Minimal Effect of Bevacizumab Treatment on Residual Vestibular Schwannomas after Partial Resection in Young Neurofibromatosis Type 2 Patients

 ,
,
Abstract
:1. Introduction
2. Results
2.1. Patients, Tumors and Operation
2.2. Postoperative Bevacizumab and Toxicity
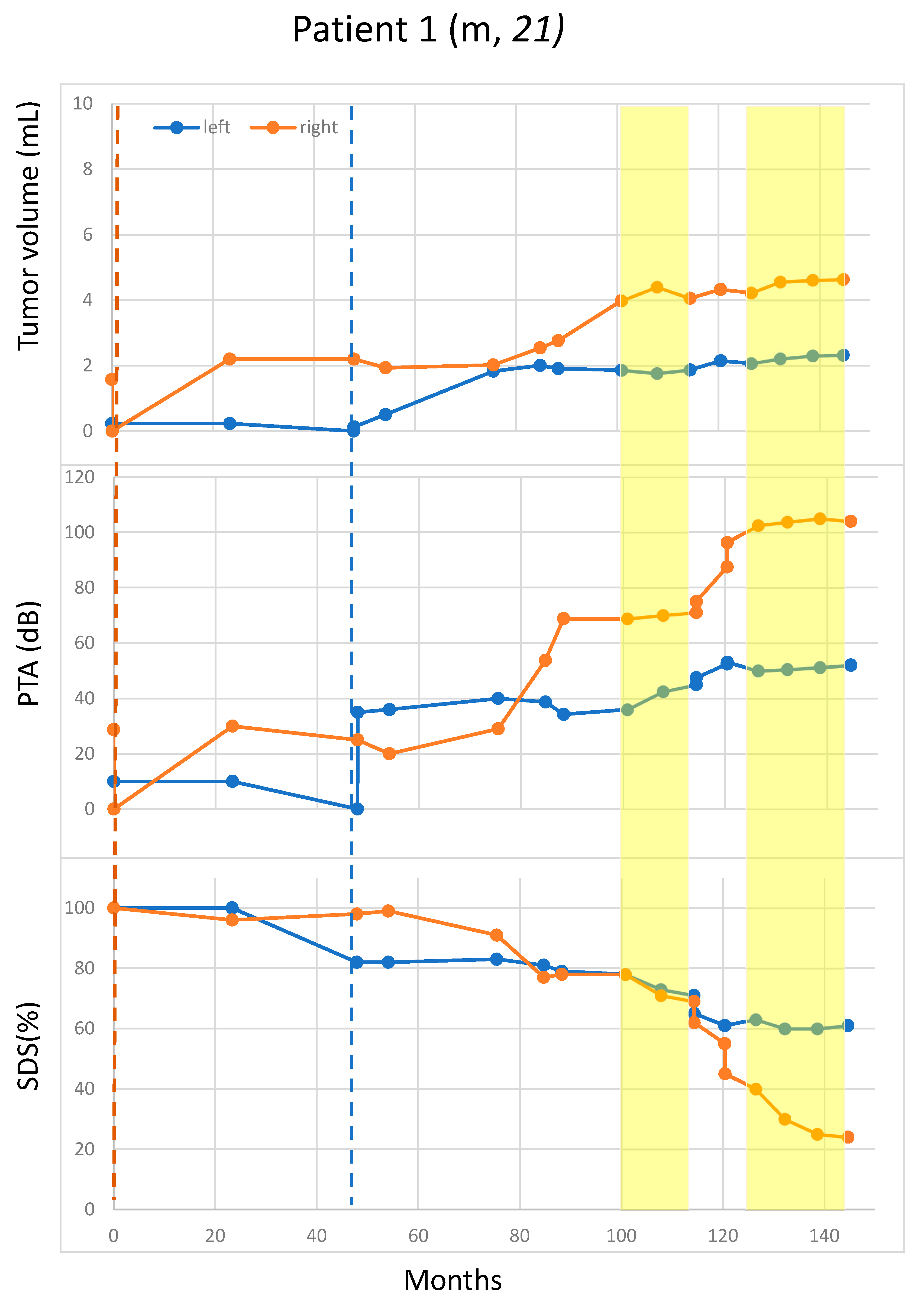
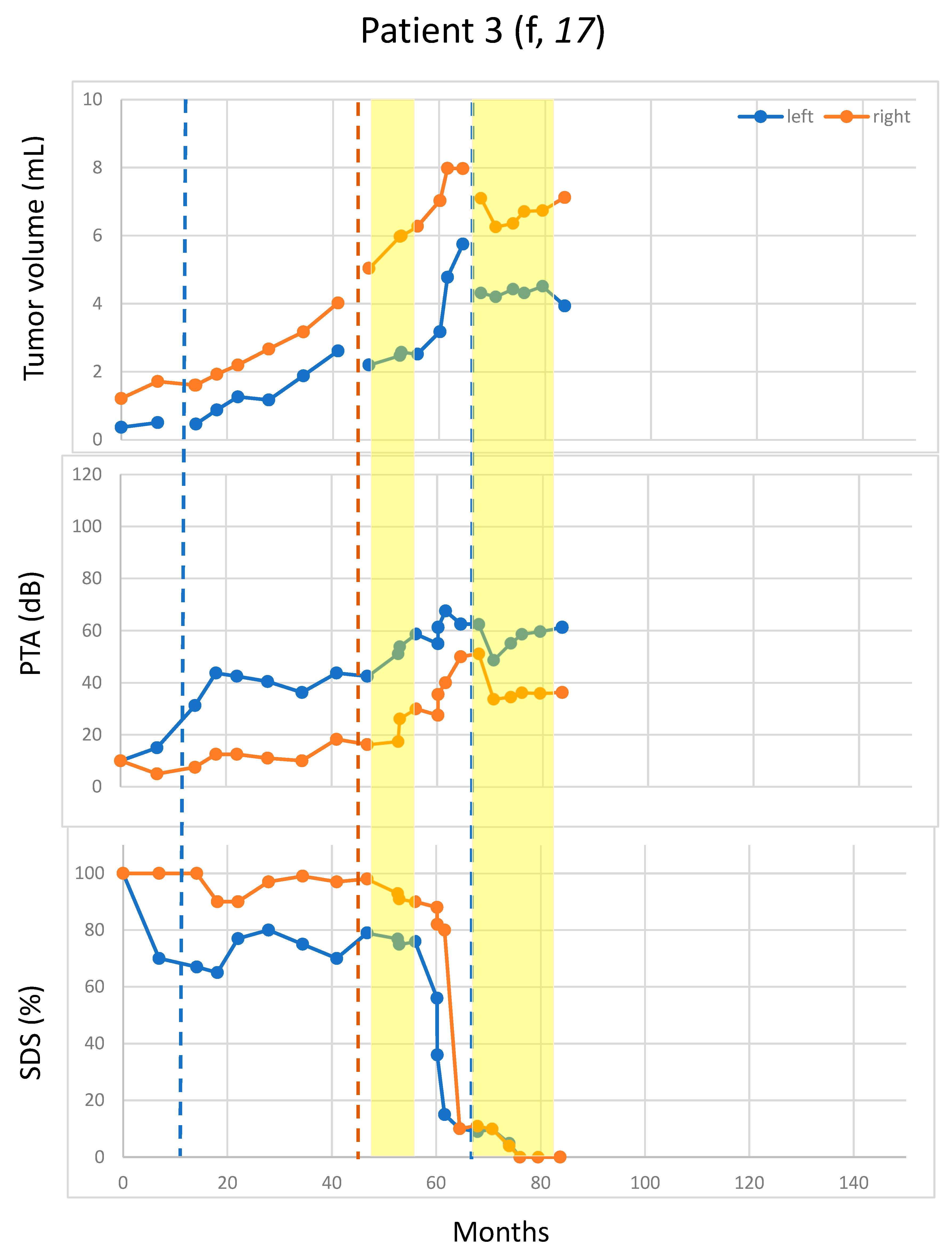
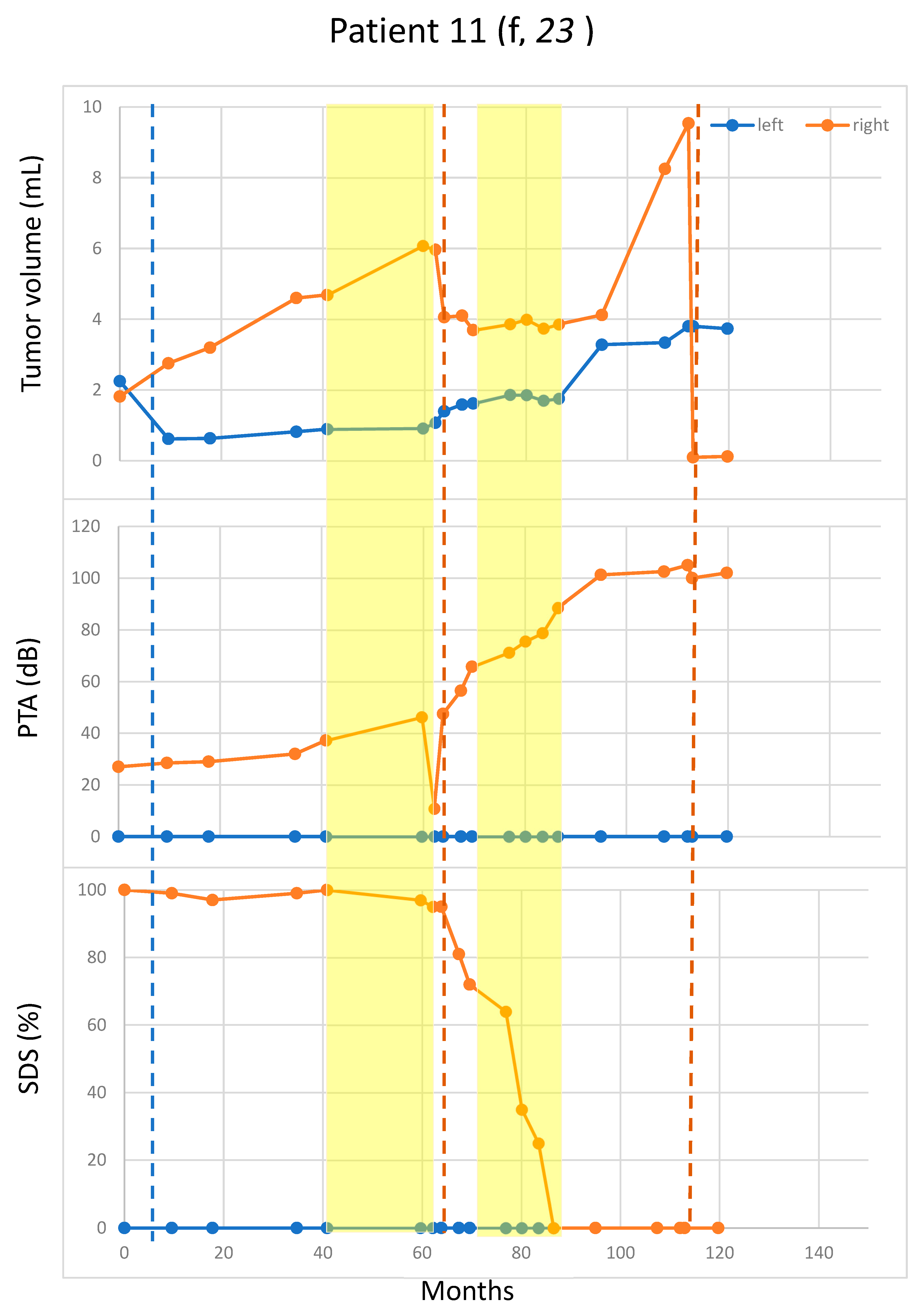
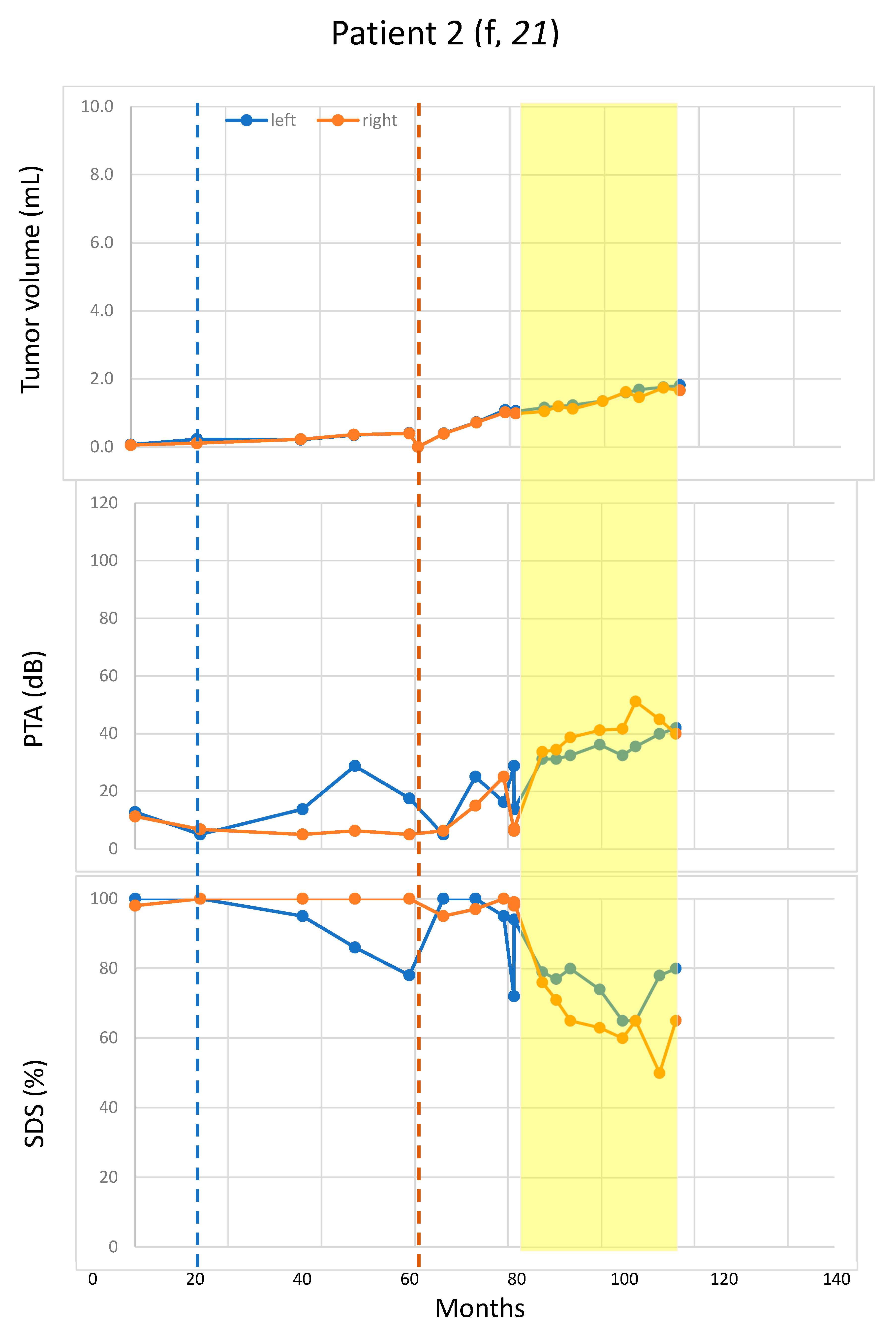
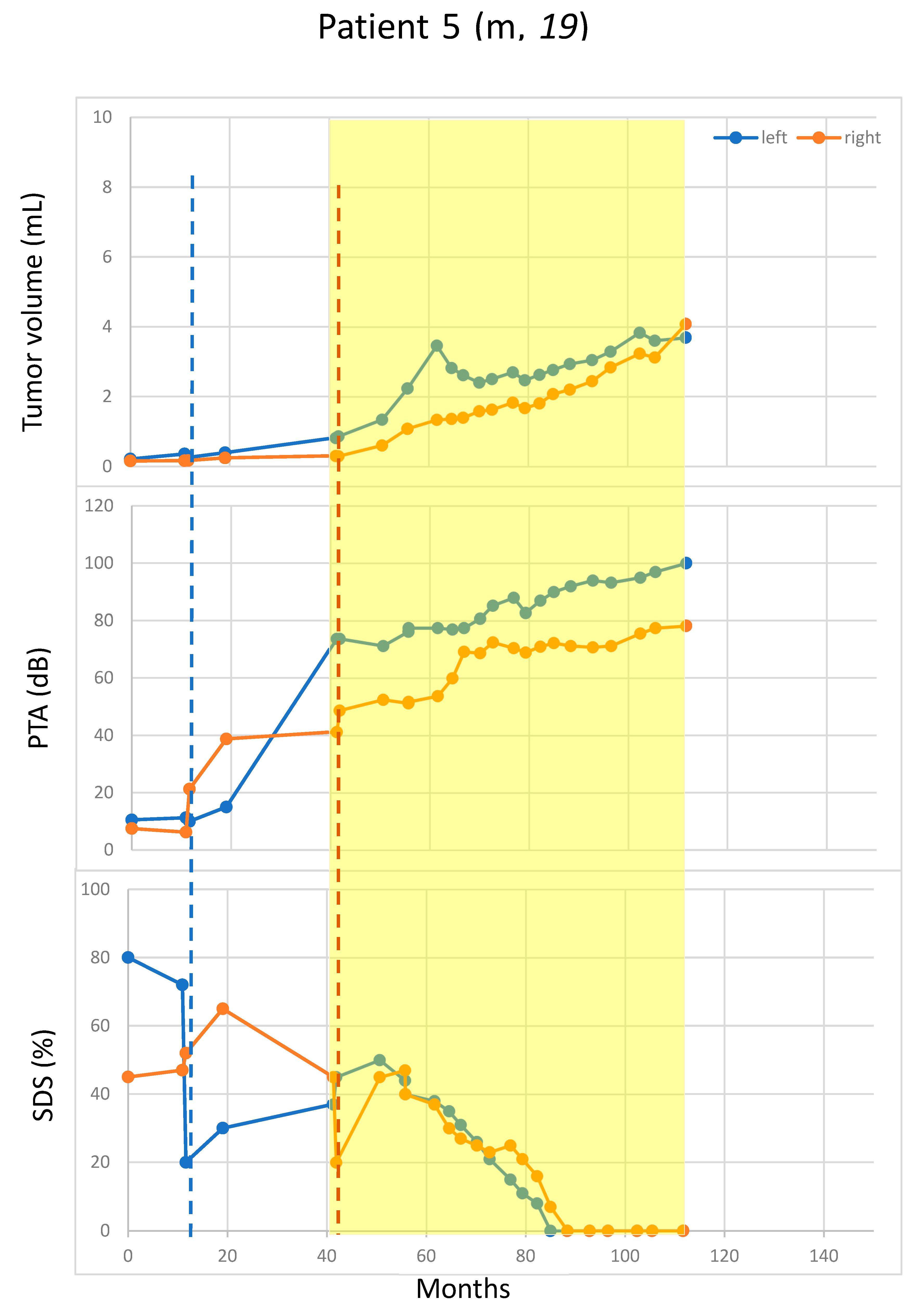
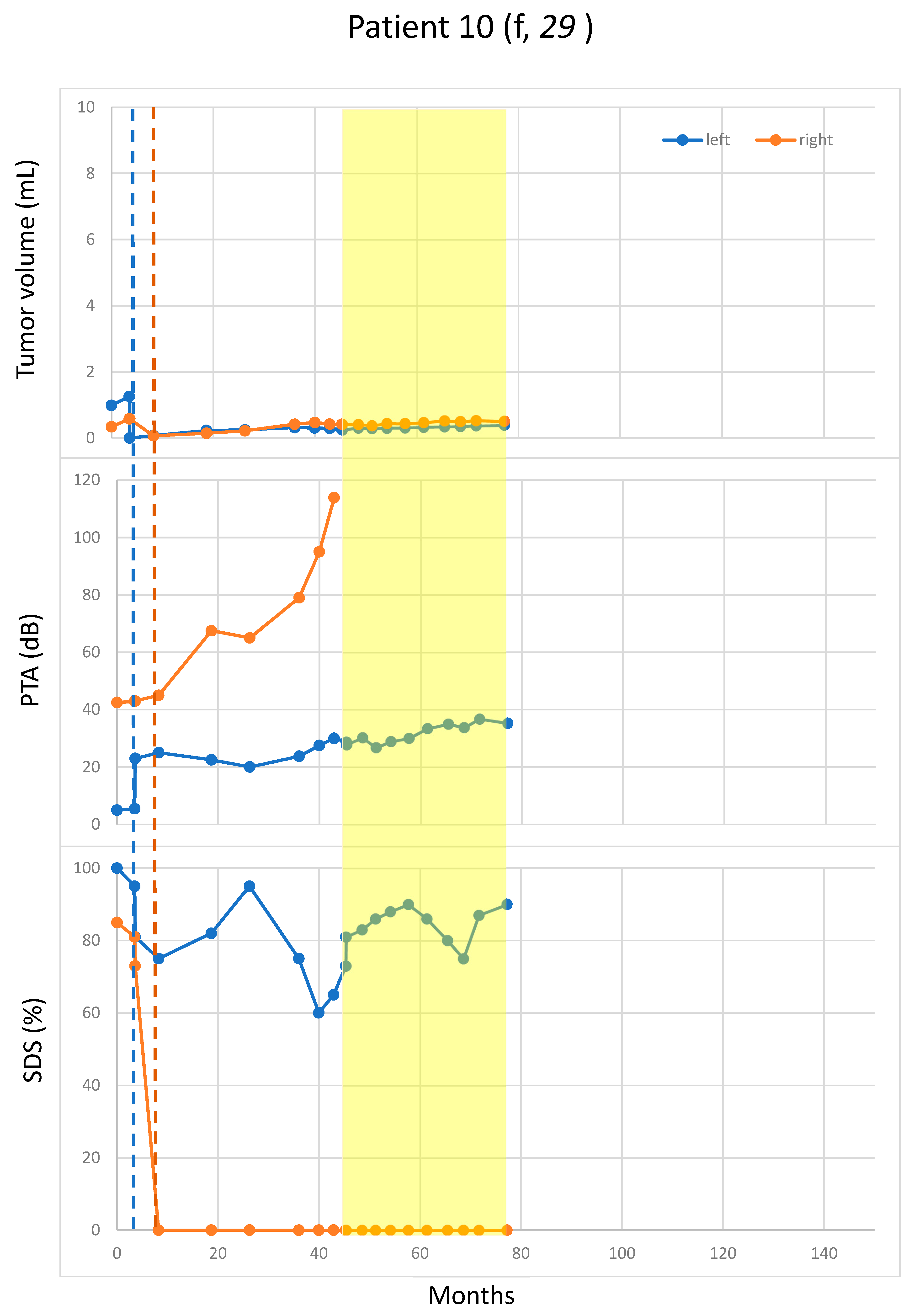
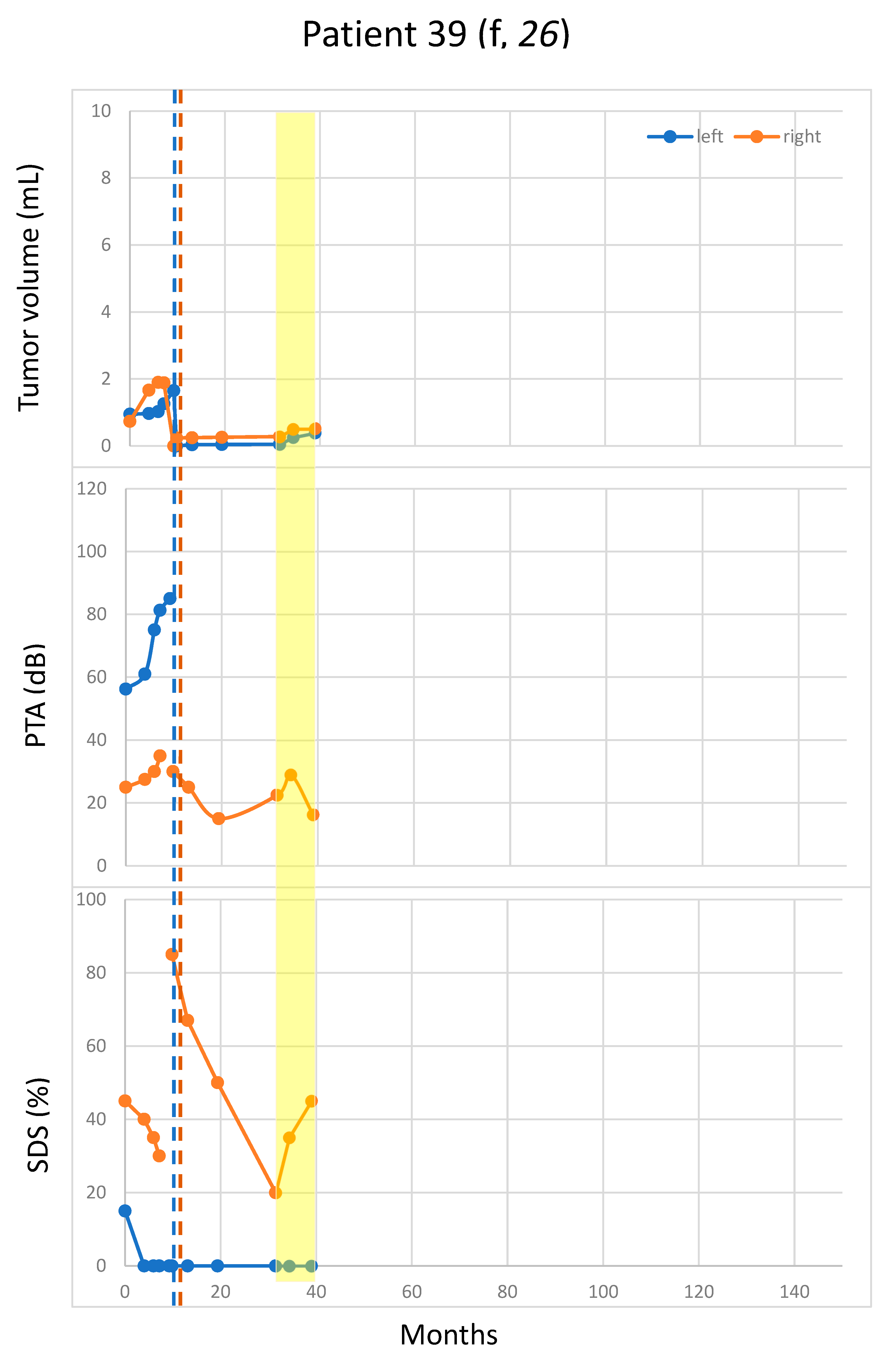
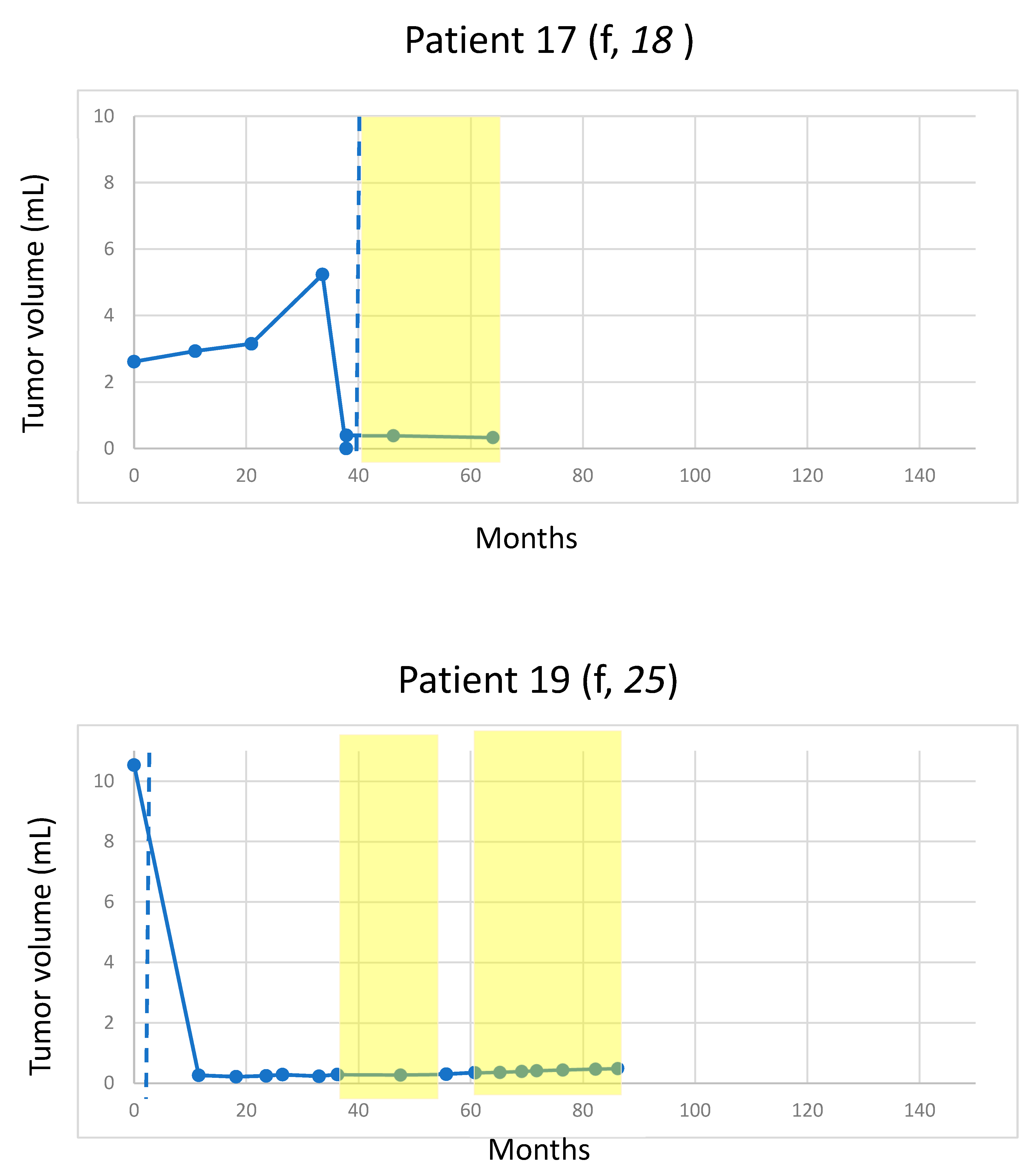
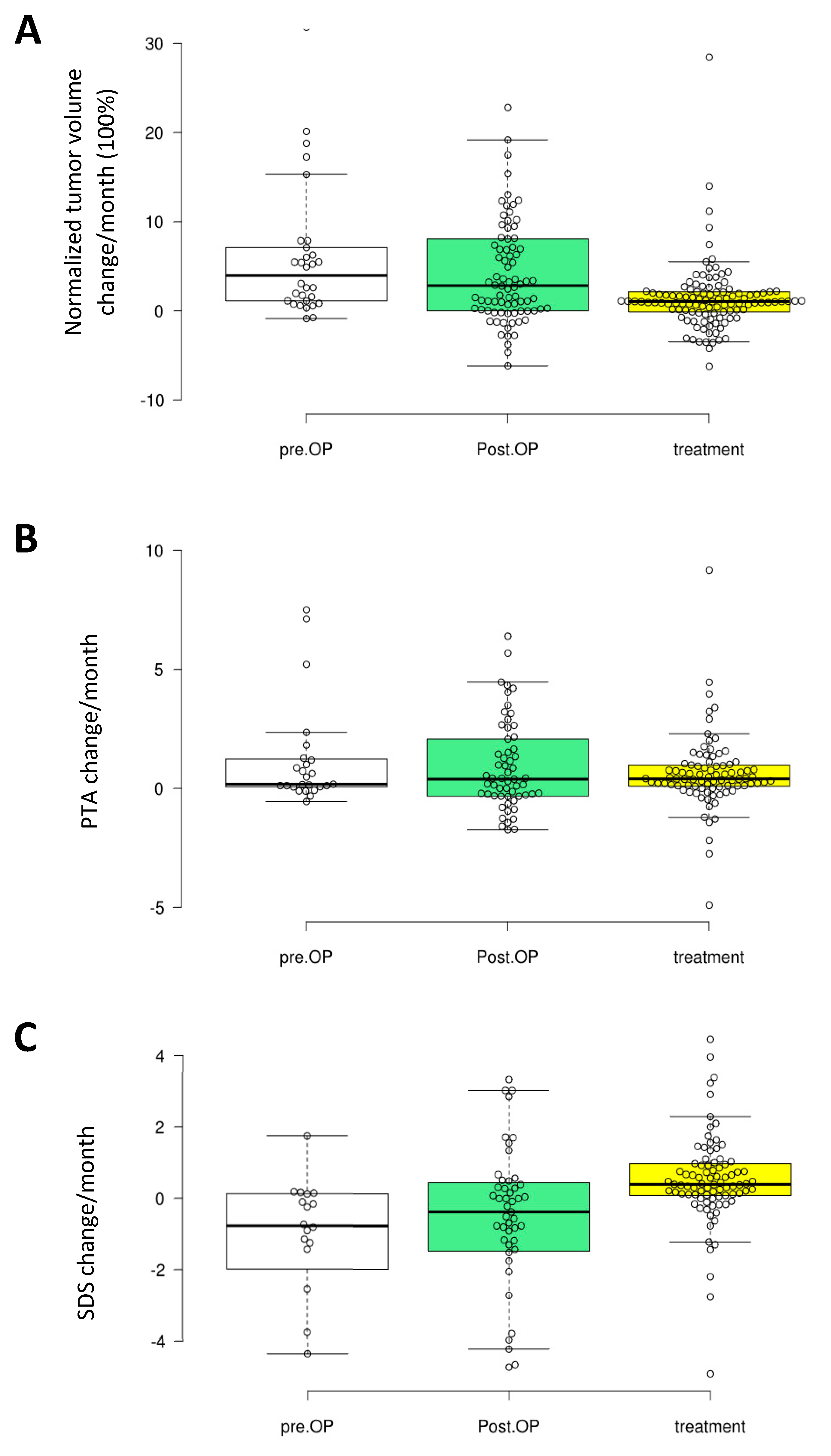
2.3. Growth of the Residual VS
2.4. Hearing
2.5. Influencing Factors on Tumor Growth Rate under Bevacizumab Treatment
3. Discussion
4. Material and Methods
4.1. Patients and Clinics
4.2. Volumetry, Growth Rate and Hearing
4.3. Data Evaluation
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Trofatter, J.A.; MacCollin, M.M.; Rutter, J.L.; Murrell, J.R.; Duyao, M.P.; Parry, D.M.; Eldridge, R.; Kley, N.; Menon, A.G.; Pulaski, K.; et al. A novel moesin-, ezrin-, radixin-like gene is a candidate for the neurofibromatosis 2 tumor suppressor. Cell 1993, 75, 826. [Google Scholar] [CrossRef]
- Parry, D.M.; Eldridge, R.; Kaiser-Kupfer, M.I.; Bouzas, E.A.; Pikus, A.; Patronas, N. Neurofibromatosis 2 (NF2): Clinical characteristics of 63 affected individuals and clinical evidence for heterogeneity. Am. J. Med Genet. 1994, 52, 450–461. [Google Scholar] [CrossRef] [PubMed]
- Asthagiri, A.R.; Parry, D.M.; Butman, J.A.; Kim, H.J.; Tsilou, E.T.; Zhuang, Z.; Lonser, R.R. Neurofibromatosis type 2. Lancet 2009, 373, 1974–1986. [Google Scholar] [CrossRef]
- Halliday, D.; Emmanouil, B.; Pretorius, P.; MacKeith, S.; Painter, S.; Tomkins, H.; Evans, D.G.; Parry, A. Genetic Severity Score predicts clinical phenotype in NF2. J. Med. Genet. 2017, 54, 657–664. [Google Scholar] [CrossRef] [PubMed]
- Emmanouil, B.; Houston, R.; May, A.; Ramsden, J.D.; Hanemann, C.O.; Halliday, D.; Parry, A.; Mackeith, S. Progression of hearing loss in neurofibromatosis type 2 according to genetic severity. Laryngoscope 2018. [Google Scholar] [CrossRef] [PubMed]
- Gugel, I.; Grimm, F.; Teuber, C.; Kluwe, L.; Mautner, V.F.; Tatagiba, M.; Schuhmann, M.U. Management of NF2-associated vestibular schwannomas in children and young adults: Influence of surgery and clinical factors on tumor volume and growth rate. J. Neurosurg. Pediatr. 2019, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Gugel, I.; Grimm, F.; Liebsch, M.; Teuber, C.; Kluwe, L.; Mautner, V.F.; Tatagiba, M.; Schuhmann, M. Positive Impact of Surgery on Long-Term Results of Hearing in Neurofibromatosis Type 2 associated Vestibular Schwannomas. Cancers 2019, 11, 1376. [Google Scholar] [CrossRef] [PubMed]
- Plotkin, S.R.; Singh, M.A.; O’Donnell, C.C.; Harris, G.J.; McClatchey, A.I.; Halpin, C. Audiologic and radiographic response of NF2-related vestibular schwannoma to erlotinib therapy. Nat. Clin. Pract. Oncol. 2008, 5, 487–491. [Google Scholar] [CrossRef] [PubMed]
- Hochart, A.; Gaillard, V.; Baroncini, M.; Andre, N.; Vannier, J.P.; Vinchon, M.; Dubrulle, F.; Lejeune, J.P.; Vincent, C.; Neve, V.; et al. Bevacizumab decreases vestibular schwannomas growth rate in children and teenagers with neurofibromatosis type 2. J. Neurooncol. 2015, 124, 229–236. [Google Scholar] [CrossRef] [PubMed]
- Plotkin, S.R.; Merker, V.L.; Halpin, C.; Jennings, D.; McKenna, M.J.; Harris, G.J.; Barker, F.G., 2nd. Bevacizumab for progressive vestibular schwannoma in neurofibromatosis type 2: A retrospective review of 31 patients. Otol. Neurotol. 2012, 33, 1046–1052. [Google Scholar] [CrossRef] [PubMed]
- Lu, V.M.; Ravindran, K.; Graffeo, C.S.; Perry, A.; Van Gompel, J.J.; Daniels, D.J.; Link, M.J. Efficacy and safety of bevacizumab for vestibular schwannoma in neurofibromatosis type 2: A systematic review and meta-analysis of treatment outcomes. J. Neurooncol. 2019, 144, 239–248. [Google Scholar] [CrossRef] [PubMed]
- Caye-Thomasen, P.; Werther, K.; Nalla, A.; Bog-Hansen, T.C.; Nielsen, H.J.; Stangerup, S.E.; Thomsen, J. VEGF and VEGF receptor-1 concentration in vestibular schwannoma homogenates correlates to tumor growth rate. Otol. Neurotol. 2005, 26, 98–101. [Google Scholar] [CrossRef] [PubMed]
- Wong, H.K.; Lahdenranta, J.; Kamoun, W.S.; Chan, A.W.; McClatchey, A.I.; Plotkin, S.R.; Jain, R.K.; di Tomaso, E. Anti-vascular endothelial growth factor therapies as a novel therapeutic approach to treating neurofibromatosis-related tumors. Cancer Res. 2010, 70, 3483–3493. [Google Scholar] [CrossRef] [PubMed]
- Osumi, H.; Matsusaka, S.; Wakatsuki, T.; Suenaga, M.; Shinozaki, E.; Mizunuma, N. Angiotensin II type-1 receptor blockers enhance the effects of bevacizumab-based chemotherapy in metastatic colorectal cancer patients. Mol. Clin. Oncol. 2015, 3, 1295–1300. [Google Scholar] [CrossRef] [PubMed]
- Levin, V.A.; Chan, J.; Datta, M.; Yee, J.L.; Jain, R.K. Effect of angiotensin system inhibitors on survival in newly diagnosed glioma patients and recurrent glioblastoma patients receiving chemotherapy and/or bevacizumab. J. Neurooncol. 2017, 134, 325–330. [Google Scholar] [CrossRef] [PubMed]
- Baser, M.E.; Friedman, J.M.; Joe, H.; Shenton, A.; Wallace, A.J.; Ramsden, R.T.; Evans, D.G. Empirical development of improved diagnostic criteria for neurofibromatosis 2. Genet. Med. 2011, 13, 576–581. [Google Scholar] [CrossRef] [PubMed]
- Samii, M.; Matthies, C. Management of 1000 vestibular schwannomas (acoustic neuromas): Hearing function in 1000 tumor resections. Neurosurgery 1997, 40, 248–260. [Google Scholar] [CrossRef] [PubMed]
- Abo-Dalo, B.; Kutsche, K.; Mautner, V.; Kluwe, L. Large intragenic deletions of the NF2 gene: Breakpoints and associated phenotypes. Genes Chromosomes Cancer 2010, 49, 171–175. [Google Scholar] [CrossRef] [PubMed]
- Morris, K.A.; Golding, J.F.; Axon, P.R.; Afridi, S.; Blesing, C.; Ferner, R.E.; Halliday, D.; Jena, R.; Pretorius, P.M.; Evans, D.G.; et al. Bevacizumab in neurofibromatosis type 2 (NF2) related vestibular schwannomas: A nationally coordinated approach to delivery and prospective evaluation. Neurooncol. Pract. 2016, 3, 281–289. [Google Scholar] [CrossRef] [PubMed] [Green Version]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient | Sex | Age | NF2 Mutation | Additional Tumor Load |
|---|---|---|---|---|
| 10 | f | 29 | No mutation found | Intraspinal extramedullary tumors |
| 39 | f | 26 | Nonsense in exon 6 | Intracranial non-vestibular schwannomas and meningiomas, intraspinal extramedullary tumors |
| 19 | f | 25 | No mutation found (Mosaic) | Intracranial meningiomas and non-vestibular schwannomas, intraspinal intra- and extramedullary tumors |
| 11 | f | 23 | Frameshifting in exon 1 | Intracranial meningiomas, intraspinal extramedullary tumors |
| 2 | f | 21 | Frameshifting in exon 5 | Intracranial meningiomas, intraspinal extramedullary tumors |
| 17 | f | 18 | Not analysed | Intracranial meningiomas, intraspinal extramedullary tumors |
| 1 | m | 21 | No mutation found (Mosaic) | Intracranial meningiomas and non-vestibular schwannomas, intraspinal intra- and extramedullary tumors |
| 5 | m | 19 | Frameshifting in exon 5 | Intracranial meningiomas and non-vestibular schwannomas, intraspinal extramedullary tumors |
| 3 | f | 17 | Nonsense in exon 6 | Intracranial meningiomas and non-vestibular schwannomas |
| Operation Side | |
|---|---|
| Left | 9 |
| Right | 7 |
| Age at diagnosis in years (mean ± std, range) | 12 ± 7, 1–20 |
| Age at surgery in years (mean ± std, range) | 16 ± 5, 8–23 |
| Age at beginning with BVZ in years (mean ± std, range) | 19 ± 4, 14–26 |
| Postoperative follow-up period without BVZ in months (mean ± std, range) | 36 ± 26, 13–63 |
| Postoperative follow-up period with BVZ in months (mean ± std, range) | 28 ± 14, range 7–43 |
| Tumor volume in cm3 (mean ± std, range) | |
| - preoperative | 2.3 ± 2.8, 0.2–10.5 |
| - postoperative native | 0.9 ± 1.4, 0.03–5 |
| - postoperative with BVZ | 2.0 ± 1.8, 0.2–6.5 |
| Resection amount | |
| - only bony decompression | 1 |
| - decompression with laser coagulation | 1 |
| - partial (<90%) | 12 |
| - subtotal (≥90–<95%) | 2 |
| - near total (≥95–<100%) | 0 |
| - total (100%, inclusive tumor capsule) | 0 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gugel, I.; Kluwe, L.; Zipfel, J.; Teuber, C.; Tatagiba, M.; Mautner, V.-F.; Schuhmann, M.U.; Grimm, F. Minimal Effect of Bevacizumab Treatment on Residual Vestibular Schwannomas after Partial Resection in Young Neurofibromatosis Type 2 Patients. Cancers 2019, 11, 1862. https://doi.org/10.3390/cancers11121862
Gugel I, Kluwe L, Zipfel J, Teuber C, Tatagiba M, Mautner V-F, Schuhmann MU, Grimm F. Minimal Effect of Bevacizumab Treatment on Residual Vestibular Schwannomas after Partial Resection in Young Neurofibromatosis Type 2 Patients. Cancers. 2019; 11(12):1862. https://doi.org/10.3390/cancers11121862
Chicago/Turabian StyleGugel, Isabel, Lan Kluwe, Julian Zipfel, Christian Teuber, Marcos Tatagiba, Victor-Felix Mautner, Martin Ulrich Schuhmann, and Florian Grimm. 2019. "Minimal Effect of Bevacizumab Treatment on Residual Vestibular Schwannomas after Partial Resection in Young Neurofibromatosis Type 2 Patients" Cancers 11, no. 12: 1862. https://doi.org/10.3390/cancers11121862