A Novel Technique to Improve Anastomotic Perfusion Prior to Esophageal Surgery: Hybrid Ischemic Preconditioning of the Stomach. Preclinical Efficacy Proof in a Porcine Survival Model

 ,
,  , , ,
, , , 
Abstract
:Simple Summary
Abstract
1. Introduction
2. Results
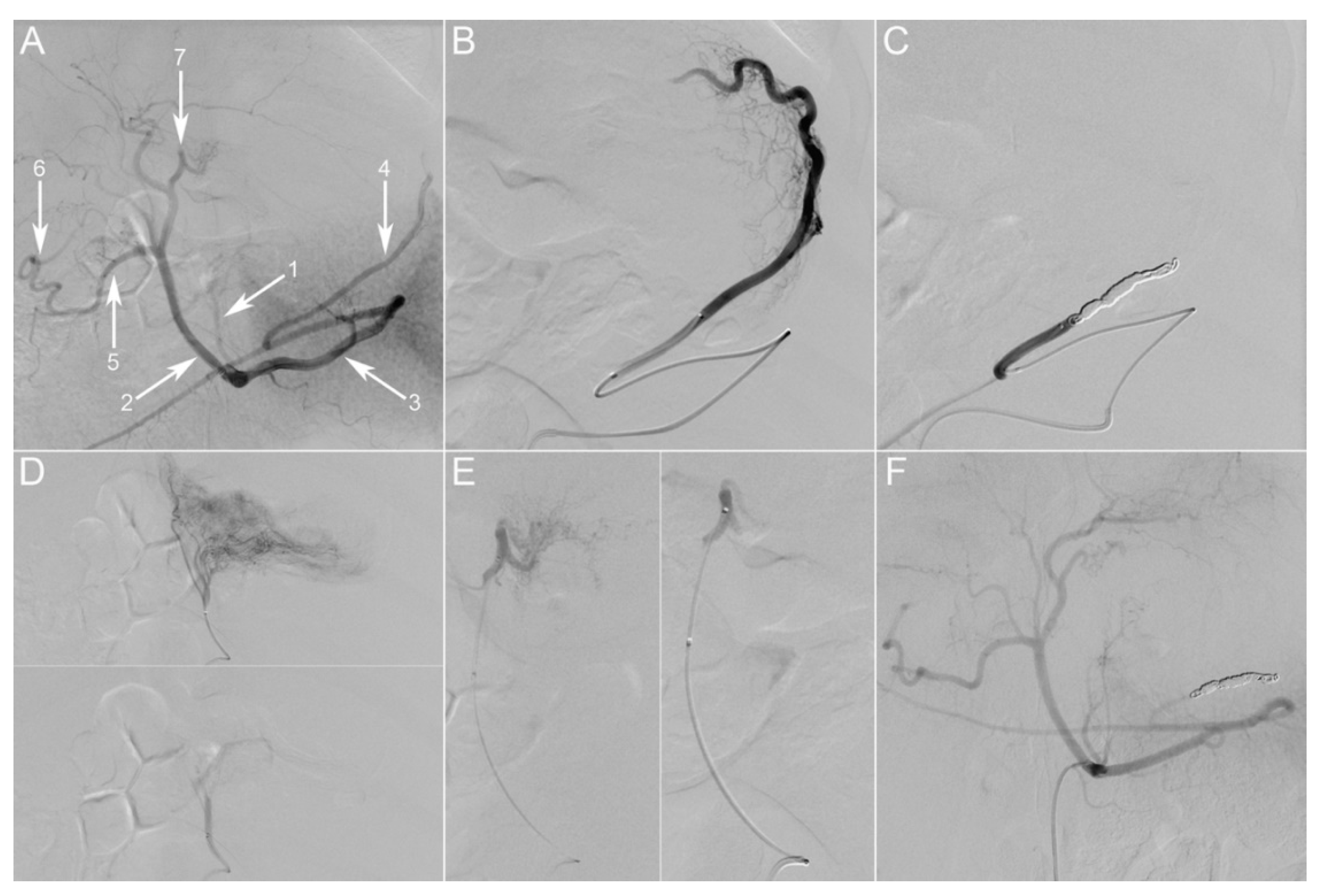
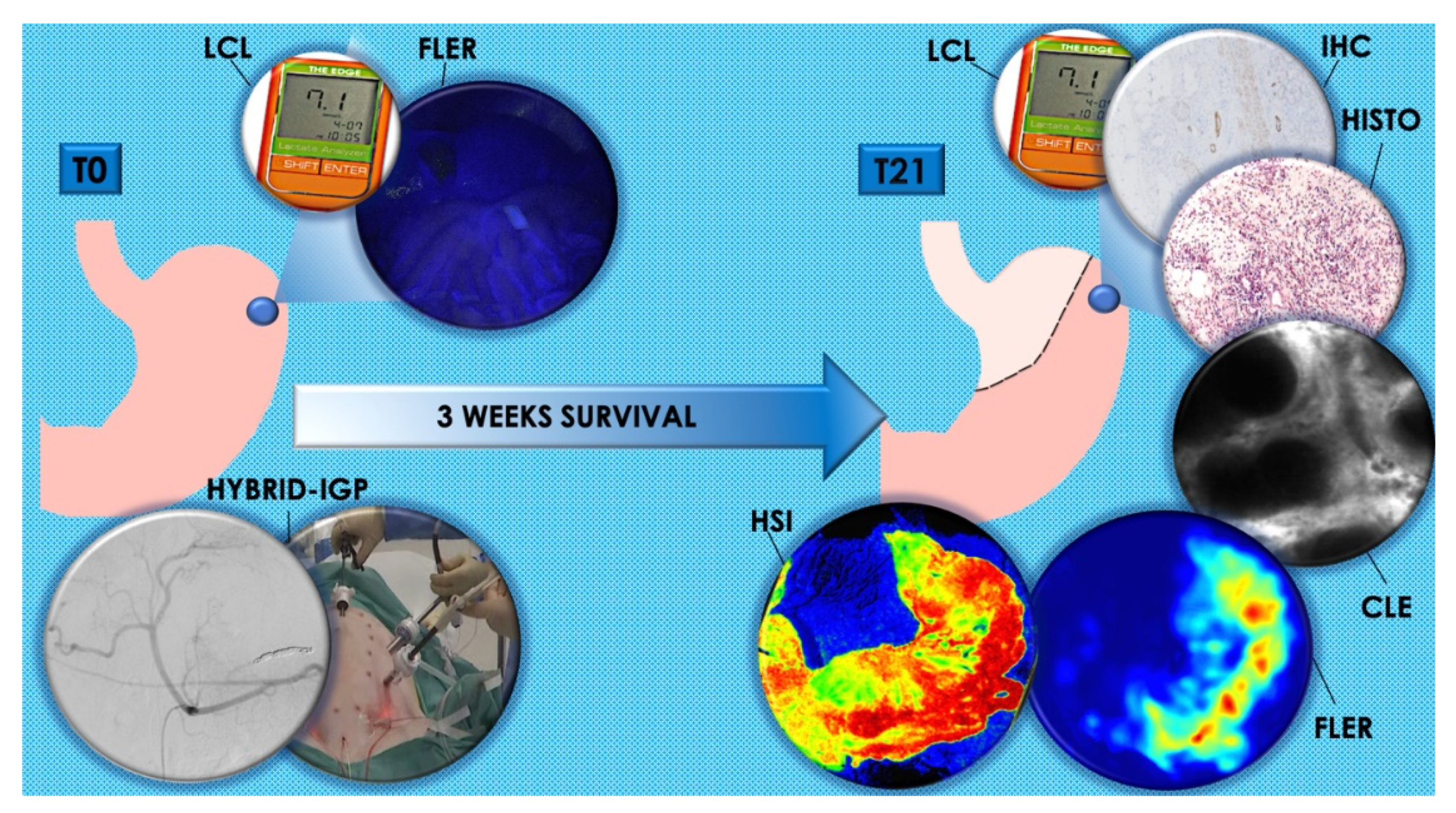
2.1. T0
FLER and LCL
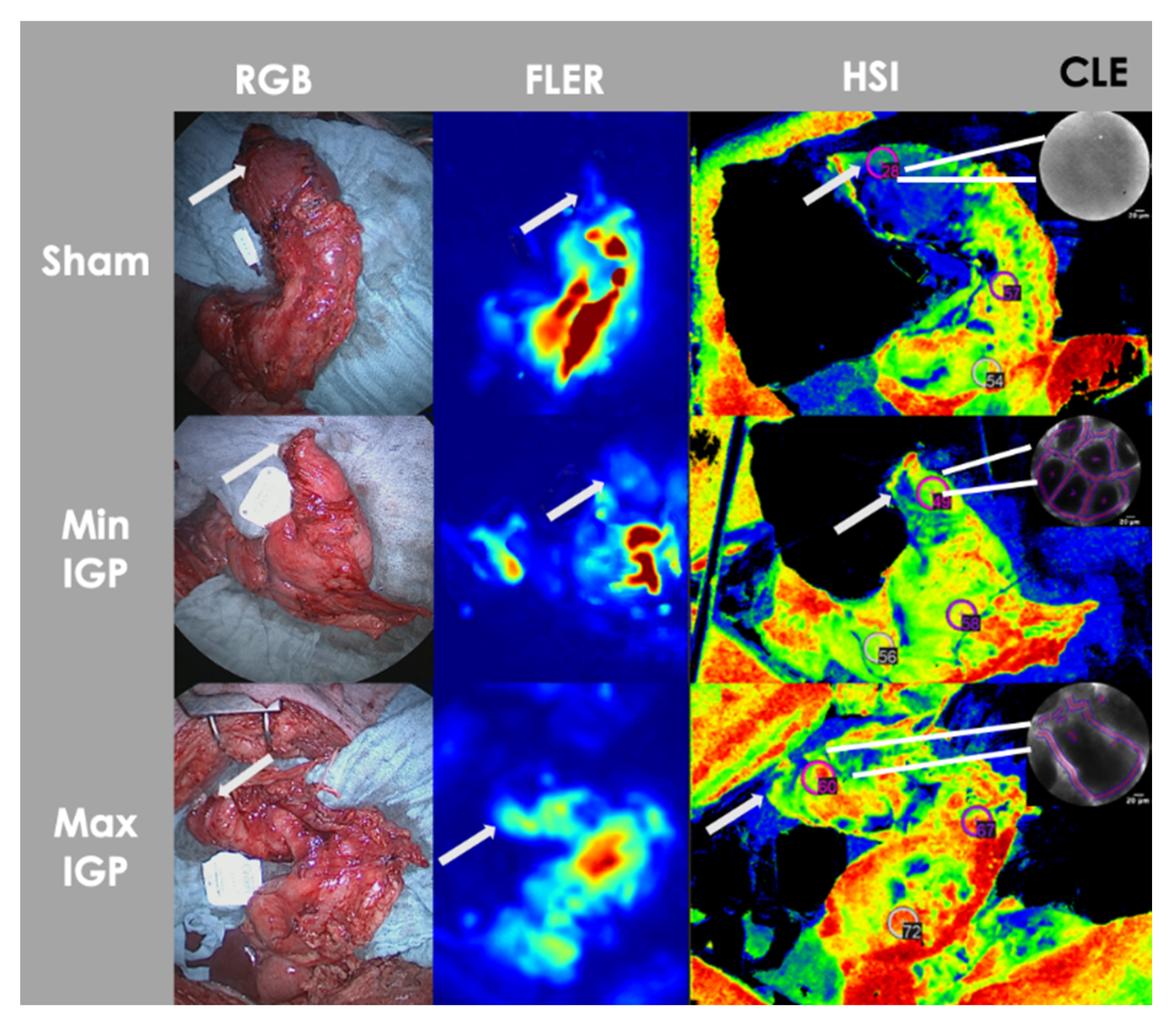
2.2. T21
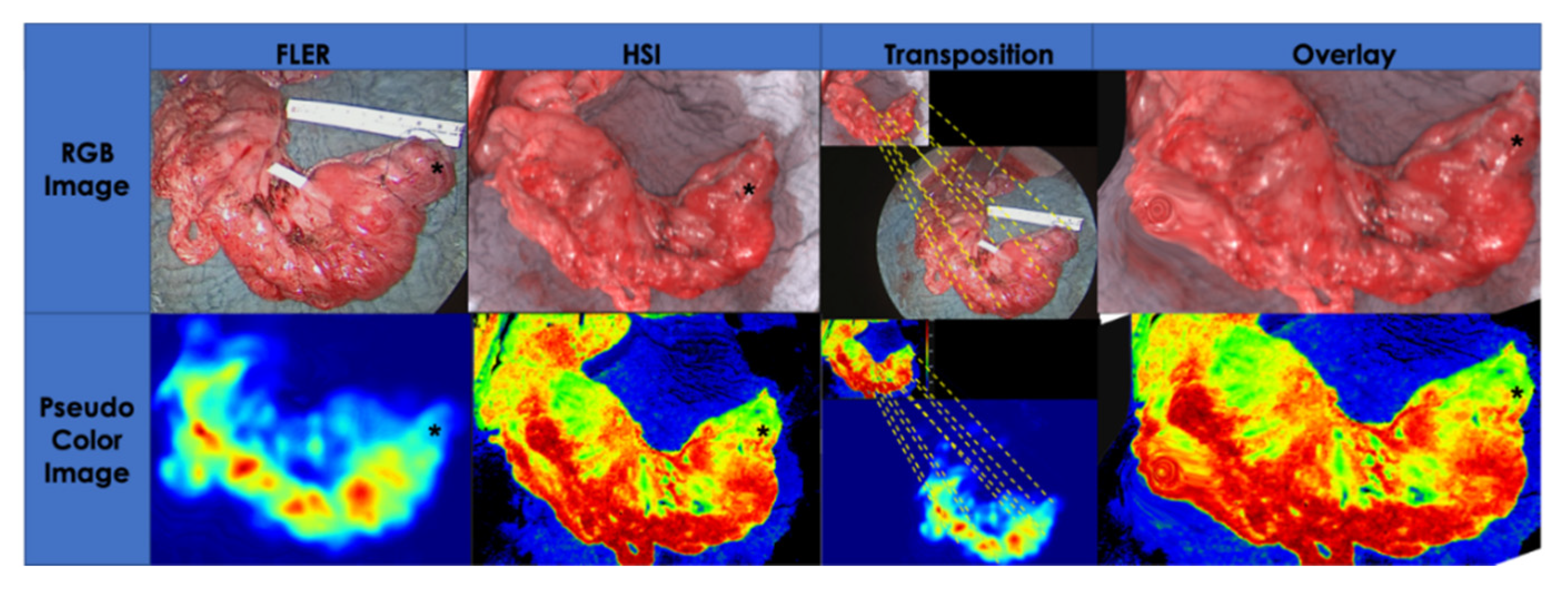
2.2.1. Serosal Quantitative Optical Imaging Measurements: HSI and FLER
2.2.2. Mucosal Quantitative Optical Imaging Measurement: CLE
2.2.3. LCL Sampling
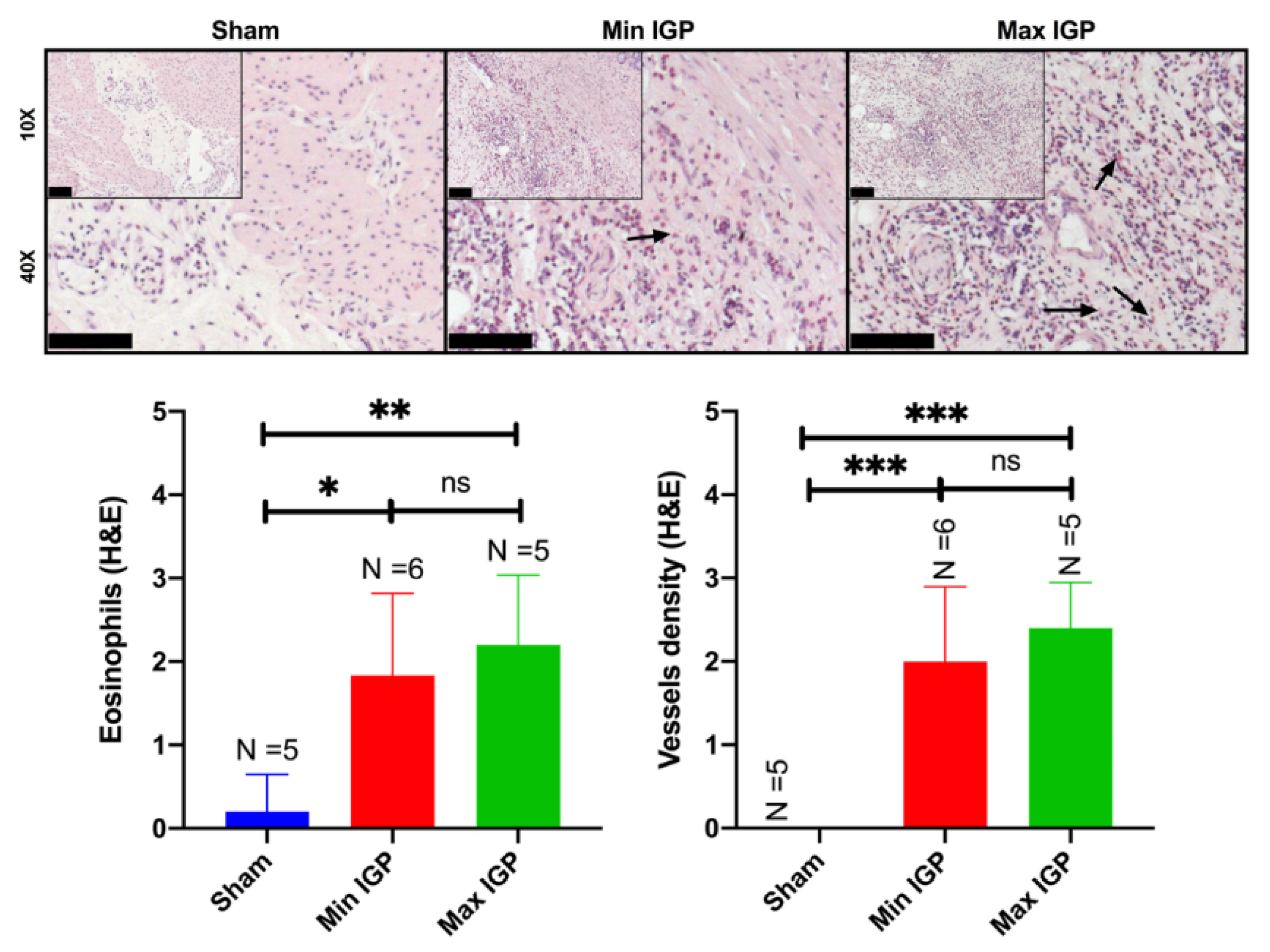
2.2.4. Histology: Capillary Density Score and Eosinophil Count Score
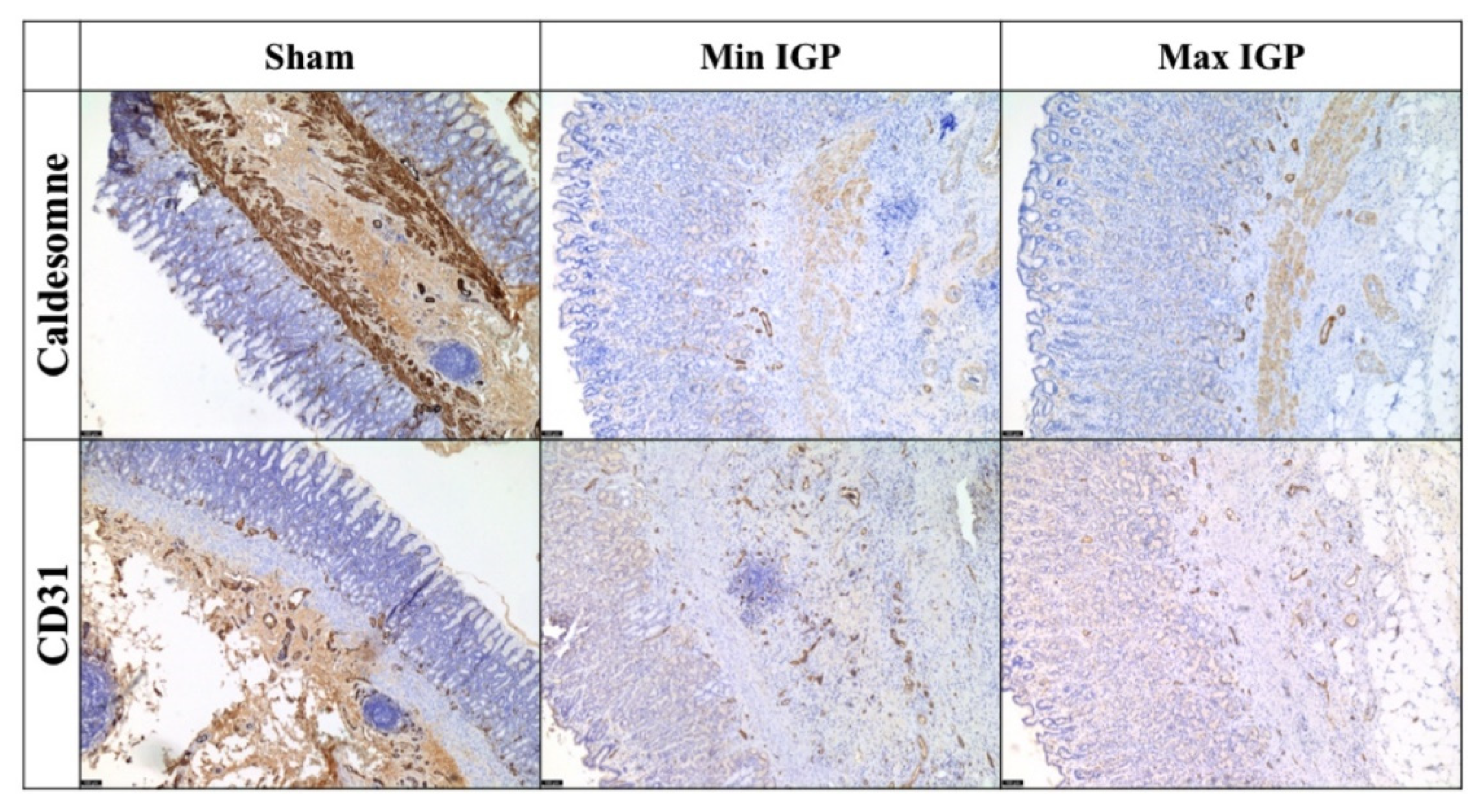
2.2.5. Immunohistochemistry Quantification
3. Discussion
4. Materials and Methods
4.1. Animals Characteristics and Experimental Set-up
4.1.1. T0 Procedure
Ischemic Gastric Preconditioning
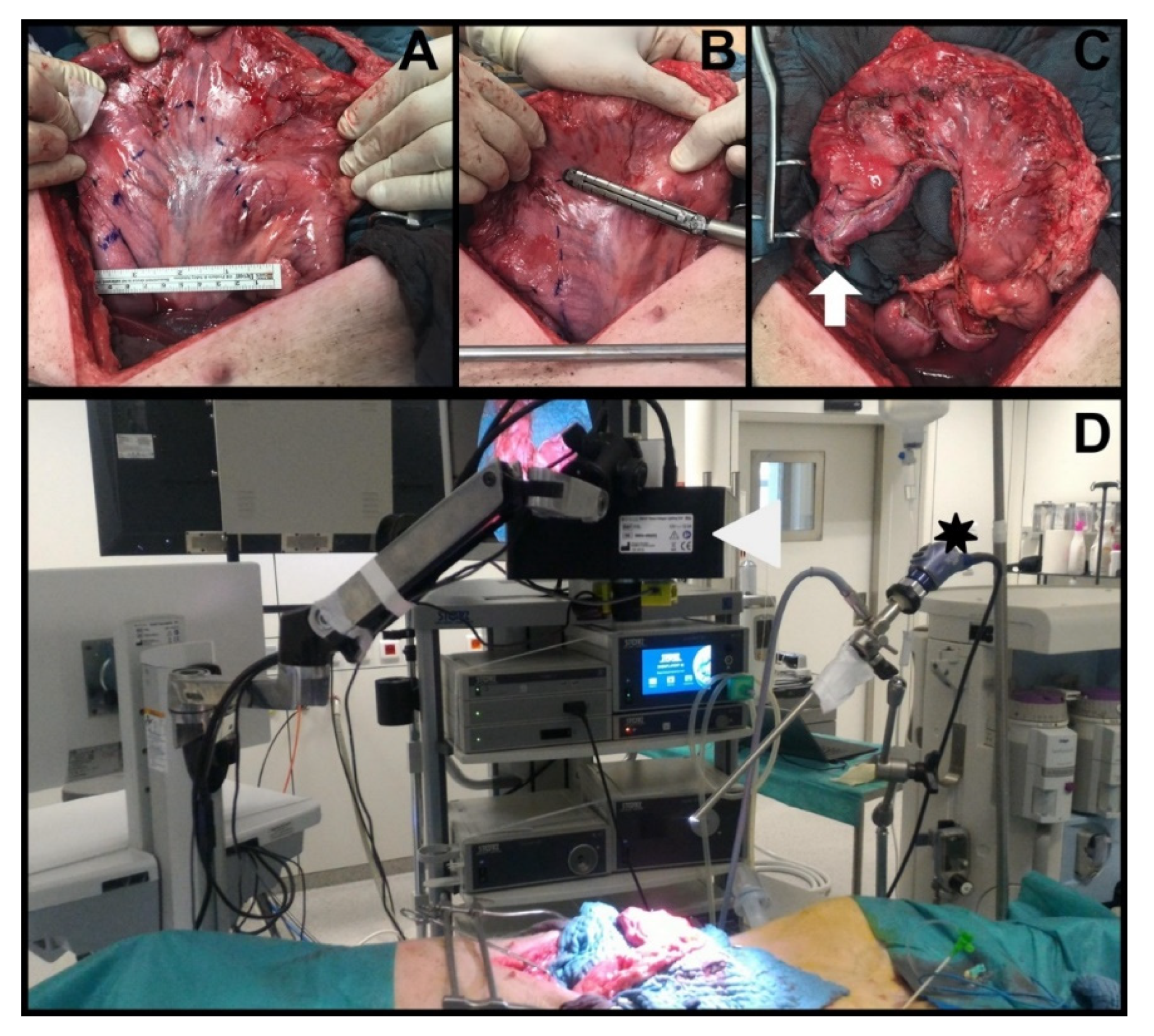
Fluorescence-Based Enhanced Reality (FLER)
Local Capillary Lactate (LCL) Measurement
4.1.2. T21 Procedure
Gastric Conduit Formation
Serosal Quantitative Optical Imaging Measurements: HSI and FLER
Mucosal Quantitative Optical Imaging Measurement: Confocal Laser Endomicroscopy (CLE)
LCL Sampling
Histology Scores: Vessel Count and Eosinophils Count
Immunohistochemistry Analysis
4.2. Sample Size Calculation and Statistical Analysis
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Hagen, P.; Hulshof, M.; Van Lanschot, J.; Steyerberg, E.; Henegouwen, M.V.B.; Wijnhoven, B.; Richel, D.; Nieuwenhuijzen, G.; Hospers, G.; Bonenkamp, J.; et al. Preoperative chemoradiotherapy for esophageal or junctional cancer. N. Engl. J. Med. 2012, 366, 2074–2084. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Low, D.E.; Kuppusamy, M.K.; Alderson, D.; Cecconello, I.; Chang, A.C.; Darling, G.; Davies, A.; D’Journo, X.B.; Gisbertz, S.S.; Griffin, S.M.; et al. Benchmarking complications associated with esophagectomy. Ann. Surg. 2019, 269, 291–298. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Booka, E.; Takeuchi, H.; Suda, K.; Fukuda, K.; Nakamura, R.; Wada, N.; Kawakubo, H.; Kitagawa, Y. Meta-analysis of the impact of postoperative complications on survival after oesophagectomy for cancer. BJS Open 2018, 2, 276–284. [Google Scholar] [CrossRef] [PubMed]
- Markar, S.; Gronnier, C.; Duhamel, A.; Mabrut, J.-Y.; Bail, J.-P.; Carrere, N.; Lefevre, J.H.; Brigand, C.; Vaillant, J.-C.; Adham, M.; et al. The impact of severe anastomotic leak on long-term survival and cancer recurrence after surgical resection for esophageal malignancy. Ann. Surg. 2015, 262, 972–980. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morse, B.C.; Simpson, J.P.; Jones, Y.R.; Johnson, B.L.; Knott, B.M.; Kotrady, J.A. Determination of independent predictive factors for anastomotic leak: Analysis of 682 intestinal anastomoses. Am. J. Surg. 2013, 206, 950–956. [Google Scholar] [CrossRef]
- Kassis, E.S.; Kosinski, A.S.; Ross, P., Jr.; Koppes, K.E.; Donahue, J.M.; Daniel, V.C. Predictors of anastomotic leak after esophagectomy: An analysis of the society of thoracic surgeons general thoracic database. Ann. Thorac. Surg. 2013, 96, 1919–1926. [Google Scholar] [CrossRef]
- Van Rossum, P.S.; Haverkamp, L.; Verkooijen, H.M.; van Leeuwen, M.S.; van Hillegersberg, R.; Ruurda, J.P. Calcification of arteries supplying the gastric tube: A new risk factor for anastomotic leakage after esophageal surgery. Radiology 2015, 274, 124–132. [Google Scholar] [CrossRef]
- Zehetner, J.; DeMeester, S.R.; Alicuben, E.T.; Oh, D.S.; Lipham, J.C.; Hagen, J.A.; DeMeester, T.R. Intraoperative assessment of perfusion of the gastric graft and correlation with anastomotic leaks after esophagectomy. Ann. Surg. 2015, 262, 74. [Google Scholar] [CrossRef] [Green Version]
- Kechagias, A.; van Rossum, P.S.; Ruurda, J.P.; van Hillegersberg, R. Ischemic conditioning of the stomach in the prevention of esophagogastric anastomotic leakage after esophagectomy. Ann. Thorac. Surg. 2016, 101, 1614–1623. [Google Scholar] [CrossRef] [Green Version]
- Heger, P.; Blank, S.; Diener, M.K.; Ulrich, A.; Schmidt, T.; Buechler, M.W.; Mihaljevic, A.L. Gastric preconditioning in advance of esophageal resection-systematic review and meta-analysis. J. Gastrointest. Surg. 2017, 21, 1523–1532. [Google Scholar] [CrossRef] [PubMed]
- Mingol-Navarro, F.; Ballester-Pla, N.; Jimenez-Rosellon, R. Ischaemic conditioning of the stomach previous to esophageal surgery. J. Thorac. Dis. 2019, 11, S663. [Google Scholar] [CrossRef]
- Markar, S.R.; Karthikesalingam, A.; Thrumurthy, S.; Low, D.E. Volume-outcome relationship in surgery for esophageal malignancy: Systematic review and meta-analysis 2000–2011. J. Gastrointest. Surg. 2012, 16, 1055–1063. [Google Scholar] [CrossRef] [PubMed]
- Siegal, S.R.; Parmar, A.D.; Haisley, K.R.; Tieu, B.H.; Schipper, P.H.; Hunter, J.G.; Dolan, J.P. Gastric Ischemic Conditioning Prior to Esophagectomy Is Associated with Decreased Stricture Rate and Overall Anastomotic Complications. J. Gastrointest. Surg. 2018, 22, 1501–1507. [Google Scholar] [CrossRef] [PubMed]
- Karliczek, A.; Harlaar, N.; Zeebregts, C.; Wiggers, T.; Baas, P.; Van Dam, G. Surgeons lack predictive accuracy for anastomotic leakage in gastrointestinal surgery. Int. J. Colorectal Dis. 2009, 24, 569–576. [Google Scholar] [CrossRef] [Green Version]
- Bludau, M.; Hölscher, A.H.; Vallböhmer, D.; Gutschow, C.; Schröder, W. Ischemic conditioning of the gastric conduit prior to esophagectomy improves mucosal oxygen saturation. Ann. Thorac. Surg. 2010, 90, 1121–1126. [Google Scholar] [CrossRef]
- Köhler, H.; Jansen-Winkeln, B.; Maktabi, M.; Barberio, M.; Takoh, J.; Holfert, N.; Moulla, Y.; Niebisch, S.; Diana, M.; Neumuth, T.; et al. Evaluation of hyperspectral imaging (HSI) for the measurement of ischemic conditioning effects of the gastric conduit during esophagectomy. Surg. Endosc. 2019, 33, 3775–3782. [Google Scholar]
- Veeramootoo, D.; Shore, A.C.; Wajed, S.A. Randomized controlled trial of laparoscopic gastric ischemic conditioning prior to minimally invasive esophagectomy, the LOGIC trial. Surg. Endosc. 2012, 26, 1822–1829. [Google Scholar] [CrossRef]
- Diana, M.; Agnus, V.; Halvax, P.; Liu, Y.Y.; Dallemagne, B.; Schlagowski, A.I.; Geny, B.; Diemunsch, P.; Lindner, V.; Marescaux, J.; et al. Intraoperative fluorescence-based enhanced reality laparoscopic real-time imaging to assess bowel perfusion at the anastomotic site in an experimental model. Br. J. Surg. 2015, 102, e169–e176. [Google Scholar] [CrossRef]
- Diana, M.; Noll, E.; Diemunsch, P.; Dallemagne, B.; Benahmed, M.A.; Agnus, V.; Soler, L.; Barry, B.; Namer, I.J.; Demartines, N.; et al. Enhanced-reality video fluorescence: A real-time assessment of intestinal viability. Ann. Surg. 2014, 259, 700–707. [Google Scholar] [CrossRef]
- Barberio, M.; Longo, F.; Fiorillo, C.; Seeliger, B.; Mascagni, P.; Agnus, V.; Lindner, V.; Geny, B.; Charles, A.-L.; Gockel, I.; et al. HYPerspectral Enhanced Reality (HYPER): A physiology-based surgical guidance tool. Surg. Endosc. 2019, 34, 1736–1744. [Google Scholar] [CrossRef] [PubMed]
- Barberio, M.; Felli, E.; Seyller, E.; Longo, F.; Chand, M.; Gockel, I.; Geny, B.; Swanström, L.; Marescaux, J.; Agnus, V.; et al. Quantitative fluorescence angiography versus hyperspectral imaging to assess bowel ischemia: A comparative study in enhanced reality. Surgery 2020, 168, 178–184. [Google Scholar] [CrossRef] [PubMed]
- Laemmel, E.; Genet, M.; Le Goualher, G.; Perchant, A.; Le Gargasson, J.-F.; Vicaut, E. Fibered confocal fluorescence microscopy (Cell-viZio™) facilitates extended imaging in the field of microcirculation. J. Vasc. Res. 2004, 41, 400–411. [Google Scholar] [CrossRef]
- Diana, M.; Dallemagne, B.; Chung, H.; Nagao, Y.; Halvax, P.; Agnus, V.; Soler, L.; Lindner, V.; Demartines, N.; Diemunsch, P.; et al. Probe-based confocal laser endomicroscopy and fluorescence-based enhanced reality for real-time assessment of intestinal microcirculation in a porcine model of sigmoid ischemia. Surg. Endosc. 2014, 2, 3224–3233. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schmidt, C.; Lautenschläger, C.; Petzold, B.; Sakr, Y.; Marx, G.; Stallmach, A. Confocal laser endomicroscopy reliably detects sepsis-related and treatment-associated changes in intestinal mucosal microcirculation. Br. J. Anaesth. 2013, 111, 996–1003. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Diana, M.; Noll, E.; Charles, A.-L.; Diemunsch, P.; Geny, B.; Liu, Y.-Y.; Marchegiani, F.; Schiraldi, L.; Agnus, V.; Lindner, V.; et al. Precision real-time evaluation of bowel perfusion: Accuracy of confocal endomicroscopy assessment of stoma in a controlled hemorrhagic shock model. Surg. Endosc. 2017, 31, 680–691. [Google Scholar] [CrossRef] [PubMed]
- Urschel, J.D.; Antkowiak, J.G.; Delacure, M.D.; Takita, H. Ischemic conditioning (delay phenomenon) improves esophagogastric anastomotic wound healing in the rat. J. Surg. Oncol. 1997, 66, 254–256. [Google Scholar] [CrossRef]
- Alfabet, C.; Montero, E.F.D.S.; Paes Leme, L.F.; Higashi, V.S.; Sallum Fo, C.F.; Fagundes, D.J.; Gomes, P.O. Progressive gastric perfusion in rats: Role of ischemic conditioning. Microsurg. Off. J. Int. Microsurg. Soc. Eur. Fed. Soc. Microsurg. 2003, 23, 513–516. [Google Scholar] [CrossRef]
- Reavis, K.M.; Chang, E.Y.; Hunter, J.G.; Jobe, B.A. Utilization of the delay phenomenon improves blood flow and reduces collagen deposition in esophagogastric anastomoses. Ann. Surg. 2005, 241, 736. [Google Scholar] [CrossRef]
- Lamas, S.; Azuara, D.; De Oca, J.; Sans, M.; Farran, L.; Alba, E.; Escalante, E.; Rafecas, A. Time course of necrosis/apoptosis and neovascularization during experimental gastric conditioning. Dis. Esophagus 2008, 21, 370–376. [Google Scholar] [CrossRef]
- Quero, G.; Lapergola, A.; Barberio, M.; Seeliger, B.; Saccomandi, P.; Guerriero, L.; Mutter, D.; Saadi, A.; Worreth, M.; Marescaux, J.; et al. Discrimination between arterial and venous bowel ischemia by computer-assisted analysis of the fluorescent signal. Surg. Endosc. 2019, 33, 1988–1997. [Google Scholar] [CrossRef] [PubMed]
- Puxeddu, I.; Alian, A.; Piliponsky, A.M.; Ribatti, D.; Panet, A.; Levi-Schaffer, F. Human peripheral blood eosinophils induce angiogenesis. Int. J. Biochem. Cell Biol. 2005, 37, 628–636. [Google Scholar] [CrossRef] [PubMed]
- Nissim Ben Efraim, A.H.; Levi-Schaffer, F. Roles of eosinophils in the modulation of angiogenesis. Chem. Immunol. Allergy 2014, 99, 138–154. [Google Scholar] [CrossRef] [PubMed]
- Varricchi, G.; Loffredo, S.; Galdiero, M.R.; Marone, G.; Cristinziano, L.; Granata, F.; Marone, G. Innate effector cells in angiogenesis and lymphangiogenesis. Curr. Opin. Immunol. 2018, 53, 152–160. [Google Scholar] [CrossRef]
- Staton, C.A.; Stribbling, S.M.; Tazzyman, S.; Hughes, R.; Brown, N.J.; Lewis, C.E. Current methods for assaying angiogenesis in vitro and in vivo. Int. J. Exp. Pathol. 2004, 85, 233–248. [Google Scholar] [CrossRef]
- Akiyama, S.; Ito, S.; Sekiguchi, H.; Fujiwara, M.; Sakamoto, J.; Kondo, K.; Kasai, Y.; Ito, K.; Takagi, H. Preoperative embolization of gastric arteries for esophageal cancer. Surgery 1996, 120, 542–546. [Google Scholar] [CrossRef]
- Diana, M.; Hübner, M.; Vuilleumier, H.; Bize, P.; Denys, A.; Demartines, N.; Schäfer, M. Redistribution of gastric blood flow by embolization of gastric arteries before esophagectomy. Ann. Thorac. Surg. 2011, 91, 1546–1551. [Google Scholar] [CrossRef]
- Ghelfi, J.; Brichon, P.-Y.; Frandon, J.; Boussat, B.; Bricault, I.; Ferretti, G.; Guigard, S.; Sengel, C. Ischemic gastric conditioning by preoperative arterial embolization before oncologic esophagectomy: A Single-Center Experience. Cardiovasc. Interv. Radiol. 2017, 40, 712–720. [Google Scholar] [CrossRef]
- Hölscher, A.H.; Schneider, P.M.; Gutschow, C.; Schröder, W. Laparoscopic ischemic conditioning of the stomach for esophageal replacement. Ann. Surg. 2007, 245, 241. [Google Scholar] [CrossRef]
- Nguyen, N.T.; Nguyen, X.-M.T.; Reavis, K.M.; Elliott, C.; Masoomi, H.; Stamos, M.J. Minimally invasive esophagectomy with and without gastric ischemic conditioning. Surg. Endosc. 2012, 26, 1637–1641. [Google Scholar] [CrossRef]
- Bludau, M.; Hölscher, A.; Vallböhmer, D.; Metzger, R.; Bollschweiler, E.; Schröder, W. Vascular endothelial growth factor expression following ischemic conditioning of the gastric conduit. Dis. Esophagus 2013, 26, 847–852. [Google Scholar] [CrossRef] [PubMed]
- Veeramootoo, D.; Shore, A.C.; Shields, B.; Krishnadas, R.; Cooper, M.; Berrisford, R.G.; Wajed, S.A. Ischemic conditioning shows a time-dependant influence on the fate of the gastric conduit after minimally invasive esophagectomy. Surg. Endosc. 2010, 24, 1126–1131. [Google Scholar] [CrossRef] [PubMed]
- Schröder, W.; Hölscher, A.H.; Bludau, M.; Vallböhmer, D.; Bollschweiler, E.; Gutschow, C. Ivor-Lewis esophagectomy with and without laparoscopic conditioning of the gastric conduit. World J. Surg. 2010, 34, 738–743. [Google Scholar] [CrossRef]
- Berrisford, R.G.; Veeramootoo, D.; Parameswaran, R.; Krishnadas, R.; Wajed, S.A. Laparoscopic ischaemic conditioning of the stomach may reduce gastric-conduit morbidity following total minimally invasive oesophagectomy. Eur. J. Cardio-Thorac. Surg. 2009, 36, 888–893. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- El-Eishi, H.; Ayoub, S.; Abd-El-Khalek, M. The arterial supply of the human stomach. Cells Tissues Organs 1973, 86, 565–580. [Google Scholar] [CrossRef]
- Akiyama, S.; Kodera, Y.; Sekiguchi, H.; Kasai, Y.; Kondo, K.; Ito, K.; Takagi, H. Preoperative embolization therapy for esophageal operation. J. Surg. Oncol. 1998, 69, 219–223. [Google Scholar] [CrossRef]
- Kilkenny, C.; Browne, W.; Cuthill, I.C.; Emerson, M.; Altman, D.G. Animal research: Reporting in vivo experiments: The ARRIVE guidelines. J. Gene Med. 2010, 12, 561–563. [Google Scholar] [CrossRef]
- Schaefer, S.; McPhail, T.; Warren, J. Image Deformation Using Moving Least Squares; ACM SIGGRAPH 2006 Papers: Boston, MA, USA; pp. 533–540.









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group | Hybrid IGP Intervention at T0 |
|---|---|
| Max IGP (n = 5) | Angiographic embolization of RGA-LGA-LGEA Laparoscopic division of SGAs |
| Min IGP (n = 5) | Angiographic embolization of LGA Laparoscopic division of SGAs |
| Sham (n = 6) | Diagnostic angiography of RGA-LGA-LGEA Diagnostic laparoscopy |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Barberio, M.; Felli, E.; Pop, R.; Pizzicannella, M.; Geny, B.; Lindner, V.; Baiocchini, A.; Jansen-Winkeln, B.; Moulla, Y.; Agnus, V.; et al. A Novel Technique to Improve Anastomotic Perfusion Prior to Esophageal Surgery: Hybrid Ischemic Preconditioning of the Stomach. Preclinical Efficacy Proof in a Porcine Survival Model. Cancers 2020, 12, 2977. https://doi.org/10.3390/cancers12102977
Barberio M, Felli E, Pop R, Pizzicannella M, Geny B, Lindner V, Baiocchini A, Jansen-Winkeln B, Moulla Y, Agnus V, et al. A Novel Technique to Improve Anastomotic Perfusion Prior to Esophageal Surgery: Hybrid Ischemic Preconditioning of the Stomach. Preclinical Efficacy Proof in a Porcine Survival Model. Cancers. 2020; 12(10):2977. https://doi.org/10.3390/cancers12102977
Chicago/Turabian StyleBarberio, Manuel, Eric Felli, Raoul Pop, Margherita Pizzicannella, Bernard Geny, Veronique Lindner, Andrea Baiocchini, Boris Jansen-Winkeln, Yusef Moulla, Vincent Agnus, and et al. 2020. "A Novel Technique to Improve Anastomotic Perfusion Prior to Esophageal Surgery: Hybrid Ischemic Preconditioning of the Stomach. Preclinical Efficacy Proof in a Porcine Survival Model" Cancers 12, no. 10: 2977. https://doi.org/10.3390/cancers12102977