Extracapsular Lymph Node Involvement in Ovarian Carcinoma

 , and
, and
Abstract
:1. Introduction
2. Results
2.1. Study Cohort
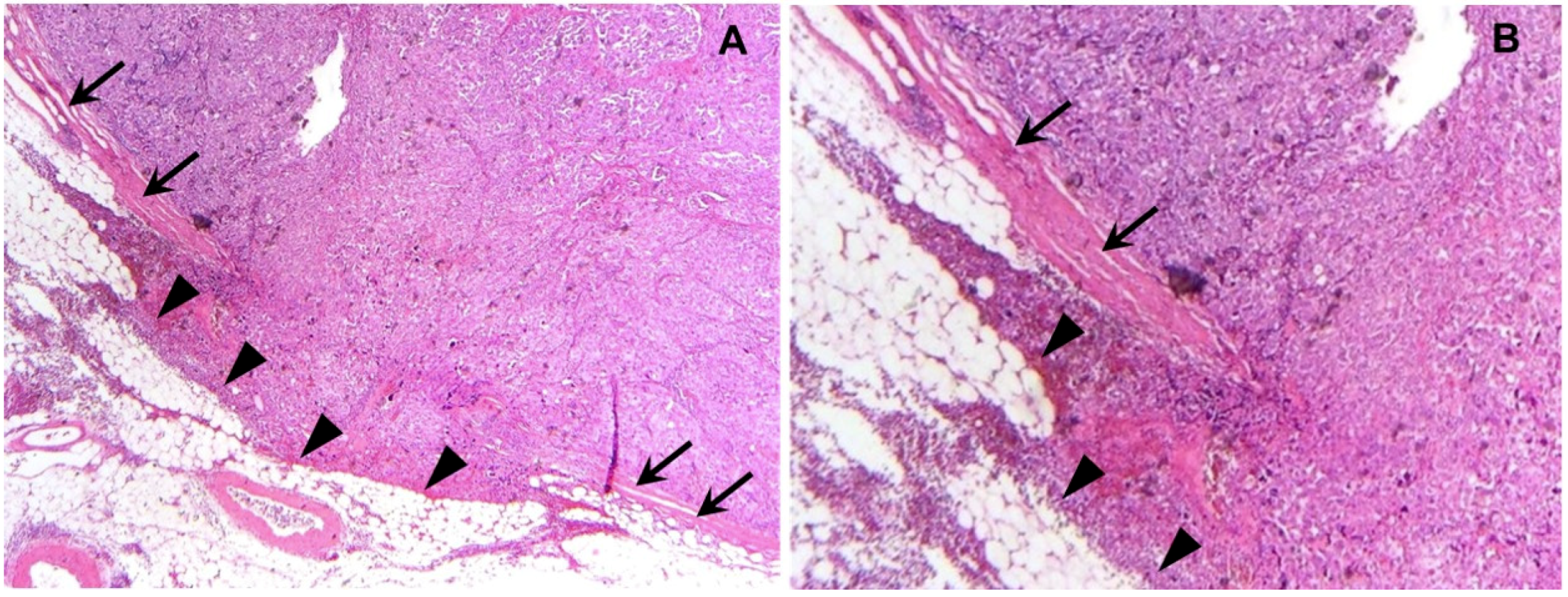
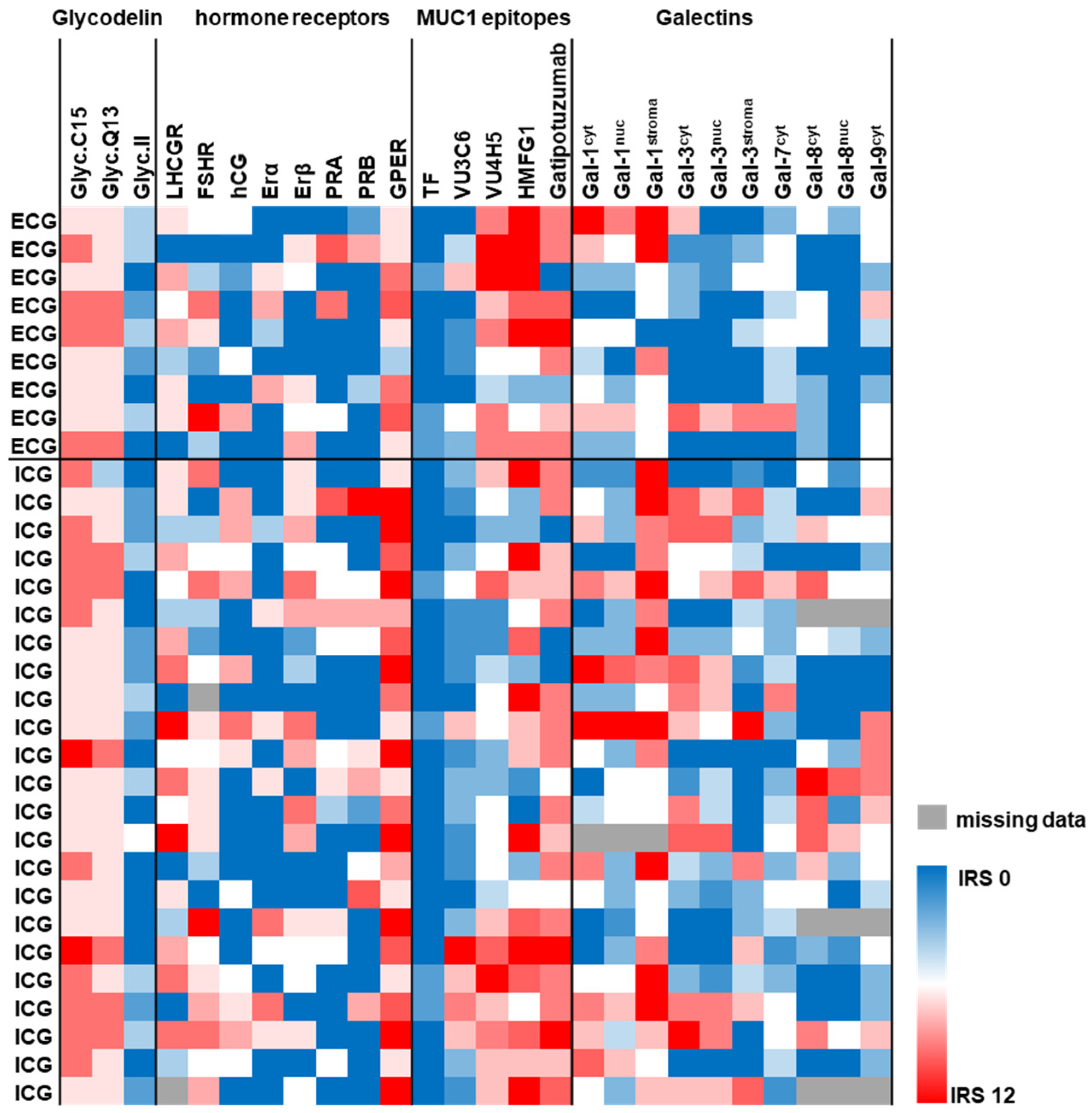
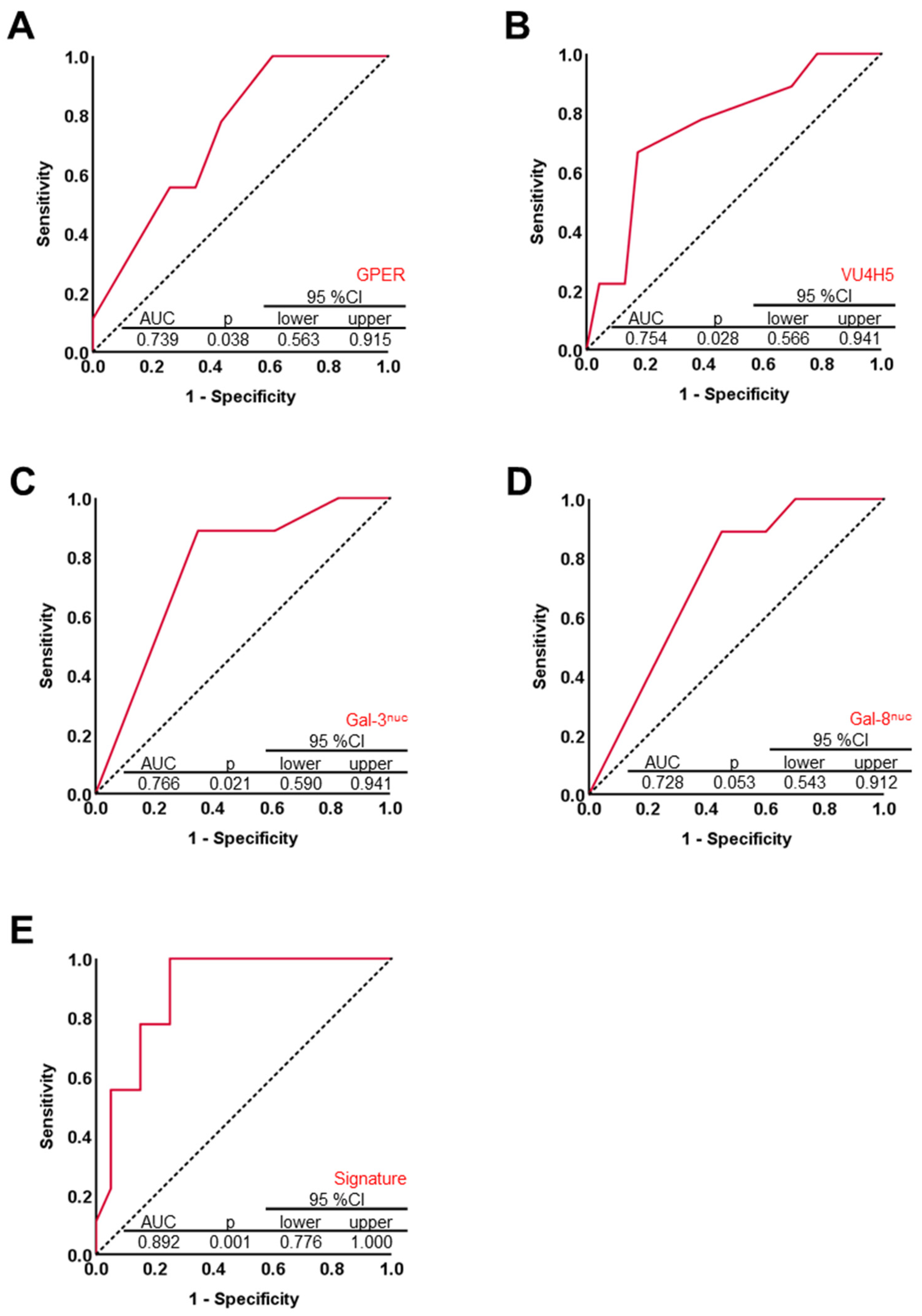
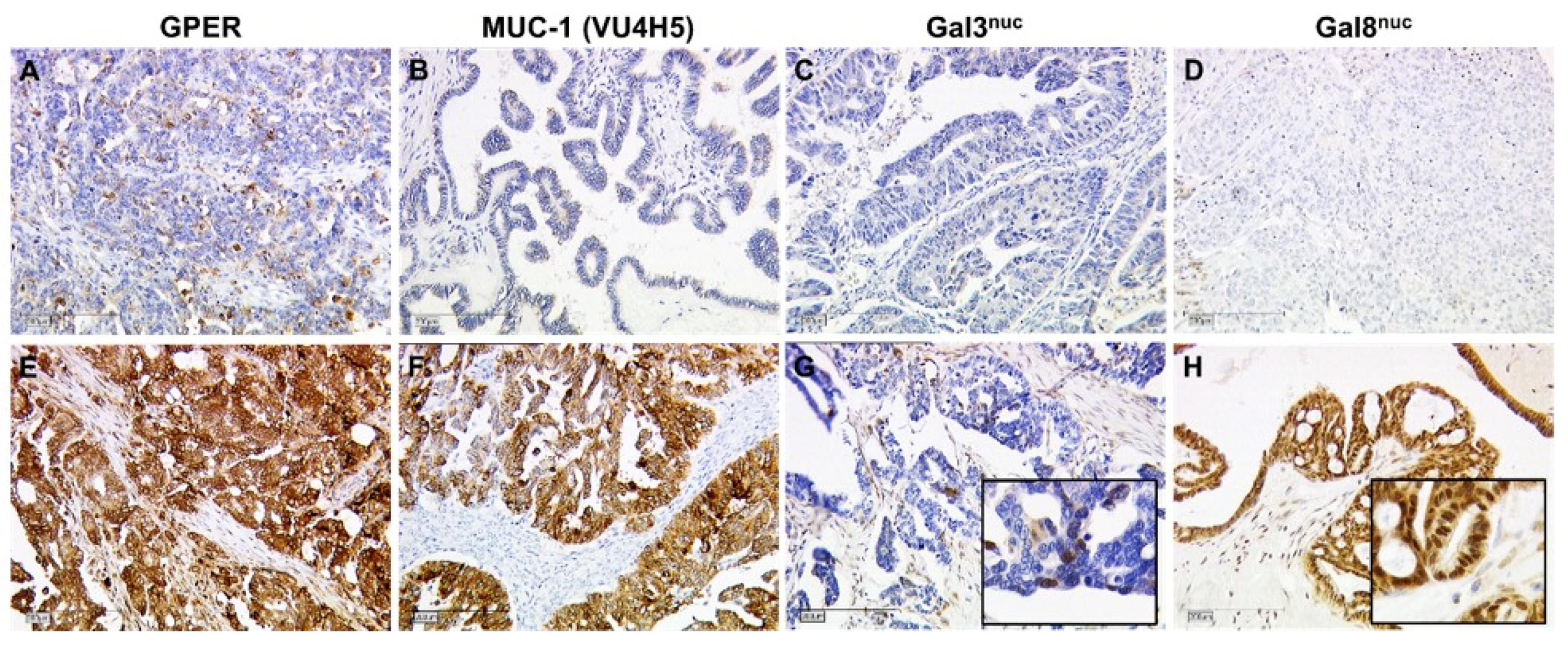
2.2. Histological Pattern of Lymph Node Involvement Is Associated with the Biomarker Profile of the Primary Tumor
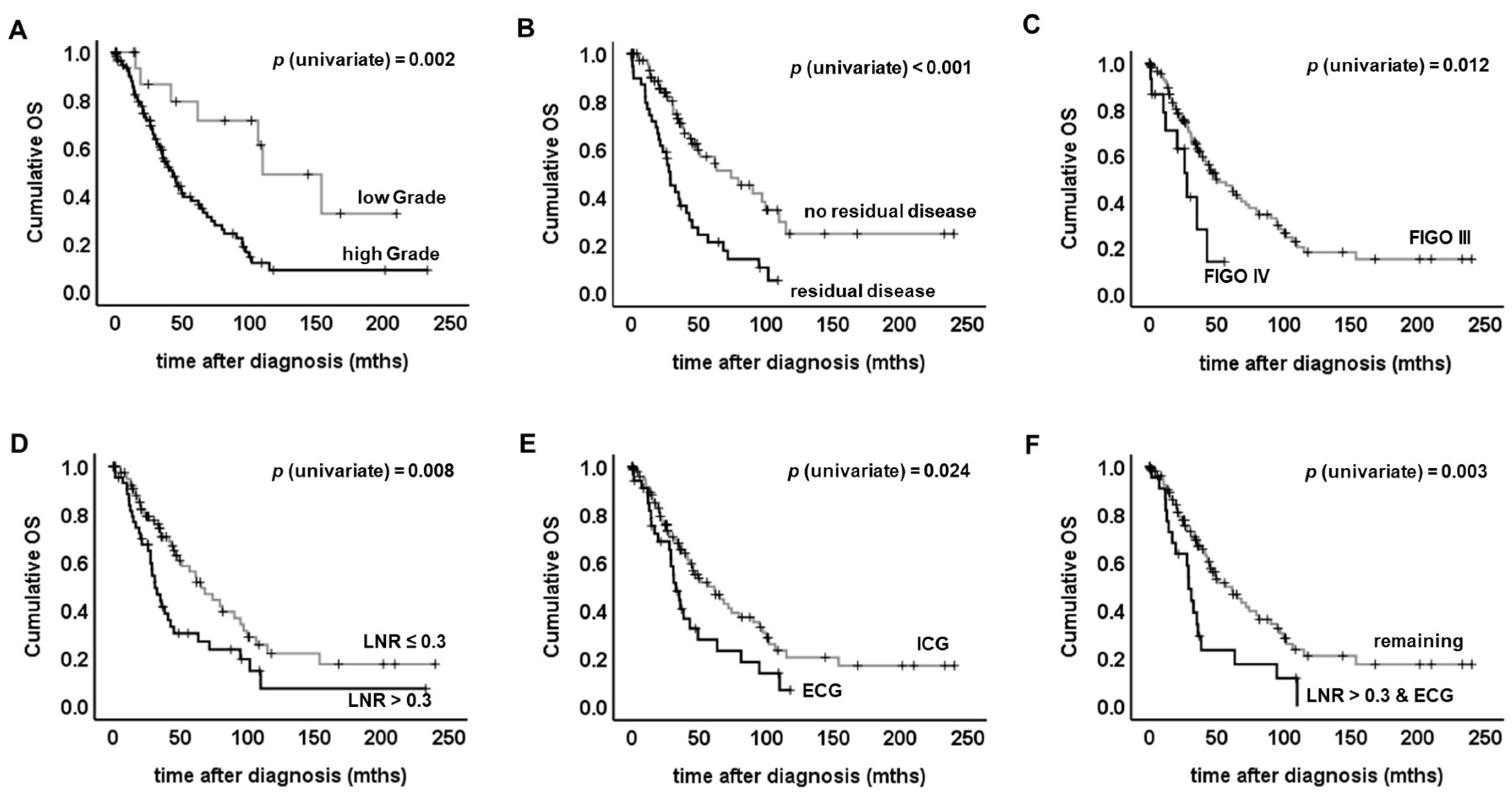
2.3. Evaluation of ECG as a Potential Prognostic Factor for Overall Survival
3. Discussion
4. Materials and Methods
4.1. Patients
4.2. Ethical Approval
4.3. Assay Methods
4.3.1. Determination of ECG and ICG
4.3.2. Immunohistochemistry
4.3.3. Statistical Analysis Methods
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Alakus, H.; Holscher, A.H.; Grass, G.; Hartmann, E.; Schulte, C.; Drebber, U.; Baldus, S.E.; Bollschweiler, E.; Metzger, R.; Monig, S.P. Extracapsular lymph node spread: A new prognostic factor in gastric cancer. Cancer 2010, 116, 309–315. [Google Scholar] [CrossRef] [PubMed]
- van der Velden, J.; van Lindert, A.C.; Lammes, F.B.; ten Kate, F.J.; Sie-Go, D.M.; Oosting, H.; Heintz, A.P. Extracapsular growth of lymph node metastases in squamous cell carcinoma of the vulva. The impact on recurrence and survival. Cancer 1995, 75, 2885–2890. [Google Scholar] [CrossRef]
- Chan, Y.W.; Lee, V.H.; Chow, V.L.; To, V.S.; Wei, W.I. Extracapsular lymph node spread in recurrent nasopharyngeal carcinoma. Laryngoscope 2011, 121, 2576–2580. [Google Scholar] [CrossRef] [PubMed]
- Fujii, T.; Yanagita, Y.; Fujisawa, T.; Hirakata, T.; Iijima, M.; Kuwano, H. Implication of extracapsular invasion of sentinel lymph nodes in breast cancer: Prediction of nonsentinel lymph node metastasis. World J. Surg. 2010, 34, 544–548. [Google Scholar] [CrossRef] [PubMed]
- Horn, L.C.; Hentschel, B.; Galle, D.; Bilek, K. Extracapsular extension of pelvic lymph node metastases is of prognostic value in carcinoma of the cervix uteri. Gynecol. Oncol. 2008, 108, 63–67. [Google Scholar] [CrossRef] [PubMed]
- Metindir, J.; Bilir Dilek, G. Evaluation of prognostic significance in extracapsular spread of pelvic lymph node metastasis in patients with cervical cancer. Eur. J. Gynaecol. Oncol. 2008, 29, 476–478. [Google Scholar]
- Luchini, C.; Nottegar, A.; Solmi, M.; Sergi, G.; Manzato, E.; Capelli, P.; Scarpa, A.; Veronese, N. Prognostic implications of extranodal extension in node-positive squamous cell carcinoma of the vulva: A systematic review and meta-analysis. Surg. Oncol. 2016, 25, 60–65. [Google Scholar] [CrossRef]
- Heublein, S.; Page, S.K.; Mayr, D.; Ditsch, N.; Jeschke, U. p53 determines prognostic significance of the carbohydrate stem cell marker TF1 (CD176) in ovarian cancer. J. Cancer Res. Clin. Oncol. 2016, 142, 1163–1170. [Google Scholar] [CrossRef]
- Yemelyanova, A.; Vang, R.; Kshirsagar, M.; Lu, D.; Marks, M.A.; Shih Ie, M.; Kurman, R.J. Immunohistochemical staining patterns of p53 can serve as a surrogate marker for TP53 mutations in ovarian carcinoma: An immunohistochemical and nucleotide sequencing analysis. Mod. Pathol. Off. J. United States Can. Acad. Pathol. Inc. 2011, 24, 1248–1253. [Google Scholar] [CrossRef]
- Tu, H.; Sun, P.; Gu, H.F.; Zhang, X.K.; Huang, H.; Wan, T.; Liu, J.H. Clinical significance and prognostic value of femoral lymph node metastasis in FIGO stage III vulvar carcinoma. Eur. J. Surg. Oncol. 2017, 43, 1768–1775. [Google Scholar] [CrossRef]
- Galic, V.; Coleman, R.L.; Herzog, T.J. Unmet needs in ovarian cancer: Dividing histologic subtypes to exploit novel targets and pathways. Curr. Cancer Drug Targets 2013, 13, 698–707. [Google Scholar] [CrossRef] [PubMed]
- Engelstaedter, V.; Heublein, S.; Schumacher, A.L.; Lenhard, M.; Engelstaedter, H.; Andergassen, U.; Guenthner-Biller, M.; Kuhn, C.; Rack, B.; Kupka, M.; et al. Mucin-1 and its relation to grade, stage and survival in ovarian carcinoma patients. BMC Cancer 2012, 12, 600. [Google Scholar] [CrossRef] [PubMed]
- Heublein, S.; Mayr, D.; Vrekoussis, T.; Friese, K.; Hofmann, S.S.; Jeschke, U.; Lenhard, M. The G-protein coupled estrogen receptor (GPER/GPR30) is a gonadotropin receptor dependent positive prognosticator in ovarian carcinoma patients. PLoS ONE 2013, 8, e71791. [Google Scholar] [CrossRef]
- Schulz, H.; Kuhn, C.; Hofmann, S.; Mayr, D.; Mahner, S.; Jeschke, U.; Schmoeckel, E. Overall Survival of Ovarian Cancer Patients Is Determined by Expression of Galectins-8 and-9. Int. J. Mol. Sci. 2018, 19, 323. [Google Scholar] [CrossRef] [PubMed]
- Schulz, H.; Schmoeckel, E.; Kuhn, C.; Hofmann, S.; Mayr, D.; Mahner, S.; Jeschke, U. Galectins-1, -3, and -7 Are Prognostic Markers for Survival of Ovarian Cancer Patients. Int. J. Mol. Sci. 2017, 18, 1230. [Google Scholar] [CrossRef] [PubMed]
- du Bois, A.; Reuss, A.; Pujade-Lauraine, E.; Harter, P.; Ray-Coquard, I.; Pfisterer, J. Role of surgical outcome as prognostic factor in advanced epithelial ovarian cancer: A combined exploratory analysis of 3 prospectively randomized phase 3 multicenter trials: By the Arbeitsgemeinschaft Gynaekologische Onkologie Studiengruppe Ovarialkarzinom (AGO-OVAR) and the Groupe d’Investigateurs Nationaux Pour les Etudes des Cancers de l’Ovaire (GINECO). Cancer 2009, 115, 1234–1244. [Google Scholar] [CrossRef] [PubMed]
- Klar, M.; Hasenburg, A.; Hasanov, M.; Hilpert, F.; Meier, W.; Pfisterer, J.; Pujade-Lauraine, E.; Herrstedt, J.; Reuss, A.; du Bois, A. Prognostic factors in young ovarian cancer patients: An analysis of four prospective phase III intergroup trials of the AGO Study Group, GINECO and NSGO. Eur. J. Cancer 2016, 66, 114–124. [Google Scholar] [CrossRef] [PubMed]
- Harter, P.; Sehouli, J.; Lorusso, D.; Reuss, A.; Vergote, I.; Marth, C.; Kim, J.W.; Raspagliesi, F.; Lampe, B.; Landoni, F.; et al. LION: Lymphadenectomy in ovarian neoplasms—A prospective randomized AGO study group led gynecologic cancer intergroup trial. J. Clin. Oncol. 2017, 35, 5500. [Google Scholar] [CrossRef]
- du Bois, A.; Reuss, A.; Harter, P.; Pujade-Lauraine, E.; Ray-Coquard, I.; Pfisterer, J. Potential role of lymphadenectomy in advanced ovarian cancer: A combined exploratory analysis of three prospectively randomized phase III multicenter trials. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2010, 28, 1733–1739. [Google Scholar] [CrossRef]
- Panici, P.B.; Maggioni, A.; Hacker, N.; Landoni, F.; Ackermann, S.; Campagnutta, E.; Tamussino, K.; Winter, R.; Pellegrino, A.; Greggi, S.; et al. Systematic aortic and pelvic lymphadenectomy versus resection of bulky nodes only in optimally debulked advanced ovarian cancer: A randomized clinical trial. J. Natl. Cancer Inst. 2005, 97, 560–566. [Google Scholar] [CrossRef] [PubMed]
- Burger, R.A.; Brady, M.F.; Bookman, M.A.; Fleming, G.F.; Monk, B.J.; Huang, H.; Mannel, R.S.; Homesley, H.D.; Fowler, J.; Greer, B.E.; et al. Incorporation of bevacizumab in the primary treatment of ovarian cancer. N. Engl. J. Med. 2011, 365, 2473–2483. [Google Scholar] [CrossRef] [PubMed]
- Perren, T.J.; Swart, A.M.; Pfisterer, J.; Ledermann, J.A.; Pujade-Lauraine, E.; Kristensen, G.; Carey, M.S.; Beale, P.; Cervantes, A.; Kurzeder, C.; et al. A phase 3 trial of bevacizumab in ovarian cancer. N. Engl. J. Med. 2011, 365, 2484–2496. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.I.; Lee, M.; Kim, H.S.; Chung, H.H.; Kim, J.W.; Park, N.H.; Song, Y.S. Effect of BRCA mutational status on survival outcome in advanced-stage high-grade serous ovarian cancer. J. Ovarian Res. 2019, 12, 40. [Google Scholar] [CrossRef] [PubMed]
- Dong, S.; Wang, R.; Wang, H.; Ding, Q.; Zhou, X.; Wang, J.; Zhang, K.; Long, Y.; Lu, S.; Hong, T.; et al. HOXD-AS1 promotes the epithelial to mesenchymal transition of ovarian cancer cells by regulating miR-186-5p and PIK3R3. J. Exp. Clin. Cancer Res. 2019, 38, 110. [Google Scholar] [CrossRef] [PubMed]
- Amano, T.; Chano, T.; Isono, T.; Kimura, F.; Kushima, R.; Murakami, T. Abundance of mitochondrial superoxide dismutase is a negative predictive biomarker for endometriosis-associated ovarian cancers. World J. Surg. Oncol. 2019, 17, 24. [Google Scholar] [CrossRef] [PubMed]
- Lenhard, M.; Tsvilina, A.; Schumacher, L.; Kupka, M.; Ditsch, N.; Mayr, D.; Friese, K.; Jeschke, U. Human chorionic gonadotropin and its relation to grade, stage and patient survival in ovarian cancer. BMC Cancer 2012, 12, 2. [Google Scholar] [CrossRef] [PubMed]
- Lenhard, M.; Tereza, L.; Heublein, S.; Ditsch, N.; Himsl, I.; Mayr, D.; Friese, K.; Jeschke, U. Steroid hormone receptor expression in ovarian cancer: Progesterone receptor B as prognostic marker for patient survival. BMC Cancer 2012, 12, 553. [Google Scholar] [CrossRef] [PubMed]
- Lenhard, M.; Lennerova, T.; Ditsch, N.; Kahlert, S.; Friese, K.; Mayr, D.; Jeschke, U. Opposed roles of follicle-stimulating hormone and luteinizing hormone receptors in ovarian cancer survival. Histopathology 2011, 58, 990–994. [Google Scholar] [CrossRef]
- Dian, D.; Lenhard, M.; Mayr, D.; Heublein, S.; Karsten, U.; Goletz, S.; Kuhn, C.; Wiest, I.; Friese, K.; Weissenbacher, T.; et al. Staining of MUC1 in ovarian cancer tissues with PankoMab-GEX detecting the tumour-associated epitope, TA-MUC1, as compared to antibodies HMFG-1 and 115D8. Histol. Histopathol. 2013, 28, 239–244. [Google Scholar]
- McShane, L.M.; Altman, D.G.; Sauerbrei, W.; Taube, S.E.; Gion, M.; Clark, G.M. Reporting recommendations for tumor marker prognostic studies. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2005, 23, 9067–9072. [Google Scholar] [CrossRef]
- Youden, W.J. Index for rating diagnostic tests. Cancer 1950, 3, 32–35. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | ICG | ECG | p | |
|---|---|---|---|---|
| n or Median (Range) | n or Median (Range) | |||
| pT | pT1/2 | 12 | 6 | ns |
| pT3 | 96 | 29 | ||
| FIGO | III | 95 | 32 | ns |
| IV | 13 | 3 | ||
| Grade | low or G1 | 18 | 1 | 0.043 |
| high or G2/3 | 88 | 34 | ||
| Histology | non-serous | 6 | 8 | 0.006 |
| serous | 102 | 27 | ||
| Age | (years) | 59.62 (33.4–81.6) | 59.46 (36.9–87.6) | ns |
| Residual disease | none | 66 | 17 | ns |
| any | 27 | 14 | ||
| Total nodes resected | 38 | 37 | ns | |
| (1–94) | (6–74) | |||
| Fraction positive nodes/total nodes resected | ≤0.3 | 79 | 11 | <0.001 |
| >0.3 | 22 | 22 |
| Characteristic | Univariate Analysis | |
|---|---|---|
| Log Rank χ2 Test | p | |
| FIGO (III vs. IV) | 6.345 | 0.012 |
| pT (pT1/2 vs. pT3) | 0.743 | 0.389 |
| Grade (G1 vs. G2/3) | 9.862 | 0.002 |
| Histology (other vs. serous) | 0.425 | 0.515 |
| Patient age (<60 years vs. ≥60 years) | 2.960 | 0.085 |
| Residual disease (none vs. any) | 16.65 | <0.001 |
| Total nodes resected (<37 vs. ≥37) | 0.223 | 0.637 |
| LNR (≤0.3 vs. >0.3) | 7.059 | 0.008 |
| ECG vs. ICG | 5.101 | 0.024 |
| LNR > 0.3 and ECG vs. remaining | 8.581 | 0.003 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Heublein, S.; Schulz, H.; Marmé, F.; Angele, M.; Czogalla, B.; Burges, A.; Mahner, S.; Mayr, D.; Jeschke, U.; Schmoeckel, E. Extracapsular Lymph Node Involvement in Ovarian Carcinoma. Cancers 2019, 11, 924. https://doi.org/10.3390/cancers11070924
Heublein S, Schulz H, Marmé F, Angele M, Czogalla B, Burges A, Mahner S, Mayr D, Jeschke U, Schmoeckel E. Extracapsular Lymph Node Involvement in Ovarian Carcinoma. Cancers. 2019; 11(7):924. https://doi.org/10.3390/cancers11070924
Chicago/Turabian StyleHeublein, Sabine, Heiko Schulz, Frederik Marmé, Martin Angele, Bastian Czogalla, Alexander Burges, Sven Mahner, Doris Mayr, Udo Jeschke, and Elisa Schmoeckel. 2019. "Extracapsular Lymph Node Involvement in Ovarian Carcinoma" Cancers 11, no. 7: 924. https://doi.org/10.3390/cancers11070924