
ARID1A and CTNNB1/β-Catenin Molecular Status Affects the Clinicopathologic Features and Prognosis of Endometrial Carcinoma: Implications for an Improved Surrogate Molecular Classification

 , , , , , , , ,
, , , , , , , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Cohort and Clinicopathologic Data
- The depth of myometrial invasion was recorded in all cases as a percentage of myometrial thickness.
- The pattern of myometrial invasion was reported, specifying whether microcystic, elongated and fragmented (MELF) [24] and/or as single invasive cells or small groups of cells (tumor budding) [25]. Characteristics of the MELF pattern include the presence of invasive small dilated glands lined by cuboidal or flattened cells with eosinophilic cytoplasm and with slit-like appearance. This invasive pattern typically has a myxoid to granulation-like reaction in the surrounding myometrium. Tumor budding is defined as invasive single/small group of cells without formation of defined structures frequently lying in an edematous or myxoid background.
- Lymphovascular space invasion (LVSI) is defined by the presence of tumor fragments within endothelial-lined vascular/lymphatic spaces outside the immediate invasive border. Intratumoral LVSI foci were not considered. A semi-quantitative three- tiered scoring system was applied: no LVSI; focal (a single focus of LVSI recognized around the tumor); substantial (diffuse or multifocal LVSI around the tumor) [26,27].
- The presence of extensive tumor necrosis was reported; necrosis only within glands or at the tumor’s surface was not scored.
- Tumor heterogeneity were reported when a tumor had two or more clearly separate morphological patterns, and each constituting at least 10% of the tumor [28].
- Tumor infiltrating lymphocytes were assessed considering intraepithelial tumor infiltrating lymphocytes (iTILs; lymphocytes located within the tumor epithelium) and stromal tumor infiltrating lymphocytes (sTILs; lymphocytes in the stroma immediately adjacent to the tumor epithelium). The number of intraepithelial lymphocytes was counted in 10 high-power fields (HPF, ×400 magnification) with the highest density of TILs. The cut-off of 40 lymphocytes per 10 HPF was used to define a high iTIL score [28,29]. sTILs counting was evaluated at ×400 magnification field from the invasive border and performed according to the semi-quantitative method of Shia: sTILs absent/mild and sTILs moderate/high [28,29].
- The mitotic index was expressed as the number of mitoses per 10 high-power fields (×400 magnification).
2.2. Immunohistochemistry
2.2.1. Immunohistochemical Assessment and Evaluation of p53 Expression
2.2.2. Immunohistochemical Assessment and Evaluation of PTEN Expression
2.2.3. Immunohistochemical Assessment and Evaluation of ARID1A Expression
2.2.4. Immunohistochemical Assessment and Evaluation of β-Catenin Expression
2.2.5. Immunohistochemical Assessment and Evaluation of MMR Protein Expression
2.2.6. Immunohistochemical Assessment and Evaluation of Ki67 Proliferative Index
2.3. DNA Extraction and Next Generation Sequencing
2.4. Methylation Specific PCR
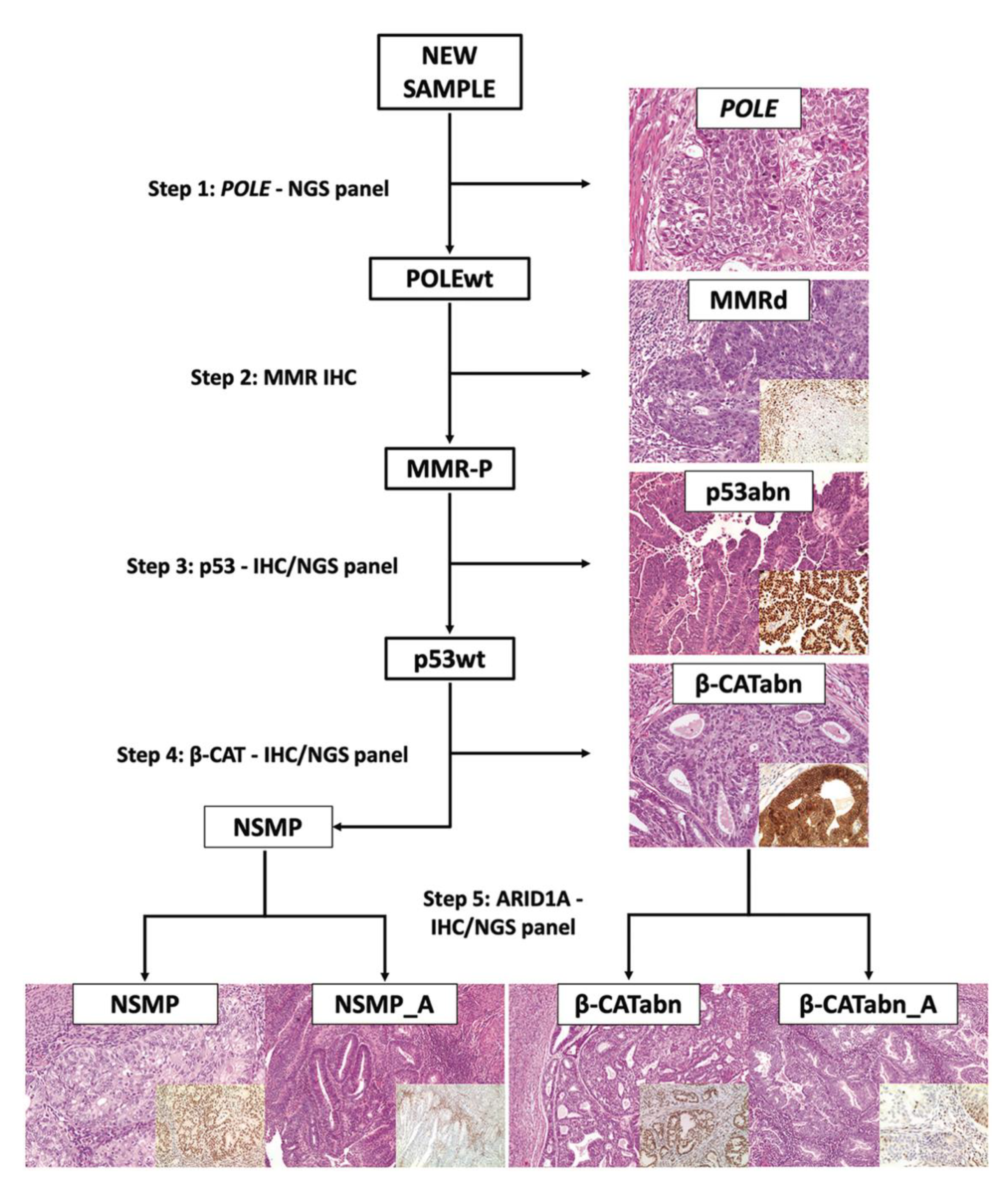
2.5. Assignation of Carcinomas to Surrogate TCGA Molecular Groups and NSMP Subgroups
2.6. Statistics
3. Results
3.1. Clinicopathologic Features of Endometrial Carcinoma and Conventional Prognostic Stratification
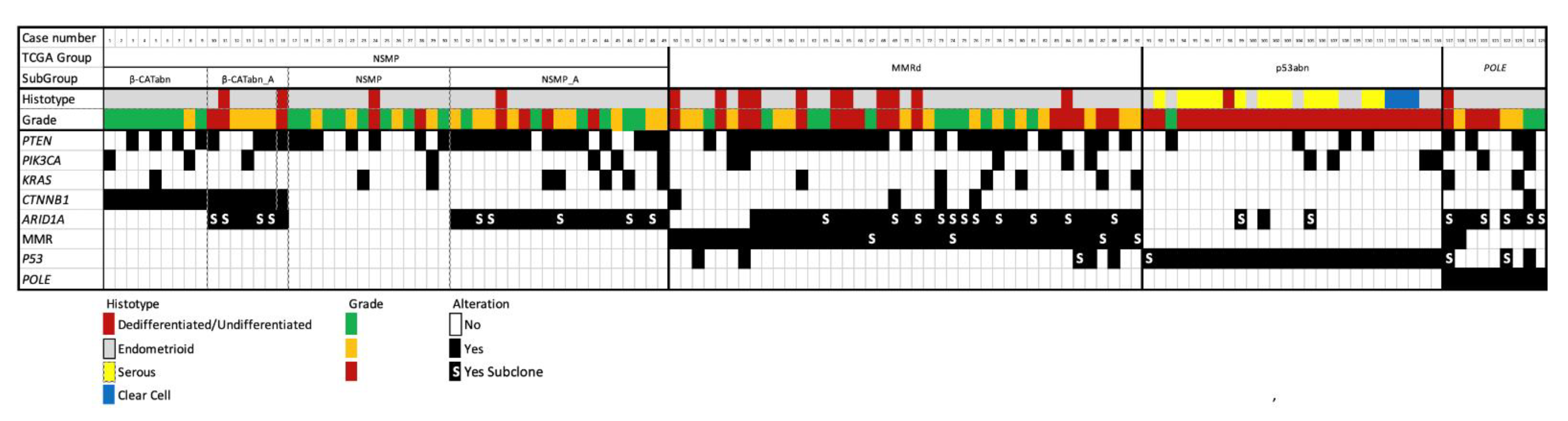
3.2. Molecular TCGA Group Assignment
3.2.1. POLE-Mutated Tumors
3.2.2. MMRd Tumors
3.2.3. p53abn Tumors
3.2.4. NSMP Tumors
3.3. CTNNB1 Mutations/β-Catenin Abnormal Expression
3.4. ARID1A Mutations/ ARID1A Loss of Expression
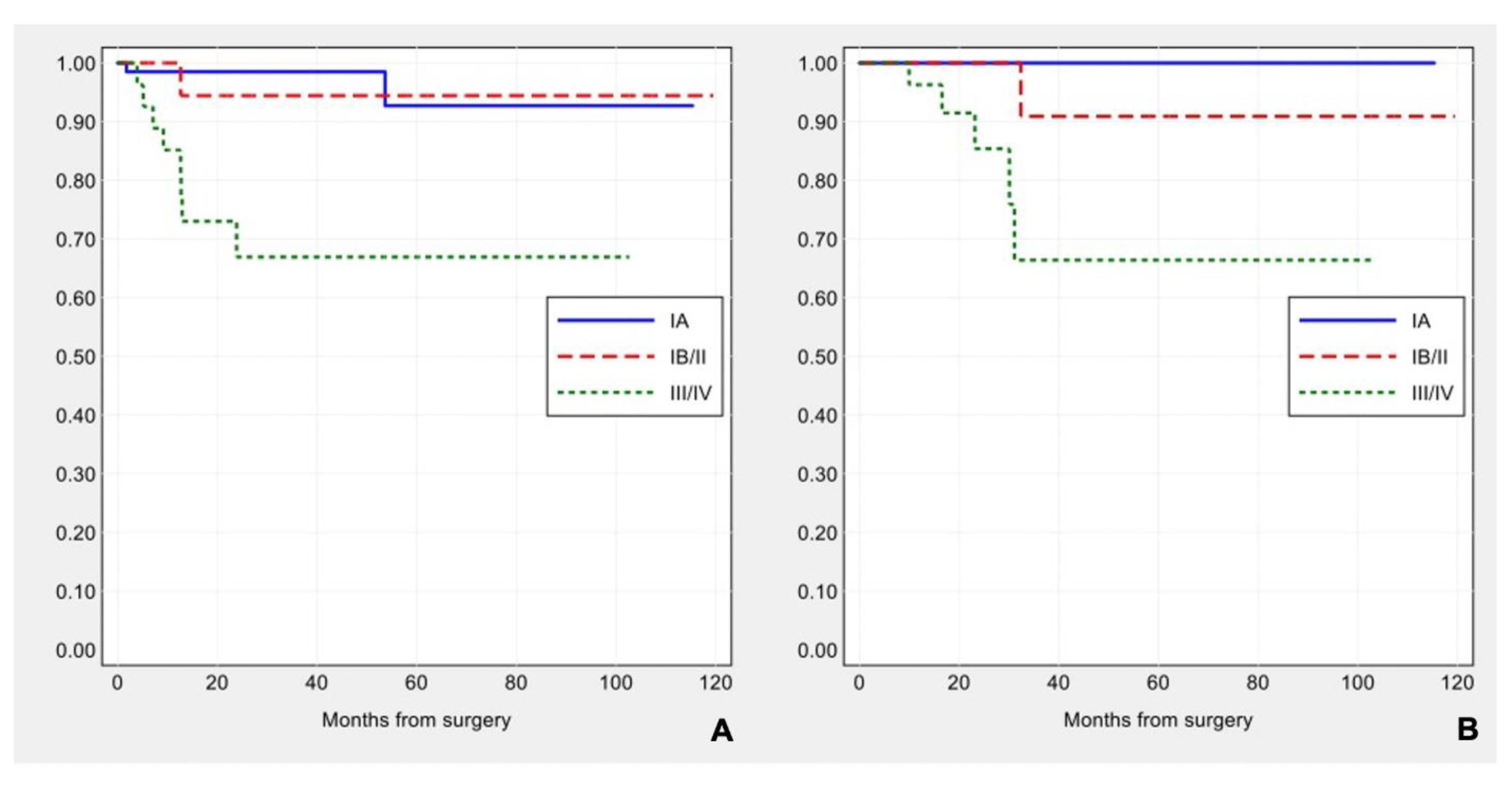
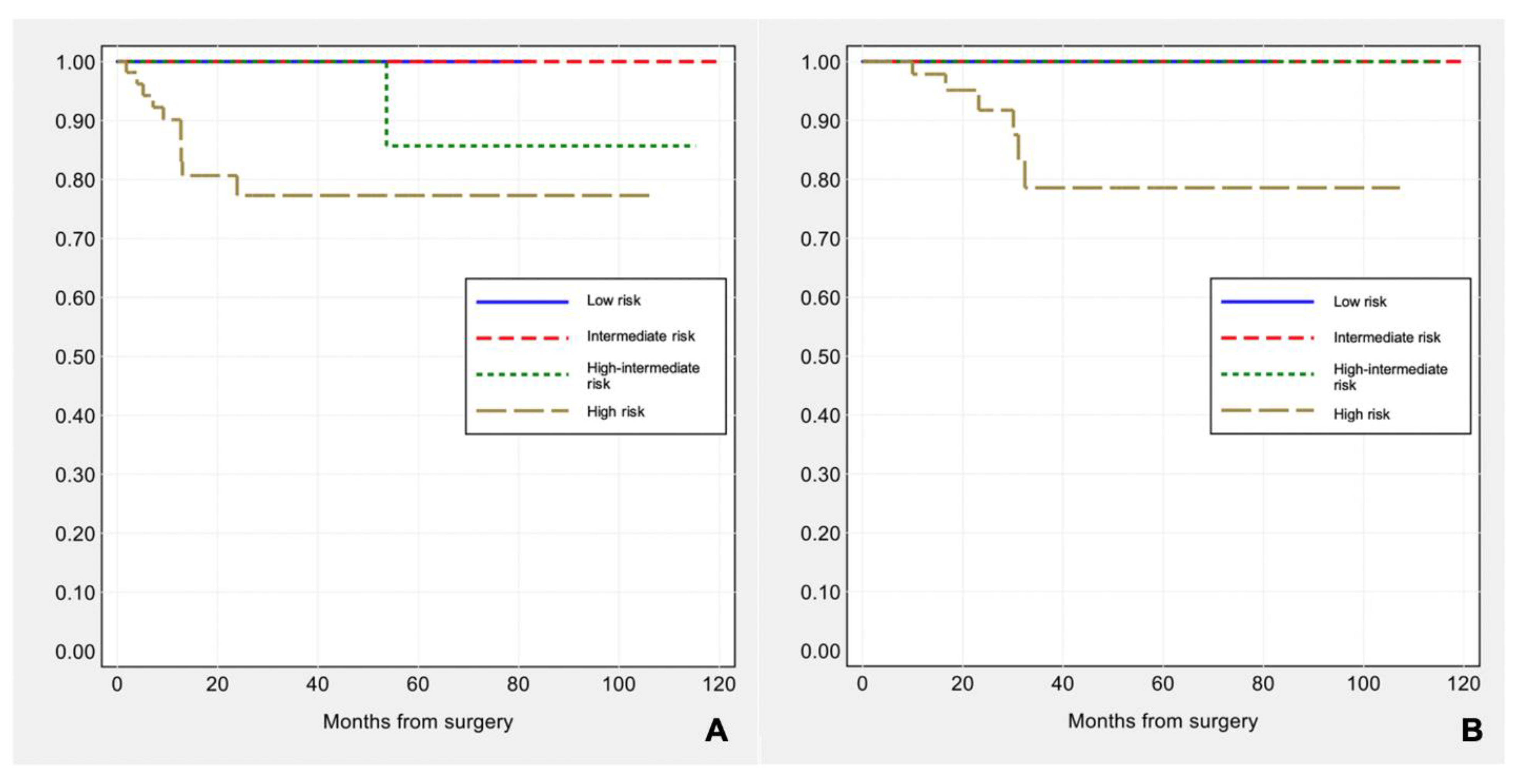
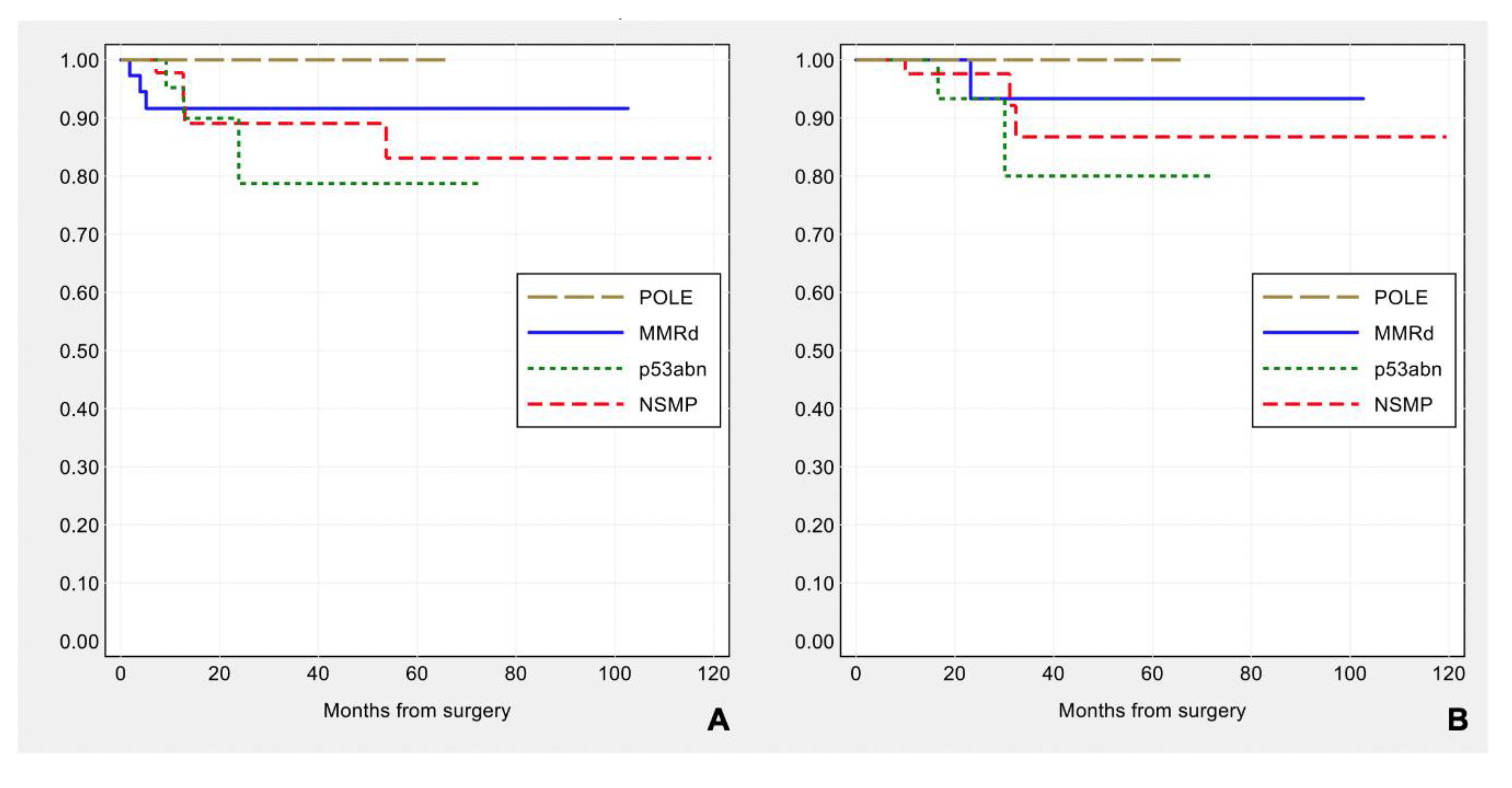
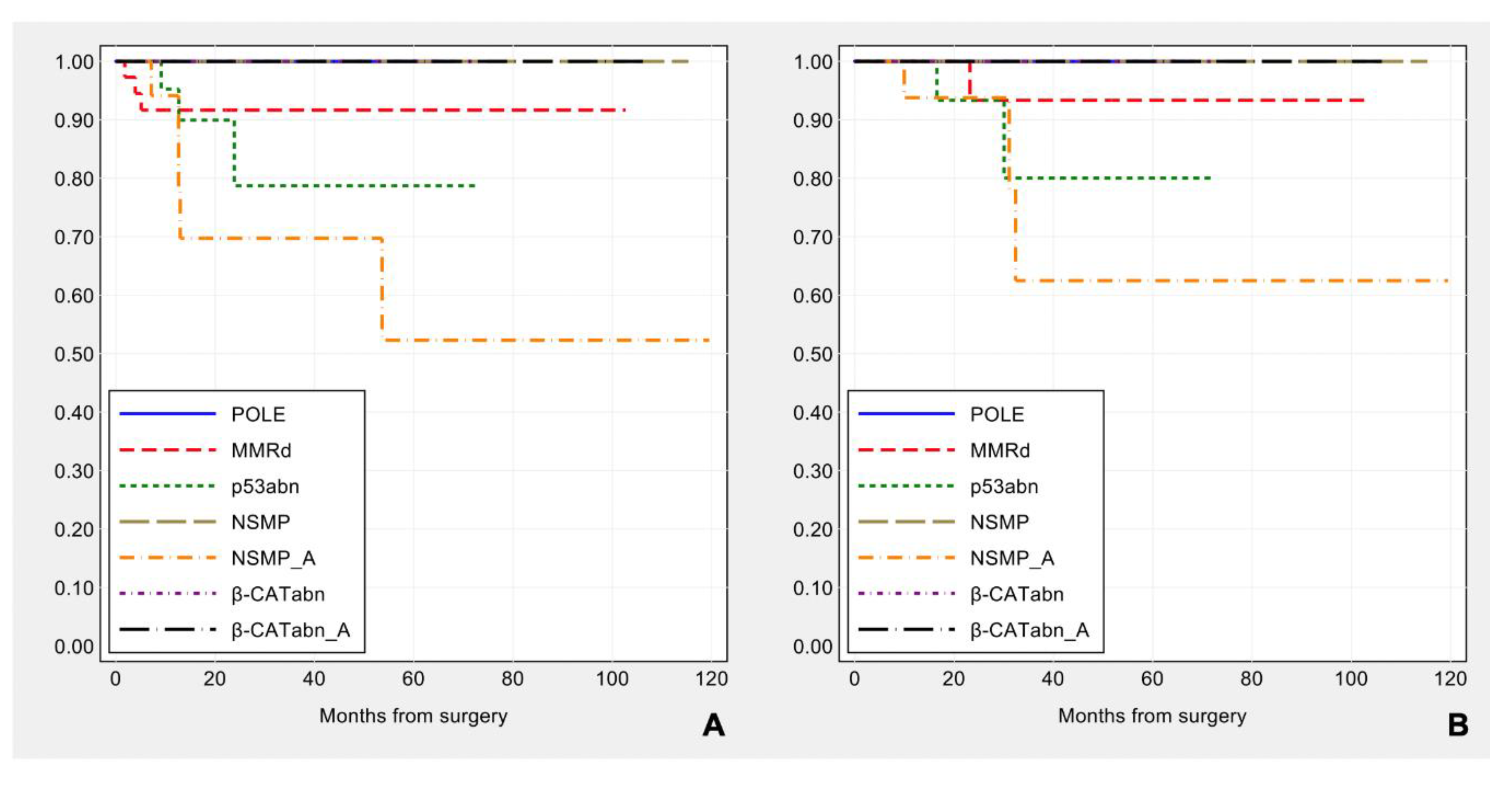
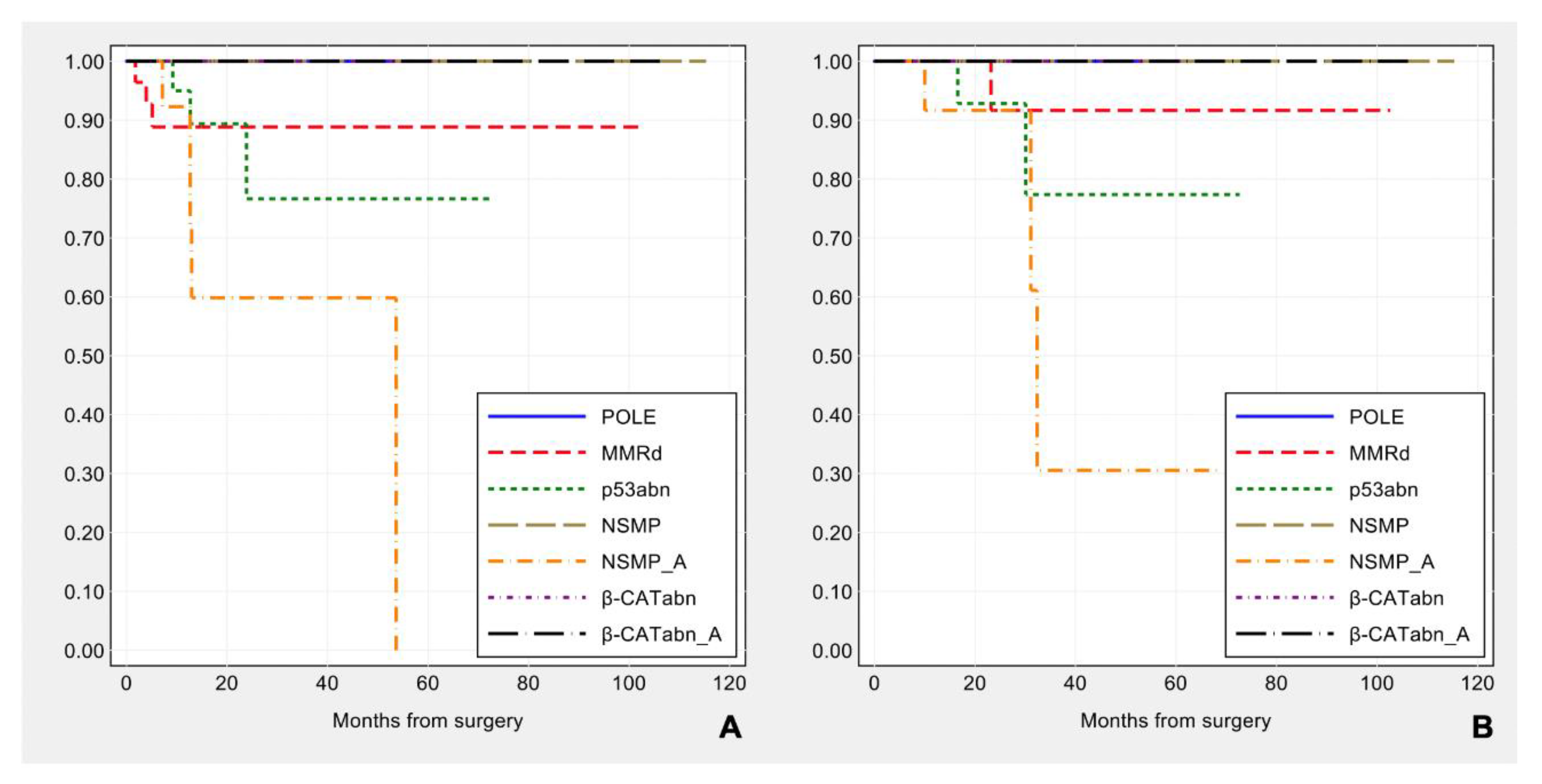
3.5. Correlation of Immuno-Molecular Subgroups with Clinical Outcome
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ferlay, J.; Colombet, M.; Soerjomataram, I.; Dyba, T.; Randi, G.; Bettio, M.; Gavin, A.; Visser, O.; Bray, F. Cancer incidence and mortality patterns in Europe: Estimates for 40 countries and 25 major cancers in 2018. Eur. J. Cancer 2018, 103, 356–387. [Google Scholar] [CrossRef]
- Allemani, C.; Matsuda, T.; Di Carlo, V.; Harewood, R.; Matz, M.; Nikšić, M.; Bonaventure, A.; Valkov, M.; Johnson, C.J.; Estève, J.; et al. Global surveillance of trends in cancer survival 2000-14 (CONCORD-3): Analysis of individual records for 37 513 025 patients diagnosed with one of 18 cancers from 322 population-based registries in 71 countries. Lancet 2018, 391, 1023–1075. [Google Scholar] [CrossRef] [Green Version]
- Gilks, C.B.; Oliva, E.; Soslow, R.A. Poor interobserver reproducibility in the diagnosis of high-grade endometrial carcinoma. Am. J. Surg. Pathol. 2013, 37, 874–881. [Google Scholar] [CrossRef] [PubMed]
- Kandoth, C.; Schultz, N.; Cherniack, A.D.; Akbani, R.; Liu, Y.; Shen, H.; Robertson, A.G.; Pashtan, I.; Shen, R.; Benz, C.C.; et al. Integrated genomic characterization of endometrial carcinoma. Nature 2013, 497, 67–73. [Google Scholar]
- Stelloo, E.; Nout, R.A.; Osse, E.M.; Jurgenliemk-Schulz, I.J.; Jobsen, J.J.; Lutgens, L.C.; van der Steen-Banasik, E.M.; Nijman, H.W.; Putter, H.; Bosse, T. Improved Risk Assessment by Integrating Molecular and Clinicopathological Factors in Early-stage Endometrial Cancer-Combined Analysis of the PORTEC Cohorts. Clin. Cancer Res. 2016, 22, 4215–4224. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Talhouk, A.; McConechy, M.K.; Leung, S.; Li-Chang, H.H.; Kwon, J.S.; Melnyk, N.; Yang, W.; Senz, J.; Boyd, N.; Karnezis, A.N.; et al. A clinically applicable molecular-based classification for endometrial cancers. Br. J. Cancer 2015, 113, 299–310. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Talhouk, A.; McConechy, M.K.; Leung, S.; Yang, W.; Lum, A.; Senz, J.; Boyd, N.; Pike, J.; Anglesio, M.; Kwon, J.S.; et al. Confirmation of ProMisE: A simple, genomics-based clinical classifier for endometrial cancer. Cancer 2017, 123, 802–813. [Google Scholar] [CrossRef] [Green Version]
- Kurnit, K.C.; Kim, G.N.; Fellman, B.M.; Urbauer, D.L.; Mills, G.B.; Zhang, W.; Broaddus, R.R. CTNNB1 (beta-catenin) mutation identifies low grade, early stage endometrial cancer patients at increased risk of recurrence. Mod. Pathol. 2017, 30, 1032–1041. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, Y.; Patel, L.; Mills, G.B.; Lu, K.H.; Sood, A.K.; Ding, L.; Kucherlapati, R.; Mardis, E.R.; Levine, D.A.; Shmulevich, I.; et al. Clinical significance of CTNNB1 mutation and Wnt pathway activation in endometrioid endometrial carcinoma. J. Natl. Cancer Inst. 2014, 106. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wilson, B.G.; Roberts, C.W. SWI/SNF nucleosome remodellers and cancer. Nat. Rev. Cancer. 2011, 11, 481–492. [Google Scholar] [CrossRef]
- Shen, J.; Peng, Y.; Wei, L.; Zhang, W.; Yang, L.; Lan, L.; Kapoor, P.; Ju, Z.; Mo, Q.; Shih, I.; et al. ARID1A Deficiency Impairs the DNA Damage Checkpoint and Sensitizes Cells to PARP Inhibitors. Cancer Discov. 2015, 5, 752–767. [Google Scholar] [CrossRef] [Green Version]
- Mathur, R. ARID1A loss in cancer: Towards a mechanistic understanding. Pharmacol Ther. 2018, 190, 15–23. [Google Scholar] [CrossRef] [PubMed]
- Guan, B.; Mao, T.L.; Panuganti, P.K.; Kuhn, E.; Kurman, R.J.; Maeda, D.; Chen, E.; Jeng, Y.M.; Wang, T.L.; Shih, I. Mutation and loss of expression of ARID1A in uterine low-grade endometrioid carcinoma. Am. J. Surg. Pathol. 2011, 35, 625–632. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rahman, M.; Nakayama, K.; Rahman, M.T.; Katagiri, H.; Katagiri, A.; Ishibashi, T.; Ishikawa, M.; Iida, K.; & Miyazaki, K. Clinicopathologic analysis of loss of AT-rich interactive domain 1A expression in endometrial cancer. Hum. Pathol. 2013, 44, 103–109. [Google Scholar] [CrossRef]
- Wiegand, K.C.; Lee, A.F.; Al-Agha, O.M.; Chow, C.; Kalloger, S.E.; Scott, D.W.; Steidl, C.; Wiseman, S.M.; Gascoyne, R.D.; Gilks, B.; et al. Loss of BAF250a (ARID1A) is frequent in high-grade endometrial carcinomas. J. Pathol. 2011, 224, 328–333. [Google Scholar] [CrossRef] [PubMed]
- Allo, G.; Bernardini, M.Q.; Wu, R.C.; Shih, I.M.; Kalloger, S.; Pollett, A.; Gilks, C.B.; Clarke, B.A. ARID1A loss correlates with mismatch repair deficiency and intact p53 expression in high-grade endometrial carcinomas. Mod. Pathol. 2014, 27, 255–261. [Google Scholar] [CrossRef] [Green Version]
- Bosse, T.; ter Haar, N.T.; Seeber, L.M.; Diest, P.J.V.; Hes, F.J.; Vasen, H.F.; Nout, R.A.; Creutzberg, C.L.; Morreau, H.; Smit, V.T. Loss of ARID1A expression and its relationship with PI3K-Akt pathway alterations, TP53 and microsatellite instability in endometrial cancer. Mod. Pathol. 2013, 26, 1525–1535. [Google Scholar] [CrossRef] [Green Version]
- Yen, T.T.; Miyamoto, T.; Asaka, S.; Chui, M.H.; Wang, Y.; Lin, S.F.; Stone, R.L.; Fader, A.N.; Asaka, R.; Kashima, H.; et al. Loss of ARID1A expression in endometrial samplings is associated with the risk of endometrial carcinoma. Gynecol. Oncol. 2018, 150, 426–431. [Google Scholar] [CrossRef]
- Wilson, M.R.; Reske, J.J.; Holladay, J.; Wilber, G.E.; Rhodes, M.; Koeman, J.; Adams, M.; Johnson, B.; Su, R.W.; Joshi, N.R.; et al. ARID1A and PI3-kinase pathway mutations in the endometrium drive epithelial transdifferentiation and collective invasion. Nat. Commun. 2019, 10, 3554. [Google Scholar] [CrossRef] [PubMed]
- Colombo, N.; Creutzberg, C.; Amant, F.; Bosse, T.; Gonzalez-Martin, A.; Ledermann, J.; Marth, C.; Nout, R.; Querleu, D.; Mirza, M.R.; et al. ESMO-ESGO-ESTRO Consensus Conference on Endometrial Cancer: Diagnosis, treatment and follow-up. Ann. Oncol. 2016, 27, 16–41. [Google Scholar] [CrossRef]
- Perrone, A.M.; Di Marcoberardino, B.; Rossi, M.; Pozzati, F.; Pellegrini, A.; Procaccini, M.; Santini, D.; De Iaco, P. Laparoscopic versus laparotomic approach to endometrial cancer. Eur. J. Gynaecol. Oncol. 2012, 33, 376–381. [Google Scholar]
- The WHO Classification of Tumours Editorial Board. WHO Classification of Tumours, Female Genital Tumours, 5th ed.; IARC: Lyon, France, 2020; Volume 4. [Google Scholar]
- FIGO: 27th volume of the ANNUAL REPORT on the Results of Treatment in Gynecological Cancer. Int. J. Gynaecol. Obstet. 2006, 95 (Suppl. 1), 23.
- Murray, S.K.; Young, R.H.; Scully, R.E. Unusual epithelial and stromal changes in myoinvasive endometrioid adenocarcinoma: A study of their frequency, associated diagnostic problems, and prognostic significance. Int. J. Gynecol. Pathol. 2003, 22, 324–333. [Google Scholar] [CrossRef]
- Euscher, E.; Fox, P.; Bassett, R.; Al-Ghawi, H.; Ali-Fehmi, R.; Barbuto, D.; Djordjevic, B.; Frauenhoffer, E.; Kim, I.; Hong, S.R.; et al. The pattern of myometrial invasion as a predictor of lymph node metastasis or extrauterine disease in low-grade endometrial carcinoma. Am. J. Surg. Pathol. 2013, 37, 1728–1736. [Google Scholar] [CrossRef] [PubMed]
- Bosse, T.; Peters, E.E.; Creutzberg, C.L.; Jurgenliemk-Schulz, I.M.; Jobsen, J.J.; Mens, J.W.; Lutgens, L.C.; van der Steen-Banasik, E.M.; Smit, V.T.; Nout, R.A. Substantial lymph-vascular space invasion (LVSI) is a significant risk factor for recurrence in endometrial cancer--A pooled analysis of PORTEC 1 and 2 trials. Eur. J. Cancer 2015, 51, 1742–1750. [Google Scholar] [CrossRef] [PubMed]
- Fujimoto, T.; Nanjyo, H.; Fukuda, J.; Nakamura, A.; Mizunuma, H.; Yaegashi, N.; Sugiyama, T.; Kurachi, H.; Sato, A.; Tanaka, T. Endometrioid uterine cancer: Histopathological risk factors of local and distant recurrence. Gynecol. Oncol. 2009, 112, 342–347. [Google Scholar] [CrossRef] [PubMed]
- Shia, J.; Black, D.; Hummer, A.J.; Boyd, J.; Soslow, R.A. Routinely assessed morphological features correlate with microsatellite instability status in endometrial cancer. Hum. Pathol. 2008, 39, 116–125. [Google Scholar] [CrossRef]
- Hendry, S.; Salgado, R.; Gevaert, T.; Russell, P.A.; John, T.; Thapa, B.; Christie, M.; van de Vijver, K.; Estrada, M.V.; Gonzalez-Ericsson, P.I.; et al. Assessing Tumor-Infiltrating Lymphocytes in Solid Tumors: A Practical Review for Pathologists and Proposal for a Standardized Method from the International Immuno-Oncology Biomarkers Working Group: Part 2: TILs in Melanoma, Gastrointestinal Tract Carcinomas, Non-Small Cell Lung Carcinoma and Mesothelioma, Endometrial and Ovarian Carcinomas, Squamous Cell Carcinoma of the Head and Neck, Genitourinary Carcinomas, and Primary Brain Tumors. Adv. Anat. Pathol. 2017, 24, 311–335. [Google Scholar]
- Singh, N.; Piskorz, A.M.; Bosse, T.; Jimenez-Linan, M.; Rous, B.; Brenton, J.D.; Gilks, C.B.; Köbel, M. p53 immunohistochemistry is an accurate surrogate for TP53 mutational analysis in endometrial carcinoma biopsies. J. Pathol. 2020, 250, 336–345. [Google Scholar] [CrossRef]
- Garg, K.; Broaddus, R.R.; Soslow, R.A.; Urbauer, D.L.; Levine, D.A.; Djordjevic, B. Pathologic scoring of PTEN immunohistochemistry in endometrial carcinoma is highly reproducible. Int. J. Gynecol. Pathol. 2012, 31, 48–56. [Google Scholar] [CrossRef] [Green Version]
- Nei, H.; Saito, T.; Yamasaki, H.; Mizumoto, H.; Ito, E.; Kudo, R. Nuclear localization of beta-catenin in normal and carcinogenic endometrium. Mol. Carcinog. 1999, 25, 207–218. [Google Scholar] [CrossRef]
- Travaglino, A.; Raffone, A.; Saccone, G.; De Luca, C.; Mollo, A.; Mascolo, M.; De Placido, G.; Insabato, L.; Zullo, F. Immunohistochemical Nuclear Expression of beta-Catenin as a Surrogate of CTNNB1 Exon 3 Mutation in Endometrial Cancer. Am. J. Clin. Pathol. 2019, 151, 529–538. [Google Scholar] [CrossRef]
- Dondi, G.; Coluccelli, S.; De Leo, A.; Ferrari, S.; Gruppioni, E.; Bovicelli, A.; Godino, L.; Coadă, C.A.; Morganti, A.G.; Giordano, A.; et al. An Analysis of Clinical, Surgical, Pathological and Molecular Characteristics of Endometrial Cancer According to Mismatch Repair Status. A Multidisciplinary Approach. Int. J. Mol. Sci. 2020, 21, 7188. [Google Scholar] [CrossRef] [PubMed]
- de Biase, D.; Acquaviva, G.; Visani, M.; Sanza, V.; Argento, C.M.; De Leo, A.; Maloberti, T.; Pession, A.; Tallini, G. Molecular Diagnostic of Solid Tumor Using a Next Generation Sequencing Custom-Designed Multi-Gene Panel. Diagnostics 2020, 10, 250. [Google Scholar] [CrossRef]
- van Roon, E.H.; van Puijenbroek, M.; Middeldorp, A.; van Eijk, R.; de Meijer, E.J.; Erasmus, D.; Wouters, K.A.; van Engeland, M.; Oosting, J.; Hes, F.J.; et al. Early onset MSI-H colon cancer with MLH1 promoter methylation, is there a genetic predisposition? BMC Cancer 2010, 10, 180. [Google Scholar] [CrossRef] [Green Version]
- Leon-Castillo, A.; Britton, H.; McConechy, M.K.; McAlpine, J.N.; Nout, R.; Kommoss, S.; Brucker, S.Y.; Carlson, J.W.; Epstein, E.; Rau, T.T.; et al. Interpretation of somatic POLE mutations in endometrial carcinoma. J. Pathol. 2020, 250, 323–335. [Google Scholar] [CrossRef]
- Kommoss, S.; McConechy, M.K.; Kommoss, F.; Leung, S.; Bunz, A.; Magrill, J.; Britton, H.; Kommoss, F.; Grevenkamp, F.; Karnezis, A.; et al. Final validation of the ProMisE molecular classifier for endometrial carcinoma in a large population-based case series. Ann. Oncol. 2018, 29, 1180–1188. [Google Scholar] [CrossRef]
- Stelloo, E.; Bosse, T.; Nout, R.A.; MacKay, H.J.; Church, D.N.; Nijman, H.W.; Leary, A.; Edmondson, R.J.; Powell, M.E.; Crosbie, E.J.; et al. Refining prognosis and identifying targetable pathways for high-risk endometrial cancer; a TransPORTEC initiative. Mod. Pathol. 2015, 28, 836–844. [Google Scholar] [CrossRef] [Green Version]
- Raffone, A.; Travaglino, A.; Mascolo, M.; Carbone, L.; Guida, M.; Insabato, L.; Zullo, F. TCGA molecular groups of endometrial cancer: Pooled data about prognosis. Gynecol. Oncol. 2019, 155, 374–383. [Google Scholar] [CrossRef]
- Espinosa, I.; De Leo, A.; D’Angelo, E.; Rosa-Rosa, J.M.; Corominas, M.; Gonzalez, A.; Palacios, J.; Prat, J. Dedifferentiated endometrial carcinomas with neuroendocrine features: A clinicopathologic, immunohistochemical, and molecular genetic study. Hum. Pathol. 2018, 72, 100–106. [Google Scholar] [CrossRef] [PubMed]
- Kim, G.; Kurnit, K.C.; Djordjevic, B.; Singh, C.; Munsell, M.F.; Wang, W.L.; Lazar, A.J.; Zhang, W.; Broaddus, R. Nuclear beta-catenin localization and mutation of the CTNNB1 gene: A context-dependent association. Mod. Pathol. 2018, 31, 1553–1559. [Google Scholar] [CrossRef] [PubMed]
- Roque, D.R.; Makowski, L.; Chen, T.H.; Rashid, N.; Hayes, D.N.; Bae-Jump, V. Association between differential gene expression and body mass index among endometrial cancers from The Cancer Genome Atlas Project. Gynecol. Oncol. 2016, 142, 317–322. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shen, J.; Ju, Z.; Zhao, W.; Wang, L.; Peng, Y.; Ge, Z.; Nagel, Z.D.; Zou, J.; Wang, C.; Kapoor, P.; et al. ARID1A deficiency promotes mutability and potentiates therapeutic antitumor immunity unleashed by immune checkpoint blockade. Nat. Med. 2018, 24, 556–562. [Google Scholar] [CrossRef] [PubMed]
- Okamura, R.; Kato, S.; Lee, S.; Jimenez, R.E.; Sicklick, J.K.; Kurzrock, R. ARID1A alterations function as a biomarker for longer progression-free survival after anti-PD-1/PD-L1 immunotherapy. J. Immunother Cancer. 2020, 8, e000438. [Google Scholar] [CrossRef] [Green Version]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Clinicopathologic Characteristics | n = 125 (%) |
|---|---|
| Age, years | 62.7 ± 10.7 |
| [56–71] | |
| Body mass index, kg/m2 | 27.5 ± 6.6 |
| [22.8–30.1] | |
| Tumor type | |
| Endometrioid | 90 (72.0) |
| Dedifferentiated/Undifferentiated | 17 (13.6) |
| Serous | 15 (12.0) |
| Clear cell | 3 (2.4) |
| Grade | |
| 1 | 36 (28.8) |
| 2 | 35 (28.0) |
| 3 | 54 (43.2) |
| Depth of invasion | |
| <50% | 90 (72.0) |
| ≥50% | 35 (28.0) |
| Lymphovascular space invasion (LVSI) | |
| Absent | 88 (70.4) |
| Present | 37 (29.6) |
| Lymph node status | |
| Negative | 95 (76.0) |
| Positive | 24 (19.2) |
| Unknown/Not tested | 6 (4.8) |
| FIGO stage | |
| IA | 71 (56.8) |
| IB | 18 (14.4) |
| II | 4 (3.2) |
| III | 30 (24.0) |
| IV | 2 (1.6) |
| ESMO (2016) | |
| Low | 18 (14.4) |
| Intermediate | 8 (6.4) |
| High–Intermediate | 42 (33.6) |
| High | 57 (45.6) |
| Extensive necrosis | |
| Absent | 66 (52.8) |
| Present | 59 (47.2) |
| MELF | |
| Absent | 79 (63.2) |
| Present | 46 (36.8) |
| Tumor budding | |
| Absent | 73 (58.4) |
| Present | 52 (41.6) |
| sTILs | |
| Low | 36 (28.8) |
| High | 89 (71.2) |
| iTILs | |
| Low | 39 (31.2) |
| High | 86 (68.8) |
| Recurrence | |
| Absent | 114 (91.2) |
| Present | 11 (8.8) |
| Clinicopathologic Characteristics | POLE | MMRd | p53abn | NSMP | p-Value |
|---|---|---|---|---|---|
| (n = 9; 7.2%) | (n = 41; 32.8%) | (n = 26; 20.8%) | (n = 49; 39.2%) | ||
| Age, years | 61.2 ± 13.9 | 64.2 ± 10.0 | 65.0 ± 10.0 | 60.6 ± 11.0 | 0.266 |
| [52–71] | [57–73] | [59–74] | [55–69] | ||
| Body mass index, kg/m2 | 25.3 ± 4.6 | 26.8 ± 6.1 | 25.4 ± 4.1 | 29.5 ± 7.8 | 0.104 |
| [21.3–28.1] | [22.7–28.2] | [22.8–27.2] | [24.0–33.8] | ||
| Tumor type | <0.001 | ||||
| Endometrioid | 8 (88.9) | 30 (73.2) | 7 (26.9) | 45 (91.8) | |
| Dedifferentiated/ Undifferentiated | 1 (11.1) | 11 (26.8) | 1 (3.8) | 4 (8.2) | |
| Serous | 0 (0.0) | 0 (0.0) | 15 (57.7) | 0 (0.0) | |
| Clear cell | 0 (0.0) | 0 (0.0) | 3 (11.5) | 0 (0.0) | |
| Heterogeneity | 4 (44.4) | 21 (51.2) | 10 (38.5) | 14 (28.6) | 0.168 |
| Grade | <0.001 | ||||
| 1 | 2 (22.2) | 11 (26.8) | 1 (3.8) | 22 (44.9) | |
| 2 | 3 (33.3) | 14 (34.1) | 0 (0.0) | 18 (36.7) | |
| 3 | 4 (44.4) | 16 (39.0) | 25 (96.2) | 9 (18.4) | |
| Depth of invasion ≥50% | 1 (11.1) | 15 (36.6) | 9 (34.6) | 10 (20.4) | 0.208 |
| LVSI | 2 (22.2) | 14 (34.1) | 11 (42.3) | 10 (20.4) | 0.196 |
| Lymph node status | 0.141 | ||||
| Negative | 8 (88.9) | 31 (75.6) | 15 (57.7) | 41 (83.7) | |
| Positive | 1 (11.1) | 8 (19.5) | 10 (38.5) | 5 (10.2) | |
| FIGO stage | 0.011 | ||||
| IA | 5 (55.6) | 19 (46.3) | 12 (46.2) | 35 (71.4) | |
| IB/II | 2 (22.2) | 12 (29.3) | 1 (3.8) | 7 (14.3) | |
| III | 2 (22.2) | 9 (22.0) | 12 (46.2) | 7 (14.3) | |
| IV | 0 (0.0) | 1 (2.4) | 1 (3.8) | 0 (0.0) | |
| Extensive necrosis | 6 (66.7) | 23 (56.1) | 11 (42.3) | 19 (38.8) | 0.235 |
| MELF | 5 (55.6) | 24 (58.5) | 3 (11.5) | 14 (28.6) | <0.001 |
| Tumor budding | 7 (77.8) | 23 (56.1) | 8 (30.8) | 14 (28.6) | 0.004 |
| High sTILs | 9 (100.0) | 35 (85.4) | 19 (73.1) | 26 (53.1) | 0.001 |
| High iTILs | 9 (100.0) | 37 (90.2) | 17 (65.4) | 23 (46.9) | <0.001 |
| Mitoses/10 HPF | 78.1 ± 34.5 | 55.3 ± 23.7 | 86.3 ± 43.7 | 33.3 ± 27.7 | <0.001 |
| [50–103] | [40–70] | [45–130] | [10–42] | ||
| Ki67 proliferative index | 58.5 ± 14.9 | 57.9 ± 14.9 | 56.0 ± 16.7 | 36.6 ± 18.3 | <0.001 |
| [55.1–68.2] | [47.1–69.6] | [49.3–69.7] | [23.3–50.0] |
| Clinicopathologic Characteristics | POLE | MMRd | p53abn | β-CATabn | NSMP | p-Value |
|---|---|---|---|---|---|---|
| (n = 9; 7.2%) | (n = 41; 32.8%) | (n = 26; 20.8%) | (n = 16; 12.8%) | (n = 33; 26.4%) | ||
| Age, years | 61.2 ± 13.9 | 64.2 ± 10.0 | 65.0 ± 10.0 | 54.3 ± 12.9 | 63.6 ± 8.5 | 0.067 |
| [52–71] | [57–73] | [59–74] | [44–63] | [58–70] | ||
| Body mass index, kg/m2 | 25.3 ± 4.6 | 26.8 ± 6.1 | 25.4 ± 4.1 | 29.0 ± 6.7 | 29.7 ± 8.3 | 0.187 |
| [21.3–28.1] | [22.7–28.2] | [22.8–27.2] | [22.5–33.5] | [24.2–36.1] | ||
| Tumor type | <0.001 | |||||
| Endometrioid | 8 (88.9) | 30 (73.2) | 7 (26.9) | 14 (87.5) | 31 (93.9) | |
| Dedifferentiated/ Undifferentiated | 1 (11.1) | 11 (26.8) | 1 (3.8) | 2 (12.5) | 2 (6.1) | |
| Serous | 0 (0.0) | 0 (0.0) | 15 (57.7) | 0 (0) | 0 (0) | |
| Clear cell | 0 (0.0) | 0 (0.0) | 3 (11.5) | 0 (0) | 0 (0) | |
| Heterogeneity | 4 (44.4) | 21 (51.2) | 10 (38.5) | 5 (31.3) | 9 (27.3) | 0.290 |
| Grade | <0.001 | |||||
| 1 | 2 (22.2) | 11 (26.8) | 1 (3.8) | 8 (50.0) | 14 (42.4) | |
| 2 | 3 (33.3) | 14 (34.1) | 0 (0.0) | 5 (31.3) | 13 (39.4) | |
| 3 | 4 (44.4) | 16 (39.0) | 25 (96.2) | 3 (18.8) | 6 (18.2) | |
| Depth of invasion ≥50% | 1 (11.1) | 15 (36.6) | 9 (34.6) | 3 (18.8) | 7 (21.2) | 0.361 |
| LVSI | 2 (22.2) | 14 (34.1) | 11 (42.3) | 3 (18.8) | 7 (21.2) | 0.350 |
| Lymph node status | 0.193 | |||||
| Negative | 8 (88.9) | 31 (75.6) | 15 (57.7) | 15 (93.8) | 26 (78.8) | |
| Positive | 1 (11.1) | 8 (19.5) | 10 (38.5) | 1 (6.3) | 4 (12.1) | |
| Unknown/Not tested | 0 (0.0) | 2 (4.9) | 1 (3.8) | 0 (0.0) | 3 (9.1) | |
| FIGO stage | 0.048 | |||||
| IA | 5 (55.6) | 19 (46.3) | 12 (46.2) | 11 (68.8) | 24 (72.7) | |
| IB/II | 2 (22.2) | 12 (29.3) | 1 (3.8) | 3 (18.8) | 4 (12.1) | |
| III | 2 (22.2) | 9 (22.0) | 12 (46.2) | 2 (12.5) | 5 (15.2) | |
| IV | 0 (0.0) | 1 (2.4) | 1 (3.8) | 0 (0.0) | 0 (0.0) | |
| Extensive necrosis | 6 (66.7) | 23 (56.1) | 11 (42.3) | 4 (25.0) | 15 (45.5) | 0.195 |
| MELF | 5 (55.6) | 24 (58.5) | 3 (11.5) | 4 (25.0) | 10 (30.3) | 0.001 |
| Tumor budding | 7 (77.8) | 23 (56.1) | 8 (30.8) | 4 (25.0) | 10 (30.3) | 0.011 |
| High sTILs | 9 (100.0) | 35 (85.4) | 19 (73.1) | 7 (43.8) | 19 (57.6) | 0.002 |
| High iTILs | 9 (100.0) | 37 (90.2) | 17 (65.4) | 4 (25.0) | 19 (57.6) | <0.001 |
| Mitoses/10 HPF | 78.1 ± 34.5 | 55.3 ± 23.7 | 86.3 ± 43.7 | 30.5 ± 30.1 | 34.6 ± 26.8 | <0.001 |
| [50–103] | [40–70] | [45–130] | [9–44] | [20–40] | ||
| Ki67 proliferative index | 58.5 ± 14.9 | 57.9 ± 14.9 | 56.0 ± 16.7 | 35.9 ± 21.6 | 36.9 ± 16.6 | <0.001 |
| [55.1–68.2] | [47.1–69.6] | [49.3–69.7] | [17.1–58.4] | [25.3–42.7] |
| Clinicopathologic Characteristics | β-Catenin Abnormal Subgroup (n = 16; 32,7%) | NSMP Subgroup (n = 33; 67,3%) | ||||
|---|---|---|---|---|---|---|
| β-CATabn | β-CATabn_A | p-Value | NSMP | NSMP_A | p-Value | |
| (n = 9) | (n = 7) | (n = 14) | (n = 19) | |||
| Age, years | 49 ± 13 | 61 ± 10 | 0.044 | 66 ± 10 | 62 ± 7 | 0.352 |
| [40–54] | [55–73] | [55–75] | [58–69] | |||
| Body mass index, kg/m2 | 27.3 ± 7.8 | 31.1 ± 4.7 | 0.186 | 27.6 ± 6.1 | 31.3 ± 9.5 | 0.229 |
| [20.3–29.1] | [28.1–33.8] | [23.4–28.9] | [24.2–37.3] | |||
| Tumor type | 0.175 | 1.000 | ||||
| Endometrioid | 9 (100) | 5 (71) | 13 (93) | 18 (95) | ||
| Dedifferentiated/Undifferentiated | 0 (0) | 2 (29) | 1 (7) | 1 (5) | ||
| Heterogeneity | 1 (11) | 4 (57) | 0.106 | 2 (14) | 7 (37) | 0.241 |
| Grade | 0.001 | 0.391 | ||||
| 1 | 8 (89) | 0 (0) | 8 (57) | 6 (32) | ||
| 2 | 1 (11) | 4 (57) | 4 (29) | 9 (47) | ||
| 3 | 0 (0) | 3 (43) | 2 (14) | 4 (21) | ||
| Depth of invasion ≥50% | 0 (0) | 3 (43) | 0.062 | 3 (21) | 4 (21) | 1.000 |
| LVSI | 0 (0) | 3 (43) | 0.062 | 2 (14) | 5 (26) | 0.670 |
| Lymph node status | 0.437 | 0.830 | ||||
| Negative | 9 (100) | 6 (86) | 12 (86) | 14 (74) | ||
| Positive | 0 (0) | 1 (14) | 1 (7) | 3 (16) | ||
| Unknown/Not tested | 0 (0) | 0 (0) | 1 (7) | 2 (11) | ||
| FIGO stage | 0.758 | 1.000 | ||||
| IA | 7 (78) | 4 (57) | 10 (71) | 14 (74) | ||
| IB/II | 1 (11) | 2 (29) | 2 (14) | 2 (11) | ||
| III | 1 (11) | 1 (14) | 2 (14) | 3 (16) | ||
| Extensive necrosis | 0 (0) | 4 (57) | 0.019 | 6 (43) | 9 (47) | 1.000 |
| MELF | 2 (22) | 2 (29) | 1.000 | 3 (21) | 7 (37) | 0.455 |
| Tumor budding | 0 (0) | 4 (57) | 0.019 | 3 (21) | 7 (37) | 0.455 |
| High sTILs | 1 (11) | 6 (86) | 0.009 | 7 (50) | 12 (63) | 0.497 |
| High iTILs | 0 (0) | 4 (57) | 0.019 | 6 (43) | 13 (68) | 0.173 |
| Mitoses/10 HPF | 9.3 ± 4.8 | 57.7 ± 26.3 | 0.001 | 31.1 ± 33.7 | 37.2 ± 21.0 | 0.100 |
| [5–10] | [42–80] | [10–40] | [24–50] | |||
| Ki67 proliferative index | 20.7 ± 11.2 | 55.4 ± 14.5 | 0.003 | 31.4 ± 18.8 | 41.5 ± 13.5 | 0.037 |
| [13.8–29.6] | [49.5–64.8] | [19.3–36.9] | [33.7–42.7] | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
De Leo, A.; de Biase, D.; Lenzi, J.; Barbero, G.; Turchetti, D.; Grillini, M.; Ravegnini, G.; Angelini, S.; Zamagni, C.; Coluccelli, S.; et al. ARID1A and CTNNB1/β-Catenin Molecular Status Affects the Clinicopathologic Features and Prognosis of Endometrial Carcinoma: Implications for an Improved Surrogate Molecular Classification. Cancers 2021, 13, 950. https://doi.org/10.3390/cancers13050950
De Leo A, de Biase D, Lenzi J, Barbero G, Turchetti D, Grillini M, Ravegnini G, Angelini S, Zamagni C, Coluccelli S, et al. ARID1A and CTNNB1/β-Catenin Molecular Status Affects the Clinicopathologic Features and Prognosis of Endometrial Carcinoma: Implications for an Improved Surrogate Molecular Classification. Cancers. 2021; 13(5):950. https://doi.org/10.3390/cancers13050950
Chicago/Turabian StyleDe Leo, Antonio, Dario de Biase, Jacopo Lenzi, Giovanna Barbero, Daniela Turchetti, Marco Grillini, Gloria Ravegnini, Sabrina Angelini, Claudio Zamagni, Sara Coluccelli, and et al. 2021. "ARID1A and CTNNB1/β-Catenin Molecular Status Affects the Clinicopathologic Features and Prognosis of Endometrial Carcinoma: Implications for an Improved Surrogate Molecular Classification" Cancers 13, no. 5: 950. https://doi.org/10.3390/cancers13050950