
Risk Stratification for Immediate Postoperative Hearing Loss by Preoperative BAER (Brainstem Auditory Evoked Response) and Audiometry in NF2-Associated Vestibular Schwannomas

 , ,
, ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients and Clinics
2.2. Volumetry, Growth Rate, and Hearing
2.3. Data Evaluation
3. Results
3.1. Patients, Tumors, and Clinics
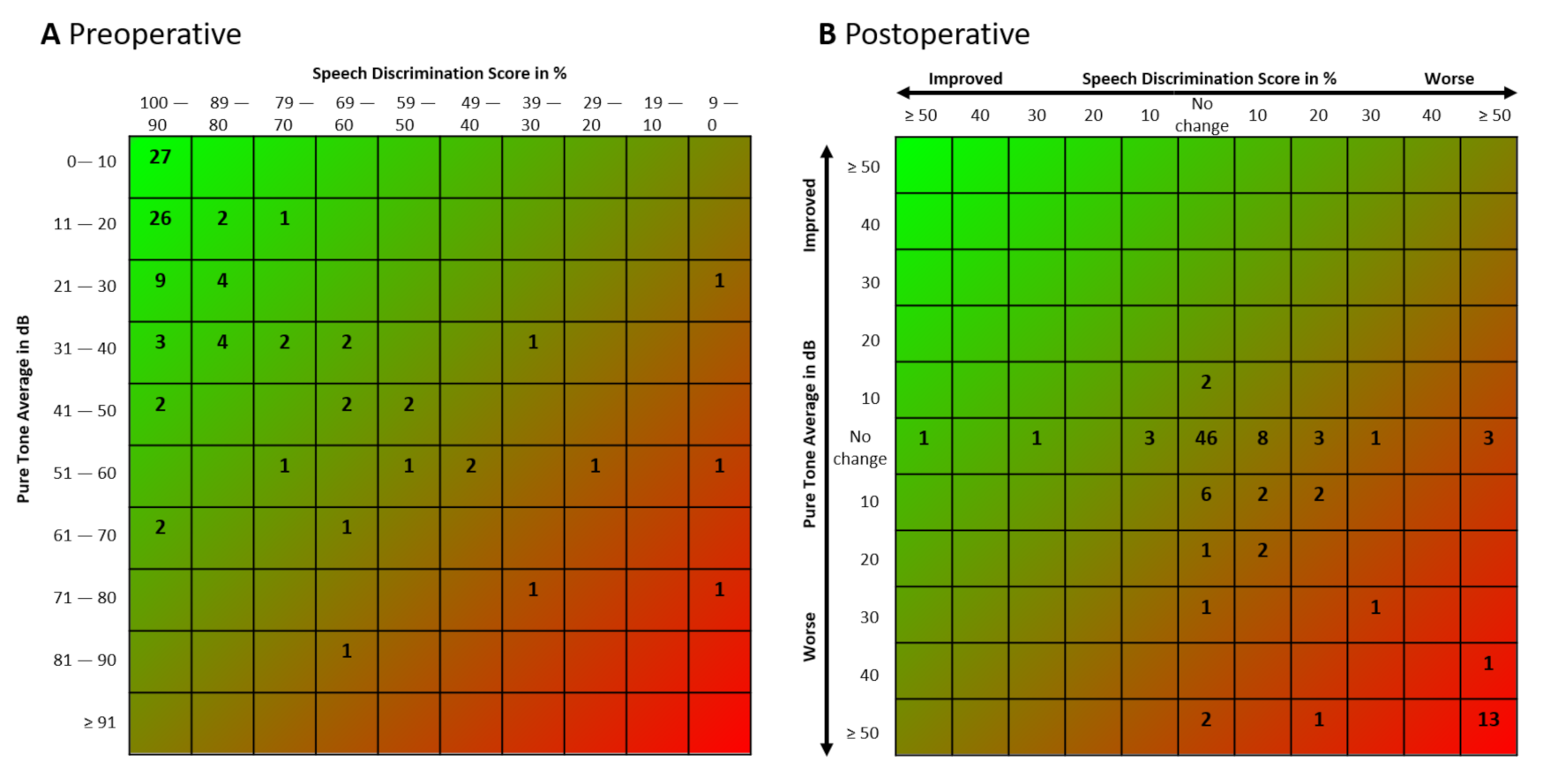
3.2. Immediate Postoperative Hearing Function
3.3. Prediction for Immediate Postoperative Hearing Deterioration or Complete Loss by Influencing Factors
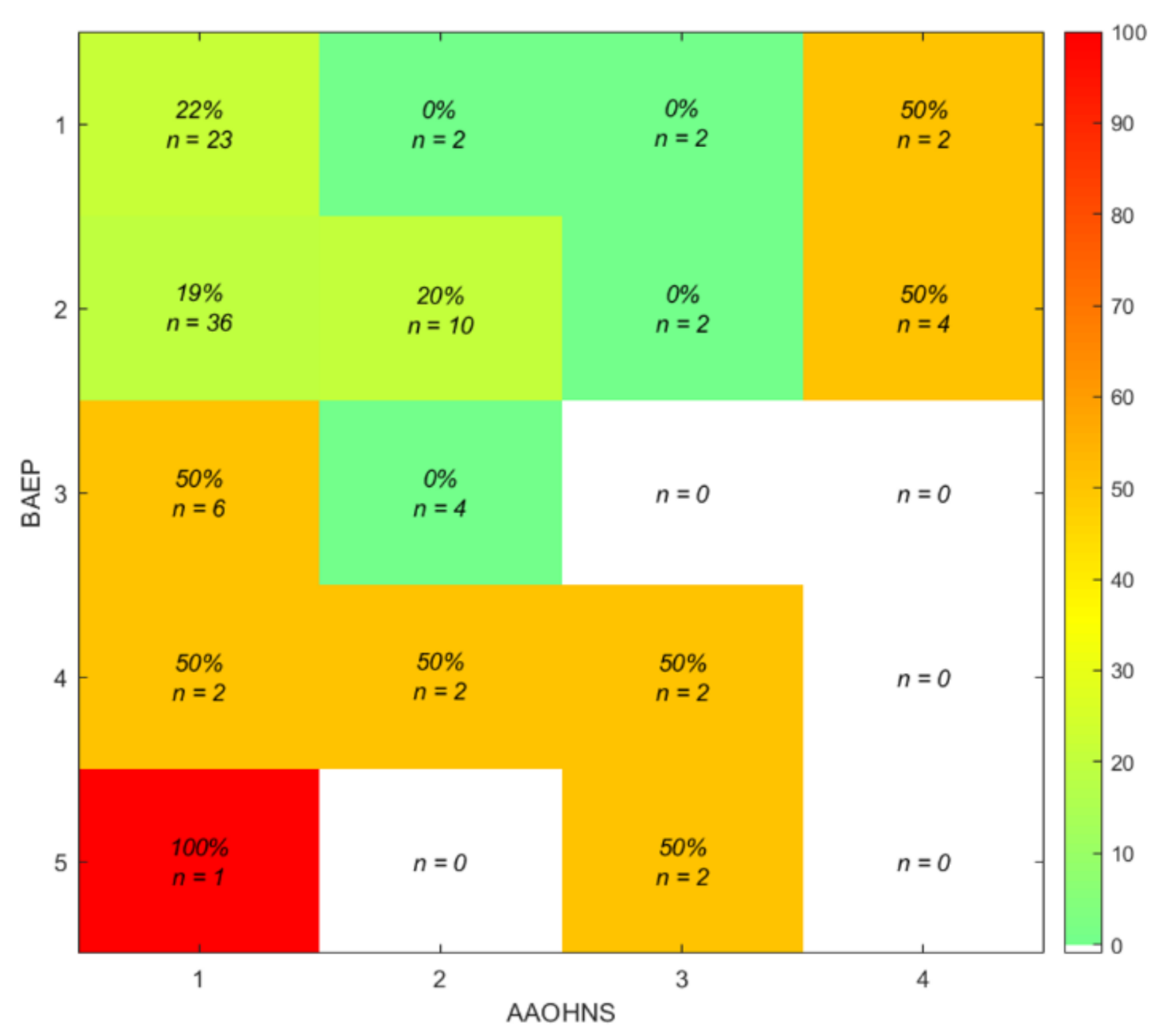
3.4. Prediction Model for Immediate Postoperative Hearing Deterioration or Complete Loss by Preoperative BAEP and AAO–HNS Class and Discrepant Cases
3.5. Prediction for Immediate Postoperative Hearing Preservation
3.6. Prediction Model for Immediate Postoperative Hearing Deterioration or Complete Loss by Resection Amount Categories
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Trofatter, J.A.; MacCollin, M.M.; Rutter, J.L.; Murrell, J.R.; Duyao, M.P.; Parry, D.M.; Eldridge, R.; Kley, N.; Menon, A.G.; Pulaski, K.; et al. A novel moesin-, ezrin-, radixin-like gene is a candidate for the neurofibromatosis 2 tumor suppressor. Cell 1993, 75, 826. [Google Scholar] [CrossRef]
- Rouleau, G.A.; Merel, P.; Lutchman, M.; Sanson, M.; Zucman, J.; Marineau, C.; Hoang-Xuan, K.; Demczuk, S.; Desmaze, C.; Plougastel, B.; et al. Alteration in a new gene encoding a putative membrane-organizing protein causes neuro-fibromatosis type 2. Nature 1993, 363, 515–521. [Google Scholar] [CrossRef]
- Evans, D.G.; Huson, S.M.; Donnai, D.; Neary, W.; Blair, V.; Newton, V.; Harris, R. A clinical study of type 2 neurofibromatosis. Q. J. Med. 1992, 84, 603–618. [Google Scholar]
- Mautner, V.F.; Lindenau, M.; Baser, M.E.; Hazim, W.; Tatagiba, M.; Haase, W.; Samii, M.; Wais, R.; Pulst, S.M. The neuroimaging and clinical spectrum of neurofibromatosis 2. Neurosurgery 1996, 38, 880–885. [Google Scholar] [CrossRef]
- Parry, D.M.; Eldridge, R.; Kaiser-Kupfer, M.I.; Bouzas, E.A.; Pikus, A.; Patronas, N. Neurofibromatosis 2 (NF2): Clinical characteristics of 63 affected individuals and clinical evidence for heterogeneity. Am. J. Med. Genet. 1994, 52, 450–461. [Google Scholar] [CrossRef] [PubMed]
- Gugel, I.; Mautner, V.F.; Kluwe, L.; Tatagiba, M.S.; Schuhmann, M.U. Cerebrovascular Insult as Presenting Symptom of Neurofibromatosis Type 2 in Children, Adolescents, and Young Adults. Front Neurol. 2018, 9, 733. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gugel, I.; Grimm, F.; Teuber, C.; Zipfel, J.; Tatagiba, M.; Mautner, V.F.; Schuhmann, M.U.; Kluwe, L. Presenting symptoms in children with neurofibromatosis type 2. Childs Nerv. Syst. 2020. [Google Scholar] [CrossRef] [PubMed]
- Halliday, D.; Emmanouil, B.; Pretorius, P.; MacKeith, S.; Painter, S.; Tomkins, H.; Evans, D.G.; Parry, A. Genetic Severity Score predicts clinical phenotype in NF2. J. Med. Genet. 2017, 54, 657–664. [Google Scholar] [CrossRef] [Green Version]
- Emmanouil, B.; Houston, R.; May, A.; Ramsden, J.D.; Hanemann, C.O.; Halliday, D.; Parry, A.; Mackeith, S. Progression of hearing loss in neurofibromatosis type 2 according to genetic severity. Laryngoscope 2018. [Google Scholar] [CrossRef]
- Gugel, I.; Grimm, F.; Liebsch, M.; Zipfel, J.; Teuber, C.; Kluwe, L.; Mautner, V.F.; Tatagiba, M.; Schuhmann, M.U. Impact of Surgery on Long-Term Results of Hearing in Neurofibromatosis Type-2 Associated Vestibular Schwannomas. Cancers 2019, 11, 91376. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gugel, I.; Grimm, F.; Teuber, C.; Kluwe, L.; Mautner, V.F.; Tatagiba, M.; Schuhmann, M.U. Management of NF2-associated vestibular schwannomas in children and young adults: Influence of surgery and clinical factors on tumor volume and growth rate. J. Neurosurg. Pediatr. 2019, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Plotkin, S.R.; Stemmer-Rachamimov, A.O.; Barker, F.G., 2nd; Halpin, C.; Padera, T.P.; Tyrrell, A.; Sorensen, A.G.; Jain, R.K.; di Tomaso, E. Hearing improvement after bevacizumab in patients with neurofibromatosis type 2. N. Engl. J. Med. 2009, 361, 358–367. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Plotkin, S.R.; Merker, V.L.; Halpin, C.; Jennings, D.; McKenna, M.J.; Harris, G.J.; Barker, F.G., 2nd. Bevacizumab for progressive vestibular schwannoma in neurofibromatosis type 2: A retrospective review of 31 patients. Otol. Neurotol. 2012, 33, 1046–1052. [Google Scholar] [CrossRef] [PubMed]
- Chung, L.K.; Nguyen, T.P.; Sheppard, J.P.; Lagman, C.; Tenn, S.; Lee, P.; Kaprealian, T.; Chin, R.; Gopen, Q.; Yang, I. A Systematic Review of Radiosurgery Versus Surgery for Neurofibromatosis Type 2 Vestibular Schwannomas. World Neurosurg. 2018, 109, 47–58. [Google Scholar] [CrossRef] [PubMed]
- Gugel, I.; Zipfel, J.; Hartjen, P.; Kluwe, L.; Tatagiba, M.; Mautner, V.F.; Schuhmann, M.U. Managing NF2-associated vestibular schwannomas in children and young adults: Review of an institutional series regarding effects of surgery and bevacizumab on growth rates, tumor volume, and hearing quality. Childs Nerv. Syst. 2020. [Google Scholar] [CrossRef] [PubMed]
- Gugel, I.; Kluwe, L.; Zipfel, J.; Teuber, C.; Tatagiba, M.; Mautner, V.F.; Schuhmann, M.U.; Grimm, F. Minimal Effect of Bevacizumab Treatment on Residual Vestibular Schwannomas after Partial Resection in Young Neurofibromatosis Type 2 Patients. Cancers 2019, 11, 1862. [Google Scholar] [CrossRef] [Green Version]
- Matthies, C.; Samii, M. Management of vestibular schwannomas (acoustic neuromas): The value of neurophysiology for intraoperative monitoring of auditory function in 200 cases. Neurosurgery 1997, 40, 459–466, Discussion 466–458. [Google Scholar]
- Matthies, C.; Samii, M. Management of vestibular schwannomas (acoustic neuromas): The value of neurophysiology for evaluation and prediction of auditory function in 420 cases. Neurosurgery 1997, 40, 919–929, Discussion 929–930. [Google Scholar] [CrossRef]
- Baser, M.E.; Friedman, J.M.; Joe, H.; Shenton, A.; Wallace, A.J.; Ramsden, R.T.; Evans, D.G. Empirical development of improved diagnostic criteria for neurofibromatosis 2. Genet. Med. 2011, 13, 576–581. [Google Scholar] [CrossRef] [Green Version]
- Samii, M.; Matthies, C. Management of 1000 vestibular schwannomas (acoustic neuromas): Hearing function in 1000 tumor resections. Neurosurgery 1997, 40, 248–260, Discussion 260–242. [Google Scholar] [CrossRef]
- Gardner, G.; Robertson, J.H. Hearing preservation in unilateral acoustic neuroma surgery. Ann. Otol. Rhinol. Laryngol. 1988, 97, 55–66. [Google Scholar] [CrossRef]
- Committee on Hearing and Equilibrium guidelines for the evaluation of hearing preservation in acoustic neuroma (vestibular schwannoma). American Academy of Otolaryngology-Head and Neck Surgery Foundation, INC. Otolaryngol. Head Neck. Surg. 1995, 113, 179–180. [CrossRef]
- Gurgel, R.K.; Jackler, R.K.; Dobie, R.A.; Popelka, G.R. A new standardized format for reporting hearing outcome in clinical trials. Otolaryngol. Head Neck. Surg. 2012, 147, 803–807. [Google Scholar] [CrossRef]
- Hosmer, D.W.; Lemeshow, S.; Sturdivant, R.X. Applied logistic regression; John Wiley & Sons: Hoboken, NJ, USA, 2013. [Google Scholar]
- Hummel, M.; Perez, J.; Hagen, R.; Gelbrich, G.; Ernestus, R.I.; Matthies, C. Auditory Monitoring in Vestibular Schwannoma Surgery: Intraoperative Development and Outcome. World Neurosurg. 2016, 96, 444–453. [Google Scholar] [CrossRef] [PubMed]
- Samii, M.; Matthies, C.; Tatagiba, M. Management of vestibular schwannomas (acoustic neuromas): Auditory and facial nerve function after resection of 120 vestibular schwannomas in patients with neurofibromatosis 2. Neurosurgery 1997, 40, 696–705. [Google Scholar] [CrossRef]
- Fan, D.; Ren, H.; Danzeng, D.; Li, H.; Wang, P. Influence of high-altitude hypoxic environments on the survival of cochlear hair cells and spiral ganglion neurons in rats. Biomed. Rep. 2016, 5, 681–685. [Google Scholar] [CrossRef] [Green Version]
- Tabuchi, K.; Nishimura, B.; Tanaka, S.; Hayashi, K.; Hirose, Y.; Hara, A. Ischemia-reperfusion injury of the cochlea: Pharmacological strategies for cochlear protection and implications of glutamate and reactive oxygen species. Curr. Neuropharmacol. 2010, 8, 128–134. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dilwali, S.; Landegger, L.D.; Soares, V.Y.; Deschler, D.G.; Stankovic, K.M. Secreted Factors from Human Vestibular Schwannomas Can Cause Cochlear Damage. Sci. Rep. 2015, 5, 18599. [Google Scholar] [CrossRef] [PubMed]
- Asthagiri, A.R.; Vasquez, R.A.; Butman, J.A.; Wu, T.; Morgan, K.; Brewer, C.C.; King, K.; Zalewski, C.; Kim, H.J.; Lonser, R.R. Mechanisms of hearing loss in neurofibromatosis type 2. PLoS ONE 2012, 7, e46132. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.Y.; Lee, J.H.; Goh, M.J.; Sung, Y.S.; Choi, Y.J.; Yoon, R.G.; Cho, S.H.; Ahn, J.H.; Park, H.J.; Baek, J.H. Clinical significance of an increased cochlear 3D fluid-attenuated inversion recovery signal intensity on an MR imaging examination in patients with acoustic neuroma. AJNR Am. J. Neuroradiol. 2014, 35, 1825–1829. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Category | Waves/Latency |
|---|---|
| 1 | Waves I, III, and V are present. Latency I–III is normal or slightly increased, (within 2 standard deviations or normal latency, 2.1 ± 0.28 milliseconds (ms). |
| 2 | Waves I, III, and V are present. Latency I–III is pathologically increased (>2.66 ms). |
| 3 | Waves I and V are present, and Wave III is lost. |
| 4 | Wave I is present or Wave V is present. |
| 5 | All waves are lost. |
| Sex (No of female/male) | 32/40 |
| Operation side (left/right) | 50/50 |
| Family history of NF2 (yes/no) | 16/56 |
| Detected mutation types in 36 patients | - |
| splicing mutations | 10 |
| nonsense mutations | 6 |
| frameshifting mutations | 14 |
| large genome alteration | 1 |
| missense mutations | 2 |
| large deletions | 3 |
| Age at diagnosis in years (mean ± SD, range) | 16 ± 9, 1–41 |
| Age at time of surgery in years (mean ± SD, range) | 22 ± 9, 8–47 |
| Tumor volume in cm3 (mean ± SD, range) | |
| preoperative | 4.51 ± 7.19, 0.11–33.92 |
| postoperative | 1.62 ± 2.79, 0–18.05 |
| significance | p < 0.001 |
| Growth rate in cm3/year (mean ± SD, range) | |
| preoperative | 0.87 ± 2.17, −0.18 to 14.96 |
| postoperative | 0.73 ± 2.29, −0.22 to 19.84 |
| significance | p = 0.341 |
| Resection amount categories | - |
| (1) only bony decompression of the IAC | 1 |
| (2) decompression of the IAC with laser coagulation (<10%) | 10 |
| (3) partial (<10% to <90%) | 61 |
| (3a) <10% | 12 |
| (3b) ≥10% to <30% | 14 |
| (3c) ≥30% to <50% | 15 |
| (3d) ≥50% to <70% | 15 |
| (3e) ≥70% to <90% | 13 |
| (4) subtotal (≥90% to <95%) | 3 |
| (5) near total (≥95% to <100%) | 7 |
| (6) total (100% including tumor capsule) | 6 |
| (7) growth progression | 7 |
| Not available | 5 |
| PTA in dB (mean ± SD, range) | - |
| preoperative | 24.14 ± 19, 1.25–81.25 |
| postoperative | 44.3 ± 42.4, 1.28–130 |
| significance | p < 0.001 |
| SDS in % (mean ± SD, range) | - |
| preoperative | 86 ± 23, 0–100 |
| postoperative | 69 ± 38, 0–100 |
| significance | p < 0.001 |
| G–R Scale [21] | Postoperative Class (No) | ||||
|---|---|---|---|---|---|
| Preoperative Class (No) | I (50) | II (20) | III (12) | IV (0) | V (18) |
| I (70) | 49 | 8 | 1 | 0 | 12 |
| II (18) | 1 | 11 | 4 | 0 | 2 |
| III (12) | 0 | 1 | 7 | 0 | 4 |
| IV (0) | 0 | 0 | 0 | 0 | 0 |
| V (0) | 0 | 0 | 0 | 0 | 0 |
| AAO–HNS Classification [22] | Postoperative Class (No) | ||||
| Preoperative Class (No) | A (49) | B (21) | C (6) | D (24) | - |
| A (68) | 48 | 9 | 1 | 10 | - |
| B (18) | 0 | 12 | 1 | 5 | |
| C (8) | 1 | 0 | 4 | 3 | |
| D (6) | 0 | 0 | 0 | 6 | |
| BAEP Classification System [18] | Postoperative Class (No) | ||||
| Preoperative Class (No) | I (18) | II (43) | III (11) | IV (8) | V (20) |
| I (29) | 14 | 9 | 1 | 1 | 4 |
| II (52) | 4 | 31 | 6 | 3 | 8 |
| III (10) | 0 | 3 | 4 | 1 | 2 |
| IV (6) | 0 | 0 | 0 | 3 | 3 |
| V (3) | 0 | 0 | 0 | 0 | 3 |
| Variables | B | S.E. | Wald | df | p | Odds Ratio | 95% CI for B | |
|---|---|---|---|---|---|---|---|---|
| LL | UL | |||||||
| Age at time of diagnosis in years | −0.029 | 0.045 | 0.412 | 1 | 0.521 | 0.972 | 0.891 | 1.060 |
| Preoperative GR in cm3/year | 0.018 | 0.264 | 0.005 | 1 | 0.946 | 1.081 | 0.607 | 1.708 |
| Preoperative volume in cm3 | 0.012 | 0.077 | 0.025 | 1 | 0.874 | 1.012 | 0.870 | 1.178 |
| Preoperative PTA in dB | 0.085 | 0.048 | 3.173 | 1 | 0.075 | 1.088 | 0.992 | 1.195 |
| Preoperative SDS in % | −0.021 | 0.034 | 0.378 | 1 | 0.539 | 0.979 | 0.915 | 1.047 |
| Preoperative AAO–HNS class | −1.377 | 1.292 | 1.135 | 1 | 0.287 | 0.252 | 0.020 | 3.178 |
| Preoperative BAEP class | 0.829 | 0.342 | 5.871 | 1 | 0.015 | 2.292 | 1.172 | 4.483 |
| Preoperative G–R class | −1.803 | 1.194 | 2.281 | 1 | 0.131 | 0.165 | 0.016 | 1.711 |
| Resection amount in % | 0.023 | 0.012 | 3.901 | 1 | 0.048 | 1.023 | 1.000 | 1.047 |
| Resection Amount Category | Immediate Postoperative Hearing Deterioration/Loss | Immediate Postoperative Hearing Preservation |
|---|---|---|
| 1 | n = 0 (0%) | n = 1 (100%) |
| 2 | n = 1 (10%) | n = 9 (90%) |
| 3 | n = 12 (20%) | n = 49 (80%) |
| 4 | n = 2 (67%) | n = 1 (33%) |
| 5 | n = 7 (100%) | n = 0 (0%) |
| 6 | n = 3 (50%) | n = 3 (50%) |
| 7 | n = 0 (0%) | n = 7 (100%) |
| Total | n = 25 (26%) | n = 70 (74%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gugel, I.; Grimm, F.; Hartjen, P.; Breun, M.; Zipfel, J.; Liebsch, M.; Löwenheim, H.; Ernemann, U.; Kluwe, L.; Mautner, V.-F.; et al. Risk Stratification for Immediate Postoperative Hearing Loss by Preoperative BAER (Brainstem Auditory Evoked Response) and Audiometry in NF2-Associated Vestibular Schwannomas. Cancers 2021, 13, 1384. https://doi.org/10.3390/cancers13061384
Gugel I, Grimm F, Hartjen P, Breun M, Zipfel J, Liebsch M, Löwenheim H, Ernemann U, Kluwe L, Mautner V-F, et al. Risk Stratification for Immediate Postoperative Hearing Loss by Preoperative BAER (Brainstem Auditory Evoked Response) and Audiometry in NF2-Associated Vestibular Schwannomas. Cancers. 2021; 13(6):1384. https://doi.org/10.3390/cancers13061384
Chicago/Turabian StyleGugel, Isabel, Florian Grimm, Philip Hartjen, Maria Breun, Julian Zipfel, Marina Liebsch, Hubert Löwenheim, Ulrike Ernemann, Lan Kluwe, Victor-Felix Mautner, and et al. 2021. "Risk Stratification for Immediate Postoperative Hearing Loss by Preoperative BAER (Brainstem Auditory Evoked Response) and Audiometry in NF2-Associated Vestibular Schwannomas" Cancers 13, no. 6: 1384. https://doi.org/10.3390/cancers13061384