |
| Final outcomes | |||
| Hospitalisation in ICU | 21 (72.4) | 1 (3.2) | 0.000 |
| Length of hospital stay (days) | 40.9 ± 25.3 | 12.65 ± 7.3 | 0.000 |
| Exitus | 5 (17.2) | 2 (6.4) | 0.049 |
| Variables | ARDS | Non-ARDS | p Value |
|---|---|---|---|
| Patients n | 29 | 31 | |
| Blood cells count | |||
| Leukocyte count (×109/L) | 6.081 ± 2.372 | 7.172 ± 2.617 | NS |
| Lymphocyte count (×109/L) | 0.988.51 ± 0.465 | 1.221 ± 0.555 | NS |
| Routine markers | |||
| LDH (U/L) | 463 ± 179 | 269 ± 61 | 0.000 |
| CRP (mg/L) | 143.6 ± 91.1 | 77.6 ± 61.2 | 0.002 |
| D-dimer (ng/mL) | 1136 ± 856 | 1260 ± 1041 | NS |
| Ferritin (ng/mL) | 1226 ± 608 | 540 ± 451 | 0.002 |
| Variables | ARDS | Non-ARDS | p Value |
|---|---|---|---|
| Patients n | 29 | 31 | |
| Blood cells count | |||
| Leukocyte count (×109/L) | 10.674 ± 3.398 | 6.550 ± 2.248 | 0.000 |
| Lymphocyte count (×109/L) | 1.371 ± 0.908 | 1.566 ± 0.741 | NS |
| Routine markers | |||
| LDH (U/L) | 330 ± 104 | 259 ± 60 | 0.002 |
| CRP (mg/L) | 77.3 ± 62.1 | 49.2 ± 63.7 | NS |
| D-dimer (ng/mL) | 3648 ± 999 | 1216 ± 1233 | 0.000 |
| Ferritin (ng/mL) | 1226 ± 608 | 540 ± 451 | 0.000 |
| Specific markers evaluated | |||
| AGE (ng/mL) | 20.88 ± 5.3 | 15.74 ± 4.7 | 0.000 |
| RAGE (ng/L) | 147.8 ± 120.6 | 504.50 ± 262.8 | 0.001 |
| IL-6 (pg/mL) | 260.5 ± 117.5 | 22.2 ± 22.3 | 0.000 |
| IL-7 (pg/mL) | 166.2 ± 174.4 | 151.6 ± 213.7 | NS |
| LOOH (μM) | 75.0 ± 4.2 | 76.9 ± 4.4 | NS |
| LPA (nM) | 142.9 ± 75.7 | 149.2 ± 74.3 | NS |
| MMP-1 (μg/L) | 2568 ± 1242 | 2519 ± 1817 | NS |
| MMP-9 (μg/L) | 236.4 ± 52.2 | 130.4 ± 91.8 | 0.000 |
| TGF-β (ng/mL) | 504.3 ± 187.7 | 481.5 ± 185.6 | NS |
| TNF-α (ng/L) | 20.89 ± 30.54 | 8.58 ± 1.20 | 0.029 |
| TNF-β (ng/L) | 16.24 ± 24.74 | 13.22 ± 17.09 | NS |
| TT (μM) | 203.4 ± 40.2 | 301.8 ± 73.1 | 0.000 |
| Variables | Exitus | Alive | p Value |
|---|---|---|---|
| Patients n | 7 | 53 | |
| Blood cells count | |||
| Leukocyte count (×109/L) | 11.377 ± 1.623 | 8.053 ± 3.315 | 0.015 |
| Lymphocyte count (×109/L) | 1.053 ± 0.506 | 1.503 ± 0.833 | 0.031 |
| Routine markers | |||
| LDH (U/L) | 402 ± 89 | 274± 78 | 0.001 |
| CRP (mg/L) | 116.5 ± 19.1 | 55.7 ± 63.9 | 0.048 |
| D-dimer (ng/mL) | 3022 ± 999 | 1989 ± 1760 | NS |
| Ferritin (ng/mL) | 1666 ± 1217 | 779 ± 476 | 0.038 |
| Specific markers evaluated | |||
| AGE (ng/mL) | 20.2 ± 5.4 | 18.0 ± 5.8 | NS |
| RAGE (ng/L) | 202.0 ± 219.6 | 357.8 ± 277.7 | NS |
| IL-6 (pg/mL) | 459.0 ± 604.3 | 104.6 ± 252.3 | 0.008 |
| IL-7 (pg/mL) | 154.0 ± 195.6 | 160.3 ± 199.1 | NS |
| LOOH (μM) | 75.5 ± 4.0 | 76.2 ± 4.4 | NS |
| LPA (nM) | 126.8 ± 76.6 | 151.3 ± 73.4 | NS |
| MMP-1 (μg/L) | 2164 ± 619 | 2604 ± 1659 | NS |
| MMP-9 (μg/L) | 159.2 ± 98.2 | 180.1 ± 92.8 | NS |
| TGF-β (ng/mL) | 371.2 ± 105.7 | 511.9 ± 191.0 | 0.009 |
| TNF-α (ng/L) | 21.66 ± 31.07 | 19.92 ± 21.33 | NS |
| TNF-β (ng/L) | 9.83 ± 0.75 | 9.97 ± 22.50 | NS |
| TT (μM) | 156.2 ± 48.5 | 266.6 ± 73.9 | 0.002 |
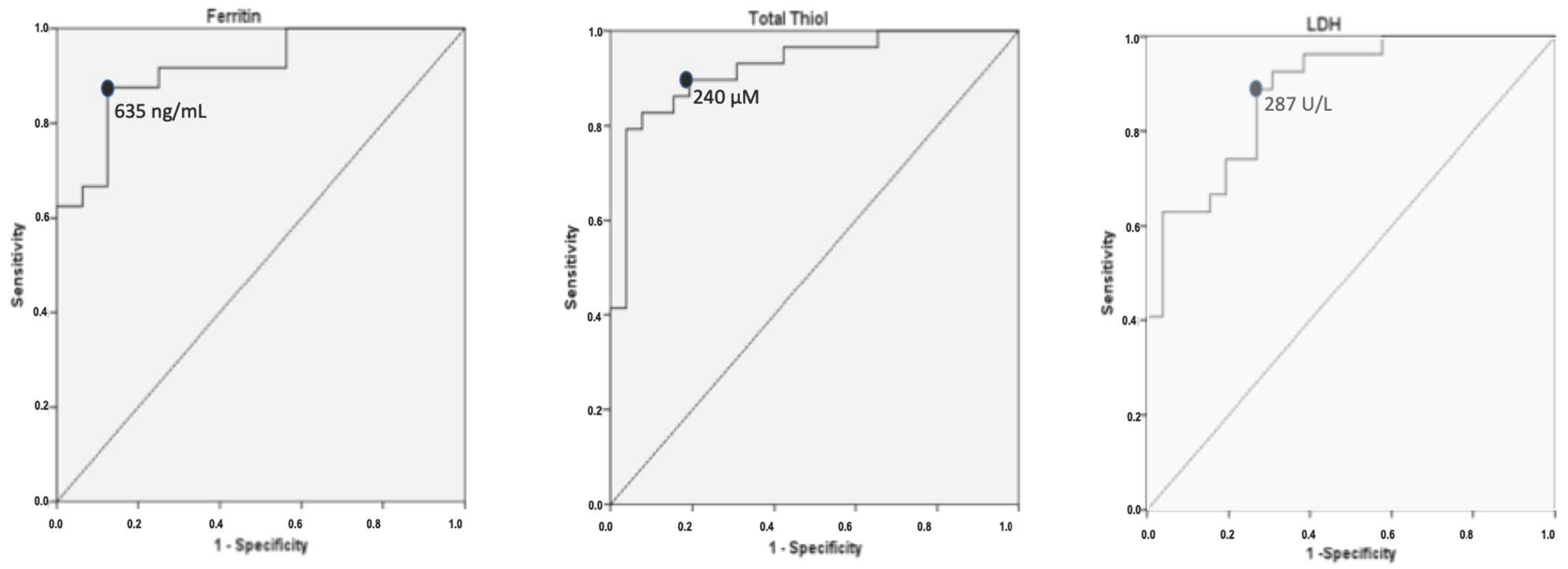
| Parameter | Sensitivity (%) | Specificity (%) | AUC | 95% CI | p Value |
|---|---|---|---|---|---|
| LDH a (U/L) | 89 | 73 | 0.89 | 0.80–0.97 | 0 |
| CRP a (mg/L) | 55.6 | 80 | 0.67 | 0.58–0.85 | 0.221 |
| Ferritin a (ng/mL) | 100 | 90 | 0.86 | 0.80–1.00 | 0.001 |
| Leukocyte count b | 84.6 | 77.8 | 0.85 | 0.75–0.95 | 0 |
| LDH b (U/L) | 46.2 | 93.5 | 0.71 | 0.57–0.85 | 0.008 |
| D-dimer b (ng/mL) | 88.5 | 73.1 | 0.86 | 0.75–0.96 | 0 |
| Ferritin b (ng/mL) | 87.5 | 81.2 | 0.91 | 0.83–1.00 | 0 |
| AGE (ng/mL) | 77.8 | 65.5 | 0.77 | 0.64–0.89 | 0.001 |
| IL-6 (pg/mL) | 79.3 | 80.6 | 0.87 | 0.79–0.96 | 0 |
| MMP-9 (µg/L) | 84.6 | 73.3 | 0.82 | 0.71–0.93 | 0 |
| TNF-α (ng/L) | 48.3 | 77.4 | 0.66 | 0.52–0.80 | 0.031 |
| TT (µM) | 86 | 85 | 0.92 | 0.85–0.99 | 0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martinez Mesa, A.; Cabrera César, E.; Martín-Montañez, E.; Sanchez Alvarez, E.; Lopez, P.M.; Romero-Zerbo, Y.; Garcia-Fernandez, M.; Velasco Garrido, J.L. Acute Lung Injury Biomarkers in the Prediction of COVID-19 Severity: Total Thiol, Ferritin and Lactate Dehydrogenase. Antioxidants 2021, 10, 1221. https://doi.org/10.3390/antiox10081221
Martinez Mesa A, Cabrera César E, Martín-Montañez E, Sanchez Alvarez E, Lopez PM, Romero-Zerbo Y, Garcia-Fernandez M, Velasco Garrido JL. Acute Lung Injury Biomarkers in the Prediction of COVID-19 Severity: Total Thiol, Ferritin and Lactate Dehydrogenase. Antioxidants. 2021; 10(8):1221. https://doi.org/10.3390/antiox10081221
Chicago/Turabian StyleMartinez Mesa, Alvaro, Eva Cabrera César, Elisa Martín-Montañez, Esther Sanchez Alvarez, Pilar Martinez Lopez, Yanina Romero-Zerbo, Maria Garcia-Fernandez, and Jose Luis Velasco Garrido. 2021. "Acute Lung Injury Biomarkers in the Prediction of COVID-19 Severity: Total Thiol, Ferritin and Lactate Dehydrogenase" Antioxidants 10, no. 8: 1221. https://doi.org/10.3390/antiox10081221