
Continued versus Interrupted Targeted Therapy during Metastasis-Directed Stereotactic Radiotherapy: A Retrospective Multi-Center Safety and Efficacy Analysis

 , , , , , , ,
, , , , , , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
3. Results
3.1. Patient Characteristics
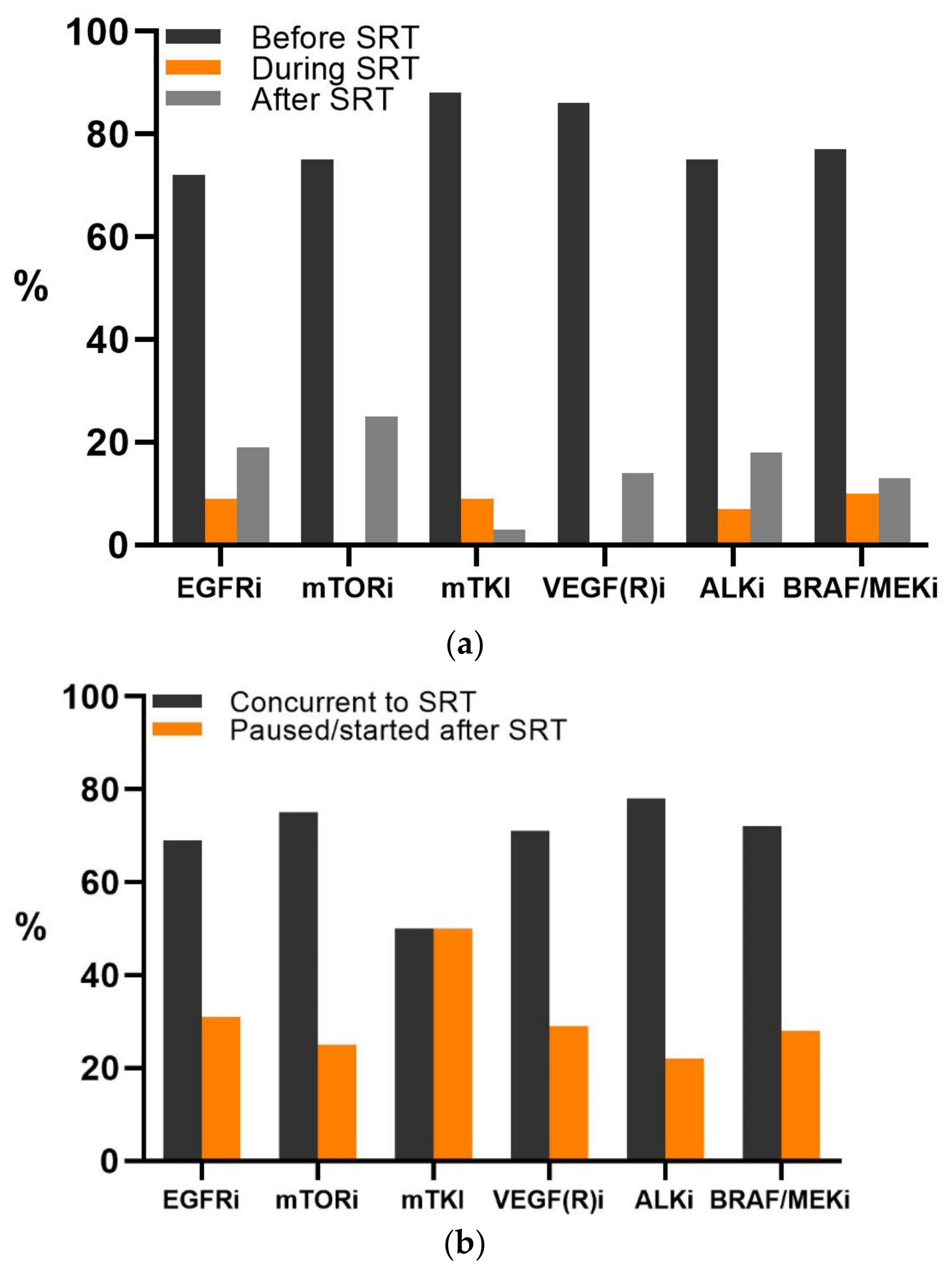
3.2. Targeted Therapy
3.3. Stereotactic Radiotherapy
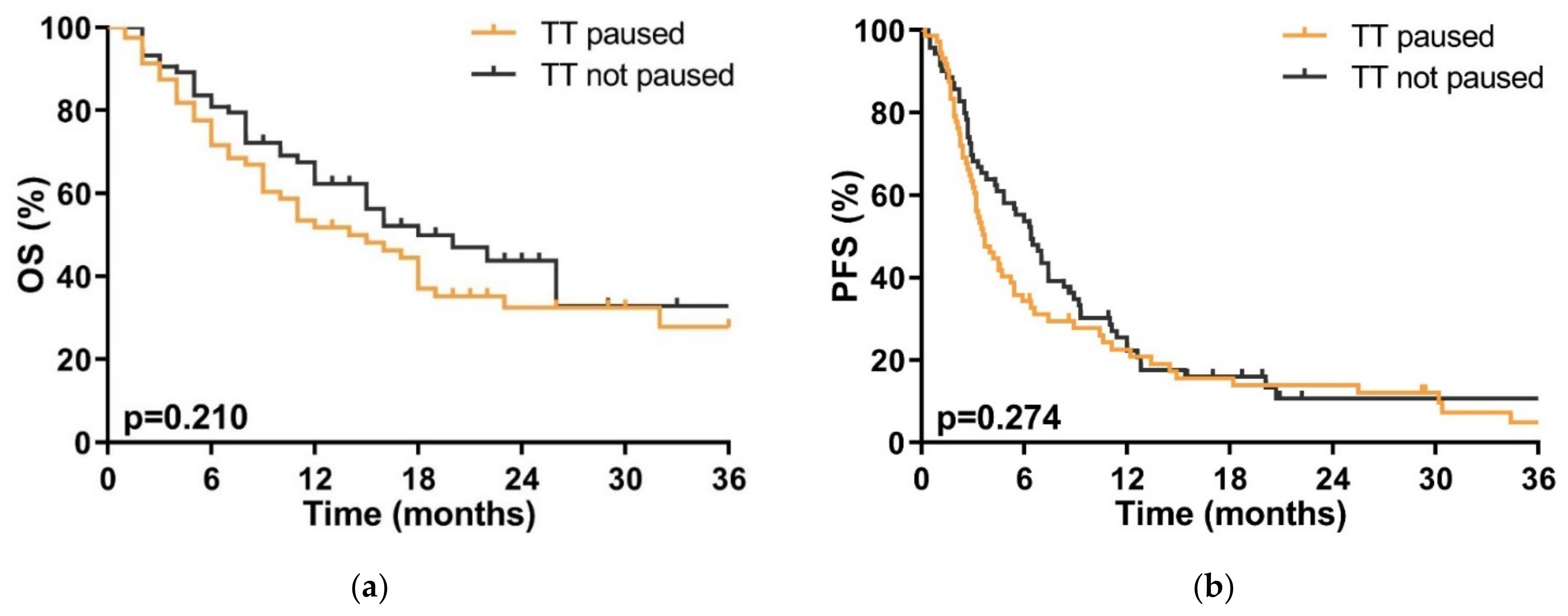
3.4. Efficacy
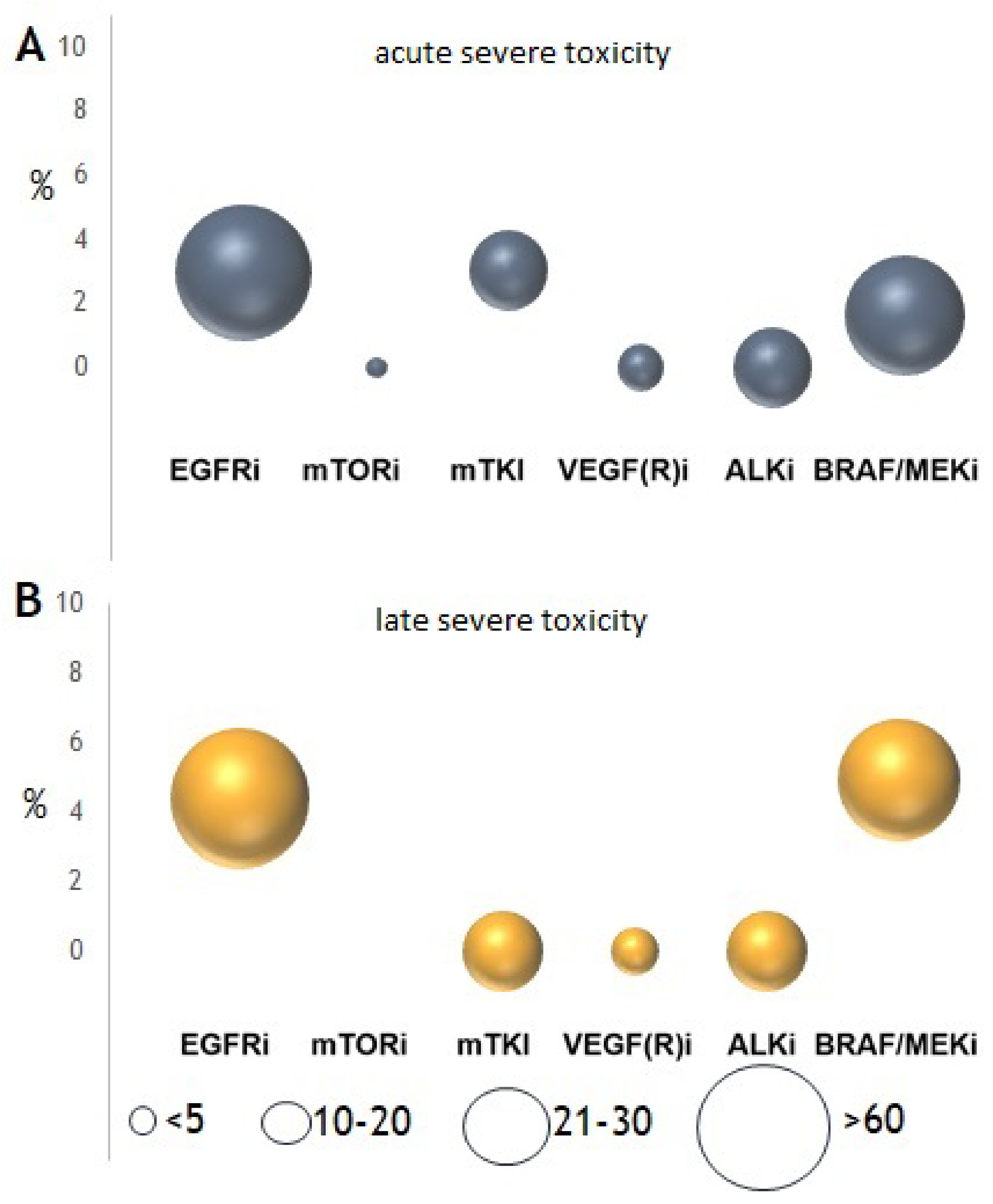
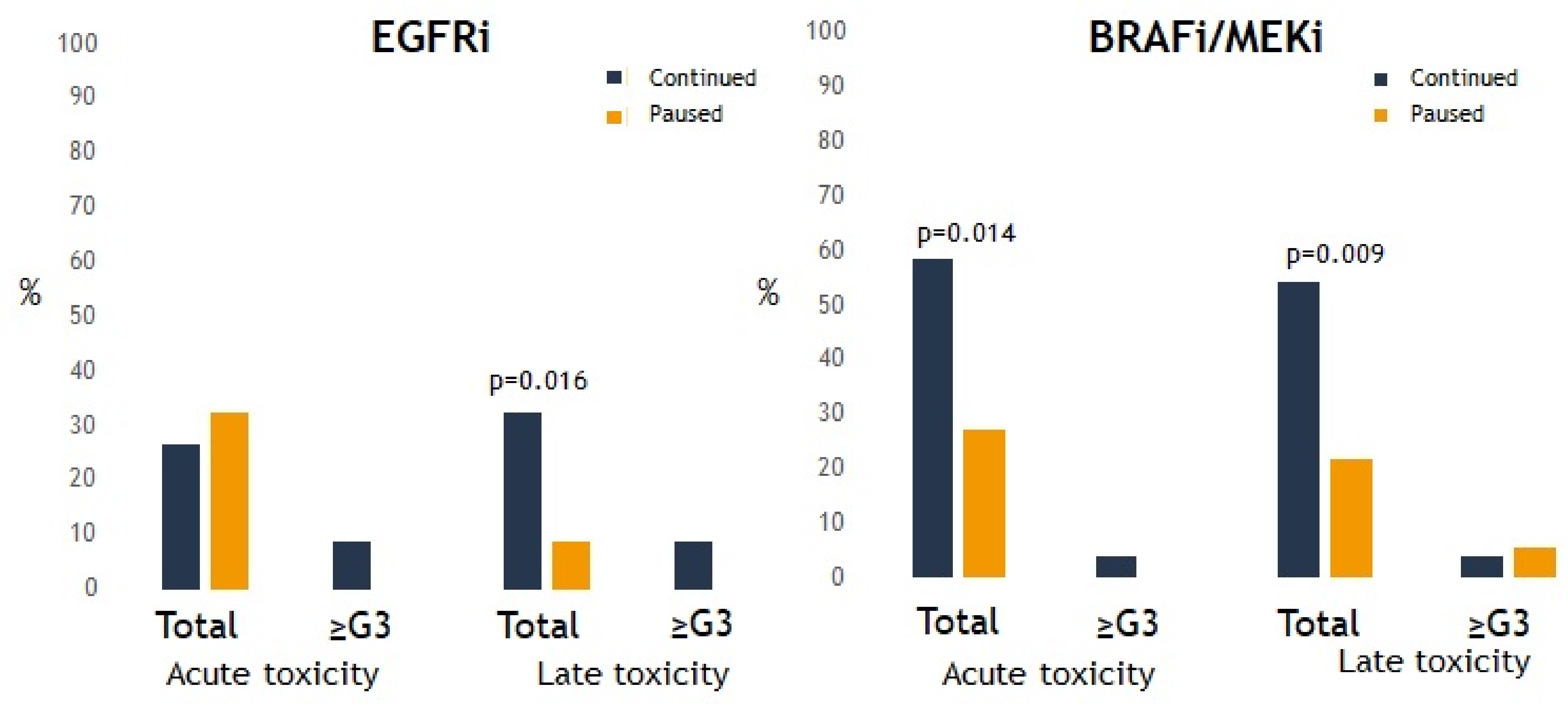
3.5. Toxicity
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Eisen, T.; Sternberg, C.N.; Robert, C.; Mulders, P.; Pyle, L.; Zbinden, S.; Izzedine, H.; Escudier, B. Targeted Therapies for Renal Cell Carcinoma: Review of Adverse Event Management Strategies. J. Natl. Cancer Inst. 2012, 104, 93–113. [Google Scholar] [CrossRef] [Green Version]
- Ramalingam, S.S.; Vansteenkiste, J.; Planchard, D.; Cho, B.C.; Gray, J.E.; Ohe, Y.; Zhou, C.; Reungwetwattana, T.; Cheng, Y.; Chewaskulyong, B.; et al. Overall Survival with Osimertinib in Untreated, EGFR-Mutated Advanced NSCLC. N. Engl. J. Med. 2020, 382, 41–50. [Google Scholar] [CrossRef] [PubMed]
- Dummer, R.; Ascierto, P.A.; Gogas, H.J.; Arance, A.; Mandala, M.; Liszkay, G.; Garbe, C.; Schadendorf, D.; Krajsova, I.; Gutzmer, R.; et al. Overall survival in patients with BRAF-mutant melanoma receiving encorafenib plus binimetinib versus vemurafenib or encorafenib (COLUMBUS): A multicentre, open-label, randomised, phase 3 trial. Lancet Oncol. 2018, 19, 1315–1327. [Google Scholar] [CrossRef]
- Le, X.; Puri, S.; Negrao, M.V.; Nilsson, M.B.; Robichaux, J.; Boyle, T.; Hicks, J.K.; Lovinger, K.L.; Roarty, E.; Rinsurongkawong, W.; et al. Landscape of EGFR-Dependent and -Independent Resistance Mechanisms to Osimertinib and Continuation Therapy Beyond Progression in EGFR-Mutant NSCLC. Clin. Cancer Res. 2018, 24, 6195–6203. [Google Scholar] [CrossRef] [Green Version]
- Schoenfeld, A.J.; Chan, J.M.; Kubota, D.; Sato, H.; Rizvi, H.; Daneshbod, Y.; Chang, J.C.; Paik, P.K.; Offin, M.; Arcila, M.E.; et al. Tumor Analyses Reveal Squamous Transformation and Off-Target Alterations As Early Resistance Mechanisms to First-line Osimertinib in EGFR-Mutant Lung Cancer. Clin. Cancer Res. 2020, 26, 2654–2663. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al-Halabi, H.; Sayegh, K.; Digamurthy, S.R.; Niemierko, A.; Piotrowska, Z.; Willers, H.; Sequist, L.V. Pattern of Failure Analysis in Metastatic EGFR-Mutant Lung Cancer Treated with Tyrosine Kinase Inhibitors to Identify Candidates for Consolidation Stereotactic Body Radiation Therapy. J. Thorac. Oncol. 2015, 10, 1601–1607. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guo, T.; Ni, J.; Yang, X.; Li, Y.; Li, Y.; Zou, L.; Wang, S.; Liu, Q.; Chu, L.; Chu, X.; et al. Pattern of Recurrence Analysis in Metastatic EGFR-Mutant NSCLC Treated with Osimertinib: Implications for Consolidative Stereotactic Body Radiation Therapy. Int. J. Radiat. Oncol. Biol. Phys. 2020, 107, 62–71. [Google Scholar] [CrossRef]
- Zeng, Y.; Ni, J.; Yu, F.; Zhou, Y.; Zhao, Y.; Li, S.; Guo, T.; Chu, L.; Yang, X.; Chu, X.; et al. The value of local consolidative therapy in Osimertinib-treated non-small cell lung cancer with oligo-residual disease. Radiat. Oncol. 2020, 15, 1–9. [Google Scholar] [CrossRef]
- Weaver, B.D.; Goodman, J.R.; Jensen, R. Concurrent Radiosurgery and Systemic Therapies for Melanoma Brain Metastases: A Systematic Review. Cureus 2019, 11, e6147. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kroeze, S.G.; Fritz, C.; Hoyer, M.; Lo, S.S.; Ricardi, U.; Sahgal, A.; Stahel, R.; Stupp, R.; Guckenberger, M. Toxicity of concurrent stereotactic radiotherapy and targeted therapy or immunotherapy: A systematic review. Cancer Treat. Rev. 2017, 53, 25–37. [Google Scholar] [CrossRef] [Green Version]
- Kroeze, S.G.C.; Fritz, C.; Basler, L.; Gkika, E.; Brunner, T.; Grosu, A.L.; Guckenberger, M. Combination of stereotactic radiotherapy and targeted therapy: Patterns-of-care survey in German-speaking countries. Strahlenther. Onkol. 2019, 195, 199–206. [Google Scholar] [CrossRef] [PubMed]
- Griffioen, A.W.; Mans, L.A.; de Graaf, A.M.A.; Nowak-Sliwinska, P.; de Hoog, C.; de Jong, T.A.M.; Vyth-Dreese, F.A.; van Beijnum, J.R.; Bex, A.; Jonasch, E. Rapid angiogenesis onset after discontinuation of sunitinib treatment of renal cell carcinoma patients. Clin. Cancer Res. 2012, 18, 3961–3971. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Available online: https://www.cancer.gov/about-cancer/treatment/types/targeted-therapies/targeted-therapies-fact-sheet (accessed on 8 August 2021).
- Hawkins, R.; Fife, K.; Hurst, M.; Wang, M.; Naicker, N.; Nolasco, S.; Eisen, T.; Matakidou, A.; Gordon, J. Treatment patterns and health outcomes in metastatic renal cell carcinoma patients treated with targeted systemic therapies in the UK. BMC Cancer 2020, 20, 670. [Google Scholar] [CrossRef]
- Merino Lara, T.; Helou, J.; Poon, I.; Sahgal, A.; Chung, H.T.; Chu, W.; Soliman, H.; Ung, Y.; Verma, S.; Cheema, P.; et al. Multisite stereotactic body radiotherapy for metastatic non-small-cell lung cancer: Delaying the need to start or change systemic therapy? Lung Cancer 2018, 124, 219–226. [Google Scholar] [CrossRef] [PubMed]
- Meyer, E.; Pasquier, D.; Bernadou, G.; Calais, G.; Maroun, P.; Bossi, A.; Theodore, C.; Albiges, L.; Stefan, D.; De Crevoisier, R.; et al. Stereotactic radiation therapy in the strategy of treatment of metastatic renal cell carcinoma: A study of the Getug group. Eur. J. Cancer 2018, 98, 38–47. [Google Scholar] [CrossRef]
- Gan, G.N.; Weickhardt, A.J.; Scheier, B.; Doebele, R.C.; Gaspar, L.E.; Kavanagh, B.D.; Camidge, D.R. Stereotactic Radiation Therapy Can Safely and Durably Control Sites of Extra-Central Nervous System Oligoprogressive Disease in Anaplastic Lymphoma Kinase-Positive Lung Cancer Patients Receiving Crizotinib. Int. J. Radiat. Oncol. Biol. Phys. 2014, 88, 892–898. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schmid, S.; Klingbiel, D.; Aeppli, S.; Britschgi, C.; Gautschi, O.; Pless, M.; Rothschild, S.; Wannesson, L.; Janthur, W.; Foerbs, D.; et al. Patterns of progression on osimertinib in EGFR T790M positive NSCLC: A Swiss cohort study. Lung Cancer 2019, 130, 149–155. [Google Scholar] [CrossRef]
- Weickhardt, A.J.; Scheier, B.; Burke, J.M.; Gan, G.; Lu, X.; Bunn, P.A., Jr.; Aisner, D.L.; Gaspar, L.E.; Kavanagh, B.D.; Doebele, R.C.; et al. Local Ablative Therapy of Oligoprogressive Disease Prolongs Disease Control by Tyrosine Kinase Inhibitors in Oncogene-Addicted Non–Small-Cell Lung Cancer. J. Thorac. Oncol. 2012, 7, 1807–1814. [Google Scholar] [CrossRef] [Green Version]
- Yu, H.A.; Sima, C.S.; Huang, J.; Solomon, S.B.; Rimner, A.; Paik, P.; Pietanza, M.C.; Azzoli, C.G.; Rizvi, N.A.; Krug, L.M.; et al. Local therapy with continued EGFR tyrosine kinase inhibitor therapy as a treatment strategy in EGFR-mutant advanced lung cancers that have developed acquired resistance to EGFR tyrosine kinase inhibitors. J. Thorac. Oncol. 2013, 8, 346–351. [Google Scholar] [CrossRef] [Green Version]
- Anker, C.J.; Grossmann, K.F.; Atkins, M.B.; Suneja, G.; Tarhini, A.A.; Kirkwood, J.M. Avoiding Severe Toxicity from Combined BRAF Inhibitor and Radiation Treatment: Consensus Guidelines from the Eastern Cooperative Oncology Group (ECOG). Int. J. Radiat. Oncol. Biol. Phys. 2016, 95, 632–646. [Google Scholar] [CrossRef] [Green Version]
- Brade, A.M.; Ng, S.; Brierley, J.; Kim, J.; Dinniwell, R.; Ringash, J.; Wong, R.R.; Cho, C.; Knox, J.; Dawson, L. Phase 1 Trial of Sorafenib and Stereotactic Body Radiation Therapy for Hepatocellular Carcinoma. Int. J. Radiat. Oncol. Biol. Phys. 2016, 94, 580–587. [Google Scholar] [CrossRef]
- Staehler, M.; Haseke, N.; Nuhn, P.; Tullmann, C.; Karl, A.; Siebels, M.; Stief, C.G.; Wowra, B.; Muacevic, A. Simultaneous anti-angiogenic therapy and single-fraction radiosurgery in clinically relevant metastases from renal cell carcinoma. BJU Int. 2011, 108, 673–678. [Google Scholar] [CrossRef]
- Kim, H.J.; Kim, W.S.; Kwon, D.H.; Cho, Y.H.; Choi, C.M. Effects of an Epithelial Growth Factor Receptor-Tyrosine Kinase Inhibitor Add-on in Stereotactic Radiosurgery for Brain Metastases Originating from Non-Small-Cell Lung Cancer. J. Korean Neurosurg. Soc. 2015, 58, 205–210. [Google Scholar] [CrossRef] [Green Version]
- Schwer, A.L.; Damek, D.M.; Kavanagh, B.D.; Gaspar, L.E.; Lillehei, K.; Stuhr, K.; Chen, C. A phase I dose-escalation study of fractionated stereotactic radiosurgery in combination with gefitinib in patients with recurrent malignant gliomas. Int. J. Radiat. Oncol. Biol. Phys. 2008, 70, 993–1001. [Google Scholar] [CrossRef] [PubMed]
- Iyengar, P.; Kavanagh, B.D.; Wardak, Z.; Smith, I.; Ahn, C.; Gerber, D.E.; Dowell, J.; Hughes, R.; Abdulrahman, R.; Camidge, D.R.; et al. Phase II trial of stereotactic body radiation therapy combined with erlotinib for patients with limited but progressive metastatic non-small-cell lung cancer. J. Clin. Oncol. 2014, 32, 3824–3830. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Zhu, X.X.; Wu, X.H.; Li, B.; Shen, T.Z.; Kong, Q.T.; Li, J.; Liu, Z.; Jiang, W.; Wang, Y.; et al. Gefitinib combined with stereotactic radiosurgery in previously treated patients with advanced non-small cell lung cancer. Am. J. Clin. Oncol. 2014, 37, 148–153. [Google Scholar] [CrossRef]
- Takeda, M.; Nakagawa, K. Toxicity profile of epidermal growth factor receptor tyrosine kinase inhibitors in patients with epidermal growth factor receptor gene mutation-positive lung cancer. Mol. Clin. Oncol. 2016, 6, 3–6. [Google Scholar] [CrossRef] [Green Version]
- Sakao, S.; Tatsumi, K. Molecular mechanisms of lung-specific toxicity induced by epidermal growth factor receptor tyrosine kinase inhibitors. Oncol. Lett. 2012, 4, 865–867. [Google Scholar] [CrossRef]
- Hecht, M.; Meier, F.; Zimmer, L.; Polat, B.; Loquai, C.; Weishaupt, C.; Forschner, A.; Gutzmer, R.; Utikal, J.; Goldinger, S.M.; et al. Clinical outcome of concomitant vs interrupted BRAF inhibitor therapy during radiotherapy in melanoma patients. Br. J. Cancer 2018, 118, 785–792. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ziegler, J.S.; Kroeze, S.; Hilbers, M.-L.; Imhof, L.; Guckenberger, M.; Levesque, M.P.; Dummer, R.; Cheng, P.; Mangana, J. Toxicity of combined targeted therapy and concurrent radiotherapy in metastatic melanoma patients: A single-center retrospective analysis. Melanoma Res. 2020, 30, 552–561. [Google Scholar] [CrossRef]
- Dummer, R.; Tsao, H.; Robert, C. How cutaneous eruptions help to understand the mode of action of kinase inhibitors. Br. J. Dermatol. 2012, 167, 965–967. [Google Scholar] [CrossRef] [PubMed]
- Fukushi, K.; Narita, T.; Hatakeyama, S.; Yamamoto, H.; Tobisawa, Y.; Yoneyama, T.; Yoneyama, T.; Hashimoto, Y.; Koie, T.; Ohyama, C. Difference in toxicity reporting between patients and clinicians during systemic chemotherapy in patients with urothelial carcinoma. Int. J. Urol. 2017, 24, 361–366. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient Characteristics | Total # of Patients (n = 158) (%) Median (Range) | Tt Continued n = 88 (56%) | Tt Paused n = 70 (44%) | p Value |
|---|---|---|---|---|
| Age (y) | 60 (26–86) | 57 (26–80) | 64 (22–86) | 0.16 |
| Sex | 0.798 | |||
| Female | 58 (37) | 28 (35) | 27 (37) | |
| Male | 100 (63) | 52 (65) | 46 (63) | |
| Primary tumor: | 0.594 | |||
| Melanoma | 46 (29) | 27 (33) | 19 (26) | |
| Non-small cell lung cancer | 69 (44) | 32 (38) | 37 (49) | |
| Renal cell carcinoma | 37 (23) | 20 (25) | 17 (22) | |
| Colorectal cancer | 6 (4) | 3 (4) | 3 (4) | |
| ECOG-PS previous to SRT treatment | 0.094 | |||
| 0–1 | 139 (98) | 72 (88) | 67 (97) | |
| 2–3 | 13 (2) | 11 (12) | 2 (3) | |
| Present metastases | 0.831 | |||
| Oligometastatic (≤5 lesions) | 64 (45) | 33 (44) | 30 (40.5) | |
| Polymetastatic (>5 lesions) | 84 (55) | 42 (56) | 41 (55) | |
| Involved organs | 0.423 | |||
| 1 | 38 (25) | 24 (30) | 14 (18) | |
| >1 (2–6) | 116 (75) | 57 (70) | 73 (82) | |
| Targeted therapy | 0.225 | |||
| EGFRi | 59 (37) | 27 (33) | 32 (43) | |
| mTKI | 29 (18) | 13 (16) | 15 (20) | |
| VEGF(R)i | 7 (4.4) | 6 (7.4) | 1 (1.4) | |
| mTORi | 4 (2.5) | 2 (2.5) | 2 (2.7) | |
| ALKi | 16 (10) | 6 (7.4) | 8 (11) | |
| BRAF(±MEK)i | 43 (27) | 27 (33) | 16 (21.6) | |
| Start of targeted therapy | 0.681 | |||
| Before SRT | 118 (77) | 73 (90) | 45 (61) | |
| time (days) | 195 (5–1490) | 200 (1–1000) | 198 (7–1490) | |
| During/after SRT | 37 (23) | 8 (10) | 29 (39) | |
| time (days) | 7 (0–49) | - | 7 (0–49) | |
| Treatment site, total | 454 | 190 | 264 | 0.241 |
| Cranial | 374 | 160 | 214 | |
| Extracranial: | 80 | 30 | 50 | |
| Lymph nodes | 2 | 1 | 1 | |
| Lung | 27 | 12 | 15 | |
| Abdomen | 13 | 3 | 10 | |
| Bone | 34 | 12 | 22 | |
| Soft tissue/muscle | 4 | 2 | 2 | |
| Prescribed dose (BED10, Gy) | ||||
| Brain SRT | 63 (44–114) | 63 (46.9–102) | 62.1 (44–114) | 0.216 |
| SBRT | 93 (53–180) | 101.2 (54–180) | 91.5 (53–159) | 0.275 |
| Tumor volume (mL) | ||||
| Cranial metastases | 1 (0.03–23.9) | 1.3 (0.04–15.3) | 0.91 (0.03–23.9) | 0.26 |
| Extracranial metastases | 7.5 (0.54–154.5) | 11.6 (0.64–154.5) | 6.4 (0.54–140.7) | 0.437 |
| Correlation of Variables to Toxicity * | Acute Severe (≥G3) Toxicity | Late Severe (≥G3) Toxicity | ||||
|---|---|---|---|---|---|---|
| No | Yes | p-Value | No | Yes | p-Value | |
| Histology | 0.133 | 0.829 | ||||
| Melanoma | 62 | 1 | 60 | 3 | ||
| Non-small cell lung cancer | 88 | 1 | 86 | 3 | ||
| Renal cell carcinoma | 47 | 2 | 48 | 1 | ||
| Colorectal cancer | 6 | 1 | 7 | 0 | ||
| ECOG-PS | 0.408 | 0.387 | ||||
| 0–1 | 185 | 4 | 182 | 7 | ||
| 2–3 | 19 | 1 | 20 | 0 | ||
| Number of organs with metastatic disease at time of SRT | ||||||
| 0–3 | 143 | 5 | 0.16 | 144 | 4 | 0.366 |
| >3 | 57 | 0 | 54 | 3 | ||
| Targeted therapy | 0.074 | 0.107 | ||||
| EGFRi | 66 | 2 | 65 | 3 | ||
| mTKI | 32 | 1 | 33 | 0 | ||
| VEGF(R)i | 14 | 0 | 14 | 0 | ||
| mTORi | 3 | 1 | 3 | 1 | ||
| ALKi | 28 | 0 | 28 | 0 | ||
| BRAF(±MEK)i | 60 | 1 | 58 | 3 | ||
| Start of targeted therapy | 0.905 | 0.646 | ||||
| Before SRT | 158 | 4 | 157 | 5 | ||
| During/after SRT | 46 | 1 | 45 | 2 | ||
| Targeted therapy paused during SRT | 0.841 | 0.188 | ||||
| Yes | 89 | 1 (2) | 90 | 0 (0) | ||
| No | 114 | 4 (3) | 111 | 7 (5) | ||
| Prescribed dose (BED10, Gy) | ||||||
| Brain SRT | 65.5 (12) | 61.9 (15) | 0.56 | 65.2 (12) | 70.3 (11) | 0.37 |
| SBRT | 98.8 (33) | 91.5 (0) | 0.826 | 98.2 (33) | 110.7 (27) | 0.602 |
| Tumor volume (cc) | ||||||
| Cranial metastases | 3.0 (5) | 0.9 (0.4) | 0.377 | 3.0 (5) | 3.2 (4) | 0.93 |
| Extracranial metastases | 19.5 (32) | 11.1 (0) | 0.794 | 19.0 (32) | 27.6 (24) | 0.706 |
| Nr. of fractions | 0.486 | 0.732 | ||||
| 1 | 130 | 4 | 129 | 5 | ||
| >1 | 70 | 1 | 69 | 2 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kroeze, S.G.C.; Fritz, C.; Schaule, J.; Blanck, O.; Kahl, K.H.; Kaul, D.; Siva, S.; Gerum, S.; Claes, A.; Sundahl, N.; et al. Continued versus Interrupted Targeted Therapy during Metastasis-Directed Stereotactic Radiotherapy: A Retrospective Multi-Center Safety and Efficacy Analysis. Cancers 2021, 13, 4780. https://doi.org/10.3390/cancers13194780
Kroeze SGC, Fritz C, Schaule J, Blanck O, Kahl KH, Kaul D, Siva S, Gerum S, Claes A, Sundahl N, et al. Continued versus Interrupted Targeted Therapy during Metastasis-Directed Stereotactic Radiotherapy: A Retrospective Multi-Center Safety and Efficacy Analysis. Cancers. 2021; 13(19):4780. https://doi.org/10.3390/cancers13194780
Chicago/Turabian StyleKroeze, Stephanie G. C., Corinna Fritz, Jana Schaule, Oliver Blanck, Klaus Henning Kahl, David Kaul, Shankar Siva, Sabine Gerum, An Claes, Nora Sundahl, and et al. 2021. "Continued versus Interrupted Targeted Therapy during Metastasis-Directed Stereotactic Radiotherapy: A Retrospective Multi-Center Safety and Efficacy Analysis" Cancers 13, no. 19: 4780. https://doi.org/10.3390/cancers13194780