Timing of Adjuvant Chemotherapy and Survival in Colorectal, Gastric, and Pancreatic Cancer. A Systematic Review and Meta-Analysis


 , , ,
, , ,
Abstract
:1. Introduction
2. Results
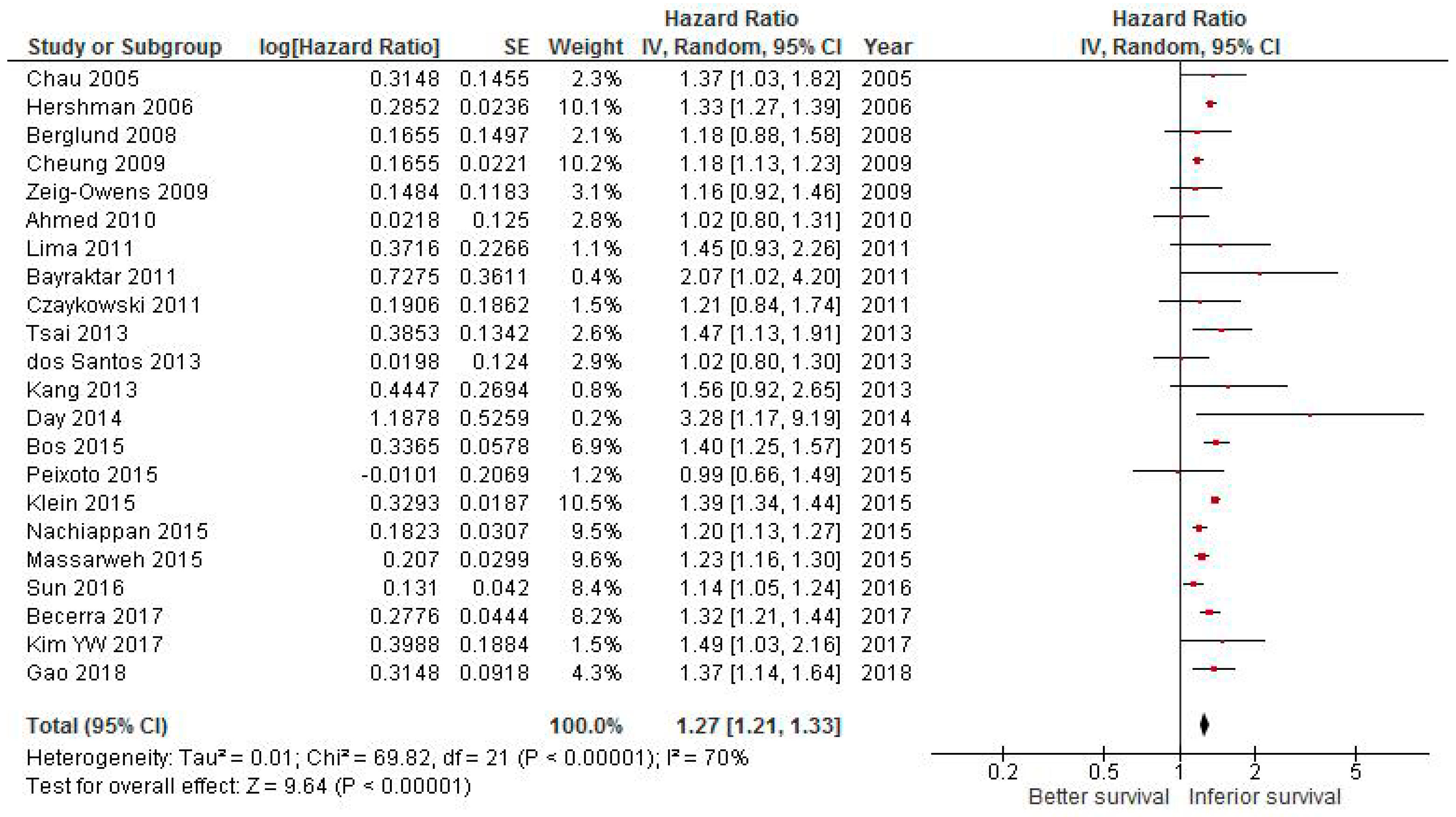
2.1. Effect of Delaying CT on Survival in Colorectal Cancer
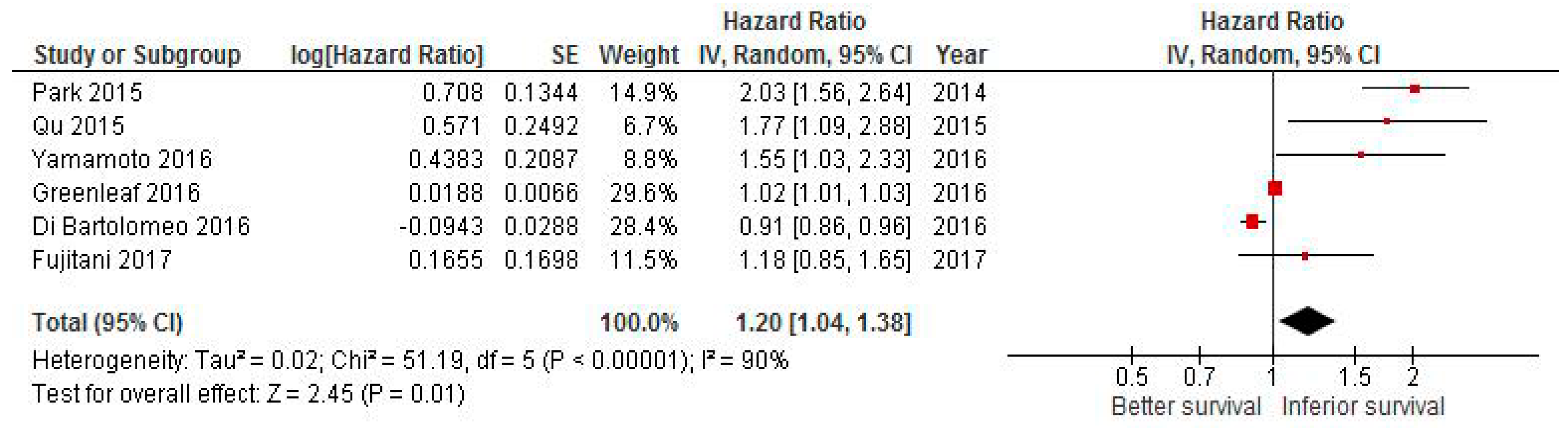
2.2. Effect of Delaying CT on Survival in Gastric Cancer
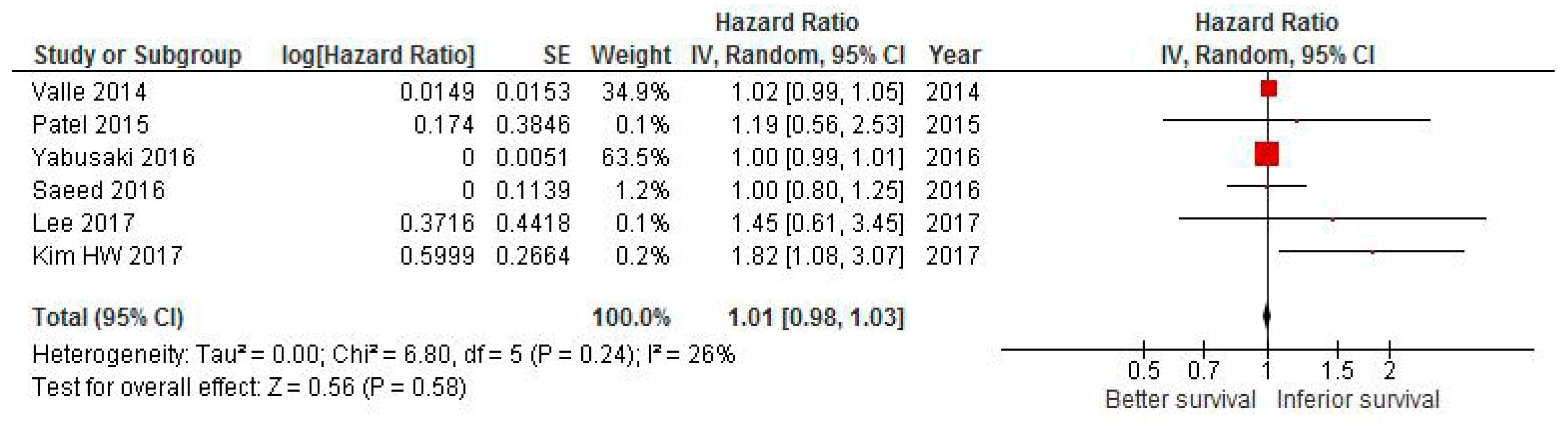
2.3. Effect of Delaying CT on Survival in Pancreatic Cancer
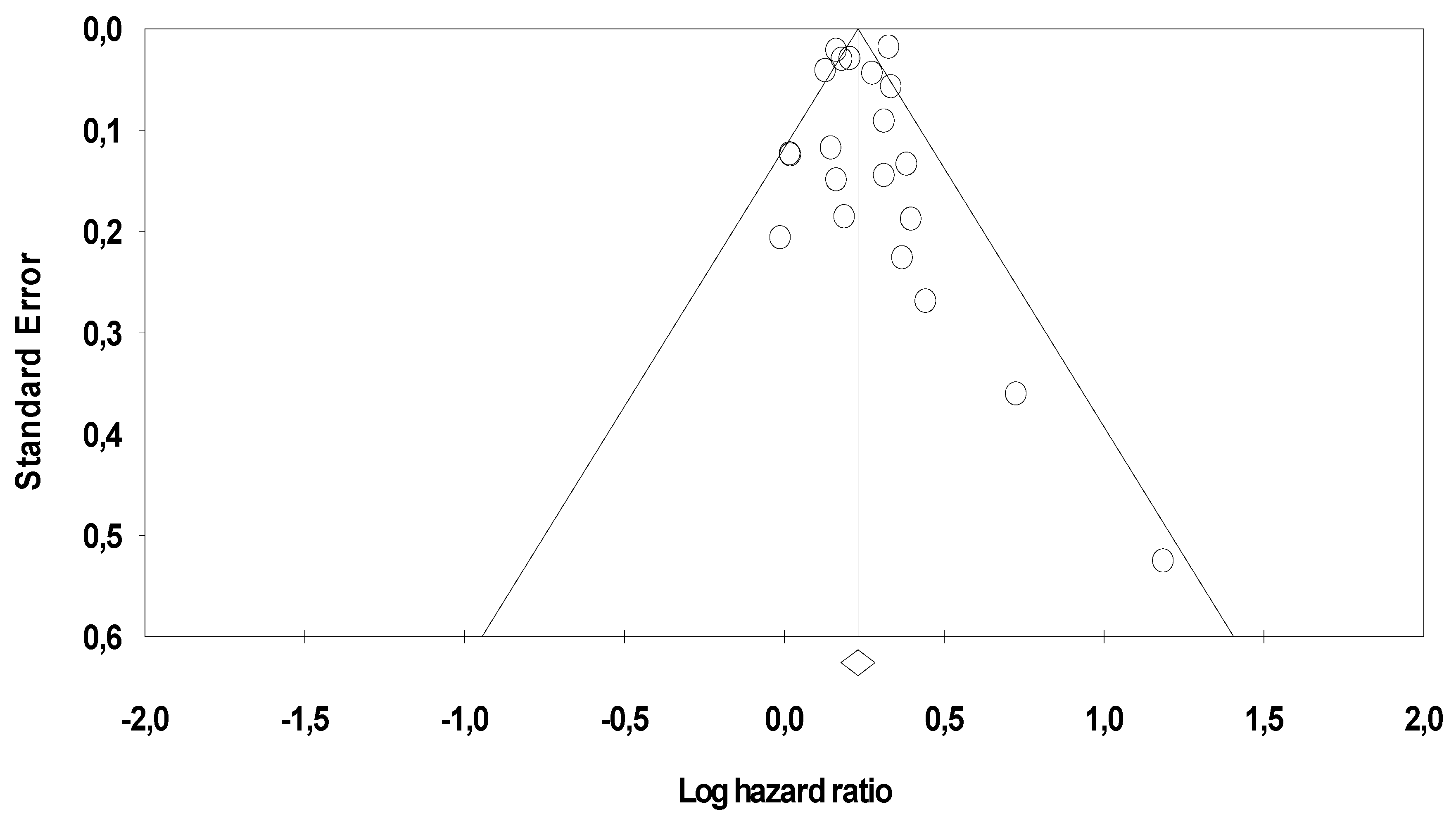
2.4. Publication Bias
3. Discussion
4. Materials and Methods
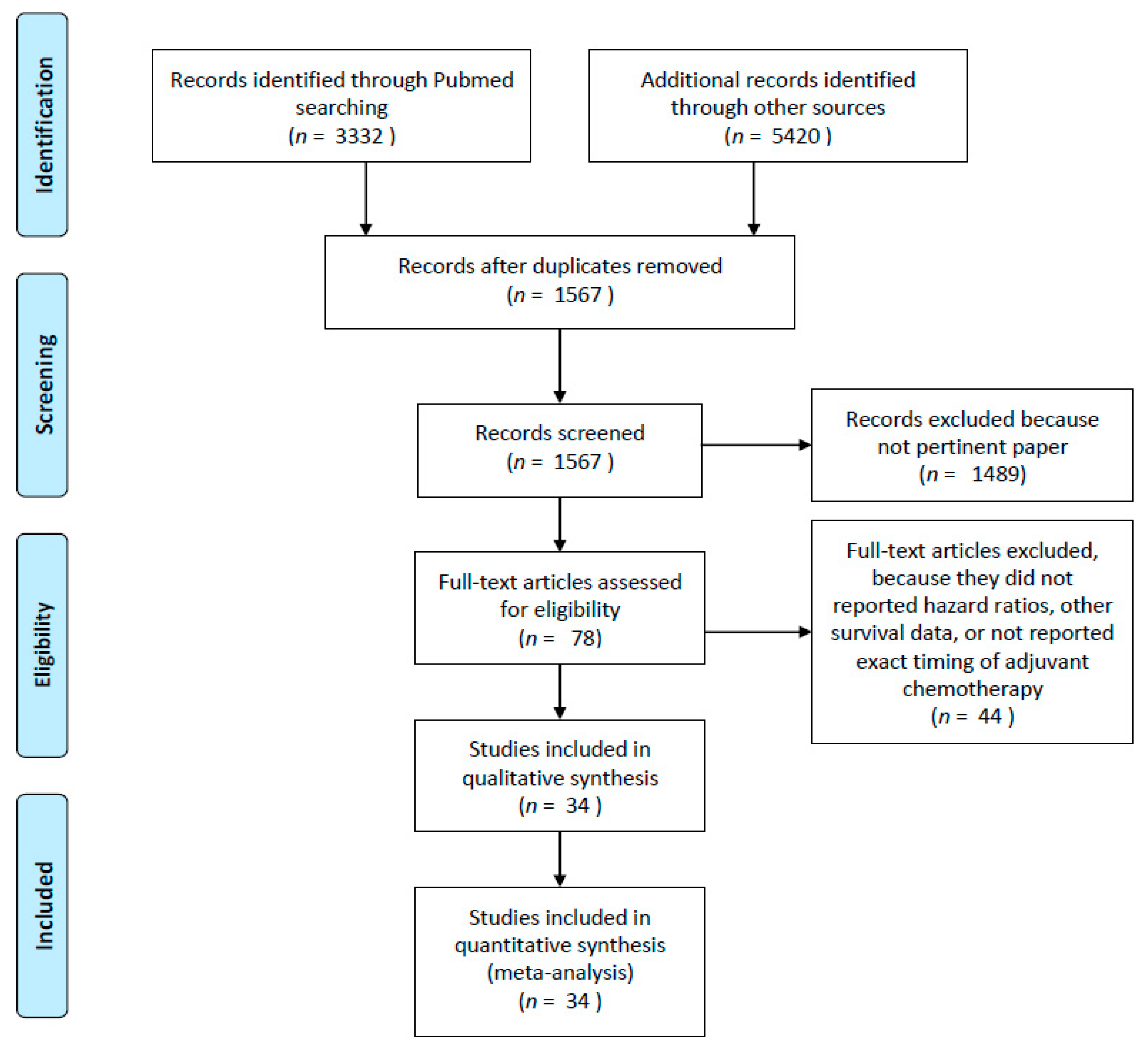
4.1. Search Strategy and Inclusion Criteria
4.2. Data Extraction
4.3. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Shah, M.A.; Renfro, L.A.; Allegra, C.J.; Andre, T.; de Gramont, A.; Schmoll, H.J.; Haller, D.G.; Alberts, S.R.; Yothers, G.; Sargent, D.J. Impact of Patient Factors on Recurrence Risk and Time Dependency of Oxaliplatin Benefit in Patients With Colon Cancer: Analysis From Modern-Era Adjuvant Studies in the Adjuvant Colon Cancer End Points (ACCENT) Database. J. Clin. Oncol. 2016, 34, 843–853. [Google Scholar] [CrossRef]
- Diaz-Nieto, R.; Orti-Rodriguez, R.; Winslet, M. Post-surgical chemotherapy versus surgery alone for resectable gastric cancer. Cochrane Database Syst. Rev. 2013. [Google Scholar] [CrossRef]
- Conroy, T.; Hammel, P.; Hebbar, M.; Ben Abdelghani, M.; Wei, A.C.; Raoul, J.L.; Chone, L.; Francois, E.; Artru, P.; Biagi, J.J.; et al. FOLFIRINOX or Gemcitabine as Adjuvant Therapy for Pancreatic Cancer. N. Engl. J. Med. 2018, 379, 2395–2406. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, S.; Ahmad, I.; Zhu, T.; Arnold, F.P.; Faiz Anan, G.; Sami, A.; Yadav, S.K.; Alvi, R.; Haider, K. Early discontinuation but not the timing of adjuvant therapy affects survival of patients with high-risk colorectal cancer: A population-based study. Dis. Colon Rectum 2010, 53, 1432–1438. [Google Scholar] [CrossRef] [PubMed]
- Bayraktar, U.D.; Chen, E.; Bayraktar, S.; Sands, L.R.; Marchetti, F.; Montero, A.J.; Rocha-Lima, C.M. Does delay of adjuvant chemotherapy impact survival in patients with resected stage II and III colon adenocarcinoma? Cancer 2011, 117, 2364–2370. [Google Scholar] [CrossRef] [PubMed]
- Becerra, A.Z.; Aquina, C.T.; Mohile, S.G.; Tejani, M.A.; Schymura, M.J.; Boscoe, F.P.; Xu, Z.; Justiniano, C.F.; Boodry, C.I.; Swanger, A.A.; et al. Variation in Delayed Time to Adjuvant Chemotherapy and Disease-Specific Survival in Stage III Colon Cancer Patients. Ann. Surg. Oncol. 2017, 24, 1610–1617. [Google Scholar] [CrossRef]
- Bos, A.C.; van Erning, F.N.; van Gestel, Y.R.; Creemers, G.J.; Punt, C.J.; van Oijen, M.G.; Lemmens, V.E. Timing of adjuvant chemotherapy and its relation to survival among patients with stage III colon cancer. Eur. J. Cancer 2015, 51, 2553–2561. [Google Scholar] [CrossRef] [PubMed]
- Cheung, W.Y.; Neville, B.A.; Earle, C.C. Etiology of delays in the initiation of adjuvant chemotherapy and their impact on outcomes for Stage II and III rectal cancer. Dis. Colon Rectum 2009, 52, 1054–1063, discussion 1064. [Google Scholar] [CrossRef]
- Czaykowski, P.M.; Gill, S.; Kennecke, H.F.; Gordon, V.L.; Turner, D. Adjuvant chemotherapy for stage III colon cancer: Does timing matter? Dis. Colon Rectum 2011, 54, 1082–1089. [Google Scholar] [CrossRef]
- Day, A.R.; Middleton, G.; Smith, R.V.; Jourdan, I.C.; Rockall, T.A. Time to adjuvant chemotherapy following colorectal cancer resection is associated with an improved survival. Colorectal Dis. 2014, 16, 368–372. [Google Scholar] [CrossRef]
- Dos Santos, L.V.; Faria, T.M.; Lima, A.B.; Abdalla, K.C.; de Moraes, E.D.; Cruz, M.R.; Lima, J.P. Timing of adjuvant chemotherapy in colorectal cancer. Colorectal Dis. 2016, 18, 871–876. [Google Scholar] [CrossRef]
- Massarweh, N.N.; Haynes, A.B.; Chiang, Y.J.; Chang, G.J.; You, Y.N.; Feig, B.W.; Cormier, J.N. Adequacy of the National Quality Forum’s Colon Cancer Adjuvant Chemotherapy Quality Metric: Is 4 Months Soon Enough? Ann. Surg. 2015, 262, 312–320. [Google Scholar] [CrossRef]
- Berglund, A.; Cedermark, B.; Glimelius, B. Is it deleterious to delay the start of adjuvant chemotherapy in colon cancer stage III? Ann. Oncol. 2008, 19, 400–402. [Google Scholar] [CrossRef]
- Chau, I.; Norman, A.R.; Cunningham, D.; Tait, D.; Ross, P.J.; Iveson, T.; Hill, M.; Hickish, T.; Lofts, F.; Jodrell, D.; et al. A randomised comparison between 6 months of bolus fluorouracil/leucovorin and 12 weeks of protracted venous infusion fluorouracil as adjuvant treatment in colorectal cancer. Ann. Oncol. 2005, 16, 549–557. [Google Scholar] [CrossRef]
- Gao, P.; Huang, X.Z.; Song, Y.X.; Sun, J.X.; Chen, X.W.; Sun, Y.; Jiang, Y.M.; Wang, Z.N. Impact of timing of adjuvant chemotherapy on survival in stage III colon cancer: A population-based study. BMC Cancer 2018, 18, 234. [Google Scholar] [CrossRef]
- Hershman, D.; Hall, M.J.; Wang, X.; Jacobson, J.S.; McBride, R.; Grann, V.R.; Neugut, A.I. Timing of adjuvant chemotherapy initiation after surgery for stage III colon cancer. Cancer 2006, 107, 2581–2588. [Google Scholar] [CrossRef]
- Kang, K.M.; Hong, K.S.; Noh, G.T.; Oh, B.Y.; Chung, S.S.; Lee, R.A.; Kim, K.H. Optimal time of initiating adjuvant chemotherapy after curative surgery in colorectal cancer patients. Ann. Coloproctol. 2013, 29, 150–154. [Google Scholar] [CrossRef]
- Kim, Y.W.; Choi, E.H.; Kim, B.R.; Ko, W.A.; Do, Y.M.; Kim, I.Y. The impact of delayed commencement of adjuvant chemotherapy (eight or more weeks) on survival in stage II and III colon cancer: A national population-based cohort study. Oncotarget 2017, 8, 80061–80072. [Google Scholar] [CrossRef]
- Klein, M.; Azaquoun, N.; Jensen, B.V.; Gogenur, I. Improved survival with early adjuvant chemotherapy after colonic resection for stage III colonic cancer: A nationwide study. J. Surg. Oncol. 2015, 112, 538–543. [Google Scholar] [CrossRef]
- Lima, I.S.; Yasui, Y.; Scarfe, A.; Winget, M. Association between receipt and timing of adjuvant chemotherapy and survival for patients with stage III colon cancer in Alberta, Canada. Cancer 2011, 117, 3833–3840. [Google Scholar] [CrossRef]
- Nachiappan, S.; Askari, A.; Mamidanna, R.; Munasinghe, A.; Currie, A.; Stebbing, J.; Faiz, O. The impact of adjuvant chemotherapy timing on overall survival following colorectal cancer resection. Eur. J. Surg. Oncol. 2015, 41, 1636–1644. [Google Scholar] [CrossRef]
- Peixoto, R.D.; Kumar, A.; Speers, C.; Renouf, D.; Kennecke, H.F.; Lim, H.J.; Cheung, W.Y.; Melosky, B.; Gill, S. Effect of delay in adjuvant oxaliplatin-based chemotherapy for stage III colon cancer. Clin. Colorectal Cancer 2015, 14, 25–30. [Google Scholar] [CrossRef]
- Sun, Z.; Adam, M.A.; Kim, J.; Nussbaum, D.P.; Benrashid, E.; Mantyh, C.R.; Migaly, J. Determining the Optimal Timing for Initiation of Adjuvant Chemotherapy After Resection for Stage II and III Colon Cancer. Dis. Colon Rectum 2016, 59, 87–93. [Google Scholar] [CrossRef]
- Tsai, W.S.; Hsieh, P.S.; Yeh, C.Y.; Chiang, J.M.; Tang, R.; Chen, J.S.; Changchien, C.R.; Wang, J.Y. Impact of chemotherapy-related prognostic factors on long-term survival in patients with stage III colorectal cancer after curative resection. Int. J. Clin. Oncol. 2013, 18, 242–253. [Google Scholar] [CrossRef]
- Zeig-Owens, R.; Gershman, S.T.; Knowlton, R.; Jacobson, J.S. Survival and time interval from surgery to start of chemotherapy among colon cancer patients. J. Registry Manag. 2009, 36, 30–41, quiz 61–32. [Google Scholar]
- Di Bartolomeo, M.; Pietrantonio, F.; Rulli, E.; Poli, D.; Berenato, R.; Caporale, M.; Bajetta, E.; Floriani, I. Impact on survival of timing and duration of adjuvant chemotherapy in radically resected gastric cancer. Tumori 2016, 102, e15–e19. [Google Scholar] [CrossRef]
- Fujitani, K.; Kurokawa, Y.; Takeno, A.; Endoh, S.; Ohmori, T.; Fujita, J.; Yamasaki, M.; Takiguchi, S.; Mori, M.; Doki, Y.; et al. Time to initiation or duration of S-1 adjuvant chemotherapy; which really impacts on survival in stage II and III gastric cancer? Gastric Cancer 2018, 21, 446–452. [Google Scholar] [CrossRef]
- Greenleaf, E.K.; Kulaylat, A.N.; Hollenbeak, C.S.; Almhanna, K.; Wong, J. Timing of Adjuvant Chemotherapy and Impact on Survival for Resected Gastric Cancer. Ann. Surg. Oncol. 2016, 23, 4203–4213. [Google Scholar] [CrossRef]
- Park, H.S.; Jung, M.; Kim, H.S.; Kim, H.I.; An, J.Y.; Cheong, J.H.; Hyung, W.J.; Noh, S.H.; Kim, Y.I.; Chung, H.C.; et al. Proper timing of adjuvant chemotherapy affects survival in patients with stage 2 and 3 gastric cancer. Ann. Surg. Oncol. 2015, 22, 224–231. [Google Scholar] [CrossRef]
- Qu, J.L.; Qu, X.J.; Li, X.; Zhang, J.D.; Teng, Y.E.; Jin, B.; Zhao, M.F.; Yu, P.; Liu, J.; Li, D.Y.; et al. Early initiation of fluorouracil-based adjuvant chemotherapy improves survival in patients with resectable gastric cancer. J. BUON 2015, 20, 800–807. [Google Scholar]
- Yamamoto, M.; Sakaguchi, Y.; Kinjo, N.; Yamaguchi, S.; Egashira, A.; Minami, K.; Ikeda, Y.; Morita, M.; Toh, Y.; Okamura, T. S-1 Adjuvant Chemotherapy Earlier After Surgery Clinically Correlates with Prognostic Factors for Advanced Gastric Cancer. Ann. Surg. Oncol. 2016, 23, 546–551. [Google Scholar] [CrossRef]
- Kim, H.W.; Lee, J.C.; Lee, J.; Kim, J.W.; Kim, J.; Hwang, J.H. Early versus delayed initiation of adjuvant treatment for pancreatic cancer. PLoS ONE 2017, 12, e0173960. [Google Scholar] [CrossRef]
- Lee, W.; Yoon, Y.S.; Han, H.S.; Jang, J.Y.; Cho, J.Y.; Jung, W.; Kwon, W.; Choi, Y.; Kim, S.W. Prognostic Relevance of the Timing of Initiating and the Completion of Adjuvant Therapy in Patients with Resected Pancreatic Ductal Adenocarcinoma. World J. Surg. 2017, 41, 562–573. [Google Scholar] [CrossRef]
- Patel, A.A.; Nagarajan, S.; Scher, E.D.; Schonewolf, C.A.; Balasubramanian, S.; Poplin, E.; Moss, R.; August, D.; Carpizo, D.; Melstrom, L.; et al. Early vs. Late Chemoradiation Therapy and the Postoperative Interval to Adjuvant Therapy Do Not Correspond to Local Recurrence in Resected Pancreatic Cancer. Pancreat. Disord. Ther. 2015, 5. [Google Scholar] [CrossRef]
- Saeed, H.; Hnoosh, D.; Huang, B.; Durbin, E.B.; McGrath, P.C.; Desimone, P.; Maynard, E.; Anthony, L.B.; Dineen, S.P.; Hosein, P.J.; et al. Defining the optimal timing of adjuvant therapy for resected pancreatic adenocarcinoma: A statewide cancer registry analysis. J. Surg. Oncol. 2016, 114, 451–455. [Google Scholar] [CrossRef]
- Valle, J.W.; Palmer, D.; Jackson, R.; Cox, T.; Neoptolemos, J.P.; Ghaneh, P.; Rawcliffe, C.L.; Bassi, C.; Stocken, D.D.; Cunningham, D.; et al. Optimal duration and timing of adjuvant chemotherapy after definitive surgery for ductal adenocarcinoma of the pancreas: Ongoing lessons from the ESPAC-3 study. J. Clin. Oncol. 2014, 32, 504–512. [Google Scholar] [CrossRef]
- Yabusaki, N.; Fujii, T.; Yamada, S.; Murotani, K.; Sugimoto, H.; Kanda, M.; Nakayama, G.; Koike, M.; Fujiwara, M.; Kodera, Y. The significance of relative dose intensity in adjuvant chemotherapy of pancreatic ductal adenocarcinoma-including the analysis of clinicopathological factors influencing relative dose intensity. Medicine (Baltimore) 2016, 95, e4282. [Google Scholar] [CrossRef] [PubMed]
- Colleoni, M.; Bonetti, M.; Coates, A.S.; Castiglione-Gertsch, M.; Gelber, R.D.; Price, K.; Rudenstam, C.M.; Lindtner, J.; Collins, J.; Thurlimann, B.; et al. Early start of adjuvant chemotherapy may improve treatment outcome for premenopausal breast cancer patients with tumors not expressing estrogen receptors. The International Breast Cancer Study Group. J. Clin. Oncol. 2000, 18, 584–590. [Google Scholar] [CrossRef] [PubMed]
- Turner, M.C.; Farrow, N.E.; Rhodin, K.E.; Sun, Z.; Adam, M.A.; Mantyh, C.R.; Migaly, J. Delay in Adjuvant Chemotherapy and Survival Advantage in Stage III Colon Cancer. J. Am. Coll. Surg. 2018, 226, 670–678. [Google Scholar] [CrossRef]
- Biagi, J.J.; Raphael, M.J.; Mackillop, W.J.; Kong, W.; King, W.D.; Booth, C.M. Association between time to initiation of adjuvant chemotherapy and survival in colorectal cancer: A systematic review and meta-analysis. JAMA 2011, 305, 2335–2342. [Google Scholar] [CrossRef] [PubMed]
- Des Guetz, G.; Nicolas, P.; Perret, G.Y.; Morere, J.F.; Uzzan, B. Does delaying adjuvant chemotherapy after curative surgery for colorectal cancer impair survival? A meta-analysis. Eur. J. Cancer 2010, 46, 1049–1055. [Google Scholar] [CrossRef]
- Chavez-MacGregor, M.; Clarke, C.A.; Lichtensztajn, D.Y.; Giordano, S.H. Delayed Initiation of Adjuvant Chemotherapy Among Patients With Breast Cancer. JAMA Oncol. 2016, 2, 322–329. [Google Scholar] [CrossRef]
- Salazar, M.C.; Rosen, J.E.; Wang, Z.; Arnold, B.N.; Thomas, D.C.; Herbst, R.S.; Kim, A.W.; Detterbeck, F.C.; Blasberg, J.D.; Boffa, D.J. Association of Delayed Adjuvant Chemotherapy With Survival After Lung Cancer Surgery. JAMA Oncol. 2017, 3, 610–619. [Google Scholar] [CrossRef]
- Gunduz, N.; Fisher, B.; Saffer, E.A. Effect of surgical removal on the growth and kinetics of residual tumour. Cancer Res. 1979, 39, 3861–3865. [Google Scholar]
- Eggermont, A.M.; Steller, E.P.; Sugarbaker, P.H. Laparotomy enhances intraperitoneal tumour growth and abrogates the antitumor effects of interleukin-2 and lymphokine-activated killer cells. Surgery 1987, 102, 71–78. [Google Scholar]
- Ono, I.; Gunji, H.; Suda, K.; Iwatsuki, K.; Kaneko, F. Evaluation of cytokines in donor site wound fluids. Scand. J. Plast. Reconstr. Surg. Hand Surg. 1994, 28, 269–273. [Google Scholar] [CrossRef]
- Frindel, E.; Malaise, E.P.; Alpen, E.; Tubiana, M. Kinetics of cell proliferation of an experimental tumour. Cancer Res. 1967, 27, 1122–1131. [Google Scholar]
- Goldie, J.H.; Coldman, A.J. A mathematic model for relating the drug sensitivity of tumors to their spontaneous mutation rate. Cancer Treat. Rep. 1979, 63, 1727–1733. [Google Scholar]
- Vinuela, E.F.; Gonen, M.; Brennan, M.F.; Coit, D.G.; Strong, V.E. Laparoscopic versus open distal gastrectomy for gastric cancer: A meta-analysis of randomized controlled trials and high-quality nonrandomized studies. Ann. Surg. 2012, 255, 446–456. [Google Scholar] [CrossRef]
- Mirkin, K.A.; Greenleaf, E.K.; Hollenbeak, C.S.; Wong, J. Time to the initiation of adjuvant chemotherapy does not impact survival in patients with resected pancreatic cancer. Cancer 2016, 122, 2979–2987. [Google Scholar] [CrossRef]
- Xia, B.T.; Ahmad, S.A.; Al Humaidi, A.H.; Hanseman, D.J.; Ethun, C.G.; Maithel, S.K.; Kooby, D.A.; Salem, A.; Cho, C.S.; Weber, S.M.; et al. Time to Initiation of Adjuvant Chemotherapy in Pancreas Cancer: A Multi-Institutional Experience. Ann. Surg. Oncol. 2017, 24, 2770–2776. [Google Scholar] [CrossRef] [PubMed]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gotzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: Explanation and elaboration. BMJ 2009, 339, b2700. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author/ Year | N° pts | Type of Study | Median Follow up (months) | Country | Stage (%) | Comparison (weeks) | Type of Analysis | NOS Scale |
|---|---|---|---|---|---|---|---|---|
| Ahmed/ 2010 [4] | 663 | Retro | 54.6 | Canada | II–III (100) | < vs > 8 | Multi | 8 |
| Bayraktar/ 2011 [5] | 186 | Retro | 42.9 | US | II–III (100) | < vs > 8 | Multi | 8 |
| Becerra/ 2017 [6] | 1133 | Retro | NR | US | III (100) | < vs > 8 | Multi | 6 |
| Berglund/ 2008 [13] | 213 | Phase III | NR | Sweden | III (100) | < vs > 8 | Multi | NA |
| Bos/2015 [7] | 6620 | Retro | 60 | Netherlands | III (100) | < vs > 8 | Multi | 8 |
| Chau/2005 [14] | 801 | Phase III | 63.6 | UK | II–III (100) | < vs 8–12 | Multi | NA |
| Czaykowski/ 2011 [9] | 345 | Retro | 69.8 | Canada | III (100) | < vs > 8 | Multi | 8 |
| Cheung/ 2009 [8] | 6059 | Retro | NR | Canada | II–III (100) | < vs > 8 | Uni | 6 |
| Day/2014 [10] | 209 | Retro | 30 | UK | I–II (33), III (67) | < vs > 8 | Multi | 7 |
| Dos Santos/ 2013 [11] | 1318 | Retro | 41 | Brazil | II–III (100) | < vs > 8 | Multi | 8 |
| Gao/2018 [15] | 9722 | Retro | NR | US | III (100) | 5–8 vs > 8 | Multi | 6 |
| Hershman/ 2006 [16] | 4382 | Retro | NR | US | III (100) | < vs > 2–3 months | Multi | 6 |
| Kang/2013 [17] | 159 | Retro | 41.5 | Korea | III (100) | < vs 5–6 | Multi | 7 |
| Kim/2017 [18] | 5355 | Retro | 42.2 | Korea | II–III (100) | < vs > 8 | Multi | 7 |
| Klein/2015 [19] | 1827 | Retro | NR | Denmark | III (100) | 4–8 vs > 8 | Multi | 6 |
| Lima/2011 [20] | 1053 | Retro | NR | Canada | III (100) | < vs > 8 | Multi | 6 |
| Massarweh/ 2015 [12] | 51,331 | Retro | NR | US | III (100) | 8 vs 8–16 | Multi | 6 |
| Nachiappan/ 2015 [21] | 30,836 | Retro | 1–184* | UK | NR | < vs 8–16 | Multi | 7 |
| Peixoto/ 2015 [22] | 635 | Retro | 57.9 | Canada | III (100) | < vs > 8 | Multi | 8 |
| Sun/2016 [23] | 7794 | Retro | 61 | US | II–III (100) | < vs > 44 days | Multi | 8 |
| Tsai/2013 [24] | 1054 | Retro | 72.5 | Taiwan | III (100) | < vs ≥ 6 | Multi | 8 |
| Zeig-Owens/ 2009 [25] | 3006 | Retro | ≥48 | US | II–III (100) | < vs > 45 days | Multi | 8 |
| Author/Year | N° pts | Type of Study | Median Follow up (months) | Country | Stage (%) | Comparison (weeks) | Type of Analysis | NOS Scale |
|---|---|---|---|---|---|---|---|---|
| Di Bartolomeo/ 2016 [26] | 1072 | Retro | 56.9 | Italy | Ib (8.2); II (31.8) III (41.6); IV (18.4) | < vs > 8 | Multi | 8 |
| Fujitani/ 2017 [27] | 498 | Retro | NR | Japan | II (36.1); III (63.9) | < vs > 6 | Multi | 6 |
| Greenleaf/ 2016 [28] | 2332 | Retro | NR | US | I (11); II (30); III (50) | 8 vs > 8 | Multi | 6 |
| Park/ 2015 [29] | 840 | Retro | 34 | Korea | II (28.6); III (71.4) | 4–8 vs 8 | Multi | 7 |
| Qu/ 2015 [30] | 266 | Retro | 28 | China | IB (4.1); II (28.2) III (67.7) | < vs > 6.4 | Multi | 6 |
| Yamamoto/ 2016 [31] | 113 | Retro | 47.6 | Japan | II (34.5); III (65.5) | < vs > 6 | Multi | 7 |
| Author/Year | N° pts | Type of Study | Median Follow up (months) | Country | Stage (%) | Comparison (weeks) | Type of Analysis | NOS Scale |
|---|---|---|---|---|---|---|---|---|
| Kim/2017 [32] | 113 | Retro | 20.3 | Korea | - | < 6 vs > 6 | Multi | 6 |
| Lee/2017 [33] | 311 | Retro | 28 | Korea | I (4.1); II 94.2; III 1.6 | < 6 vs > 6 | Multi | 7 |
| Patel/2015 [34] | 34 | Retro | 22 | US | N0 38; N+ 62 | < 8 vs > 12 | Uni | 6 |
| Saeed/2016 [35] | 420 | Retro | 19.3 | US | I (8.5); II (87.1); III 4.2 | < 8 vs > 8 | Multi | 7 |
| Valle/2014 [36] | 985 | Phase III | 58.7 | Europe | I (10); II 29; III 58; IVa 4 | < 8 vs > 8 | Multi | 8 |
| Yabusaki/2016 [37] | 168 | Prosp | 24.5 | Japan | I–III (100) | < 8 vs > 8 | Multi | 7 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Petrelli, F.; Zaniboni, A.; Ghidini, A.; Ghidini, M.; Turati, L.; Pizzo, C.; Ratti, M.; Libertini, M.; Tomasello, G. Timing of Adjuvant Chemotherapy and Survival in Colorectal, Gastric, and Pancreatic Cancer. A Systematic Review and Meta-Analysis. Cancers 2019, 11, 550. https://doi.org/10.3390/cancers11040550
Petrelli F, Zaniboni A, Ghidini A, Ghidini M, Turati L, Pizzo C, Ratti M, Libertini M, Tomasello G. Timing of Adjuvant Chemotherapy and Survival in Colorectal, Gastric, and Pancreatic Cancer. A Systematic Review and Meta-Analysis. Cancers. 2019; 11(4):550. https://doi.org/10.3390/cancers11040550
Chicago/Turabian StylePetrelli, Fausto, Alberto Zaniboni, Antonio Ghidini, Michele Ghidini, Luca Turati, Claudio Pizzo, Margherita Ratti, Michela Libertini, and Gianluca Tomasello. 2019. "Timing of Adjuvant Chemotherapy and Survival in Colorectal, Gastric, and Pancreatic Cancer. A Systematic Review and Meta-Analysis" Cancers 11, no. 4: 550. https://doi.org/10.3390/cancers11040550