
Preservation of Organ Function in Locally Advanced Non-Metastatic Gastrointestinal Stromal Tumors (GIST) of the Stomach by Neoadjuvant Imatinib Therapy

 ,
,  , , and
, , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Material and Methods
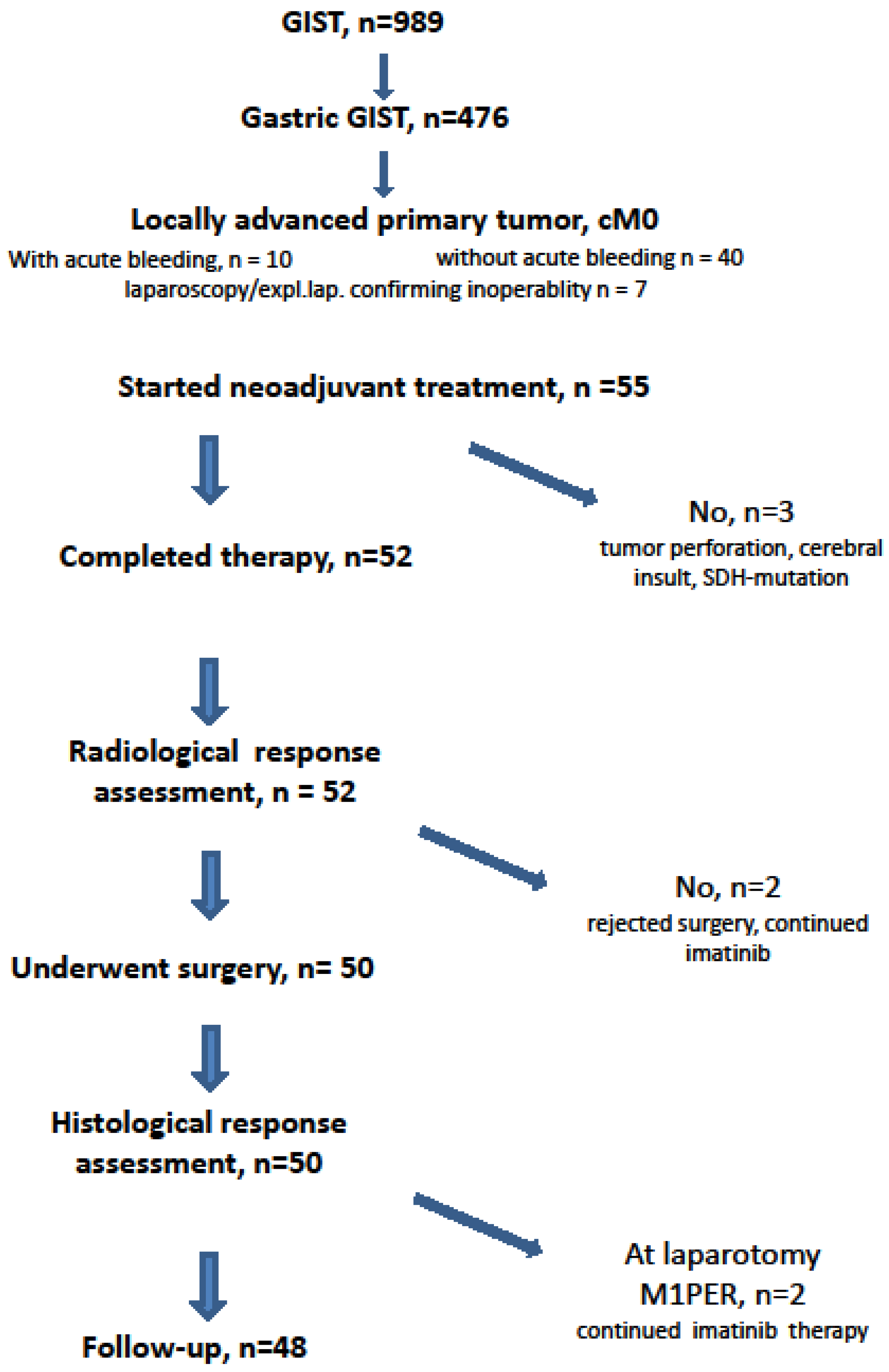
2.1. Patient Selection
2.2. Clinical Condition
2.3. Imatinib Mesylate Therapy and Response Assessment
2.4. Conduct of Surgery
2.5. Postoperative Drug Therapy
2.6. Follow-Up
2.7. Statistical Analysis
3. Results
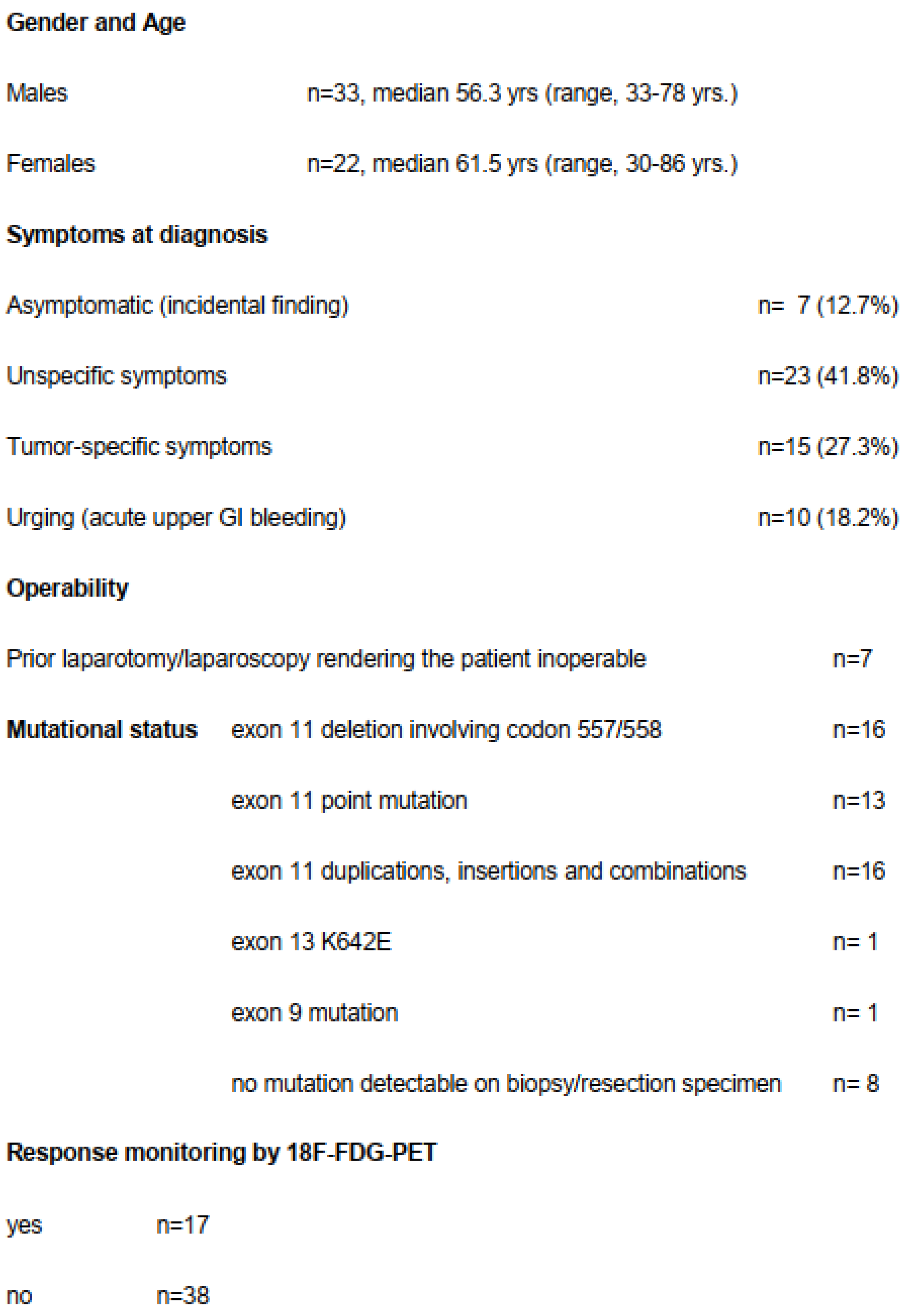
3.1. Demographic and Clinicopathological Data
3.2. Mutational Data
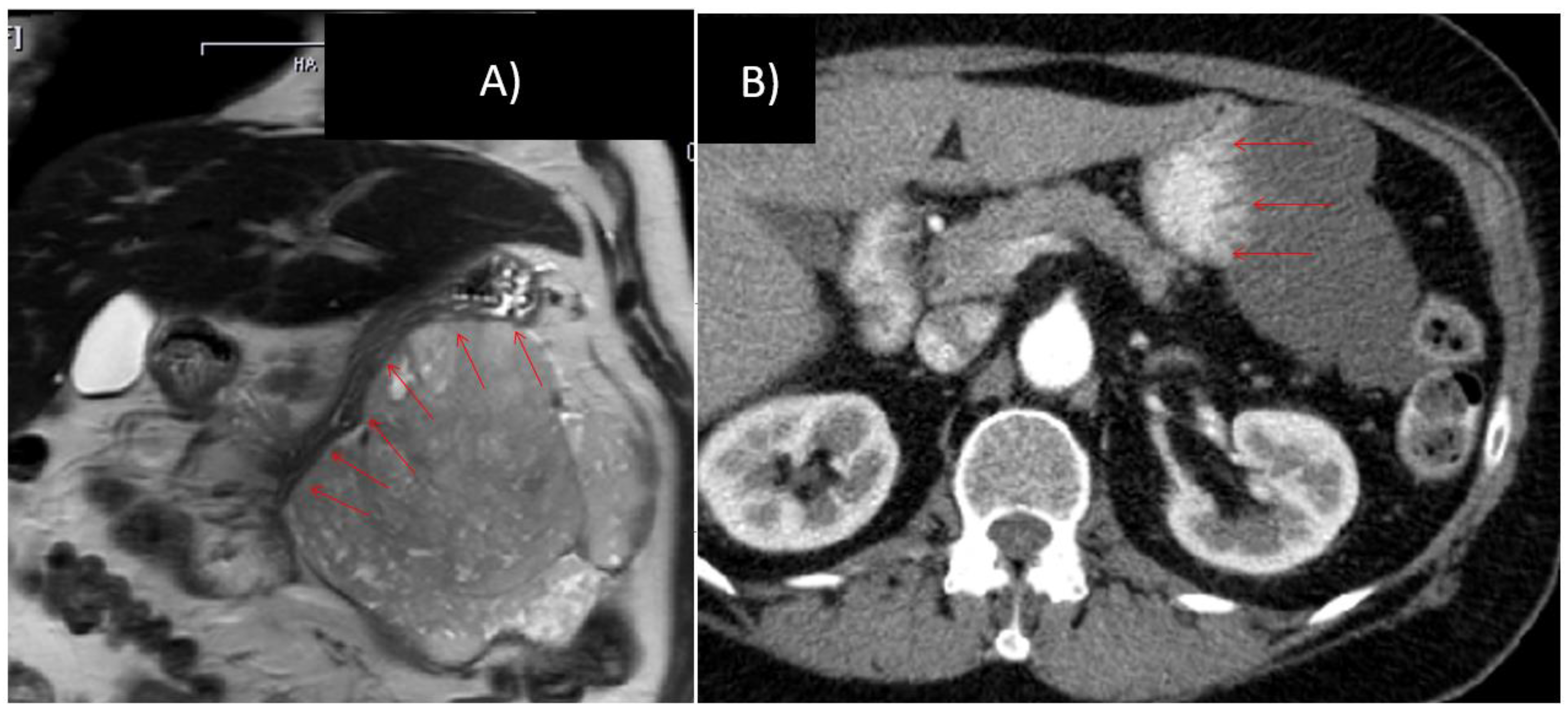
3.3. Imatinib Therapy and Clinical Response
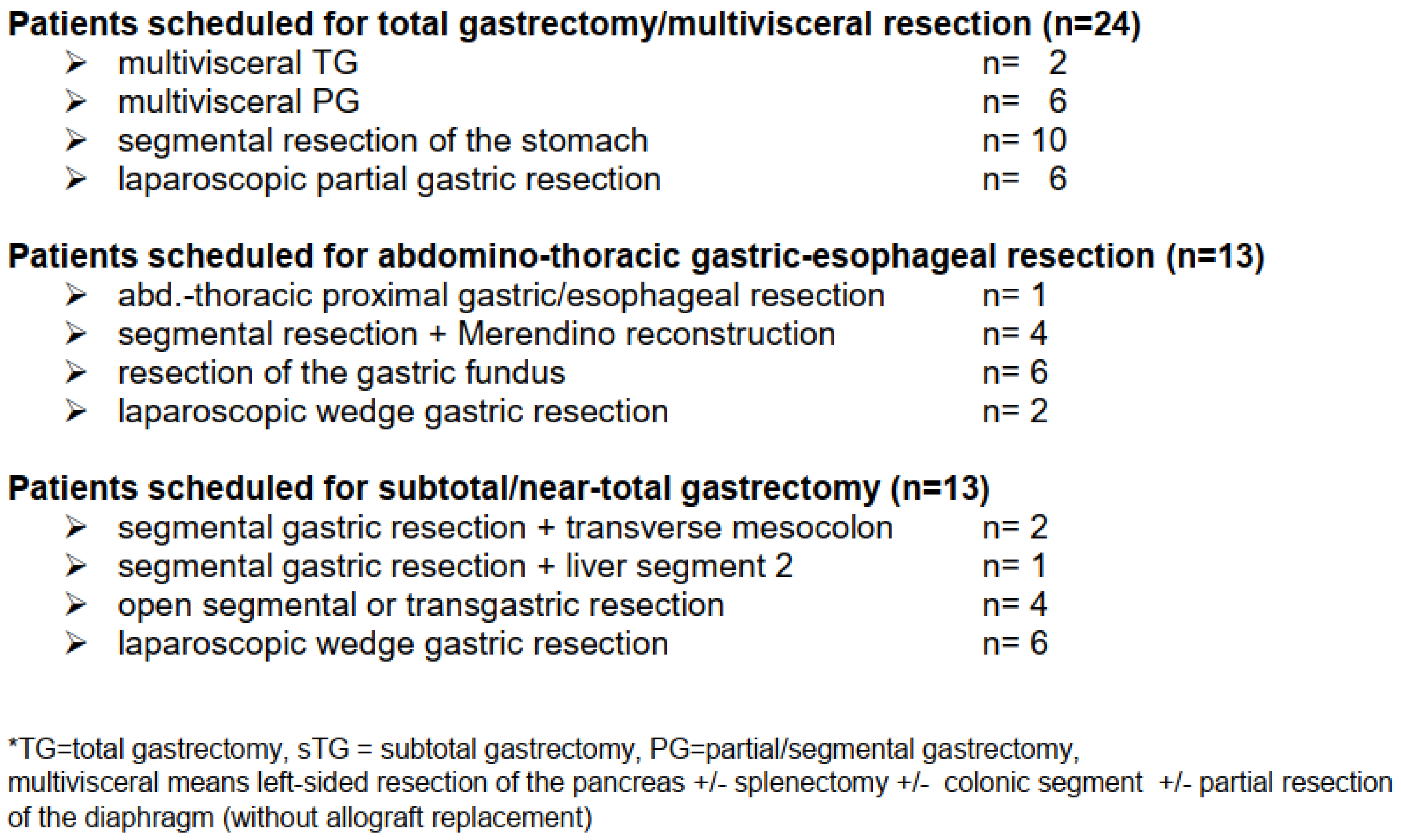
3.4. Surgical Data
3.5. Histopathological Data
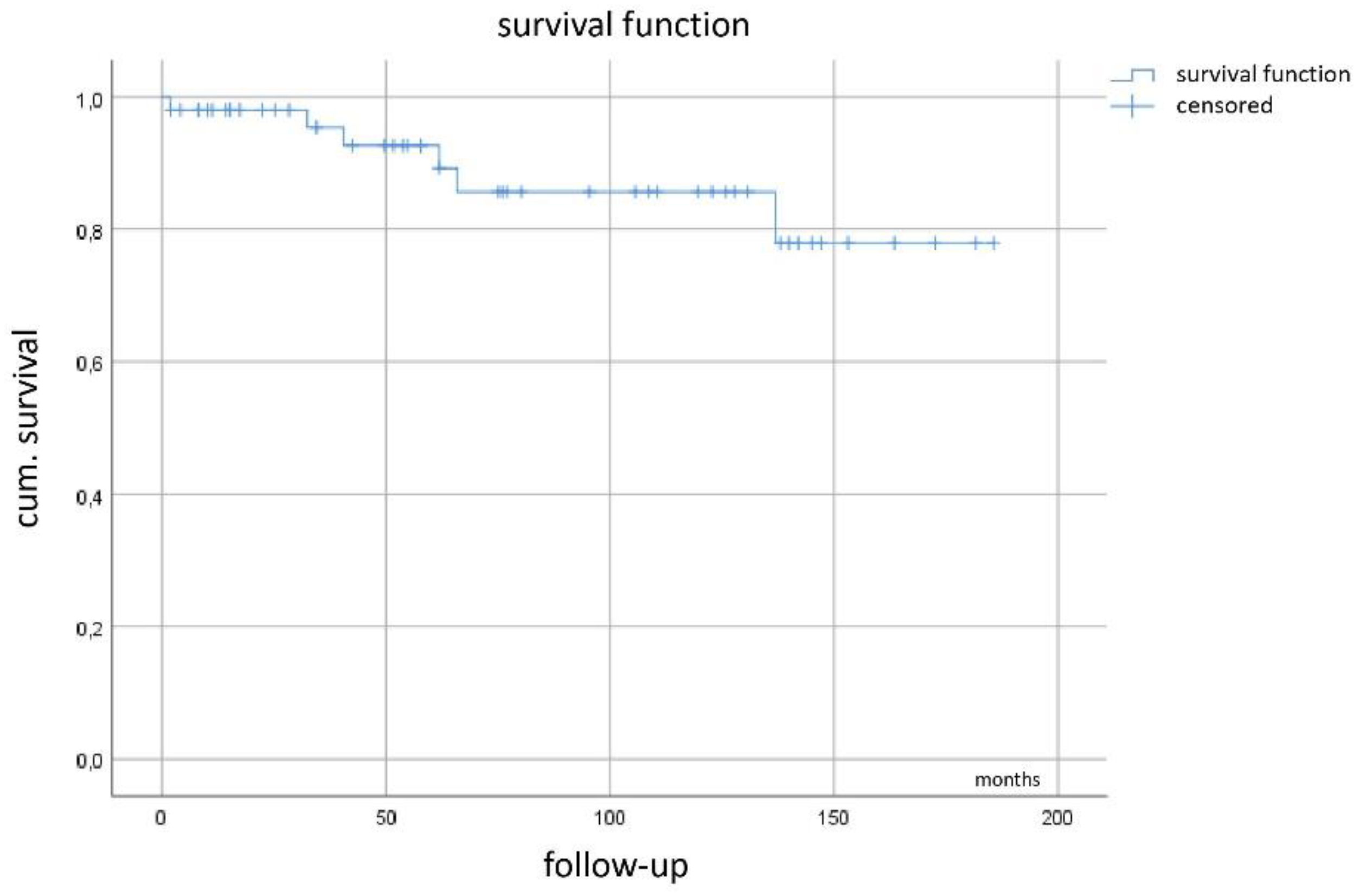
3.6. Recurrence-Free Survival
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Fletcher, C.D.; Berman, J.J.; Corless, C.; Gorstein, F.; Lasota, J.; Longley, B.J.; Miettinen, M.; O’Leary, T.J.; Remotti, H.; Rubin, B.P.; et al. Diagnosis of gastrointestinal stromal tumors: A consensus approach. Hum. Pathol. 2002, 33, 459–465. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nilsson, B.; Bümming, P.; Meis-Kindblom, J.M.; Oden, A.; Dortok, A.; Gustavsson, B.; Sablinska, K.; Kindblom, L.G. Gastrointestinal stromal tumors: The incidence, prevalence, clinical course, and prognostication in the preimatinib mesylate era—A population-based study in western Sweden. Cancer 2005, 103, 821–829. [Google Scholar] [CrossRef] [PubMed]
- DeMatteo, R.P.; Lewis, J.J.; Leung, D.; Mudan, S.S.; Woodruff, J.M.; Brennan, M.F. Two hundred gastrointestinal stromal tumors: Recurrence patterns and prognostic factors for survival. Ann. Surg. 2000, 231, 51–58. [Google Scholar] [CrossRef]
- Miettinen, M.; Lasota, J. Gastrointestinal stromal tumors: Review on morphology, molecular pathology, prognosis, and differential diagnosis. Arch. Pathol. Lab. Med. 2006, 130, 1466–1478. [Google Scholar]
- Hirota, S. Gain-of-function Mutations of c-kit in human gastrointestinal stromal tumors. Science 1998, 279, 577–580. [Google Scholar] [CrossRef]
- Heinrich, M.C.; Corless, C.L.; Duensing, A.; McGreevey, L.; Chen, C.J.; Joseph, N.; Singer, S.; Griffith, D.J.; Haley, A.; Town, A.; et al. PDGFRA activating mutations in gastrointestinal stromal tumors. Science 2003, 299, 708–710. [Google Scholar] [CrossRef]
- Roberts, P.J.; Eisenberg, B. Clinical presentation of gastrointestinal stromal tumors and treatment of operable disease. Eur. J. Cancer 2002, 38, 37–38. [Google Scholar] [CrossRef]
- Dematteo, R.P.; Heinrich, M.C.; El-Rifai, W.M.; Demetri, G. Clinical management of gastrointestinal stromal tumors: Before and after STI-571. Hum. Pathol. 2002, 33, 466–477. [Google Scholar] [CrossRef]
- Joensuu, H.; Roberts, P.J.; Sarlomo-Rikala, M.; Andersson, L.C.; Tervahartiala, P.; Tuveson, D.; Silberman, S.; Capdeville, R.; Dimitrijevic, S.; Druker, B.; et al. Effect of the tyrosine kinase inhibitor STI571 in a patient with a metastatic gastrointestinal stromal tumor. N. Engl. J. Med. 2001, 344, 1052–1056. [Google Scholar] [CrossRef]
- Heinrich, M.C.; Blanke, C.D.; Druker, B.J.; Corless, C.L. Inhibition of KIT Tyrosine Kinase Activity: A Novel Molecular Approach to the Treatment of KIT-Positive Malignancies. J. Clin. Oncol. 2002, 20, 1692–1703. [Google Scholar] [CrossRef]
- Demetri, G.D.; Demetri, G.D.; von Mehren, M.; Blanke, C.D.; Van den Abbeele, A.D.; Eisenberg, B.; Roberts, P.J.; Heinrich, M.C.; Tuveson, D.A.; Singer, S.; et al. Efficacy and safety of imatinib mesylate in advanced gastrointestinal stromal tumors. N. Engl. J. Med. 2002, 347, 472–480. [Google Scholar] [CrossRef] [PubMed]
- van Oosterom, A.T.; Judson, I.; Verweij, J.; Stroobants, S.; Donato di Paola, E.; Dimitrijevic, S.; Martens, M.; Webb, A.; Sciot, R.; van Glabbeke, M.; et al. Safety and efficacy of imatinib (STI571) in metastatic gastrointestinal stromal tumours: A phase I study. Lancet 2001, 358, 1421–1423. [Google Scholar] [CrossRef]
- Demetri, G.D.; von Mehren, M.; Antonescu, C.R.; DeMatteo, R.P.; Ganjoo, K.N.; Maki, R.G.; Pisters, P.W.T.; Raut, C.P.; Riedel, R.F.; Schuetze, S.; et al. NCCN Task Force report: Update on the management of patients with gastrointestinal stromal tumors. J. Natl. Compr. Cancer Netw. 2010, 8 (Suppl. 2), 1–41. [Google Scholar] [CrossRef] [Green Version]
- Demetri, G.D.; Wang, Y.; Wehrle, E.; Racine, A.; Nikolova, Z.; Blanke, C.D.; Joensuu, H.; von Mehren, M. Imatinib plasma levels are correlated with clinical benefit in patients with unresectable/metastatic gastrointestinal stromal tumors. J. Clin. Oncol. 2009, 27, 3141–3147. [Google Scholar] [CrossRef]
- Eisenberg, B.L.; Harris, J.; Blanke, C.D.; Demetri, G.D.; Heinrich, M.C.; Watson, J.C.; Hoffman, J.P.; Okuno, S.; Kane, J.M.; von Mehren, M. Phase II trial of neoadjuvant/adjuvant imatinib mesylate (IM) for advanced primary and metastatic/recurrent operable gastrointestinal stromal tumor (GIST): Early results of RTOG 0132/ACRIN 6665. J. Surg. Oncol. 2009, 99, 42–47. [Google Scholar] [CrossRef] [Green Version]
- Shrikhande, S.V.; Marda, S.S.; Suradkar, K.; Arya, S.; Shetty, G.S.; Bal, M.; Shukla, P.J.; Goel, M.; Mohandas, K.M. Gastrointestinal stromal tumors: Case series of 29 patients defining the role of imatinib prior to surgery. World J. Surg. 2012, 36, 864–871. [Google Scholar] [CrossRef]
- Koontz, M.Z.; Visser, B.M.; Kunz, P.L. Neoadjuvant imatinib for borderline resectable GIST. J. Natl. Compr. Cancer Netw. 2012, 10, 1477–1482. [Google Scholar] [CrossRef] [Green Version]
- Tielen, R.; Verhoef, C.; van Coevorden, F.; Gelderblom, H.; Sleijfer, S.; Hartgrink, H.H.; Bonenkamp, J.J.; van der Graaf, W.T.; de Wilt, J.H. Surgical treatment of locally advanced, non-metastatic, gastrointestinal stromal tumours after treatment with imatinib. Eur. J. Surg. Oncol. 2013, 39, 150–155. [Google Scholar] [CrossRef] [Green Version]
- Fiore, M.; Palassini, E.; Fumagalli, E.; Pilotti, S.; Tamborini, E.; Stacchiotti, S.; Pennacchioli, E.; Casali, P.G.; Gronchi, A. Preoperative imatinib mesylate for unresectable or locally advanced primary gastrointestinal stromal tumors (GIST). Eur. J. Surg. Oncol. 2009, 35, 739–745. [Google Scholar] [CrossRef]
- Andtbacka, R.H.; Ng, C.S.; Scaife, C.L.; Cormier, J.N.; Hunt, K.K.; Pisters, P.W.T.; Pollock, R.E.; Benjamin, R.S.; Burgess, M.A.; Chen, L.L.; et al. Surgical resection of gastrointestinal stromal tumors after treatment with imatinib. Ann. Surg. Oncol. 2007, 14, 14–24. [Google Scholar] [CrossRef] [PubMed]
- Raut, C.P.; Posner, M.; Desai, J.; Morgan, J.A.; George, S.; Zahrieh, D.; Fletcher, C.D.M.; Demetri, G.D.; Bertagnolli, M.M. Surgical management of advanced gastrointestinal stromal tumors after treatment with targeted systemic therapy using kinase inhibitors. J. Clin. Oncol. 2006, 24, 2325–2331. [Google Scholar] [CrossRef] [PubMed]
- Blesius, A.; Cassier, P.A.; Bertucci, F.; Fayette, J.; Ray-Coquard, I.; Bui, B.; Adenis, A.; Rios, M.; Didier, C.; Perol, D.; et al. Neoadjuvant imatinib in patients with locally advanced non metastatic GIST in the prospective BFR14 trial. BMC Cancer 2011, 11, 72. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hohenberger, P.; Langer, C.; Wendtner, C.M.; Hohenberger, W.; Pustowka, A.; Wardelmann, E.; Andre, E.; Licht, T. Neoadjuvant treatment of locally advanced GIST: Results of APOLLON, a prospective, open label phase II study in KIT- or PDGFRA-positive tumors. J. Clin. Oncol. 2012, 30, abstr 10031. [Google Scholar] [CrossRef]
- Rutkowski, P.; Gronchi, A.; Hohenberger, P.; Bonvalot, S.; Schoffski, P.; Bauer, S.; Fumagalli, E.; Nyckowski, P.; Nguyen, B.P.; Kerst, J.M.; et al. Neoadjuvant Imatinib in Locally Advanced Gastrointestinal Stromal Tumors (GIST): The EORTC STBSG Experience. Ann. Surg. Oncol. 2013, 20, 2937–2943. [Google Scholar] [CrossRef]
- Wang, S.Y.; Wu, C.E.; Lai, C.C.; Chen, J.S.; Tsai, C.Y.; Cheng, C.T.; Yeh, T.S.; Yeh, C.N. Prospective evaluation of preoperative IM use in locally advanced gastrointestinal stromal tumors: Emphasis on the optimal duration of preoperative IM use, safety, and oncological outcome. Cancers 2019, 11, 424. [Google Scholar] [CrossRef] [Green Version]
- Staiger, W.I.; Ronellenfitsch, U.; Kaehler, G.; Schildhaus, H.U.; Dimitrakopoulou-Strauss, A.; Schwarzbach, M.H.; Hohenberger, P. The Merendino procedure following preoperative imatinib mesylate for locally advanced gastrointestinal stromal tumor of the esophagogastric junction. World J. Surg. Oncol. 2008, 6, 37. [Google Scholar] [CrossRef] [Green Version]
- Eisenhauer, E.A.; Therasse, P.; Bogaerts, J.; Schwartz, L.H.; Sargent, D.; Ford, R.; Dancey, J.; Arbuck, S.; Gwyther, S.; Mooney, M.; et al. New response evaluation criteria in solid tumours: Revised RECIST guideline (version 1.1). Eur. J. Cancer 2009, 45, 228–247. [Google Scholar] [CrossRef]
- Rutkowski, P.; Skoczylas, J.; Wisniewski, P. Is the surgical margin in gastrointestinal stromal tumors different? Visc. Med. 2018, 34, 347–352. [Google Scholar] [CrossRef]
- Hohenberger, P.; Bonvalot, S.; van Coevorden, F.; Rutkowski, P.; Stoeckle, E.; Olungu, C.; Litiere, S.; Wardelmann, E.; Gronchi, A.; Casali, P. Quality of surgery and surgical reporting for patients with primary gastrointestinal stromal tumors participating in the EORTC STBSG 62024 adjuvant imatinib study. Eur. J. Cancer 2019, 120, 47–53. [Google Scholar] [CrossRef]
- Dindo, D.; Demartines, N.; Clavien, P.A. Classification of Surgical Complications: A New Proposal With Evaluation in a Cohort of 6336 Patients and Results of a Survey. Ann. Surg. 2004, 240, 205–213. [Google Scholar] [CrossRef]
- Hermanek, P.; Wittekind, C. The pathologist and the residual tumor (R) classification. Pathol. Res. Pract. 1994, 190, 115–123. [Google Scholar] [CrossRef]
- Kaplan, E.L.; Meier, P. Nonparametric estimation from incomplete observations. J. Am. Stat. Assoc. 1958, 53, 457–481. [Google Scholar] [CrossRef]
- Mantel, N. Evaluation of survival data and two new rank order statistics arising in its consideration. Cancer Chemother. Rep. 1966, 50, 163–170. [Google Scholar] [PubMed]
- Bachet, J.B.; Landi, B.; Laurent-Puig, P.; Italiano, A.; Le Cesne, A.; Levy, P.; Safar, V.; Duffaud, F.; Blay, J.Y.; Emile, J.F. Diagnosis, prognosis and treatment of patients with gastrointestinal stromal tumour (GIST) and germline mutation of KIT exon 13. Eur. J. Cancer 2013, 49, 2531–2541. [Google Scholar] [CrossRef] [PubMed]
- Casali, P.G.; Abecassis, N.; Aro, H.T.; Bauer, S.; Biagini, R.; Bielack, S.; Boukovinas, I.; Bovee, J.V.M.G.; Brodowicz, T.; Brotto, J.M.; et al. Gastrointetinal stromal tumors: ESMO-EURACAN clinical practice guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2018, 29, 267. [Google Scholar] [CrossRef]
- Jakob, J.; Hohenberger, P. Neoadjuvant therapy to downstage the extent of resection of gastrointestinal stromal tumors. Visc. Med. 2018, 34, 359–365. [Google Scholar] [CrossRef]
- Choi, H. Response evaluation of gastrointestinal stromal tumors. Oncologist 2008, 13 (Suppl. 2), 4–7. [Google Scholar] [CrossRef] [Green Version]
- Van den Abbeele, A.D. The lessons of GIST–PET and PET/CT: A new paradigm for imaging. Oncologist 2008, 13 (Suppl. 2), 8–13. [Google Scholar] [CrossRef]
- Bonvalot, S.; Eldweny, H.; Pechoux, C.L.; Vanel, D.; Terrier, P.; Cavalcanti, A.; Robert, C.; Lassau, N.; Cesne, A.L. Impact of Surgery on Advanced Gastrointestinal Stromal Tumors (GIST) in the Imatinib Era. Ann. Surg. Oncol. 2006, 13, 1596–1603. [Google Scholar] [CrossRef]
- Wang, D.; Zhang, Q.; Blanke, C.D.; Demetri, G.D.; Heinrich, M.C.; Watson, J.C.; Hoffman, J.P.; Okuno, S.; Kane, J.M.; von Mehren, M.; et al. Phase II Trial of Neoadjuvant/adjuvant Imatinib Mesylate for Advanced Primary and Metastatic/recurrent Operable Gastrointestinal Stromal Tumors: Long-term Follow-up Results of Radiation Therapy Oncology Group 0132. Ann. Surg. Oncol. 2011, 19, 1074–1080. [Google Scholar] [CrossRef] [Green Version]
- Gronchi, A.; Fiore, M.; Miselli, F.; Lagonigro, M.S.; Coco, P.; Messina, A.; Pilotti, S.; Casali, P.G. Surgery of residual disease following molecular-targeted therapy with imatinib mesylate in advanced/metastatic GIST. Ann. Surg. 2007, 245, 341–346. [Google Scholar] [CrossRef] [PubMed]
- Rutkowski, P.; Nowecki, Z.; Nyckowski, P.; Dziewirski, W.; Grzesiakowska, U.; Nasierowska-Guttmejer, A.; Krawczyk, M.; Ruka, W. Surgical treatment of patients with initially inoperable and/or metastatic gastrointestinal stromal tumors (GIST) during therapy with imatinib mesylate. J. Surg. Oncol. 2006, 93, 304–311. [Google Scholar] [CrossRef] [PubMed]
- Hohenberger, P.; Ronellenfitsch, U.; Oladeji, O.; Pink, D.; Ströbel, P.; Wardelmann, E.; Reichardt, P. Pattern of recurrence in patients with ruptured primary gastrointestinal stromal tumour. Br. J. Surg. 2010, 97, 1854–1859. [Google Scholar] [CrossRef] [PubMed]
- Gronchi, A.; Raut, C.P. The combination of surgery and imatinib in GIST: A reality for localized tumors at high risk, an open issue for metastatic ones. Ann. Surg. Oncol. 2012, 19, 1051–1055. [Google Scholar] [CrossRef] [PubMed]
- Hohenberger, P.; Eisenberg, B. Role of surgery combined with kinase inhibition in the management of gastrointestinal stromal tumor (GIST). Ann. Surg. Oncol. 2010, 17, 2585–2600. [Google Scholar] [CrossRef] [PubMed]
- Tang, S.; Yin, Y.; Shen, C.; Chen, J.; Yin, X.; Zhang, B.; Yao, Y.; Yang, J.; Chen, Z. Preoperative imatinib mesylate (IM) for huge gastrointestinal stromal tumors (GIST). World J. Surg. Oncol. 2017, 15, 79. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Joensuu, H.; Vehtari, A.; Riihimäki, J.; Nishida, T.; Steigen, S.E.; Brabec, P.; Plank, L.; Nilsson, B.; Cirilli, C.; Braconi, C.; et al. Risk of recurrence of gastrointestinal stromal tumour after surgery: An analysis of pooled population-based cohorts. Lancet Oncol. 2012, 13, 265–274. [Google Scholar] [CrossRef]
- McAuliffe, J.C.; Hunt, K.K.; Lazar, A.J.; Choi, H.; Qiao, W.; Thall, P.; Pollock, R.E.; Benjamin, R.S.; Trent, J.C. A randomized, phase II study of preoperative plus postoperative imatinib in GIST: Evidence of rapid radiographic response and temporal induction of tumor cell apoptosis. Ann. Surg. Oncol. 2009, 16, 910–919. [Google Scholar] [CrossRef] [Green Version]
- Cavnar, M.J.; Seier, K.; Gönen, M.; Curtini, C.; Balachandran, V.P.; Tap, W.D.; Antonescu, C.R.; Singer, S.; DeMatteo, R.P. Prognostic factors after neoadjuvant imatinib for newly diagnosed primary gastrointestinal stromal tumor. J. Gastrointest. Surg. 2020. [Google Scholar] [CrossRef]
- Haller, F.; Detken, S.; Schulten, H.J.; Happel, N.; Gunawan, B.; Kuhlgatz, J.; Füzesi, L. Surgical management after neoadjuvant imatinib therapy in gastrointestinal stromal tumours (GISTs) with respect to imatinib resistance caused by secondary KIT mutations. Ann. Surg. Oncol. 2007, 14, 526–532. [Google Scholar] [CrossRef]
- Edinburgh: Scottis Intercollegiate Guidelines Network. Available online: http://www.sign.ac.uk/ (accessed on 10 April 2008).






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Tumor Size | |||
| Tumor size at start of treatment: Tumor size prior to surgery: | 113 mm (range, 65–330 mm) (measured by CT/MRI) 69 mm (range, 25–228 mm) (measured by CT/MRI) | ||
| Tumor size at resection specimen: | 62 mm (range, 22–200 mm) (measured by pathology) | ||
| Pathology Review of the Resection Specimen | |||
| Complete necrosis (no viable tumor cells) | n = 12 (24%) | ||
| Near total (>95% necrosis) | n = 10 (20%) | ||
| Subtotal (>90% necrosis) | n = 7 (14%) | ||
| Partial remission (>50% necrosis) | n = 14 (28%) | ||
| Stable disease (<50% necrosis) | n = 7 (14%) | ||
| Correlation of Response to Therapy (Pearson, Two-Sided; Spearman) | |||
| Δtumor diameter pre vs. post | p = 0.078 | p = 0.089 | |
| RECIST 1.1 | p = 0.2 | p = 0.21 | |
| Mutational type exon 11 | p = 0.04 | p = 0.037 | |
| point mutation | |||
| del involving codons 557_558 | |||
| others |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vassos, N.; Jakob, J.; Kähler, G.; Reichardt, P.; Marx, A.; Dimitrakopoulou-Strauss, A.; Rathmann, N.; Wardelmann, E.; Hohenberger, P. Preservation of Organ Function in Locally Advanced Non-Metastatic Gastrointestinal Stromal Tumors (GIST) of the Stomach by Neoadjuvant Imatinib Therapy. Cancers 2021, 13, 586. https://doi.org/10.3390/cancers13040586
Vassos N, Jakob J, Kähler G, Reichardt P, Marx A, Dimitrakopoulou-Strauss A, Rathmann N, Wardelmann E, Hohenberger P. Preservation of Organ Function in Locally Advanced Non-Metastatic Gastrointestinal Stromal Tumors (GIST) of the Stomach by Neoadjuvant Imatinib Therapy. Cancers. 2021; 13(4):586. https://doi.org/10.3390/cancers13040586
Chicago/Turabian StyleVassos, Nikolaos, Jens Jakob, Georg Kähler, Peter Reichardt, Alexander Marx, Antonia Dimitrakopoulou-Strauss, Nils Rathmann, Eva Wardelmann, and Peter Hohenberger. 2021. "Preservation of Organ Function in Locally Advanced Non-Metastatic Gastrointestinal Stromal Tumors (GIST) of the Stomach by Neoadjuvant Imatinib Therapy" Cancers 13, no. 4: 586. https://doi.org/10.3390/cancers13040586