Impact of CD56 Continuously Recognizable as Prognostic Value of Acute Promyelocytic Leukemia: Results of Multivariate Analyses in the Japan Adult Leukemia Study Group (JALSG)-APL204 Study and a Review of the Literature

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
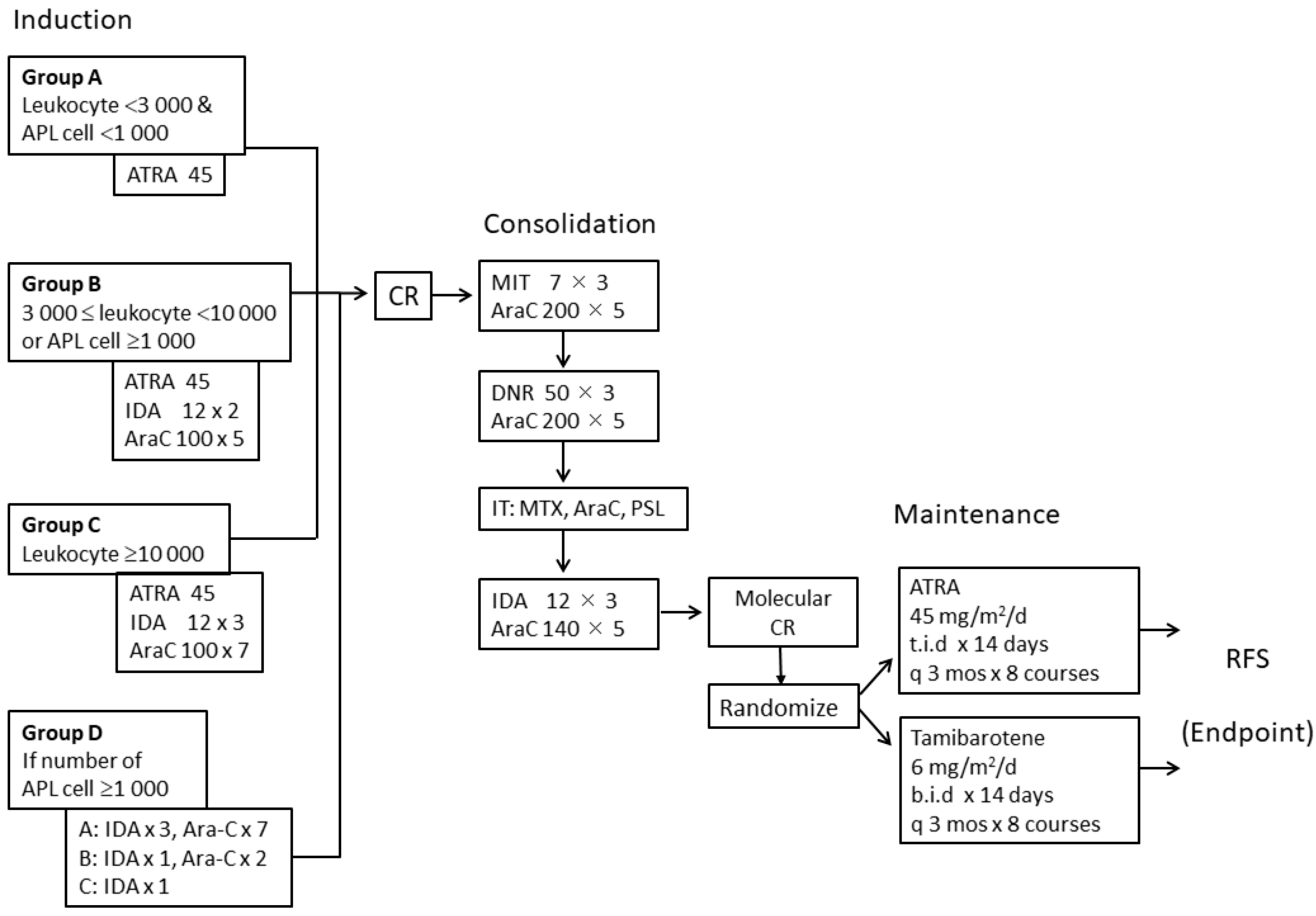
2.2. Treatments
2.3. Immunophenotypic Analyses
2.4. Definition of Outcomes
2.5. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Treatment Outcome
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Tallman, M.S.; Andersen, J.W.; Schiffer, C.A.; Appelbaum, F.R.; Feusner, J.H.; Ogden, A.; Shepherd, L.; Willman, C.; Bloomfield, C.D.; Rowe, J.M.; et al. All-trans-retinoic acid in acute promyelocytic leukemia. N. Engl. J. Med. 1997, 337, 1021–1028. [Google Scholar] [CrossRef] [PubMed]
- Fenaux, P.; Chastang, C.; Chevret, S.; Sanz, M.; Dombret, H.; Archimbaud, E.; Fey, M.; Rayon, C.; Huguet, F.; Sotto, J.J.; et al. A randomized comparison of all trans retinoic acid (ATRA) followed by chemotherapy and ATRA plus chemotherapy and the role of maintenance therapy in newly diagnosed acute promyelocytic leukemia: The European APL Group. Blood 1999, 94, 1192–1200. [Google Scholar] [CrossRef]
- Burnett, A.K.; Grimwade, D.; Solomon, E.; Wheatley, K.; Goldstone, A.H. Presenting white blood cell count and kinetics of molecular remission predict prognosis in acute promyelocytic leukemia treated with all-trans retinoic acid: Result of the Randomized MRC Trial. Blood 1999, 93, 4131–4143. [Google Scholar] [CrossRef]
- Sanz, M.A.; Lo Coco, F.; Martín, G.; Avvisati, G.; Rayón, C.; Barbui, T.; Díaz-Mediavilla, J.; Fioritoni, G.; González, J.D.; Liso, V.; et al. Definition of relapse risk and role of nonanthracycline drugs for consolidation in patients with acute promyelocytic leukemia: A joint study of the PETHEMA and GIMEMA cooperative groups. Blood 2000, 96, 1247–1253. [Google Scholar] [PubMed]
- Tallman, M.S.; Andersen, J.W.; Schiffer, C.A.; Appelbaum, F.R.; Feusner, J.H.; Woods, W.G.; Ogden, A.; Weinstein, H.; Shepherd, L.; Willman, C.; et al. All-trans retinoic acid in acute promyelocytic leukemia: Long-term outcome and prognostic factor analysis from the North American Intergroup protocol. Blood 2002, 100, 4298–4302. [Google Scholar] [CrossRef] [PubMed]
- Adès, L.; Chevret, S.; Raffoux, E.; de Botton, S.; Guerci, A.; Pigneux, A.; Stoppa, A.M.; Lamy, T.; Rigal-Huguet, F.; Vekhoff, A.; et al. Is cytarabine useful in the treatment of acute promyelocytic leukemia? Results of a randomized trial from the European Acute Promyelocytic Leukemia Group. J. Clin. Oncol. 2006, 24, 5703–5710. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Asou, N.; Kishimoto, Y.; Kiyoi, H.; Okada, M.; Kawai, Y.; Tsuzuki, M.; Horikawa, K.; Matsuda, M.; Shinagawa, K.; Kobayashi, T.; et al. A randomized study with or without intensified maintenance chemotherapy in patients with acute promyelocytic leukemia who have become negative for PML-RARalpha transcript after consolidation therapy: The Japan Adult Leukemia Study Group (JALSG) APL97 study. Blood 2007, 110, 59–66. [Google Scholar] [CrossRef] [PubMed]
- Kelaidi, C.; Chevret, S.; De Botton, S.; Raffoux, E.; Guerci, A.; Thomas, X.; Pigneux, A.; Lamy, T.; Rigal-Huguet, F.; Meyer-Monard, S.; et al. Improved outcome of acute promyelocytic leukemia with high WBC counts over the last 15 years: The European APL Group experience. J. Clin. Oncol. 2009, 27, 2668–2676. [Google Scholar] [CrossRef] [PubMed]
- Lo-Coco, F.; Avvisati, G.; Vignetti, M.; Breccia, M.; Gallo, E.; Rambaldi, A.; Paoloni, F.; Fioritoni, G.; Ferrara, F.; Specchia, G.; et al. Front-line treatment of acute promyelocytic leukemia with AIDA induction followed by risk-adapted consolidation for adults younger than 61 years: Results of the AIDA-2000 trial of the GIMEMA Group. Blood 2010, 116, 3171–3179. [Google Scholar] [CrossRef]
- Adès, L.; Guerci, A.; Raffoux, E.; Sanz, M.; Chevallier, P.; Lapusan, S.; Recher, C.; Thomas, X.; Rayon, C.; Castaigne, S.; et al. Very long-term outcome of acute promyelocytic leukemia after treatment with all-trans retinoic acid and chemotherapy: The European APL Group experience. Blood 2010, 115, 1690–1696. [Google Scholar] [CrossRef] [Green Version]
- Sanz, M.A.; Montesinos, P.; Rayón, C.; Holowiecka, A.; de la Serna, J.; Milone, G.; de Lisa, E.; Brunet, S.; Rubio, V.; Ribera, J.M.; et al. Risk-adapted treatment of acute promyelocytic leukemia based on all-trans retinoic acid and anthracycline with addition of cytarabine in consolidation therapy for high-risk patients: Further improvements in treatment outcome. Blood 2010, 115, 5137–5146. [Google Scholar] [CrossRef]
- Avvisati, G.; Lo-Coco, F.; Paoloni, F.P.; Petti, M.C.; Diverio, D.; Vignetti, M.; Latagliata, R.; Specchia, G.; Baccarani, M.; Di Bona, E.; et al. AIDA 0493 protocol for newly diagnosed acute promyelocytic leukemia: Very long-term results and role of maintenance. Blood 2011, 117, 4716–4725. [Google Scholar] [CrossRef] [PubMed]
- Cervera, J.; Montesinos, P.; Hernandez-Rivas, J.; Calosanz, M.J.; Aventin, A.; Ferro, M.T.; Luño, E.; Sánchez, J.; Vellenga, E.; Rayón, C.; et al. Additional chromosomal abnormalities treated with all-trans retinoic acid and chemotherapy. Haematologica 2010, 95, 424–431. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Murray, C.K.; Estey, E.; Paietta, E.; Howard, R.S.; Edenfield, W.J.; Pierce, S.; Mann, K.P.; Bolan, C.; Byrd, J.C. CD56 expression in acute promyelocytic leukemia: A possible indicator of poor treatment outcome? J. Clin. Oncol. 1999, 17, 293–297. [Google Scholar] [CrossRef] [PubMed]
- Rasekh, E.O.; Elsayed, G.M.; Madney, Y.; El Gammal, M.M. Prognostic significance of bcr-1 and bcr-3 isoforms of PML-RARA and FLT3-ITD in patients with acute promyelocytic leukemia. Clin. Lymphoma Myeloma Leuk. 2020, 20, 156–167. [Google Scholar] [CrossRef] [PubMed]
- Lucena-Araujo, A.R.; Kim, H.T.; Jacomo, R.H.; Melo, R.A.; Bittencourt, R.; Pasquini, R.; Pagnano, K.; Fagundes, E.M.; Chauffaille-Mde, L.; Chiattone, C.S.; et al. Internal tandem duplication of the FLT3 gene confer poor overall survival in patients with acute promyelocytic leukemia treated with all-trans retinoic acid and anthracycline-based chemotherapy: An International Consortium on acute promyelocytic leukemia study. Ann. Hematol. 2014, 93, 2001–2010. [Google Scholar]
- Noguera, N.I.; Breccia, M.; Divona, M.; Diverio, D.; Costa, V.; De Santis, S.; Avvisati, G.; Pinazzi, M.B.; Petti, M.C.; Mandelli, F.; et al. Alterations of the FLT3 gene in acute promyelocyticleukemia: Association with diagnostic characteristics and analysis of clinical outcome in patients treated with the Italian AIDA protocol. Leukemia 2002, 16, 2185–2189. [Google Scholar] [CrossRef] [Green Version]
- Liquori, A.; Ibañez, M.; Sargas, C.; Sanz, M.Á.; Barragán, E.; Cervera, J. Acute promyelocytic leukemia: A constellation of molecular events around a single PML-RARA fusion gene. Cancers 2020, 12, 624. [Google Scholar] [CrossRef] [Green Version]
- Testa, U.; Lo-Coco, F. Prognostic factors in acute promyelocytic leukemia: Strategies to define high-risk patients. Ann. Hematol. 2016, 95, 673–680. [Google Scholar] [CrossRef]
- Sanz, M.A.; Fenaux, P.; Tallman, M.S.; Estey, E.H.; Löwenberg, B.; Naoe, T.; Lengfelder, E.; Döhner, H.; Burnett, A.K.; Chen, S.J.; et al. Management of acute promyelocytic leukemia: Updated recommendations from an expert panel of the European LeukemiaNet. Blood 2019, 133, 1630–1643. [Google Scholar] [CrossRef] [Green Version]
- Shinagawa, K.; Yanada, M.; Sakura, T.; Ueda, Y.; Sawa, M.; Miyatake, J.; Dobashi, N.; Kojima, M.; Hatta, Y.; Emi, N.; et al. Tamibarotene as maintenance therapy for acute promyelocytic leukemia: Results from a randomized controlled trial. J. Clin. Oncol. 2014, 32, 3729–3735. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Takeshita, A.; Asou, N.; Atsuta, Y.; Sakura, T.; Ueda, Y.; Sawa, M.; Dobashi, N.; Taniguchi, Y.; Suzuki, R.; Nakagawa, M.; et al. Tamibarotene maintenance improved relapse-free survival of acute promyelocytic leukemia: A final result of prospective, randomized, JALSG-APL204 Study. Leukemia 2019, 33, 358–370. [Google Scholar] [CrossRef]
- Kagechika, H.; Kawachi, E.; Hashimoto, Y.; Himi, T.; Shudo, K. Retinobenzoic acids: 1. Structure-activity relationships of aromatic amides with retinoidal activity. J. Med. Chem. 1988, 31, 2182–2192. [Google Scholar] [CrossRef] [PubMed]
- Hashimoto, Y.; Kagechika, H.; Kawachi, E.; Fukasawa, H.; Saito, G.; Shudo, K. Correlation of differentiation-inducing activity of retinoids on human leukemia cell lines HL-60 and NB4. J. Cancer Res. Clin. Oncol. 1995, 121, 696–698. [Google Scholar] [CrossRef]
- Takeshita, A.; Shibata, Y.; Shinjo, K.; Yanagi, M.; Tobita, T.; Ohnishi, K.; Miyawaki, S.; Shudo, K.; Ohno, R. Successful treatment of relapse of acute promyelocytic leukemia with a new synthetic retinoid, Am80. Ann. Intern. Med. 1996, 124, 893–896. [Google Scholar] [CrossRef] [PubMed]
- Tobita, T.; Takeshita, A.; Kitamura, K.; Ohnishi, K.; Yanagi, M.; Hiraoka, A.; Karasuno, T.; Takeuchi, M.; Miyawaki, S.; Ueda, R.; et al. Treatment with a new synthetic retinoid, Am80, of acute promyelocytic leukemia relapsed from complete remission induced by all-trans retinoic acid. Blood 1997, 90, 967–973. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ono, T.; Takeshita, A.; Kishimoto, Y.; Kiyoi, H.; Okada, M.; Yamauchi, T.; Emi, N.; Horikawa, K.; Matsuda, M.; Shinagawa, K.; et al. Expression of CD56 is an unfavorable prognostic factor for acute promyelocytic leukemia with higher initial white blood cell counts. Cancer Sci. 2014, 105, 97–104. [Google Scholar] [CrossRef]
- Bene, M.C.; Castoldi, G.; Knapp, W.; Ludwig, W.D.; Matutes, E.; Orfao, A.; van’t Veer, M.B. Proposals for the immunological classification of acute leukemias. European Group for the Immunological Characterization of Leukemias (EGIL). Leukemia 1995, 9, 1783–1786. [Google Scholar]
- Fine, J.P.; Gray, R.J. A proportional hazards model for the subdistribution of a competing risk. J. Am. Stat. Assoc. 1999, 94, 496–509. [Google Scholar] [CrossRef]
- Raspadori, D.; Damiani, D.; Lenoci, M.; Rondelli, D.; Testoni, N.; Nardi, G.; Sestigiani, C.; Mariotti, C.; Birtolo, S.; Tozzi, M.; et al. CD56 antigenic expression in acute myeloid leukemia identifies patients with poor clinical prognosis. Leukemia 2001, 15, 1161–1164. [Google Scholar] [CrossRef]
- Raspadori, D.; Damiani, D.; Michieli, M.; Stocchi, R.; Gentili, S.; Gozzetti, A.; Masolini, P.; Michelutti, A.; Geromin, A.; Fanin, R.; et al. CD56 and PGP expression in acute myeloid leukemia: Impact on clinical outcome. Haematologica 2002, 87, 1135–1140. [Google Scholar] [PubMed]
- Novotny, J.R.; Nückel, H.; Dührsen, U. Correlation between expression of CD56/NCAM and severe leukostasis in hyperleukocytic acute myelomonocytic leukaemia. Eur. J. Haematol. 2006, 76, 299–308. [Google Scholar] [CrossRef] [PubMed]
- Chang, H.; Brandwein, J.; Yi, Q.L.; Chun, K.; Patterson, B.; Brien, B. Extramedullary infiltrates of AML are associated with CD56 expression, 11q23 abnormalities and inferior clinical outcome. Leuk. Res. 2004, 28, 1007–1011. [Google Scholar] [CrossRef]
- Sasca, D.; Szybinski, J.; Schüler, A.; Shah, V.; Heidelberger, J.; Haehnel, P.S.; Dolnik, A.; Kriege, O.; Fehr, E.M.; Gebhardt, W.H.; et al. NCAM1 (CD56) promotes leukemogenesis and confers drug resistance in AML. Blood 2019, 133, 2305–2319. [Google Scholar] [CrossRef] [PubMed]
- Lin, P.; Hao, S.; Medeiros, L.J.; Estey, E.H.; Pierce, S.A.; Wang, X.; Glassman, A.B.; Bueso-Ramos, C.; Huh, Y. Expression of CD2 in acute promyelocytic leukemia correlates with short form of PML-RARalpha transcripts and poorer prognosis. Am. J. Clin. Pathol. 2004, 121, 402–407. [Google Scholar] [CrossRef] [PubMed]
- Breccia, M.; De Propris, M.S.; Stefanizzi, C.; Raponi, S.; Modica, M.; Colafigli, G.; Minotti, C.; Latagliata, R.; Diverio, D.; Guarini, A.; et al. Negative prognostic value of CD34 antigen also if expressed on a small population of acute promyelocytic leukemia cells. Ann. Hematol. 2014, 93, 1819–1823. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.J.; Cho, D.; Chung, I.J.; Cho, S.H.; Park, K.S.; Park, M.R.; Ryang, D.W.; Kim, H.J. CD34 expression is associated with poor clinical outcome in patients with acute promyelocytic leukemia. Am. J. Haematol. 2003, 73, 149–153. [Google Scholar] [CrossRef] [PubMed]
- Montesinos, P.; Rayón, C.; Vellenga, E.; Brunet, S.; González, J.; González, M.; Holowiecka, A.; Esteve, J.; Bergua, J.; González, J.D.; et al. Clinical significance of CD56 expression in patients with acute promyelocytic leukemia treated with all-trans retinoic acid and anthracycline-based regimens. Blood 2011, 117, 1799–1805. [Google Scholar] [CrossRef] [Green Version]
- Ito, S.; Ishida, Y.; Oyake, T.; Satoh, M.; Aoki, Y.; Kowata, S.; Uchiyama, T.; Enomoto, S.; Sugawara, T.; Numaoka, H.; et al. Clinical and biological significance of CD56 antigen expression in acute promyelocytic leukemia. Leuk. Lymphoma 2004, 45, 1783–1789. [Google Scholar] [CrossRef]
- Breccia, M.; De Propris, M.S.; Minotti, C.; Stefanizzi, C.; Raponi, S.; Colafigli, G.; Latagliata, R.; Guarini, A.; Foà, R. Aberrant phenotypic expression of CD15 and CD56 identifies poor prognostic acute promyelocytic leukemia patients. Leuk. Res. 2014, 38, 194–197. [Google Scholar] [CrossRef]
- Ferrara, F.; Morabito, F.; Martino, B.; Specchia, G.; Liso, V.; Nobile, F.; Boccuni, P.; Di Noto, R.; Pane, F.; Annunziata, M.; et al. CD56 expression is an indicator of poor clinical outcome in patients with acute promyelocytic leukemia treated with simultaneous all-trans-retinoic acid and chemotherapy. J. Clin. Oncol. 2000, 18, 1295–1300. [Google Scholar] [CrossRef] [PubMed]
- Sobas, M.; Montesinos, P.; Boluda, B.; Bernal, T.; Vellenga, E.; Nomdedeu, J.; González-Campos, J.; Chillón, M.; Holowiecka, A.; Esteve, J.; et al. PETHEMA, HOVON, PALG, and GATLA cooperative groups. An analysis of the impact of CD56 expression in de novo acute promyelocytic leukemia patients treated with upfront all-trans retinoic acid and anthracycline-based regimens. Leuk. Lymphoma 2019, 60, 1030–1035. [Google Scholar] [CrossRef] [PubMed]
- Lou, Y.; Ma, Y.; Suo, S.; Ni, W.; Wang, Y.; Pan, H.; Tong, H.; Qian, W.; Meng, H.; Mai, W.; et al. Prognostic factors of patients with newly diagnosed acute promyelocytic leukemia treated with arsenic trioxide-based frontline therapy. Leuk. Res. 2015, 39, 938–944. [Google Scholar] [CrossRef]
- Lo-Coco, F.; Avvisati, G.; Vignetti, M.; Thiede, C.; Orlando, S.M.; Iacobelli, S.; Ferrara, F.; Fazi, P.; Cicconi, L.; Di Bona, E.; et al. Retinoic acid and arsenic trioxide for acute promyelocytic leukemia. N. Engl. J. Med. 2013, 369, 111–121. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Platzbecker, U.; Avvisati, G.; Cicconi, L.; Thiede, C.; Paoloni, F.; Vignetti, M.; Fazi, P.; Ferrara, F.; Divona, M.; Albano, F.; et al. Long-term results of all-trans retinoic acid and arsenic trioxide in non-high-risk acute promyelocytic leukemia: Update of the APL0406 Italian-German randomized trial. Leukemia 2020, 34, 914–918. [Google Scholar]
- Burnett, A.K.; Russell, N.H.; Hills, R.K.; Bowen, D.; Kell, J.; Knapper, S.; Morgan, Y.G.; Lok, J.; Grech, A.; Jones, G.; et al. Arsenic trioxide and all-trans retinoic acid treatment for acute promyelocytic leukaemia in all risk groups (AML17): Results of a randomised, controlled, phase 3 trial. Lancet Oncol. 2015, 16, 1295–1305. [Google Scholar] [CrossRef]
- Iland, H.J.; Collins, M.; Bradstock, K.; Supple, S.G.; Catalano, A.; Hertzberg, M.; Browett, P.; Grigg, A.; Firkin, F.; Campbell, L.J.; et al. Use of arsenic trioxide in remission induction and consolidation therapy for acute promyelocytic leukaemia in the Australasian Leukaemia and Lymphoma Group (ALLG) APML4 study: A non-randomised phase 2 trial. Lancet Haematol. 2015, 2, e357–e366. [Google Scholar] [CrossRef]
- Abaza, Y.; Kantarjian, H.; Garcia-Manero, G.; Estey, E.; Borthakur, G.; Jabbour, E.; Faderl, S.; O’Brien, S.; Wierda, W.; Pierce, S.; et al. Long-term outcome of acute promyelocytic leukemia treated with all-trans-retinoic acid, arsenic trioxide, and gemtuzumab. Blood 2017, 129, 1275–1283. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Before Induction (n = 344) | Randomly Assigned for Maintenance Therapy | p-Value | |
|---|---|---|---|---|
| ATRA (n = 135) | Tamibarotene (n = 134) | |||
| Age (years) | 0.597 | |||
| Median (range) | 48 (15–70) | 48 (15–70) | 46 (16–69) | |
| Sex | 0.758 | |||
| Male/Female | 183/161 | 70/65 | 72/62 | |
| Performance status | 0.858 | |||
| 0/1/2/3 | 188/126/19/11 | 72/50/8/5 | 78/43/8/5 | |
| Leukocyte count (×109/L) | 0.841 | |||
| Median (range) | 1.4 (0.1–127) | 1.3 (0.2–111) | 1.4 (0.2–88.5) | |
| APL cell count (×109/L) | 0.502 | |||
| Median (range) | 0.3 (0–109) | 0.2 (0–09) | 0.4 (0–87) | |
| Platelet count (×109/L) | 0.343 | |||
| Median (range) | 31 (1–470) | 28 (2–208) | 32 (1–470) | |
| Sanz’s risk category | 0.939 | |||
| Low | 117 | 47 | 44 | |
| Intermediate | 157 | 62 | 64 | |
| High | 70 | 26 | 26 | |
| Fibrinogen level (mg/dL) | 0.578 | |||
| Median (range) | 144 (8–810) | 147 (27–593) | 137 (8–496) | |
| FDP | 0.784 | |||
| Median (range) | 50.3 (0–800) | 53.7 (2.5–800) | 51.4 (0–576.5) | |
| DIC score | 0.946 | |||
| 0–2 | 37 | 14 | 15 | |
| 3–9 | 241 | 93 | 97 | |
| Undetermined † | 66 | 28 | 22 | |
| FAB subtype | 0.434 | |||
| M3/M3v | 323/21 | 126/9 | 128/6 | |
| Induction therapy group | 0.984 | |||
| A/B/C/D | 112/48/70/114 | 47/18/26/44 | 45/20/26/43 | |
| Additional Chromosome change other than t (15;17) | 0.453 | |||
| None | 225 | 93 | 88 | |
| Present | 111 | 39 | 45 | |
| Undetermined * | 8 | 3 | 1 | |
| Clinical Features | Cases Achieving CR | Cases Who did not Achieve CR | p-Value |
|---|---|---|---|
| No. of Cases | No. of Cases | ||
| Total | 319 | 25 | |
| Age (years) | 0.283 | ||
| 15–59 | 258 | 18 | |
| 60–70 | 61 | 7 | |
| Sex | 0.124 | ||
| Male/Female | 166/153 | 17/8 | |
| FAB subtype | 0.201 | ||
| M3/M3v | 301/18 | 22/3 | |
| Leukocyte count (×109/L) | 0.011 | ||
| <3.0 | 220 | 11 | |
| ≥3.0 | 99 | 14 | |
| 0.044 | |||
| <10.0 | 258 | 16 | |
| ≥10.0 | 61 | 9 | |
| Platelet count (×109/L) | 0.244 | ||
| <40.0 | 192 | 18 | |
| ≥40.0 | 127 | 7 | |
| Sanz’s risk category | 0.130 | ||
| Low | 110 | 7 | |
| Intermediate | 148 | 9 | |
| High | 61 | 9 | |
| Performance status | 0.397 | ||
| 0/1/2/3 | 178/113/18/10 | 10/13/1/1 | |
| CD34 | 0.417 | ||
| <10% | 225 | 18 | |
| ≥10% | 79 | 4 | |
| CD56 | 0.212 | ||
| <10% | 263 | 17 | |
| ≥10% | 40 | 5 | |
| Additional Chromosome change other than t (15;17) | 0.351 | ||
| None | 211 | 14 | |
| Present | 101 | 10 | |
| Induction therapy | 0.066 | ||
| A/B/C/D | 109/45/61/104 | 3/3/9/10 | |
| (a) | |||||
| Clinical Features | No. of Cases | Median (Range) | HR | 95% CI | p-Value |
| Age (years) | |||||
| 15–59 vs. 60–70 | 221 vs. 48 | 46 (15–70) | 0.62 | 0.21–1.78 | 0.373 |
| Sex | |||||
| Male vs. Female | 141 vs. 128 | 0.73 | 0.36–1.47 | 0.376 | |
| Leukocyte count (×109/L) | |||||
| <3.0 vs. ≥3.0 | 184 vs. 85 | 1.3 (0.2–111) | 2.72 | 1.36–5.45 | 0.003 |
| <10.0 vs. ≥10.0 | 217 vs. 52 | 3.39 | 1.67–6.87 | <0.001 | |
| Platelet (×109/L) | |||||
| <40 vs. ≥40 | 164 vs. 105 | 30 (1–470) | 0.77 | 0.37–1.59 | 0.477 |
| Sanz’s risk category | |||||
| Low, Intermediate, and High | 52, 126, and 91 | 0.001 | |||
| Performance status | |||||
| 0, 1, 2, and 3 | 149, 94, 16 and 10 | 0.302 | |||
| CD34-positive blast | |||||
| <10% vs. ≥10% | 191 vs. 65 | 3 (0–91) | 2.13 | 1.02–4.45 | 0.040 |
| CD56-positive blast | |||||
| <10% vs. ≥10% | 221 vs. 34 | 2 (0–99) | 3.04 | 1.34–6.90 | 0.005 |
| Additional Chromosome change other than t (15;17) | |||||
| None vs. Presence | 181 vs. 84 | 1.09 | 0.53–2.26 | 0.821 | |
| Induction Therapy | |||||
| A, B, C, and D | 92, 38, 52 and 87 | 0.005 | |||
| Maintenance Therapy | |||||
| ATRA vs. Tamibarotene | 135 vs. 134 | 0.44 | 0.21–0.93 | 0.027 | |
| (b) | |||||
| Clinical Features | No. of Cases | Median (Range) | HR | 95% CI | p-Value |
| Leukocyte count (×109/L) | |||||
| <10.0 vs. ≥10.0 | 204 vs. 51 | 1.4 (0.2–111) | 3.55 | 1.68–7.50 | 0.001 |
| CD56-positive blast | |||||
| <10% vs. ≥10% | 221 vs. 34 | 2 (0–99) | 3.19 | 1.40–7.27 | 0.006 |
| Maintenance Therapy | |||||
| ATRA vs. Tamibarotene | 125 vs. 130 | 0.41 | 0.19–0.91 | 0.028 | |
| CD No. | No. of Cases | OS (%) | p-Value | EFS (%) | p-Value | No. of Cases | RFS (%) | p-Value | CIR (%) | p-Value | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| − | + | − | + | − | + | − | + | |||||||
| CD2 | 193 vs. 107 | 90.5 | 81.9 | 0.084 | 84.3 | 72.7 | 0.030 | 153 vs. 80 | 92.2 | 83.8 | 0.053 | 6.7 | 16.6 | 0.019 |
| CD4 | 223 vs. 42 | 87.2 | 97.6 | 0.116 | 78.7 | 95.2 | 0.029 | 170 vs. 37 | 87.6 | 94.6 | 0.204 | 12.1 | 2.7 | 0.094 |
| CD5 | 246 vs. 11 | 88.4 | 100.0 | 0.231 | 80.3 | 90.0 | 0.366 | 192 vs. 10 | 87.5 | 90.0 | 0.847 | 11.7 | 11.1 | 0.932 |
| CD7 | 299 vs. 15 | 88.4 | 80.0 | 0.094 | 81.8 | 66.7 | 0.033 | 236 vs. 10 | 89.8 | 80.0 | 0.372 | 10.0 | 10.0 | 0.979 |
| CD8 | 243 vs. 10 | 88.6 | 100.0 | 0.259 | 80.9 | 88.9 | 0.445 | 187 vs. 9 | 88.8 | 88.9 | 0.970 | 10.4 | 12.5 | 0.873 |
| CD11b | 95 vs. 17 | 86.9 | 76.5 | 0.216 | 83.1 | 76.5 | 0.467 | 74 vs. 11 | 93.2 | 100.0 | 0.377 | 6.76 | 0.0 | 0.372 |
| CD14 | 301 vs. 20 | 88.2 | 90.0 | 0.319 | 80.5 | 85.0 | 0.615 | 239 vs. 14 | 89.1 | 85.7 | 0.741 | 10.7 | 7.1 | 0.689 |
| CD15 | 67 vs. 22 | 87.9 | 77.3 | 0.190 | 82.0 | 77.3 | 0.543 | 55 vs. 15 | 90.9 | 100.0 | 0.263 | 9.1 | 0.0 | 0.258 |
| CD19 | 284 vs. 34 | 87.7 | 88.2 | 0.756 | 80.9 | 79.0 | 0.615 | 224 vs. 24 | 88.8 | 91.7 | 0.646 | 10.4 | 9.1 | 0.751 |
| CD20 | 244 vs. 9 | 89.1 | 100.0 | 0.292 | 81.3 | 88.9 | 0.528 | 189 vs. 8 | 88.4 | 87.5 | 0.941 | 10.8 | 12.5 | 0.858 |
| CD34 | 243 vs. 83 | 89.4 | 89.1 | 0.158 | 82.2 | 75.5 | 0.172 | 191 vs. 65 | 91.1 | 81.5 | 0.040 | 8.5 | 17.5 | 0.056 |
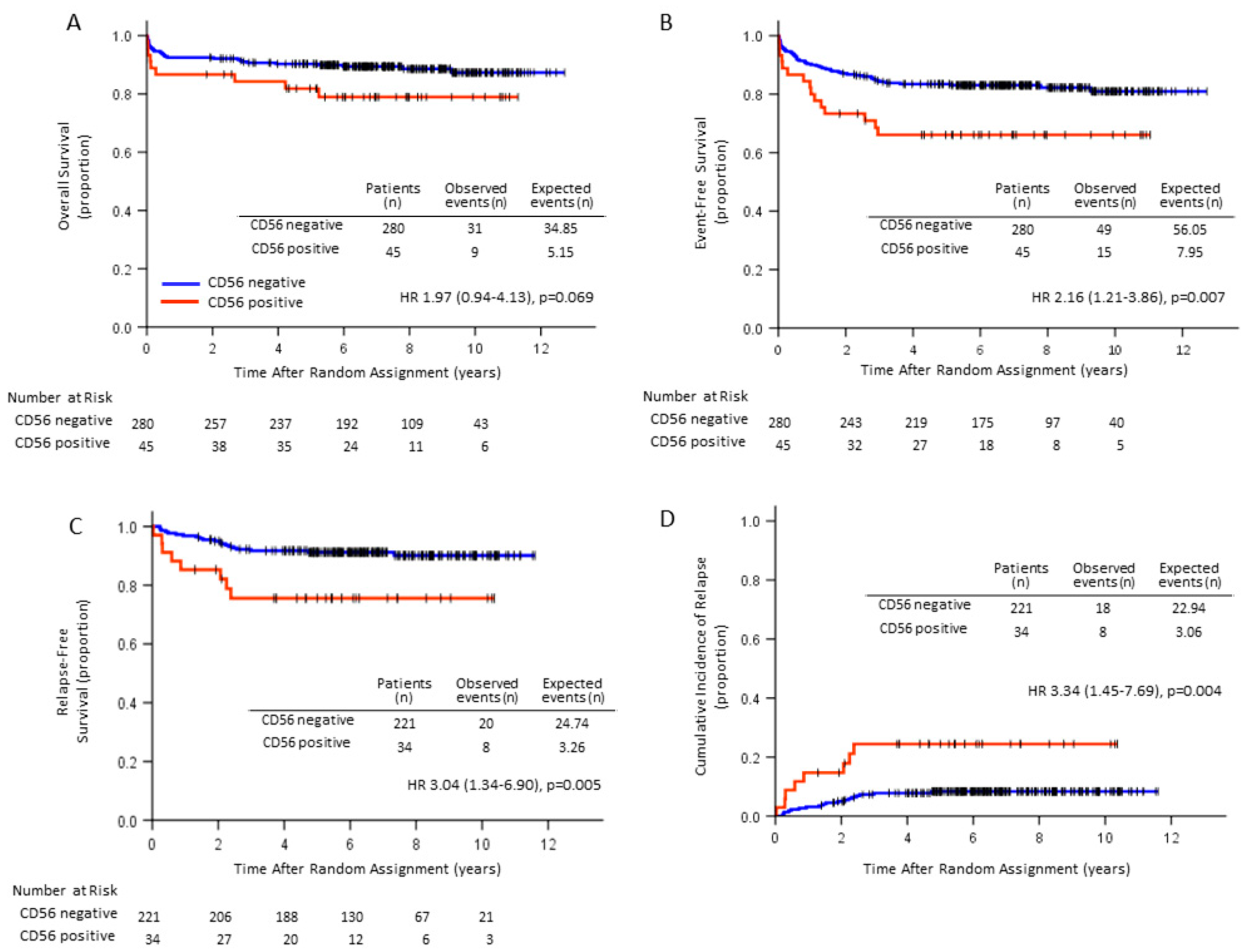
| CD56 | 280 vs. 45 | 89.4 | 78.9 | 0.069 | 83.1 | 66.1 | 0.007 | 221 vs. 34 | 91.0 | 76.5 | 0.005 | 8.1 | 23.5 | 0.004 |
| DR | 245 vs. 72 | 87.9 | 88.8 | 0.732 | 80.2 | 81.8 | 0.937 | 191 vs. 57 | 89.9 | 87.0 | 0.850 | 6.8 | 5.3 | 0.997 |
| Characteristic | CD56-Positive | CD56-Negative | p-Value | ||
|---|---|---|---|---|---|
| (n = 45) | (n = 280) | ||||
| Age (years) | 0.903 | ||||
| Median (range) | 45 (20–69) | 48 (15–70) | |||
| Sex | 0.068 | ||||
| Male/Female | 18/27 | 153/127 | |||
| Performance status | 0.363 | ||||
| 0/1/2/3 | 21/21/3/0 | 154/102/14/10 | |||
| Leukocyte count (× 109/L) | 0.304 | ||||
| Median (range) | 1.7 (0.4–27) | 1.3 (0.1–111) | |||
| APL cell count (× 109/L) | 0.543 | ||||
| Median (range) | 0.7 (0–96.5) | 0.2 (0–109) | |||
| Platelet count (× 109/L) | 0.569 | ||||
| Median (range) | 33 (3–160) | 30 (1–237) | |||
| Sanz’s risk category | 0.939 | ||||
| Low | 11 | 93 | |||
| Intermediate | 21 | 132 | |||
| High | 13 | 55 | |||
| Fibrinogen level (mg/dL) | 0.478 | ||||
| Median (range) | 166 (45–545) | 139 (8–810) | |||
| FDP | 0.522 | ||||
| Median (range) | 51.2 (7.5–255.5) | 52.5 (0–800) | |||
| DIC score | 0.717 | ||||
| 0–2 | 5 | 28 | |||
| 3–9 | 30 | 203 | |||
| Undetermined † | 10 | 49 | |||
| Morphology | 0.172 | ||||
| M3/M3v | 40/5 | 264/16 | |||
| Induction therapy group | 0.897 | ||||
| A/B/C/D | 13/6/11/15 | 90/40/55/95 | |||
| Additional Chromosome change other than t (15;17) | 0.923 | ||||
| None | 30 | 184 | |||
| Present | 15 | 89 | |||
| Undetermined * | 0 | 7 | |||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Takeshita, A.; Asou, N.; Atsuta, Y.; Furumaki, H.; Sakura, T.; Ueda, Y.; Sawa, M.; Dobashi, N.; Taniguchi, Y.; Suzuki, R.; et al. Impact of CD56 Continuously Recognizable as Prognostic Value of Acute Promyelocytic Leukemia: Results of Multivariate Analyses in the Japan Adult Leukemia Study Group (JALSG)-APL204 Study and a Review of the Literature. Cancers 2020, 12, 1444. https://doi.org/10.3390/cancers12061444
Takeshita A, Asou N, Atsuta Y, Furumaki H, Sakura T, Ueda Y, Sawa M, Dobashi N, Taniguchi Y, Suzuki R, et al. Impact of CD56 Continuously Recognizable as Prognostic Value of Acute Promyelocytic Leukemia: Results of Multivariate Analyses in the Japan Adult Leukemia Study Group (JALSG)-APL204 Study and a Review of the Literature. Cancers. 2020; 12(6):1444. https://doi.org/10.3390/cancers12061444
Chicago/Turabian StyleTakeshita, Akihiro, Norio Asou, Yoshiko Atsuta, Hiroaki Furumaki, Toru Sakura, Yasunori Ueda, Masashi Sawa, Nobuaki Dobashi, Yasuhiro Taniguchi, Rikio Suzuki, and et al. 2020. "Impact of CD56 Continuously Recognizable as Prognostic Value of Acute Promyelocytic Leukemia: Results of Multivariate Analyses in the Japan Adult Leukemia Study Group (JALSG)-APL204 Study and a Review of the Literature" Cancers 12, no. 6: 1444. https://doi.org/10.3390/cancers12061444