1. Introduction
The spread of the COVID-19 epidemic has brought a sharp increase in pressure on all hospitals and their healthcare systems [
1,
2,
3]. In 2020 in Europe, spread of the disease is now recognised has having occurred in two waves. The first, between March and May, reaching its peak number of cases towards the end of March, the second started in September and peaked in November [
4,
5]. These two phases in the spread of the disease differed both in terms of clinical mortality and characteristics of the individuals affected and in terms of the responses implemented by different countries. During the second wave, many countries sought to keep all treatment activities up and running, avoiding the closures that had occurred during the initial phase and trying to achieve coexistence with the spread of the virus [
6].
Fan et al. [
7] point out that worldwide—in 43 of the 53 countries surveyed—lethality of COVID-19 was reduced during the second wave, although the reasons for this are not fully understood. From the orthopaedic surgery point of view, Arshad et al. [
8] show that, in the second wave, the UK healthcare system succeeded in improving operating theatre management over that of the first wave, returning to pre-pandemic levels. However, Tyas et al. [
9] show a significant reduction in the application of best care practices in patients with a diagnosis of hip fracture, particularly with a reduction in multidisciplinary assessment activities. However, data on the outcomes for patients who underwent femur fracture surgery during the second wave are extremely limited; in particular, observations regarding the outcomes of clinical care are rarely reported [
10,
11]. Through a clinical audit analysing the first wave of COVID-19 (from March to June 2020), the authors found a pressure ulcers incidence of 21% in patients undergoing surgery for femur fracture, with a more than doubled relative risk of developing pressure ulcers as compared to femur fracture surgical patients in the pre-pandemic period.
Pressure ulcers and failure to recover deambulation are among the most significant, most sensitive indicators of the quality of the nursing care and physiotherapy provided [
12]. Chiari et al. [
13] highlighted several care-related factors as risk factors independent of pressure ulcers. These include, late catheter removal, less caregiver attendance, and less frequent changes of patient posture.
The aim of this work was therefore to measure the healthcare outcomes for patients undergoing surgery for femur fractures during the second wave of the COVID-19 pandemic within a context of the reopening orthopaedic surgery units and living with the pandemic and compare them with pre-pandemic outcomes.
2. Materials and Methods
2.1. Study Design, Setting and Sample
The retrospective observational study was conducted in a single-speciality orthopaedic hospital and covered the period running from 1 September to 20 December 2020. The data were extracted from the hospital’s computer system by consulting the patients’ medical records.
The enrolment criteria were as follows: Age over 65 years, diagnosis of fragility fractures of the femur. Patients with pathological femur fracture, a diagnosis of COVID-19 or who did not sign a consent form permitting use of the data were excluded from the study. This group of patients constituted the second wave (P2) pandemic group. In line with the previous study conducted during the first wave of the pandemic, the pre-pandemic control group (group PP: pre-pandemic) consisted of patients who underwent surgery between 1 March and 30 June 2019.
The study was conducted in accordance with the Declaration of Helsinki, and it was part of a larger research protocol approved by the hospital’s Ethics Committee (CE AVEC: 27/2021/Oss/IOR). The research protocol was registered on
ClinicalTrials.gov (NCT04882670).
2.2. Pre-Pandemic Standard Care
The on-duty orthopaedic surgeon established the surgical technique on the basis of patient age, clinical conditions, and type of fracture. Surgery was guaranteed within the first 48 h after fracture and could only be postponed for medical reasons. At admission, the patient’s risk of developing a pressure ulcer was assessed by the nurse using the Braden scale [
14]: a score of less than 17 predicted the need to use a higher-specification foam or a dynamic anti-decubitus mattress within 24 h. The nurses were responsible for moving the patient every 4 h after surgery and checking the pressure points to minimise and monitor the occurrence of any pressure ulcers. Skin care followed EPUAP guidelines [
15]. Rehabilitation treatment consisted of two sessions daily, starting the day after surgery. The aim of the rehabilitation programme was to restore standing and walking as early as possible. Each individual physiotherapy session also included exercises, performed in bed, to move the operated limb, both actively and with assistance.
During the hospital stay, each patient was allowed to have a care giver present during the day.
2.3. Hospital Reorganisation during the Second Wave of the Pandemic
Throughout the pandemic period, the hospital was identified as the referral hospital for the treatment of fractures. During the first wave, all deferrable surgery was suspended, and only emergency surgeries, such as femur fractures and osteo-oncology procedures, were performed. Of the hospital’s 11 orthopaedic wards, 4 were closed and the two wards dedicated to osteo-oncological surgery were merged. Out-patient activity was suspended. The professional resources recovered from this reorganisation were used to make up for the lack of personnel created by the spread of the pandemic as people were reassigned to supporting surveillance and screening activities implemented by Occupational Medicine and to managing the new procedure for care of patients entering the in-patient wards from the emergency department. A dedicated department was also created for the hospitalization of confirmed/probable/suspected COVID-19 cases.
During the second wave of the pandemic, in-hospital activity had been restored for most surgical wards. Only the 11-bed Physical and Rehabilitation Medicine ward had not been reopened. The healthcare staff were once more returned to their assigned departments. In the management of admissions, procedures were implemented to screen patients who underwent molecular swabbing within 48 h prior to admission. Patients who entered in-patient wards through the Emergency Department were required to remain in isolation in the department dedicated to suspected COVID-19 cases for the time needed to obtain the results of the molecular swabs.
Inside the hospital, the use of protective equipment was required in compliance with current regional and national regulations; moreover, to limit contacts and crowding inside the hospital, the presence of care givers was not permitted. Relatives of in-patients could receive information on the condition of their loved ones through discussions with the ward doctors, but they were not granted admission to the in-patient ward.
2.4. Measures
The incidence of pressure ulcers in each category, recorded in the patient’s medical record, was the primary outcome of this study. The diagnosis of pressure ulcer and definition of its category was made following the classification given in the EPUAP guidelines [
15]. Assessment of deambulation recovery time—measured as the days between the date of surgery and the date on which the patient walked for the first time, regardless of the aid used—and the number of falls recorded were the secondary outcomes of the study. Through a team of professionals experienced in the field of postoperative orthopaedic care and a search of the literature [
13,
16], variables were defined to help describe postoperative care and data collected. To facilitate reading, the variables have been separated into 3 groups:
- -
variables relating to organisation of surgical and healthcare activities, i.e., number of patients admitted, number of operators dedicated to care and complexity of the patients treated. In this context, the average weight of the in-patients and the case-mix index (CMI) were evaluated [
17]. These two indicators are calculated on the basis of the diagnosis-related group (DRG) used nationally to classify different patients according to the medical resources required for their treatment. The case-mix index reflects severity of the diseases treated and the difficulty required for their treatment within the hospital setting [
18,
19,
20];
- -
variables related to basic patient characteristics;
- -
variables related to the healthcare approaches.
3. Results
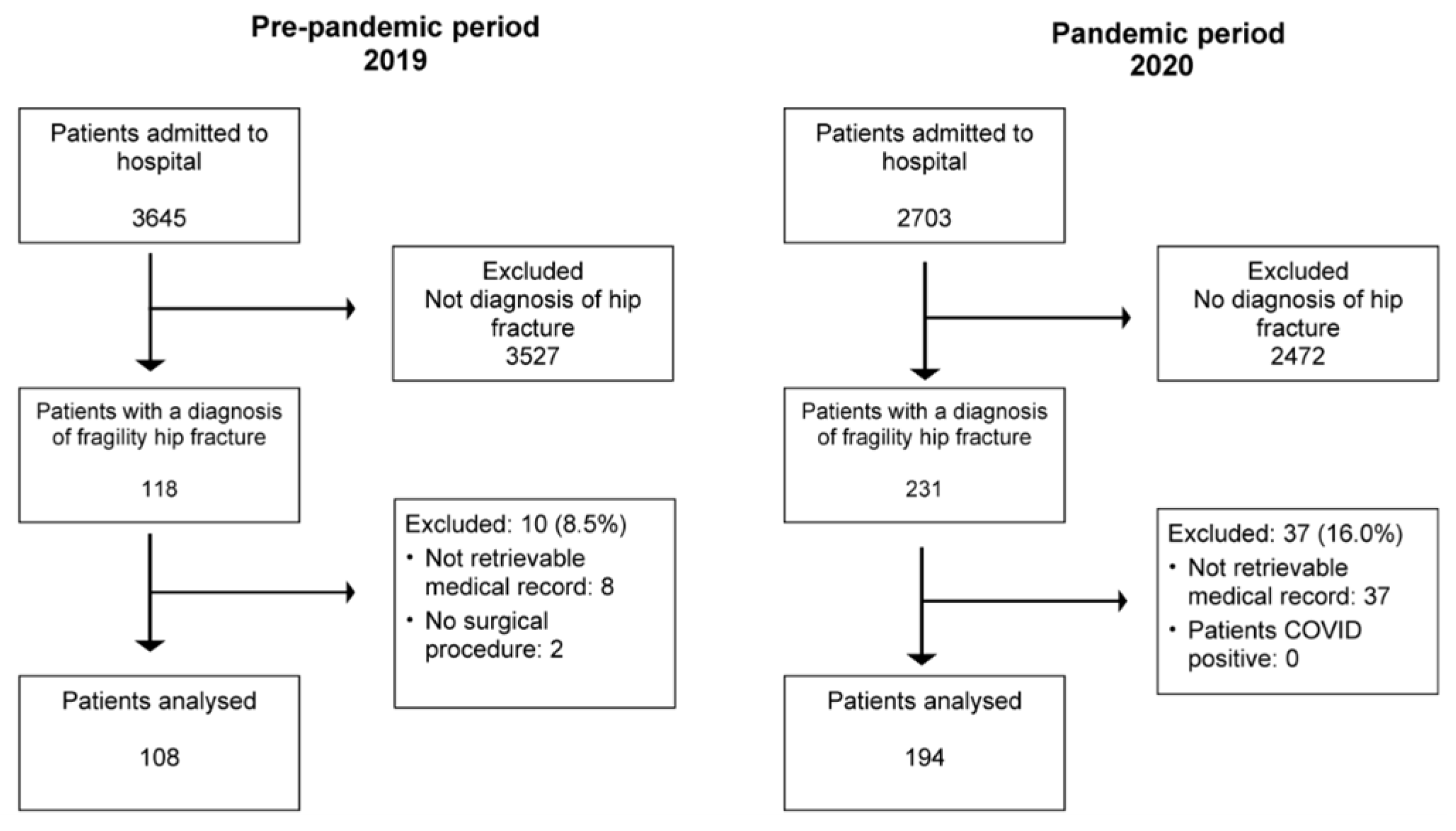
A total of 349 patients were recruited for the study through the computerised medical record system; of these, 47 (13.5%) were excluded on the basis of the established inclusion-exclusion criteria, including 10 in the pre-pandemic group and 37 in the P2 group. The pre-pandemic group consisted of 108 patients and the second wave pandemic group included 194 patients.
Figure 1 summarises the recruitment flowchart.
3.1. Profile of Hip Fracture Patients Admitted during the Second Wave of the Pandemic
The baseline characteristics of the patients that underwent surgery during the second wave were similar to those of the pre-pandemic reference patient population. The type of fracture was the only variable that differed statistically between the two groups: there was a reduction in the number of patients diagnosed with a femoral neck fracture, and consequently the type of surgery performed for this was also reduced, while the number of osteosynthesis procedures increased.
Table 1 summarises the basic patient characteristics, the variables of the healthcare approach, and the outcomes measured. As regards the healthcare approach, some differences emerged regarding the use of air mattresses—this significantly dropped from 89.8% in the pre-pandemic period to 71%—and in bladder catheter management—the number of days on the catheter and number of patients discharged with a catheter dropped during the pandemic period.
The incidence of pressure ulcers increased from 10% in the pre-pandemic period to 21% in the second wave (p = 0.016). In the pandemic period, there was a reduction in sacrum and second-degree ulcers while, at the same time, there was a sharp increase in heel and first-degree ulcers. The mean time to onset did not differ between the two study periods. A look at the recovery of deambulation shows no significant difference in either the number of people able to recover walking (78.7% vs. 76%; p = 0.56) or the recovery time in terms of days needed to walk the first time (3 days vs. 2 days; p = 0.44). In the pre-pandemic period only one event/fall was recorded for one patient, i.e., 0.9%, while, during the P2 period, four such events/falls were recorded for three patients, i.e., 2.1%.
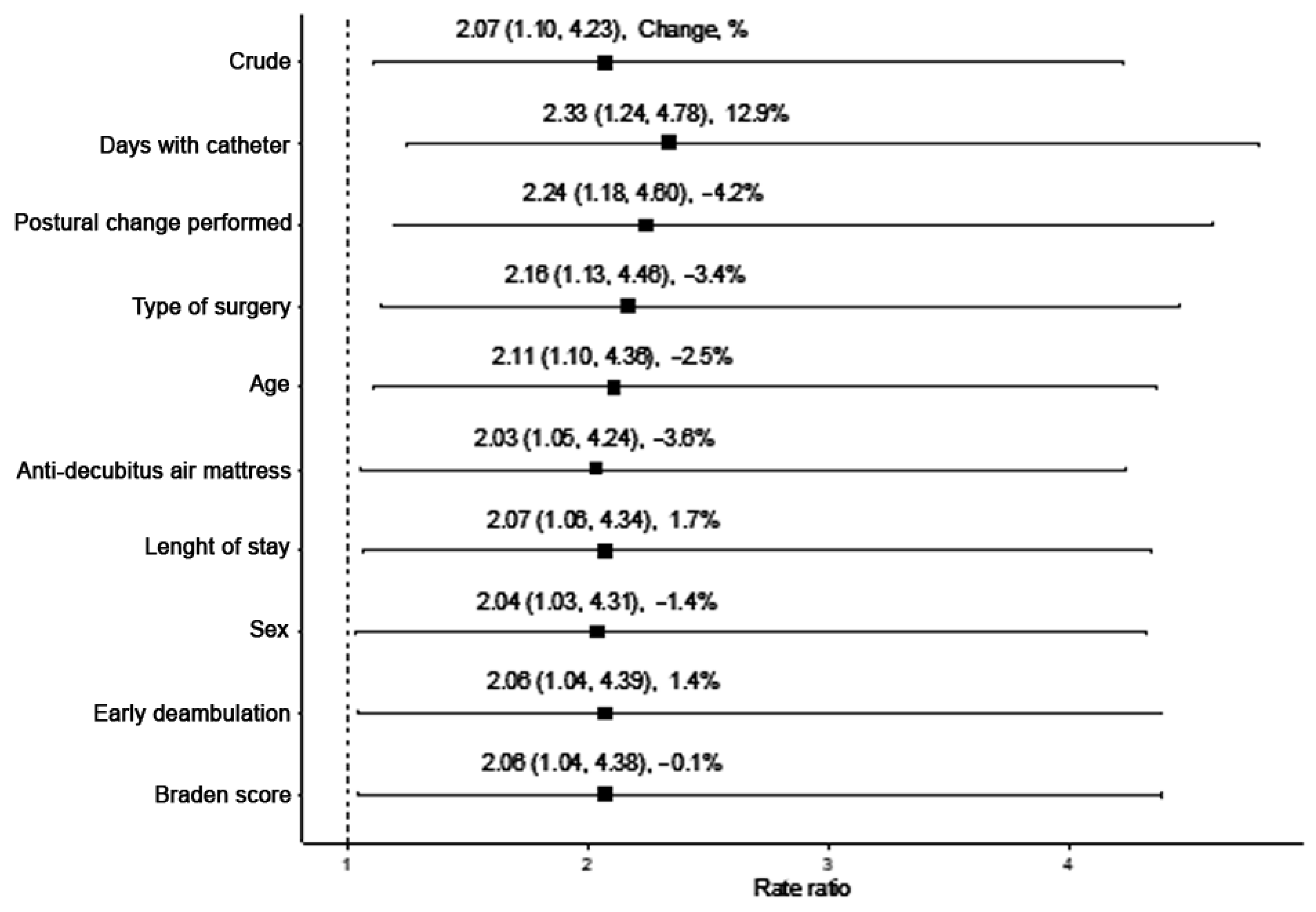
3.2. Relative Risk of Pressure Ulcers and Predictive Factors
Calculation of the crude relative risk (RR) for the incidence of pressure ulcers was 2.06 (
p = 0.023), showing a significant increase for patients admitted during the second wave (
Table 2).
Correcting the crude RR calculation for patient characteristics and characteristics of the healthcare approach (
Figure 2) did not reveal any variables that could bring a statistically significant change in RR value.
3.3. Organisation of Orthopaedic Surgery and the Healthcare Path
In 2019 and 2020, the flow of ordinary admissions showed a 25.8% drop in admissions, from 3645 to 2703. Instead, the number of patients operated on for femur fractures increased from 3% (108 patients) in 2019 to 8% in 2020 (231 patients).
Table 3 summarises the data on surgical activity performed and complexity of the patients treated by this hospital during the second wave.
The number of available beds was reduced by 21% during the pandemic period, although this reduction was partially offset by a 15% increase in occupancy rate. There was no change in the number of professionals dedicated to care within the in-patient wards while, during the pandemic period, as staff recruitment was liberalised, 12.2% of the staff were new recruits (recruited less than 12 months previously). During the pandemic period, 36 healthcare professionals (14.7%) were infected with COVID-19. The complexity of patients treated increased, with average patient incidence of complexity rising from 1.48 in the pre-pandemic period to 1.56 in the pandemic period. Similarly, the case-mix index saw a similar trend, rising from 0.99 to 1.01.
4. Discussion
In patients undergoing femur fracture surgery during the second wave of COVID-19, the incidence of pressure ulcers was 21%, a significant increase over the 10% seen in the pre-pandemic period. In the second wave of the pandemic, the relative risk of developing a pressure ulcer was 2.06 as compared to the pre-pandemic period and this was in line with the relative risk calculated for the first wave.
The population of persons undergoing surgery during the second wave of COVID-19 did not differ significantly from the pre-pandemic period; the mean age of the patients admitted for femur fracture during the second wave was 84 years, and there was no statistically significant difference from the age of the same population during the pre-pandemic period (mean age = 82 years). Looking at clinical practice factors that could be changed and that are known to prevent pressure ulcers, some significant differences emerged between the pre-pandemic period and the second wave. Bladder catheter management improved during the second wave and thus the number of people discharged with a bladder catheter and the number of days on a bladder catheter was reduced, a protective factor for patients. At the same time, moving of the patient did not differ statistically between the two periods, while the use of air mattresses fell from 90% in the pre-pandemic phase to 71%. Where air mattresses were not available, an anti-decubitus foam mattress was provided.
In correcting the RR calculation for factors linked to patient characteristics and variables linked to the healthcare approach, it was found that none of the factors taken into consideration significantly modified this indicator. The explanation for the different RR in the two periods could be sought in the different organisation of the work established so that elective surgery could be resumed within a pandemic context. First, during the pandemic period, to reduce the risk of spreading the infection, the presence of any caregivers/family members was suspended. Polancich et al. [
21] postulated that this deficiency could be one of the possible explanations for the increased incidence in pressure ulcers during hospitalisation in patients diagnosed with COVID-19. Chiari et al. [
13] identified reduced caregiver presence as an independent risk factor for pressure ulcers. Second, although the flow of admissions and available beds was reduced during the pandemic period, an increase in the bed occupancy rate and the average stay for hip fracture patients made up the difference, thus the resulting workload was comparable in the two periods. In addition, in the second wave of the pandemic, the average patient complexity was increased, resulting in a higher care burden, which may have contributed to the increase in RR. Third, during the pandemic there was a significant increase in the number of newly recruited staff (12%). This reduction in healthcare staff experience may have contributed to the increased risk of pressure ulcers despite the main prevention measures in place.
In terms of the recovery of deambulation, the number of patients who were unable to recover deambulation during their hospital stay remained limited even in the second wave. No statistically significant differences emerged compared to the pre-pandemic period and the data were in line with the first phase of the spread of COVID-19. Similarly, there was no significant difference in the early recovery of deambulation.
Limits
The study has some limitations. First, this is a retrospective study. This means that it is limited by the accuracy with which the medical records were compiled, i.e., the completeness and precision of the data. Secondly, it was not possible to find any specific information on the years of experience the healthcare staff had in orthopaedic care, a factor that could affect the risk of developing pressure ulcers. These authors believe that by conducting the study within a single-speciality orthopaedic hospital, this aspect was limited.
Further multi-centre studies aimed at analysing patients undergoing different types of orthopaedic surgeries are necessary to better understand the extent of the impact of the pandemic.
5. Conclusions
During the second wave of COVID-19, the risk of pressure ulcers for patients undergoing femur fracture surgery increased significantly. This variation cannot be attributed to the clinical characteristics of the patients or the levels of care provided, but could be explained by the absence of a caregiver for these patients and the increased average complexity of the patients managed in the orthopaedic setting. The hospital management of femur fracture patients should be carefully monitored, and these aspects taken into account when restoring the hospital’s normal surgical activities.
Author Contributions
Conceptualization, M.M., C.F. and E.A.; methodology, C.F. and E.A.; formal analysis, A.E. and M.M.; investigation, T.B.; resources, A.M. and A.M.O.; data curation, T.B.; writing—original draft preparation, M.M.; writing—review and editing, A.M. and E.A.; supervision, A.M.; project administration, C.F.; funding acquisition A.M.O. All authors have read and agreed to the published version of the manuscript.
Funding
The APC was funded by Fondi 5 × 1000 anno 2018.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the Institutional Review Board (or Ethics Committee) of Area Vasta Emilia Centro (CE AVEC: 27/2021/Oss/IOR, 01 February 2021).
Informed Consent Statement
Patient consent was waived due to retrospective nature of the study.
Data Availability Statement
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Di Gennaro, F.; Pizzol, D.; Marotta, C.; Antunes, M.; Racalbuto, V.; Veronese, N.; Smith, L. Coronavirus Diseases (COVID-19) Current Status and Future Perspectives: A Narrative Review. Int. J. Environ. Res. Public Health 2020, 17, 2690. [Google Scholar] [CrossRef] [Green Version]
- Haffer, H.; Schömig, F.; Rickert, M.; Randau, T.; Raschke, M.; Wirtz, D.; Pumberger, M.; Perka, C. Impact of the COVID-19 Pandemic on Orthopaedic and Trauma Surgery in University Hospitals in Germany: Results of a Nationwide Survey. J. Bone Joint Surg. Am. 2020, 102, e78. [Google Scholar] [CrossRef] [PubMed]
- Bchetnia, M.; Girard, C.; Duchaine, C.; Laprise, C. The outbreak of the novel severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2): A review of the current global status. J. Infect. Public Health 2020, 13, 1601–1610. [Google Scholar] [CrossRef] [PubMed]
- Diaz, R.S.; Vergara, T.R.C. The COVID-19 second wave: A perspective to be explored. Braz. J. Infect. Dis. 2021, 25, 101537. [Google Scholar] [CrossRef] [PubMed]
- Bontempi, E. The europe second wave of COVID-19 infection and the Italy “strange” situation. Environ. Res. 2021, 193, 110476. [Google Scholar] [CrossRef] [PubMed]
- Contou, D.; Fraissé, M.; Pajot, O.; Tirolien, J.A.; Mentec, H.; Plantefève, G. Comparison between first and second wave among critically ill COVID-19 patients admitted to a French ICU: No prognostic improvement during the second wave? Crit. Care 2021, 25, 3. [Google Scholar] [CrossRef]
- Fan, G.; Yang, Z.; Lin, Q.; Zhao, S.; Yang, L.; He, D. Decreased Case Fatality Rate of COVID-19 in the Second Wave: A study in 53 countries or regions. Transbound. Emerg. Dis. 2021, 68, 213–215. [Google Scholar] [CrossRef]
- Arshad, F.; Hanif, U.K.; Arshad, A.; Chaudary, M.I.; Khan, A.; Kelleher, J.; Sadiq, S.; Wasim, A.S.; Chaudhry, F. Orthopaedic Trauma Theatre Efficiency in the COVID-19 Pandemic: Are We Returning to Normality? Cureus 2021, 13, e13221. [Google Scholar] [CrossRef] [PubMed]
- Tyas, B.; Wilkinson, M.; Singisetti, K. Effect of Covid-19 on best practice care of hip fracture patients: An analysis from the National Hip Fracture Database (NHFD). Surgeon 2021, 19, e298–e303. [Google Scholar] [CrossRef] [PubMed]
- Aiken, L.H.; Sloane, D.; Griffiths, P.; Rafferty, A.M.; Bruyneel, L.; McHugh, M.; Maier, C.B.; Moreno-Casbas, T.; Ball, J.E.; Ausserhofer, D.; et al. Nursing skill mix in European hospitals: Cross-sectional study of the association with mortality, patient ratings, and quality of care. BMJ Qual. Saf. 2017, 26, 559–568. [Google Scholar] [CrossRef] [Green Version]
- Stifter, J.; Sermersheim, E.; Ellsworth, M.; Dowding, E.; Day, E.; Silvestri, K.; Margwarth, J.; Korkmaz, K.; Walkowiak, N.; Boudreau, L.; et al. COVID-19 and Nurse-Sensitive Indicators: Using Performance Improvement Teams to Address Quality Indicators During a Pandemic. J. Nurs. Care Qual. 2021, 36, 1–6. [Google Scholar] [CrossRef]
- Lyder, C.H.; Wang, Y.; Metersky, M.; Curry, M.; Kliman, R.; Verzier, N.R.; Hunt, D.R. Hospital-acquired pressure ulcers: Results from the national Medicare Patient Safety Monitoring System study. J. Am. Geriatr. Soc. 2012, 60, 1603–1608. [Google Scholar] [CrossRef] [PubMed]
- Chiari, P.; Forni, C.; Guberti, M.; Gazineo, D.; Ronzoni, S.; D’Alessandro, F. Predictive Factors for Pressure Ulcers in an Older Adult Population Hospitalized for Hip Fractures: A Prognostic Cohort Study. PLoS ONE 2017, 12, e0169909. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pancorbo-Hidalgo, P.L.; Garcia-Fernandez, F.P.; Lopez-Medina, I.M.; Alvarez-Nieto, C. Risk assessment scales for pressure ulcer prevention: A systematic review. J. Adv. Nurs. 2006, 54, 94–110. [Google Scholar] [CrossRef]
- National Pressure Ulcer Advisory Panel; European Pressure Ulcer Advisory Panel and Pan Pacific Pressure Injury Alliance. Prevention and Treatment of Pressure Ulcers: Quick Reference Guide; Haesler, E., Ed.; Cambridge Media: Osborne Park, Australia, 2014.
- Gillespie, B.M.; Walker, R.M.; Latimer, S.L.; Thalib, L.; Whitty, J.A.; McInnes, E.; Chaboyer, W.P. Repositioning for pressure injury prevention in adults. Cochrane Database Syst. Rev. 2020, 6, CD009958. [Google Scholar] [PubMed]
- D’Andrea, V.; Catania, A.; Di Matteo, F.M.; Savino, G.; Greco, R.; Di Marco, C.; De Antoni, E. L’indice di case-mix e la durata della degenza [Case-mix index and length of hospitalization]. G Chir. 2010, 31, 211–214. [Google Scholar] [PubMed]
- Ammar, W.; Khalife, J.; El-Jardali, F.; Romanos, J.; Harb, H.; Hamadeh, G.; Dimassi, H. Hospital accreditation, reimbursement and case mix: Links and insights for contractual systems. BMC Health Serv. Res. 2013, 13, 505. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Frazee, R.C.; Matejicka, A.V., 2nd; Abernathy, S.W.; Davis, M.; Isbell, T.S.; Regner, J.L.; Smith, R.W.; Jupiter, D.C.; Papaconstantinou, H.T. Concurrent chart review provides more accurate documentation and increased calculated case mix index, severity of illness, and risk of mortality. J. Am. Coll. Surg. 2015, 220, 652–656. [Google Scholar] [CrossRef]
- Mark, B.A.; Harless, D.W. Adjusting for patient acuity in measurement of nurse staffing: Two approaches. Nurs. Res. 2011, 60, 107–114. [Google Scholar] [CrossRef] [PubMed]
- Polancich, S.; Hall, A.G.; Miltner, R.; Poe, T.; Enogela, E.M.; Montgomery, A.P.; Patrician, P.A. Learning During Crisis: The Impact of COVID-19 on Hospital-Acquired Pressure Injury Incidence. J. Healthc. Qual. 2021, 43, 137–144. [Google Scholar] [CrossRef] [PubMed]
| Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).


 ,
, 


{kind=link}
{kind=link}