Age at Onset and Presenting Symptoms of Neurofibromatosis Type 2 as Prognostic Factors for Clinical Course of Vestibular Schwannomas

 ,
,
Abstract
:1. Introduction
2. Results
2.1. Patients, Tumors, and Presenting Symptoms
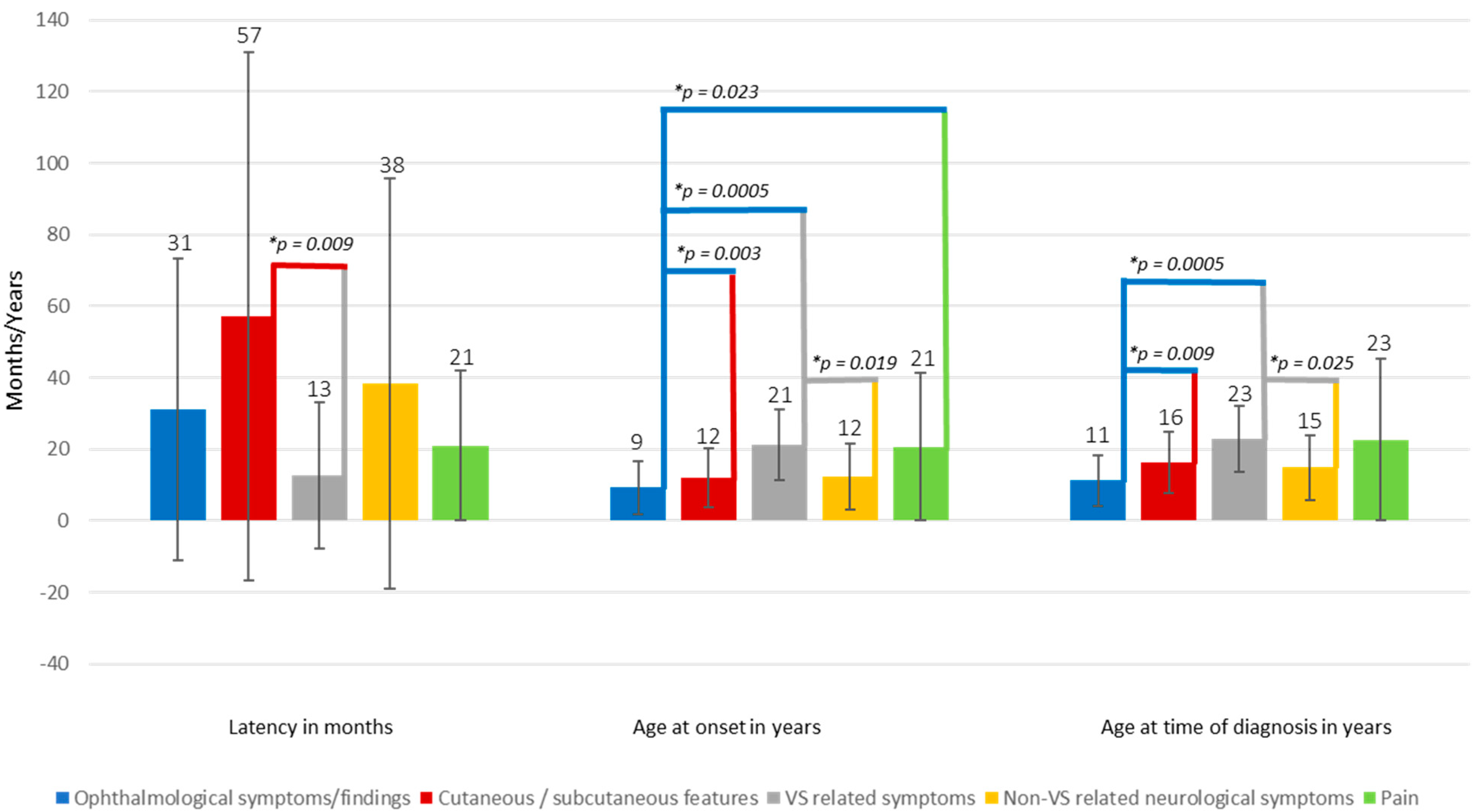
2.2. Influence of Presenting Symptom(s) on Time to Diagnosis
2.3. Association of Age at Onset with VS Related Parameters
2.4. Association of Presenting Symptoms with VS Related Parameters
3. Discussion
4. Material and Methods
4.1. Patients and Clinical Characteristics
4.2. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Rouleau, G.A.; Merel, P.; Lutchman, M.; Sanson, M.; Zucman, J.; Marineau, C.; Hoang-Xuan, K.; Demczuk, S.; Desmaze, C.; Plougastel, B.; et al. Alteration in a new gene encoding a putative membrane-organizing protein causes neuro-fibromatosis type 2. Nature 1993, 363, 515–521. [Google Scholar] [CrossRef] [PubMed]
- Trofatter, J.A.; MacCollin, M.M.; Rutter, J.L.; Murrell, J.R.; Duyao, M.P.; Parry, D.M.; Eldridge, R.; Kley, N.; Menon, A.G.; Pulaski, K.; et al. A novel moesin-, ezrin-, radixin-like gene is a candidate for the neurofibromatosis 2 tumor suppressor. Cell 1993, 75, 826. [Google Scholar] [CrossRef]
- Asthagiri, A.R.; Parry, D.M.; Butman, J.A.; Kim, H.J.; Tsilou, E.T.; Zhuang, Z.; Lonser, R.R. Neurofibromatosis type 2. Lancet 2009, 373, 1974–1986. [Google Scholar] [CrossRef] [Green Version]
- Parry, D.M.; Eldridge, R.; Kaiser-Kupfer, M.I.; Bouzas, E.A.; Pikus, A.; Patronas, N. Neurofibromatosis 2 (NF2): Clinical characteristics of 63 affected individuals and clinical evidence for heterogeneity. Am. J. Med. Genet. 1994, 52, 450–461. [Google Scholar] [CrossRef]
- Gugel, I.; Grimm, F.; Teuber, C.; Kluwe, L.; Mautner, V.F.; Tatagiba, M.; Schuhmann, M.U. Management of NF2-associated vestibular schwannomas in children and young adults: Influence of surgery and clinical factors on tumor volume and growth rate. J. Neurosurg. Pediatr. 2019, 1–9. [Google Scholar] [CrossRef]
- Plotkin, S.R.; Singh, M.A.; O′Donnell, C.C.; Harris, G.J.; McClatchey, A.I.; Halpin, C. Audiologic and radiographic response of NF2-related vestibular schwannoma to erlotinib therapy. Nat. Clin. Pract. Oncol. 2008, 5, 487–491. [Google Scholar] [CrossRef]
- Plotkin, S.R.; Stemmer-Rachamimov, A.O.; Barker, F.G., 2nd; Halpin, C.; Padera, T.P.; Tyrrell, A.; Sorensen, A.G.; Jain, R.K.; di Tomaso, E. Hearing improvement after bevacizumab in patients with neurofibromatosis type 2. N. Engl. J. Med. 2009, 361, 358–367. [Google Scholar] [CrossRef] [Green Version]
- Plotkin, S.R.; Merker, V.L.; Halpin, C.; Jennings, D.; McKenna, M.J.; Harris, G.J.; Barker, F.G., 2nd. Bevacizumab for progressive vestibular schwannoma in neurofibromatosis type 2: A retrospective review of 31 patients. Otol. Neurotol. 2012, 33, 1046–1052. [Google Scholar] [CrossRef]
- Gugel, I.; Kluwe, L.; Zipfel, J.; Teuber, C.; Tatagiba, M.; Mautner, V.F.; Schuhmann, M.U.; Grimm, F. Minimal Effect of Bevacizumab Treatment on Residual Vestibular Schwannomas after Partial Resection in Young Neurofibromatosis Type 2 Patients. Cancers 2019, 11, 1862. [Google Scholar] [CrossRef] [Green Version]
- Blakeley, J.O.; Evans, D.G.; Adler, J.; Brackmann, D.; Chen, R.; Ferner, R.E.; Hanemann, C.O.; Harris, G.; Huson, S.M.; Jacob, A.; et al. Consensus recommendations for current treatments and accelerating clinical trials for patients with neurofibromatosis type 2. Am. J. Med. Genet. Part A 2012, 158A, 24–41. [Google Scholar] [CrossRef] [Green Version]
- Choi, J.W.; Lee, J.Y.; Phi, J.H.; Wang, K.C.; Chung, H.T.; Paek, S.H.; Kim, D.G.; Park, S.H.; Kim, S.K. Clinical course of vestibular schwannoma in pediatric neurofibromatosis Type 2. J. Neurosurg. Pediatr. 2014, 13, 650–657. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Evans, D.G.; Birch, J.M.; Ramsden, R.T. Paediatric presentation of type 2 neurofibromatosis. Arch. Dis. Child. 1999, 81, 496–499. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matsuo, M.; Ohno, K.; Ohtsuka, F. Characterization of early onset neurofibromatosis type 2. Brain Dev. 2014, 36, 148–152. [Google Scholar] [CrossRef] [PubMed]
- Evans, D.G.R.; Salvador, H.; Chang, V.Y.; Erez, A.; Voss, S.D.; Druker, H.; Scott, H.S.; Tabori, U. Cancer and Central Nervous System Tumor Surveillance in Pediatric Neurofibromatosis 2 and Related Disorders. Clin. Cancer Res. 2017, 23, e54–e61. [Google Scholar] [CrossRef] [Green Version]
- Ruggieri, M.; Gabriele, A.L.; Polizzi, A.; Salpietro, V.; Nicita, F.; Pavone, P.; Platania, N.; Milone, P.; Distefano, A.; Privitera, G.; et al. Natural history of neurofibromatosis type 2 with onset before the age of 1 year. Neurogenetics 2013, 14, 89–98. [Google Scholar] [CrossRef]
- Mautner, V.F.; Tatagiba, M.; Guthoff, R.; Samii, M.; Pulst, S.M. Neurofibromatosis 2 in the pediatric age group. Neurosurgery 1993, 33, 92–96. [Google Scholar] [CrossRef]
- Mautner, V.; Hazim, W.; Pohlmann, K.; Berger, R.; Kluwe, L.; Haase, W. Ophthalmologic spectrum of neurofibromatosis type 2 in childhood. Klin. Mon. Fur Augenheilkd. 1996, 208, 58–62. [Google Scholar] [CrossRef]
- Gaudioso, C.; Listernick, R.; Fisher, M.J.; Campen, C.J.; Paz, A.; Gutmann, D.H. Neurofibromatosis 2 in children presenting during the first decade of life. Neurology 2019, 93, e964–e967. [Google Scholar] [CrossRef]
- MacCollin, M.; Mautner, V.F. The diagnosis and management of neurofibromatosis 2 in childhood. Semin. Pediatr. Neurol. 1998, 5, 243–252. [Google Scholar] [CrossRef]
- Gugel, I.; Grimm, F.; Teuber, C.; Zipfel, J.; Tatagiba, M.; Mautner, V.F.; Schuhmann, M.U.; Kluwe, L. Presenting symptoms in children with neurofibromatosis type 2. Childs Nerv. Syst. 2020. [Google Scholar] [CrossRef]
- Evans, D.G.; Huson, S.M.; Donnai, D.; Neary, W.; Blair, V.; Newton, V.; Harris, R. A clinical study of type 2 neurofibromatosis. Q. J. Med. 1992, 84, 603–618. [Google Scholar] [PubMed]
- Gugel, I.; Mautner, V.F.; Kluwe, L.; Tatagiba, M.S.; Schuhmann, M.U. Cerebrovascular Insult as Presenting Symptom of Neurofibromatosis Type 2 in Children, Adolescents, and Young Adults. Front. Neurol. 2018, 9, 733. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fan, D.; Ren, H.; Danzeng, D.; Li, H.; Wang, P. Influence of high-altitude hypoxic environments on the survival of cochlear hair cells and spiral ganglion neurons in rats. Biomed Rep. 2016, 5, 681–685. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tabuchi, K.; Nishimura, B.; Tanaka, S.; Hayashi, K.; Hirose, Y.; Hara, A. Ischemia-reperfusion injury of the cochlea: Pharmacological strategies for cochlear protection and implications of glutamate and reactive oxygen species. Curr. Neuropharmacol. 2010, 8, 128–134. [Google Scholar] [CrossRef] [Green Version]
- Dilwali, S.; Landegger, L.D.; Soares, V.Y.; Deschler, D.G.; Stankovic, K.M. Secreted Factors from Human Vestibular Schwannomas Can Cause Cochlear Damage. Sci. Rep. 2015, 5, 18599. [Google Scholar] [CrossRef]
- Asthagiri, A.R.; Vasquez, R.A.; Butman, J.A.; Wu, T.; Morgan, K.; Brewer, C.C.; King, K.; Zalewski, C.; Kim, H.J.; Lonser, R.R. Mechanisms of hearing loss in neurofibromatosis type 2. PLoS ONE 2012, 7, e46132. [Google Scholar] [CrossRef]
- Gugel, I.; Grimm, F.; Liebsch, M.; Zipfel, J.; Teuber, C.; Kluwe, L.; Mautner, V.F.; Tatagiba, M.; Schuhmann, M.U. Impact of Surgery on Long-Term Results of Hearing in Neurofibromatosis Type-2 Associated Vestibular Schwannomas. Cancers 2019, 11, 1376. [Google Scholar] [CrossRef] [Green Version]
- Morris, K.A.; Golding, J.F.; Axon, P.R.; Afridi, S.; Blesing, C.; Ferner, R.E.; Halliday, D.; Jena, R.; Pretorius, P.M.; The UK NF2 Research Group; et al. Bevacizumab in neurofibromatosis type 2 (NF2) related vestibular schwannomas: A nationally coordinated approach to delivery and prospective evaluation. Neurooncol. Pract. 2016, 3, 281–289. [Google Scholar] [CrossRef] [Green Version]
- Plotkin, S.R.; Duda, D.G.; Muzikansky, A.; Allen, J.; Blakeley, J.; Rosser, T.; Campian, J.L.; Clapp, D.W.; Fisher, M.J.; Tonsgard, J.; et al. Multicenter, Prospective, Phase II and Biomarker Study of High-Dose Bevacizumab as Induction Therapy in Patients With Neurofibromatosis Type 2 and Progressive Vestibular Schwannoma. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2019, 37, 3446–3454. [Google Scholar] [CrossRef]
- Shinya, Y.; Hasegawa, H.; Shin, M.; Sugiyama, T.; Kawashima, M.; Takahashi, W.; Iwasaki, S.; Kashio, A.; Nakatomi, H.; Saito, N. Long-Term Outcomes of Stereotactic Radiosurgery for Vestibular Schwannoma Associated with Neurofibromatosis Type 2 in Comparison to Sporadic Schwannoma. Cancers 2019, 11, 1498. [Google Scholar] [CrossRef] [Green Version]
- Otsuka, G.; Saito, K.; Nagatani, T.; Yoshida, J. Age at symptom onset and long-term survival in patients with neurofibromatosis Type 2. J. Neurosurg. 2003, 99, 480–483. [Google Scholar] [CrossRef] [PubMed]
- Baser, M.E.; Friedman, J.M.; Aeschliman, D.; Joe, H.; Wallace, A.J.; Ramsden, R.T.; Evans, D.G. Predictors of the risk of mortality in neurofibromatosis 2. Am. J. Hum. Genet. 2002, 71, 715–723. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Evans, D.G.; Trueman, L.; Wallace, A.; Collins, S.; Strachan, T. Genotype/phenotype correlations in type 2 neurofibromatosis (NF2): Evidence for more severe disease associated with truncating mutations. J. Med. Genet. 1998, 35, 450–455. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anand, G.; Vasallo, G.; Spanou, M.; Thomas, S.; Pike, M.; Kariyawasam, D.S.; Mehta, S.; Parry, A.; Durie-Gair, J.; Nicholson, J.; et al. Diagnosis of sporadic neurofibromatosis type 2 in the paediatric population. Arch. Dis. Child. 2018, 103, 463–469. [Google Scholar] [CrossRef] [PubMed]
- Sisk, R.A.; Berrocal, A.M.; Schefler, A.C.; Dubovy, S.R.; Bauer, M.S. Epiretinal membranes indicate a severe phenotype of neurofibromatosis type 2. Retina 2010, 30, S51–S58. [Google Scholar] [CrossRef] [PubMed]
- Ruggieri, M.; Iannetti, P.; Polizzi, A.; La Mantia, I.; Spalice, A.; Giliberto, O.; Platania, N.; Gabriele, A.L.; Albanese, V.; Pavone, L. Earliest clinical manifestations and natural history of neurofibromatosis type 2 (NF2) in childhood: A study of 24 patients. Neuropediatrics 2005, 36, 21–34. [Google Scholar] [CrossRef]
- Sheeladevi, S.; Lawrenson, J.G.; Fielder, A.R.; Suttle, C.M. Global prevalence of childhood cataract: A systematic review. Eye 2016, 30, 1160–1169. [Google Scholar] [CrossRef] [Green Version]
- Han, K.E.; Baek, S.H.; Kim, S.H.; Lim, K.H.; Epidemiologic Survey Committee of the Korean Ophthalmological Society. Prevalence and risk factors of strabismus in children and adolescents in South Korea: Korea National Health and Nutrition Examination Survey, 2008–2011. PLoS ONE 2018, 13, e0191857. [Google Scholar] [CrossRef] [Green Version]
- Baser, M.E.; Friedman, J.M.; Wallace, A.J.; Ramsden, R.T.; Joe, H.; Evans, D.G. Evaluation of clinical diagnostic criteria for neurofibromatosis 2. Neurology 2002, 59, 1759–1765. [Google Scholar] [CrossRef]
- Mautner, V.F.; Lindenau, M.; Baser, M.E.; Kluwe, L.; Gottschalk, J. Skin abnormalities in neurofibromatosis 2. Arch. Dermatol. 1997, 133, 1539–1543. [Google Scholar] [CrossRef]
- Nunes, F.; MacCollin, M. Neurofibromatosis 2 in the pediatric population. J. Child Neurol. 2003, 18, 718–724. [Google Scholar] [CrossRef] [PubMed]
- Pathmanaban, O.N.; Sadler, K.V.; Kamaly-Asl, I.D.; King, A.T.; Rutherford, S.A.; Hammerbeck-Ward, C.; McCabe, M.G.; Kilday, J.P.; Beetz, C.; Poplawski, N.K.; et al. Association of Genetic Predisposition with Solitary Schwannoma or Meningioma in Children and Young Adults. JAMA Neurol. 2017, 74, 1123–1129. [Google Scholar] [CrossRef] [PubMed]
- Perry, A.; Giannini, C.; Raghavan, R.; Scheithauer, B.W.; Banerjee, R.; Margraf, L.; Bowers, D.C.; Lytle, R.A.; Newsham, I.F.; Gutmann, D.H. Aggressive phenotypic and genotypic features in pediatric and NF2-associated meningiomas: A clinicopathologic study of 53 cases. J. Neuropathol. Exp. Neurol. 2001, 60, 994–1003. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, T.; Igarashi, H.; Ito, T.; Jensen, R.T. Important of case-reports/series, in rare diseases: Using neuroendocrine tumors as an example. World J. Clin. Cases 2014, 2, 608–613. [Google Scholar] [CrossRef]
- Carey, J.C. The importance of case reports in advancing scientific knowledge of rare diseases. Adv. Exp. Med. Biol. 2010, 686, 77–86. [Google Scholar] [CrossRef]
- Baser, M.E.; Friedman, J.M.; Joe, H.; Shenton, A.; Wallace, A.J.; Ramsden, R.T.; Evans, D.G. Empirical development of improved diagnostic criteria for neurofibromatosis 2. Genet. Med. 2011, 13, 576–581. [Google Scholar] [CrossRef] [Green Version]
- Samii, M.; Matthies, C. Management of 1000 vestibular schwannomas (acoustic neuromas): Hearing function in 1000 tumor resections. Neurosurgery 1997, 40, 248–260; discussion 260–242. [Google Scholar] [CrossRef]


{kind=link}
| Age at Time of Diagnosis in Years | All Age Groups | ≤18 | >18 |
|---|---|---|---|
| No. of patients/tumors | 106/194 | 61/115 | 45/79 |
| Sex (No. of female/male) | 55/51 | 31/30 | 24/21 |
| Age at in year (mean ± SD, range) | |||
| Onset | 16 ± 11, 0–46 | 9 ± 6, 0–18 | 25 ± 9, 0–46 |
| Diagnosis | 18 ± 10, 1–44 | 11 ± 5, 1–18 | 29 ± 7, 19–44 |
| Deafness | 26 ± 11, 13–59, n = 44 | 19 ± 5, 13–31, n = 24 | |
| 35 ± 11, 22–59, | |||
| n = 20 | |||
| Time of surgery per ear | 24 ± 10, 9–56, n = 121 | 18 ± 5, 9–30, n = 73 | 33 ± 8, 22–56, n = 48 |
| At beginning of hearing loss | 24 ± 11, 7–58, n = 135 | 18 ± 5, 7–30, n = 81 | 34 ± 9, 19–58, n = 54 |
Family history of NF2
| 21/85 | 12/49 | 9/36 |
| Detected mutation types | In 49 patients | In 41 patients | In 8 patients |
| Splicing mutations | 11 | 8 | 3 |
| Nonsense mutations | 11 | 8 | 3 |
| Frameshifting mutations | 14 | 14 | 0 |
| Large genome alteration | 1 | 1 | 0 |
| Missense mutation | 2 | 0 | 2 |
| Large deletion | 5 | 5 | 0 |
| Mosaic | 13 patients | 2 patients | 11 patients |
| No mutation detected in blood and tumor DNA | 7 patients | 3 patients | 4 patients |
| At presentation (mean ± SD, range) | |||
| Tumor volume in cm3 | |||
| 2.86 ± 5.73, 0–32.72, | 2.39 ± 5.61, 0–33, | 3.55 ± 5.83, 0.02–28.05, | |
| n = 194 | n = 115 | n = 79 | |
| Growth rate in cm3/year | |||
| 0.82 ± 1.95, −1.66–14.96, | 0.72 ± 1.71, −1.66–10.84, | 0.96 ± 2.24, −0.08–14.96, | |
| n = 159 | n = 93 | n = 66 | |
| PTA in dB | |||
| 31.22 ± 37.81, 1–130, | 21.45 ± 29.4, 1.25–130, | 44.91 ± 43.61, 1–130, | |
| n = 185 | n = 108 | n = 77 | |
| SDS in % | |||
| 77.94 ± 35.85, 0–100, | 86.93 ± 28.87, 0–100, | 65.39 ± 40.56, 0–100, | |
| n = 183 | n = 106 | n = 77 |
| First Symptom(s)/Sign(s) | In All | ≤18 | >18 |
|---|---|---|---|
| Ophthalmological | 36 | 31 | 5 |
| Visual impairment/loss *a | 16 | 13 | 3 |
| Strabismus *b | 17 | 15 | 2 |
| Proptosis *c | 3 | 3 | 0 |
| VS related symptoms | 58 | 19 | 39 |
| Hypacusis | 26 | 9 | 17 |
| Sudden hearing loss | 5 | 0 | 5 |
| Tinnitus | 10 | 1 | 9 |
| Balance disorders | 5 | 3 | 2 |
| Dizziness | 5 | 1 | 4 |
| Hoarseness | 1 | 1 | 0 |
| Facial palsy (due to VS) | 6 | 4 | 2 |
| Non-VS related neurological symptoms | 31 | 18 | 19 |
| Seizures | 5 | 3 | 2 |
| Motor deficits | 9 | 7 | 2 |
| Sensory deficits | 2 | 2 | 0 |
| Dysarthria | 2 | 1 | 1 |
| Fine motor skill disorder | 1 | 0 | 1 |
| Facial palsy (non-VS related) | 4 | 2 | 2 |
| Muscle wasting *d | 5 | 2 | 3 |
| Memory impairment *e | 1 | 1 | 0 |
| Vomiting/nausea *f | 2 | 0 | 2 |
| Pain | 11 | 4 | 7 |
| Back-/neck-/and radiating pain | 9 | 4 | 5 |
| Headache | 2 | 0 | 2 |
| Family history/incidental finding | 10 | 5 | 5 |
| Positive family history | 5 | 3 | 2 |
| Incidental finding (asymptomatic) | 6 | 2 | 4 |
| Mono-/Polysymptomatic | |||
| Monosymptomatic patients | 42 | 23 | 19 |
| Polysymptomatic patients (≥2 symptoms) | 58 | 35 | 23 |
| Asymptomatic | 6 | 3 | 3 |
| Presenting Symptom (Related) Pathology/Feature | All | ≤18 | >18 |
|---|---|---|---|
| Vestibular schwannoma (VS) | 58(55%) | 19(31%) | 39(87%) |
| Cutaneous (plexiform)/subcutaneous schwannoma | 37(35%) | 25(41%) | 12(27%) |
| Intracranial meningioma *a | 12(11%) | 7(11%) | 5(11%) |
| Cataract | 11(10%) | 10(16%) | 1(2%) |
| Retinal Hamartoma/Maculopathy | 9(8%) | 10(16%) | 5(11%) |
| Intracranial non-VS schwannoma *b | 6(6%) | 4(7%) | 2(4%) |
| Neuropathy/Muscle wasting | 4(4%) | 3(5%) | 1(2%) |
| Café au lait spots | 3(3%) | 1(2%) | 2(4%) |
| Ischemic brainstem stroke | 2(2%) | 1(2%) | 1(2%) |
| Spinal extramedullary tumors (schwannoma, meningioma) | 2(2%) | 2(3%) | 0 |
| Spinal intramedullary tumor (ependymoma) | 2(2%) | 1(2%) | 1(2%) |
| SAH bleeding due to aneurysm | 1(1%) | 1(2%) | 0 |
| Cerebral dysplasia | 1(1%) | 1(2%) | 0 |
| Bifrontal angiomatosis | 1(1%) | 1(2%) | 0 |
| Positive Correlation of Age at Onset with | |
| GR at presentation in cm3/year | r = 0.065, p = 0.217 |
| Volume at presentation in cm3 | r = 0.150, p = 0.034 |
| PTA at presentation in dB | r = 0.283, p = 0.0001 |
| Age at deafness in years | r = 0.814, p = 0.0001 |
| Age at time of surgery in years | r = 0.835, p = 0.0001 |
| Age at beginning of hearing loss in years | r = 0.816, p = 0.0001 |
| Negative (Inversed) Correlation of Age at onset with | |
| SDS at diagnosis in % | r = −0.252, p = 0.001 |
| Variable | U | z | p | Median Non-VS Presenting Symptom | Median VS Presenting Symptom |
|---|---|---|---|---|---|
| GR at presentation | 2871 | −0.469 | 0.639 | 0.138 cm3/year | 0.169 cm3/year |
| Volume at presentation | 3743 | −1.758 | 0.079 | 0.389 cm3 | 0.905 cm3 |
| PTA at presentation | 3152 | −2.727 | 0.006 | 10 dB | 25 dB |
| SDS at presentation | 3081 | −2.852 | 0.004 | 100% | 95% |
| Age at deafness | 250 | 1.034 | 0.301 | 22 years | 25 years |
| Age at time of surgery | 2272 | 2.727 | 0.006 | 19 years | 24 years |
| Age at beginning of hearing loss | 2711 | 2.361 | 0.018 | 19 years | 23 years |
| GR postoperative | 1332 | −1.745 | 0.081 | 0.276 cm3/year | 0.069 cm3/year |
| PTA postoperative | 1779 | 2.689 | 0.007 | 26 dB | 55.25 dB |
| SDS postoperative | 1006 | −2.175 | 0.03 | 85% | 50% |
| GR under BVZ | 538 | 0.609 | 0.542 | 0.066 cm3/year | 0.063 cm3/year |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gugel, I.; Grimm, F.; Zipfel, J.; Teuber, C.; Ernemann, U.; Kluwe, L.; Tatagiba, M.; Mautner, V.-F.; Schuhmann, M.U. Age at Onset and Presenting Symptoms of Neurofibromatosis Type 2 as Prognostic Factors for Clinical Course of Vestibular Schwannomas. Cancers 2020, 12, 2355. https://doi.org/10.3390/cancers12092355
Gugel I, Grimm F, Zipfel J, Teuber C, Ernemann U, Kluwe L, Tatagiba M, Mautner V-F, Schuhmann MU. Age at Onset and Presenting Symptoms of Neurofibromatosis Type 2 as Prognostic Factors for Clinical Course of Vestibular Schwannomas. Cancers. 2020; 12(9):2355. https://doi.org/10.3390/cancers12092355
Chicago/Turabian StyleGugel, Isabel, Florian Grimm, Julian Zipfel, Christian Teuber, Ulrike Ernemann, Lan Kluwe, Marcos Tatagiba, Victor-Felix Mautner, and Martin Ulrich Schuhmann. 2020. "Age at Onset and Presenting Symptoms of Neurofibromatosis Type 2 as Prognostic Factors for Clinical Course of Vestibular Schwannomas" Cancers 12, no. 9: 2355. https://doi.org/10.3390/cancers12092355