
Comparison of Intraductal RFA Plus Stent versus Stent-Only Treatment for Unresectable Perihilar Cholangiocarcinoma—A Systematic Review and Meta-Analysis

 , and
, and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Selection Criteria and Search Strategy
2.2. Outcomes
2.3. Quality Assessment
2.4. Statistical Analysis
3. Results
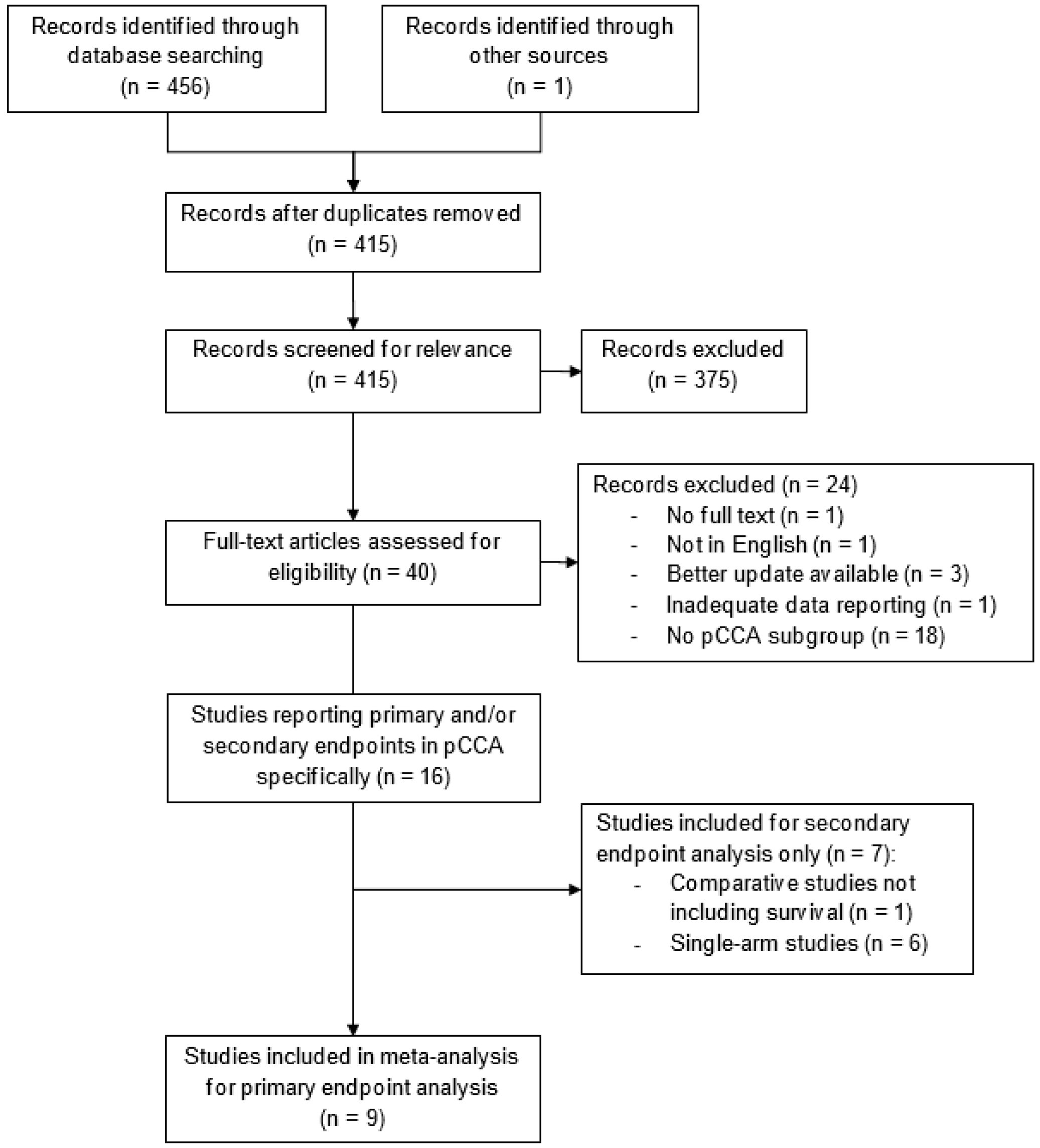
3.1. Study Selection
3.2. Baseline Characteristics
3.3. Quality Assessment
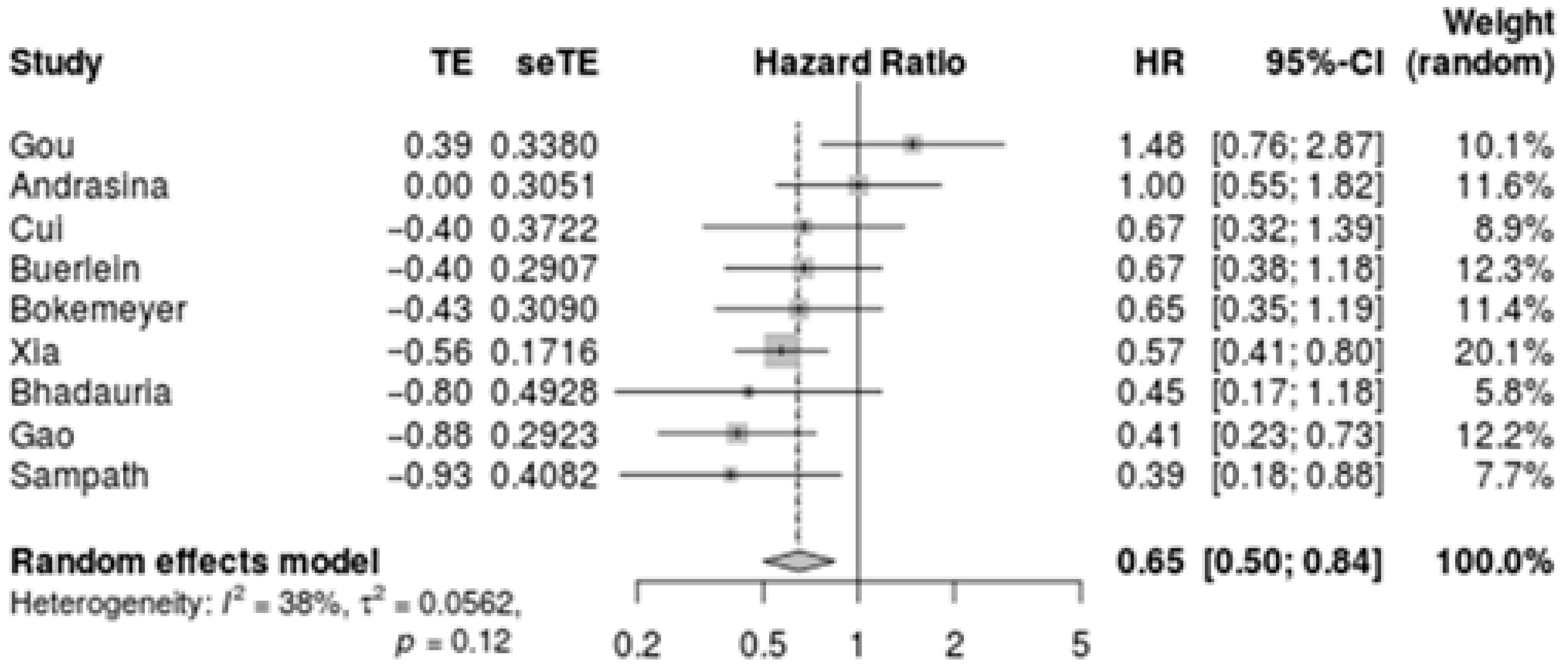
3.4. Primary Outcome—Difference in Overall Survival
3.5. Secondary Outcomes
3.5.1. Median Survival
3.5.2. Stent Patency
3.5.3. Complications
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Blechacz, B. Cholangiocarcinoma: Current knowledge and new developments. Gut Liver 2017, 11, 13–26. [Google Scholar] [CrossRef] [PubMed]
- Banales, J.M.; Cardinale, V.; Carpino, G.; Marzioni, M.; Andersen, J.B.; Invernizzi, P.; Lind, G.E.; Folseraas, T.; Forbes, S.J.; Fouassier, L.; et al. Expert consensus document: Cholangiocarcinoma: Current knowledge and future perspectives consensus statement from the european network for the study of cholangiocarcinoma (ens-cca). Nat. Rev. Gastroenterol. Hepatol. 2016, 13, 261–280. [Google Scholar] [CrossRef]
- Khan, S.A.; Tavolari, S.; Brandi, G. Cholangiocarcinoma: Epidemiology and risk factors. Liver Int. 2019, 39 (Suppl. S1), 19–31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zografos, G.N.; Farfaras, A.; Zagouri, F.; Chrysikos, D.; Karaliotas, K. Cholangiocarcinoma: Principles and current trends. Hepatobiliary Pancreat. Dis. Int. 2011, 10, 10–20. [Google Scholar] [CrossRef]
- Esnaola, N.F.; Meyer, J.E.; Karachristos, A.; Maranki, J.L.; Camp, E.R.; Denlinger, C.S. Evaluation and management of intrahepatic and extrahepatic cholangiocarcinoma. Cancer 2016, 122, 1349–1369. [Google Scholar] [CrossRef] [Green Version]
- Chaiteerakij, R.; Harmsen, W.S.; Marrero, C.R.; Aboelsoud, M.M.; Ndzengue, A.; Kaiya, J.; Therneau, T.M.; Sanchez, W.; Gores, G.J.; Roberts, L.R. A new clinically based staging system for perihilar cholangiocarcinoma. Am. J. Gastroenterol. 2014, 109, 1881–1890. [Google Scholar] [CrossRef] [Green Version]
- Kahaleh, M.; Tokar, J.; Conaway, M.R.; Brock, A.; Le, T.; Adams, R.B.; Yeaton, P. Efficacy and complications of covered wallstents in malignant distal biliary obstruction. Gastrointest. Endosc. 2005, 61, 528–533. [Google Scholar] [CrossRef]
- Singhal, D.; van Gulik, T.M.; Gouma, D.J. Palliative management of hilar cholangiocarcinoma. Surg. Oncol. 2005, 14, 59–74. [Google Scholar] [CrossRef]
- Jang, S.; Stevens, T.; Parsi, M.A.; Bhatt, A.; Kichler, A.; Vargo, J.J. Superiority of self-expandable metallic stents over plastic stents in treatment of malignant distal biliary strictures. Clin. Gastroenterol. Hepatol. 2020, 20, e182–e195. [Google Scholar] [CrossRef]
- Sawas, T.; Al Halabi, S.; Parsi, M.A.; Vargo, J.J. Self-expandable metal stents versus plastic stents for malignant biliary obstruction: A meta-analysis. Gastrointest. Endosc. 2015, 82, 256–267. [Google Scholar] [CrossRef]
- Xia, M.X.; Pan, Y.L.; Cai, X.B.; Wu, J.; Gao, D.J.; Ye, X.; Wang, T.T.; Hu, B. Comparison of endoscopic bilateral metal stent drainage with plastic stents in the palliation of unresectable hilar biliary malignant strictures: Large multicenter study. Dig. Endosc. 2021, 33, 179–189. [Google Scholar] [CrossRef] [PubMed]
- Almadi, M.A.; Barkun, A.; Martel, M. Plastic vs. Self-expandable metal stents for palliation in malignant biliary obstruction: A series of meta-analyses. Off. J. Am. Coll. Gastroenterol. ACG 2017, 112, 260–273. [Google Scholar] [CrossRef] [PubMed]
- Dumonceau, J.M.; Tringali, A.; Papanikolaou, I.S.; Blero, D.; Mangiavillano, B.; Schmidt, A.; Vanbiervliet, G.; Costamagna, G.; Devière, J.; García-Cano, J.; et al. Endoscopic biliary stenting: Indications, choice of stents, and results: European society of gastrointestinal endoscopy (esge) clinical guideline—Updated october 2017. Endoscopy 2018, 50, 910–930. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sofi, A.A.; Khan, M.A.; Das, A.; Sachdev, M.; Khuder, S.; Nawras, A.; Lee, W. Radiofrequency ablation combined with biliary stent placement versus stent placement alone for malignant biliary strictures: A systematic review and meta-analysis. Gastrointest. Endosc. 2018, 87, 944–951. [Google Scholar] [CrossRef] [PubMed]
- Steel, A.W.; Postgate, A.J.; Khorsandi, S.; Nicholls, J.; Jiao, L.; Vlavianos, P.; Habib, N.; Westaby, D. Endoscopically applied radiofrequency ablation appears to be safe in the treatment of malignant biliary obstruction. Gastrointest. Endosc. 2011, 73, 149–153. [Google Scholar] [CrossRef] [PubMed]
- Di Martino, M.; Rompianesi, G.; Mora-Guzman, I.; Martin-Perez, E.; Montalti, R.; Troisi, R.I. Systematic review and meta-analysis of local ablative therapies for resectable colorectal liver metastases. Eur. J. Surg. Oncol. 2020, 46, 772–781. [Google Scholar] [CrossRef] [PubMed]
- Li, J.K.; Liu, X.H.; Cui, H.; Xie, X.H. Radiofrequency ablation versus hepatic resection for small hepatocellular carcinoma: Systematic review of randomized controlled trials with meta-analysis and trial sequential analysis. Radiology 2018, 287, 461–472. [Google Scholar] [CrossRef]
- Han, K.; Ko, H.K.; Kim, K.W.; Won, H.J.; Shin, Y.M.; Kim, P.N. Radiofrequency ablation in the treatment of unresectable intrahepatic cholangiocarcinoma: Systematic review and meta-analysis. J. Vasc. Interv. Radiol. 2015, 26, 943–948. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; The Prisma Group. Preferred reporting items for systematic reviews and meta-analyses: The prisma statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Wells, G.A.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 1 December 2021).
- Jadad, A.R.; Moore, R.A.; Carroll, D.; Jenkinson, C.; Reynolds, D.J.; Gavaghan, D.J.; McQuay, H.J. Assessing the quality of reports of randomized clinical trials: Is blinding necessary? Control. Clin. Trials 1996, 17, 1–12. [Google Scholar] [CrossRef]
- Munn, Z.; Barker, T.H.; Moola, S.; Tufanaru, C.; Stern, C.; McArthur, A.; Stephenson, M.; Aromataris, E. Methodological quality of case series studies: An introduction to the JBI critical appraisal tool. JBI Evid. Synth. 2020, 18, 2127–2133. [Google Scholar] [CrossRef] [PubMed]
- Andrasina, T.; Rohan, T.; Panek, J.; Kovalcikova, P.; Kunovsky, L.; Ostrizkova, L.; Valek, V. The combination of endoluminal radiofrequency ablation and metal stent implantation for the treatment of malignant biliary stenosis—Randomized study. Eur. J. Radiol. 2021, 142, 109830. [Google Scholar] [CrossRef] [PubMed]
- Bhadauria, A.S.; Mohindra, S.; Pandey, G.; Saraswat, V. Early experience with endobiliary radiofrequency ablation (endo-rfa) in patients with unresectable malignant hilar biliary obstruction. Indian J. Gastroenterol. 2020, 34, 390. [Google Scholar] [CrossRef]
- Bokemeyer, A.; Matern, P.; Bettenworth, D.; Cordes, F.; Nowacki, T.M.; Heinzow, H.; Kabar, I.; Schmidt, H.; Ullerich, H.; Lenze, F. Endoscopic radiofrequency ablation prolongs survival of patients with unresectable hilar cholangiocellular carcinoma—A case-control study. Sci. Rep. 2019, 9, 13685. [Google Scholar] [CrossRef]
- Buerlein, R.; Strand, D.S.; Patrie, J.T.; Sauer, B.G.; Shami, V.M.; Scheiman, J.M.; Zaydfudim, V.M.; Bauer, T.W.; Adams, R.B.; Wang, A.Y. 544 ercp-directed biliary ablation prolongs survival in patients with unresectable perihilar cholangiocarcinoma compared to stenting alone. Gastrointest. Endosc. 2019, 89, AB91–AB92. [Google Scholar] [CrossRef]
- Cui, W.; Wang, Y.; Fan, W.; Lu, M.; Zhang, Y.; Yao, W.; Li, J. Comparison of intraluminal radiofrequency ablation and stents vs. Stents alone in the management of malignant biliary obstruction. Int. J. Hyperth. 2017, 33, 853–861. [Google Scholar] [CrossRef] [PubMed]
- Gao, D.J.; Yang, J.F.; Ma, S.R.; Wu, J.; Wang, T.T.; Jin, H.B.; Xia, M.X.; Zhang, Y.C.; Shen, H.Z.; Ye, X.; et al. Endoscopic radiofrequency ablation plus plastic stent placement versus stent placement alone for unresectable extrahepatic biliary cancer: A multicenter randomized controlled trial. Gastrointest. Endosc. 2021, 94, 91–100. [Google Scholar] [CrossRef]
- Gou, Q.; Wu, L.; Cui, W.; Mo, Z.; Zeng, D.; Gan, L.; He, J.; Mai, Q.; Shi, F.; Chen, M.; et al. Stent placement combined with intraluminal radiofrequency ablation and hepatic arterial infusion chemotherapy for advanced biliary tract cancers with biliary obstruction: A multicentre, retrospective, controlled study. Eur. Radiol. 2021, 31, 5851–5862. [Google Scholar] [CrossRef]
- Sampath, K.; Hyder, S.M.; Gardner, T.; Gordon, S.R. The effect of endoscopic radiofrequency ablation on survival in patients with unresectable peri-hilar cholangiocarcinoma. Gastrointest. Endosc. 2016, 83, AB595. [Google Scholar] [CrossRef]
- Xia, M.X.; Wang, S.P.; Yuan, J.G.; Gao, D.J.; Ye, X.; Wang, T.T.; Wu, J.; Zhou, D.X.; Hu, B. Effect of endoscopic radiofrequency ablation on the survival of patients with inoperable malignant biliary strictures: A large cohort study. J. Hepatobiliary Pancreat. Sci. 2021, 1–10. [Google Scholar] [CrossRef]
- Cui, W.; Li, J. Iddf2019-abs-0077 percutaneous endobiliary radiofrequency ablation and self-expandable metal stent placement versus stent placement alone for malignant biliary obstruction. Gut 2019, 68, A129. [Google Scholar] [CrossRef]
- Laquiere, A.; Boustiere, C.; Leblanc, S.; Penaranda, G.; Desilets, E.; Prat, F. Safety and feasibility of endoscopic biliary radiofrequency ablation treatment of extrahepatic cholangiocarcinoma. Surg. Endosc. 2016, 30, 1242–1248. [Google Scholar] [CrossRef] [PubMed]
- Tal, A.O.; Vermehren, J.; Friedrich-Rust, M.; Bojunga, J.; Sarrazin, C.; Zeuzem, S.; Trojan, J.; Albert, J.G. Intraductal endoscopic radiofrequency ablation for the treatment of hilar non-resectable malignant bile duct obstruction. World J. Gastrointest. Endosc. 2014, 6, 13–19. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Cui, W.; Fan, W.; Zhang, Y.; Yao, W.; Huang, K.; Li, J. Percutaneous intraductal radiofrequency ablation in the management of unresectable bismuth types iii and iv hilar cholangiocarcinoma. Oncotarget 2016, 7, 53911–53920. [Google Scholar] [CrossRef] [Green Version]
- Han, S.Y.; Kim, D.U.; Kang, D.H.; Baek, D.H.; Lee, T.H.; Cho, J.H. Usefulness of intraductal rfa in patients with malignant biliary obstruction. Medicine 2020, 99, e21724. [Google Scholar] [CrossRef]
- Kang, H.; Han, S.Y.; Cho, J.H.; Kim, E.J.; Kim, D.U.; Yang, J.K.; Jeon, S.; Park, G.; Lee, T.H. Efficacy and safety of temperature-controlled intraductal radiofrequency ablation in advanced malignant hilar biliary obstruction: A pilot multicenter randomized comparative trial. J. Hepatobiliary Pancreat. Sci. 2021, 00, 1–10. [Google Scholar] [CrossRef]
- Lee, Y.N.; Moon, J.H.; Park, J.K.; Jo, S.J.; Lee, T.H. Efficacy of endobiliary radiofrequency ablation plus stenting versus stenting alone in patients with inoperable hilar cholangiocarcinoma. Gut Liver 2019, 13, 19. [Google Scholar]
- Laleman, W.; van der Merwe, S.; Verbeke, L.; Vanbeckevoort, D.; Aerts, R.; Prenen, H.; van Cutsem, E.; Verslype, C. A new intraductal radiofrequency ablation device for inoperable biliopancreatic tumors complicated by obstructive jaundice: The ignite-1 study. Endoscopy 2017, 49, 977–982. [Google Scholar] [CrossRef]
- Cha, B.H.; Jang, M.J.; Lee, S.H. Survival benefit of intraductal radiofrequency ablation for malignant biliary obstruction: A systematic review with meta-analysis. Clin. Endosc. 2021, 54, 100–106. [Google Scholar] [CrossRef]
- van Keulen, A.M.; Franssen, S.; van der Geest, L.G.; de Boer, M.T.; Coenraad, M.; van Driel, L.M.; Erdmann, J.I.; Haj Mohammad, N.; Heij, L.; Klümpen, H.J.; et al. Nationwide treatment and outcomes of perihilar cholangiocarcinoma. Liver Int. 2021, 41, 1945–1953. [Google Scholar] [CrossRef]
- Gaspersz, M.P.; Buettner, S.; van Vugt, J.L.A.; Roos, E.; Coelen, R.J.S.; Vugts, J.; Belt, E.J.; de Jonge, J.; Polak, W.G.; Willemssen, F.E.; et al. Conditional survival in patients with unresectable perihilar cholangiocarcinoma. HPB 2017, 19, 966–971. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shin, D.W.; Kim, M.J.; Lee, J.C.; Kim, J.; Woo, S.M.; Lee, W.J.; Lee, K.H.; Hwang, J.H. Gemcitabine plus cisplatin chemotherapy prolongs the survival in advanced hilar cholangiocarcinoma: A large multicenter study. Am. J. Clin. Oncol. 2020, 43, 422–427. [Google Scholar] [CrossRef] [PubMed]
- Valle, J.W.; Borbath, I.; Khan, S.A.; Huguet, F.; Gruenberger, T.; Arnold, D.; ESMO Guidelines Committee. Biliary cancer: Esmo clinical practice guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2016, 27, v28–v37. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Chen, L.; Zhu, G.Y.; Yao, X.; Dong, R.; Guo, J.H. Interventional treatment for cholangiocarcinoma. Front. Oncol 2021, 11, 671327. [Google Scholar] [CrossRef] [PubMed]
- Den Brok, M.H.; Sutmuller, R.P.; van der Voort, R.; Bennink, E.J.; Figdor, C.G.; Ruers, T.J.; Adema, G.J. In situ tumor ablation creates an antigen source for the generation of antitumor immunity. Cancer Res. 2004, 64, 4024–4029. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giardino, A.; Innamorati, G.; Ugel, S.; Perbellini, O.; Girelli, R.; Frigerio, I.; Regi, P.; Scopelliti, F.; Butturini, G.; Paiella, S.; et al. Immunomodulation after radiofrequency ablation of locally advanced pancreatic cancer by monitoring the immune response in 10 patients. Pancreatology 2017, 17, 962–966. [Google Scholar] [CrossRef]
- Hansler, J.; Wissniowski, T.-T.; Schuppan, D.; Witte, A.; Bernatik, T.; Hahn, E.-G.; Strobel, D. Activation and dramatically increased cytolytic activity of tumor specific t lymphocytes after radio-frequency ablation in patients with hepatocellular carcinoma and colorectal liver metastases. World J. Gastroenterol. 2006, 12, 3716–3721. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Study | Country | Period | Study Design | CCA Type | Intervention | RFA Setting | Stent Type | N (RFA vs. Stent) | Median Survival in Months | Palliative Treatment | |||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| R/P | Design | RFA | Stent | pCTx | Other | ||||||||
| Andrasina [23] | Czech Republic | 2010–2019 | P | RCT | Bismuth II–IV | PTC | 10 W for 90–120 s, Habib | ucSEMS | 21 vs. 22 | 12.3 | 12.3 | 14 vs. 13 | BTx: 18 vs. 16 |
| Bhadauria [24] * | India | NR | P | Cohort | Bismuth I–IV | NR | 8–10 W for 120 s, Habib | Plastic | 10 vs. 7 | 15.8 | 7.1 | NR | NR |
| Bokemeyer [25] | Germany | 2006–2011 controls, 2012–2017 cases | R | Case control | Bismuth III–IV | ERCP | 8–10 W for 90 s, Habib | Plastic | 17 vs. 20 | 11.3 | 7.3 | 6 vs. 7 | NR |
| SEMS | 3 vs. 2 | ||||||||||||
| Buerlein [26] * | USA | 2011–2018 | R | Cohort | Bismuth I–IV | ERCP | NR | NR | 20 vs. 29 | 10.0 | 6.7 | NR | PDT: 2 vs. 0 |
| Cui [27,32] | China | 2013–2015 | R | Cohort | Bismuth I–IV | PTC | 10 W for 90 s, Habib | ucSEMS | 46 vs. 28 | 8.0 | 4.7 | NR | NR |
| Gao [28] | China | 2013–2017 | P | RCT | Bismuth I–III | ERCP, repeat after 3 months | 7–10 W for 90 s, Habib | Plastic | 25 vs. 22 | HR: 0.414 | NR | NR | |
| Gou [29] | China | 2013–2018 | R | Cohort | Bismuth I–IV | PTC | 10 W for 120 s, Habib | ucSEMS | 18 vs. 17 | HR: 1.480 | NR | HAIC: 18 vs 0 | |
| Sampath [30] * | USA | 2010–2015 | R | Cohort | Bismuth I–IV | ERCP | NR | Plastic | 8 vs. 10 | 11.8 | 4.7 | 8 vs. 11 (+/−RTx) | NR |
| SEMS | 2 vs. 5 | ||||||||||||
| Xia [31] | China | 2012–2019 | R | Matched Cohort | Bismuth I–IV | ERCP | 10–12 W for 60–120 s, Habib | Both | 47 vs. 132 | 10.5 | 6.0 | NR | NR |
| Study | Intervention | Stent Type | Group | N | Stent Patency | p-Value or HR (95% CI) |
|---|---|---|---|---|---|---|
| Andrasina [23] | PTC | ucSEMS | RFA + stent | 20 * | Median 9.6 months [95% CI 5.2–11.2] | 0.029 |
| Stent-only | 22 † | Median 4.5 months [95% CI 0.8–10.3] | ||||
| Cui [27,32] | PTC | ucSEMS | RFA + stent | 25 | Median 7.6 months [95% CI 6.8–9.2] | 0.009 |
| Stent-only | 14 | Median 4.3 months [95% CI 1.7–8.5] | ||||
| Gou [29] | PTC | ucSEMS | RFA + stent | 18 | NR | 1.173 [95% CI 0.685–2.011] |
| Stent-only | 17 | |||||
| Kang [37] | ERCP | Plastic exchanged for ucSEMS | RFA + stent | 13 | Median 5.9 months [range 2.0–9.8] | NR |
| Stent-only | 13 | Median 4.0 months [range 3.4–4.6] | ||||
| Lee [38] | NR | NR | RFA + stent | 21 | Median 8.0 months | 0.01 |
| Stent-only | 21 | Median 4.0 months | ||||
| Laleman [39] | ERCP | Both | RFA + stent | 9 | Median 4.6 months [range: 1.7–11.2] | NA |
| Study | No. per Group | Overall AE Rate | Cholangitis | Cholecystitis | Pancreatitis | Liver Abscess | Bleeding | Abdominal Pain | Perforation | p-Value | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Buerlein [26] | RFA | 20 | NR | 40% | NR | NR | 10% | NR | 10% | NR | >0.05 |
| Stent-only | 29 | NR | 41% | NR | NR | 21% | NR | 6.9% | NR | ||
| Gao [28] | RFA | 25 | NR | NR | 28% | NR | NR | NR | NR | NR | NR |
| Stent-only | 22 | NR | NR | 0% | NR | NR | NR | NR | NR | ||
| Lee [38] | RFA | 21 | NR | NR | NR | NR | NR | NR | NR | NR | >0.05 |
| Stent-only | 21 | ||||||||||
| Sampath [30] | RFA | 10 | NR | 30% | NR | NR | NR | NR | NR | 0% (bile leak) | NR |
| Stent-only | 15 | NR | 0% | NR | NR | NR | NR | NR | 7% (bile leak) | ||
| Han [36] | RFA | 21 | 14.3% | 0% | 10% | 0% | NR | 0% | NR | 0% | NA |
| Laquière [33] | RFA | 12 | NR | 8% | NR | NR | NR | 0% | NR | NR | NA |
| Wang [35] | RFA | 9 | NR | 44% | NR | 0% | NR | 0% | 33% | 0% | NA |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
de Jong, D.M.; Fritzsche, J.A.; Audhoe, A.S.; Yi, S.S.L.; Bruno, M.J.; Voermans, R.P.; van Driel, L.M.J.W. Comparison of Intraductal RFA Plus Stent versus Stent-Only Treatment for Unresectable Perihilar Cholangiocarcinoma—A Systematic Review and Meta-Analysis. Cancers 2022, 14, 2079. https://doi.org/10.3390/cancers14092079
de Jong DM, Fritzsche JA, Audhoe AS, Yi SSL, Bruno MJ, Voermans RP, van Driel LMJW. Comparison of Intraductal RFA Plus Stent versus Stent-Only Treatment for Unresectable Perihilar Cholangiocarcinoma—A Systematic Review and Meta-Analysis. Cancers. 2022; 14(9):2079. https://doi.org/10.3390/cancers14092079
Chicago/Turabian Stylede Jong, David M., Jeska A. Fritzsche, Amber S. Audhoe, Suzanne S. L. Yi, Marco J. Bruno, Rogier P. Voermans, and Lydi M. J. W. van Driel. 2022. "Comparison of Intraductal RFA Plus Stent versus Stent-Only Treatment for Unresectable Perihilar Cholangiocarcinoma—A Systematic Review and Meta-Analysis" Cancers 14, no. 9: 2079. https://doi.org/10.3390/cancers14092079