
Prevalence of Cancer Predisposition Germline Variants in Male Breast Cancer Patients: Results of the German Consortium for Hereditary Breast and Ovarian Cancer

 , , , , , add
Show full author list
, , , , , add
Show full author list
Abstract
:Simple Summary
Abstract
1. Introduction
2. Material and Methods
2.1. Study Sample
2.2. Gene Selection and Next-Generation-Sequencing (NGS) Analysis
2.3. Variant Annotation and Classification
2.4. Control Sample and Statistical Analysis
3. Results
3.1. Prevalence of BRCA1/2 Pathogenic Variants and Cancer Characteristics in the Overall Study Sample
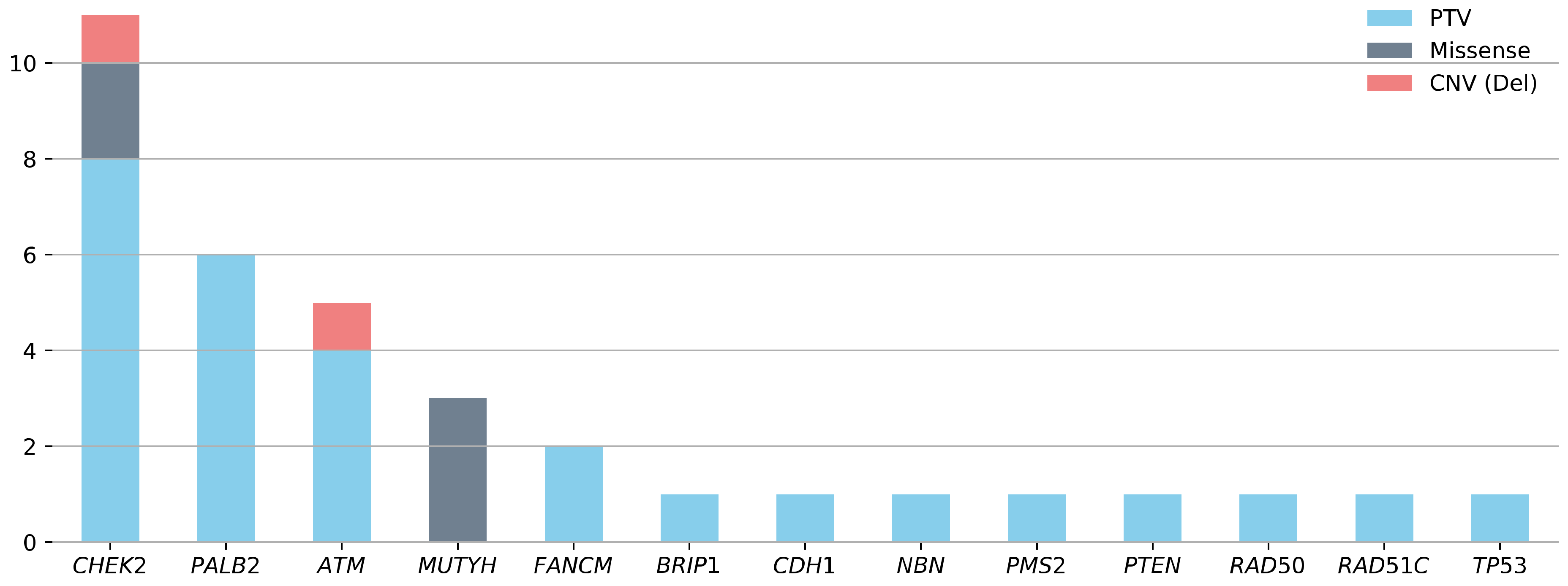
3.2. Prevalence of Pathogenic Variants in BRCA1/2-Negative Patients with mBC
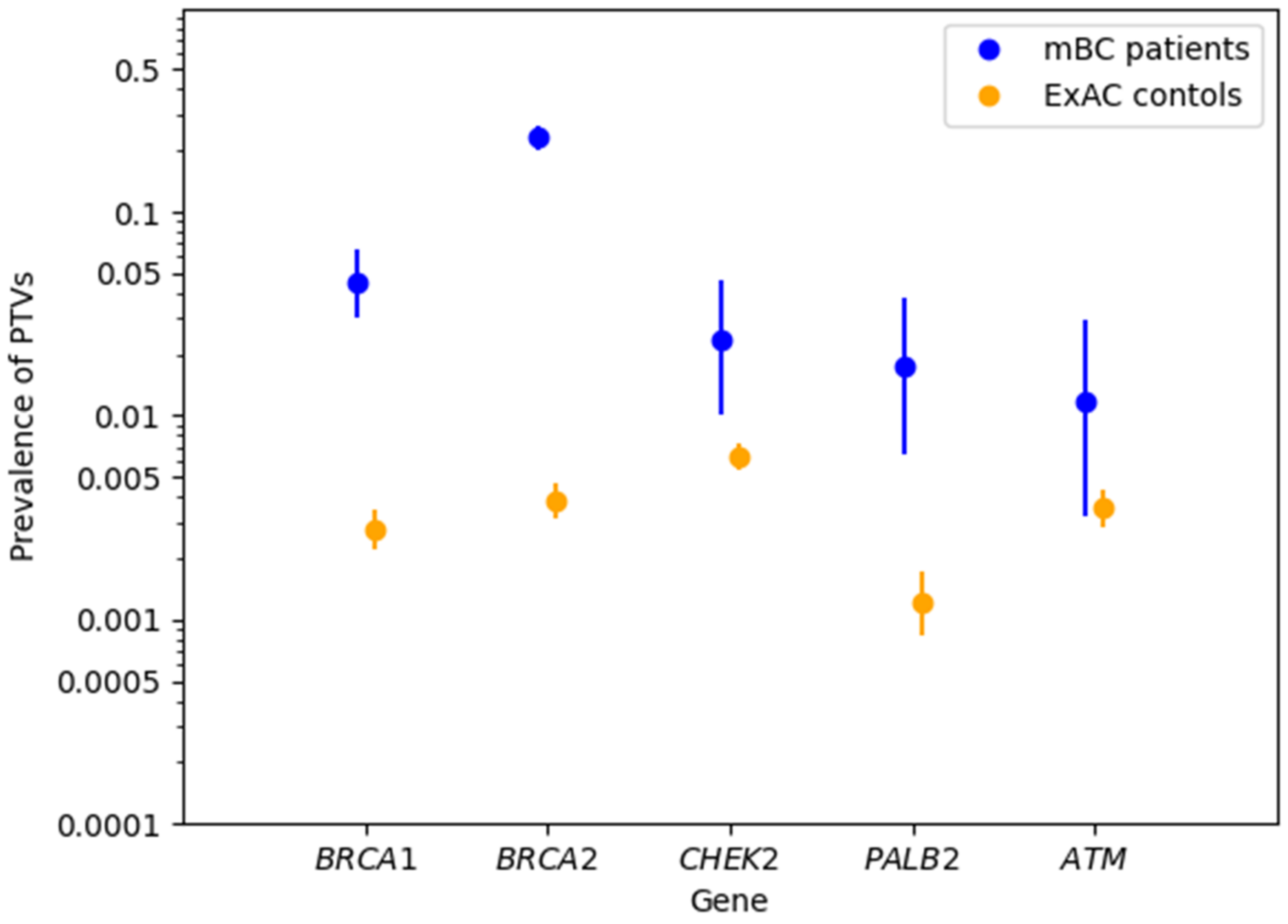
3.3. Associations between mBC and Protein-Truncating Variants in BRCA1/2 and Non-BRCA1/2 Cancer Predisposition Genes
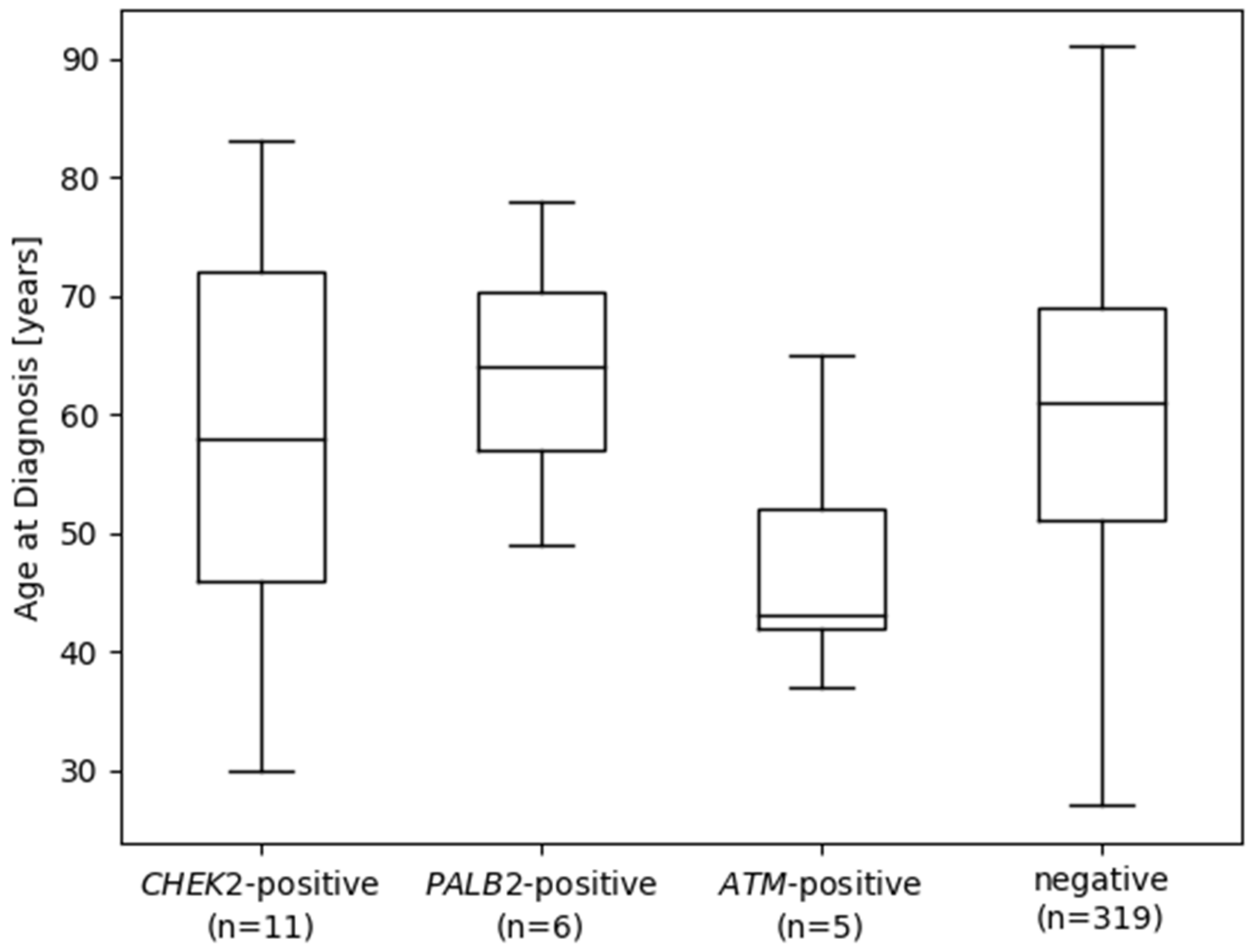
3.4. Pathogenic Variants in Cancer Predisposition Genes according to Cancer Family History, Age at Diagnosis, and Tumor Characteristics
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| AAD | age at first diagnosis |
| ACMG | American College of Medical Genetics |
| BC | breast cancer |
| CCG | Cologne Center for Genomics |
| CI | confidence interval |
| CNV | copy number variation |
| ER | estrogen receptor |
| ExAC | Exome Aggregation Consortium |
| FH | family history |
| GC-HBOC | German Consortium for Hereditary Breast and Ovarian Cancer |
| HER2 | human epidermal growth factor receptor 2 |
| IARC | International Agency for Research on Cancer |
| mBC | male breast cancer |
| MLPA | multiplex ligation-dependent probe amplification |
| NCCN | National Comprehensive Cancer Network |
| NFE | non-Finnish European |
| NGS | next-generation sequencing |
| PR | progesterone receptor |
| PTV | protein-truncating variant |
| PV | pathogenic variant |
| OC | ovarian cancer |
| OR | odds ratio |
| TCGA | The Cancer Genome Atlas |
| VUS | variant of uncertain significance |
References
- Konduri, S.; Singh, M.; Bobustuc, G.; Rovin, R.; Kassam, A. Epidemiology of Male Breast Cancer. Breast 2020, 54, 8–14. [Google Scholar] [CrossRef] [PubMed]
- Ly, D.; Forman, D.; Ferlay, J.; Brinton, L.A.; Cook, M.B. An International Comparison of Male and Female Breast Cancer Incidence Rates. Int. J. Cancer 2013, 132, 1918–1926. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Robert Koch-Institut. Krebs in Deutschland 2015/2016; Robert Koch-Institut, und Gesellschaft der Epidemiologischen Krebsregister in Deutschland, E.V.: Berlin, Germany, 2019. [Google Scholar] [CrossRef]
- Giordano, S.H. Breast Cancer in Men. N. Engl. J. Med. 2018, 378, 2311–2320. [Google Scholar] [CrossRef] [PubMed]
- Leon-Ferre, R.A.; Giridhar, K.V.; Hieken, T.J.; Mutter, R.W.; Couch, F.J.; Jimenez, R.E.; Hawse, J.R.; Boughey, J.C.; Ruddy, K.J. A Contemporary Review of Male Breast Cancer: Current Evidence and Unanswered Questions. Cancer Metastasis Rev. 2018, 37, 599–614. [Google Scholar] [CrossRef]
- Campos, F.A.B.; Rouleau, E.; Torrezan, G.T.; Carraro, D.M.; Casali da Rocha, J.C.; Mantovani, H.K.; da Silva, L.R.; Osório, C.A.B.d.T.; Moraes Sanches, S.; Caputo, S.M.; et al. Genetic Landscape of Male Breast Cancer. Cancers 2021, 13, 3535. [Google Scholar] [CrossRef]
- Fentiman, I.S. Male Breast Cancer Is Not Congruent with the Female Disease. Crit. Rev. Oncol./Hematol. 2016, 101, 119–124. [Google Scholar] [CrossRef]
- De Juan, I.; Palanca, S.; Domenech, A.; Feliubadaló, L.; Segura, Á.; Osorio, A.; Chirivella, I.; de la Hoya, M.; Sánchez, A.B.; Infante, M.; et al. BRCA1 and BRCA2 Mutations in Males with Familial Breast and Ovarian Cancer Syndrome. Results of a Spanish Multicenter Study. Fam. Cancer 2015, 14, 505–513. [Google Scholar] [CrossRef]
- Ottini, L. Male Breast Cancer: A Rare Disease That Might Uncover Underlying Pathways of Breast Cancer. Nat. Rev. Cancer 2014, 14, 643–644. [Google Scholar] [CrossRef]
- Li, S.; Silvestri, V.; Leslie, G.; Rebbeck, T.R.; Neuhausen, S.L.; Hopper, J.L.; Nielsen, H.R.; Lee, A.; Yang, X.; McGuffog, L.; et al. Cancer Risks Associated With BRCA1 and BRCA2 Pathogenic Variants. J. Clin. Oncol. 2022, 40, JCO2102112. [Google Scholar] [CrossRef]
- Barnes, D.R.; Silvestri, V.; Leslie, G.; McGuffog, L.; Dennis, J.; Yang, X.; Adlard, J.; Agnarsson, B.A.; Ahmed, M.; Aittomäki, K.; et al. Breast and Prostate Cancer Risks for Male BRCA1 and BRCA2 Pathogenic Variant Carriers Using Polygenic Risk Scores. JNCI J. Natl. Cancer Inst. 2021, 114, djab147. [Google Scholar] [CrossRef]
- kConFab Investigators; Hereditary Breast and Ovarian Cancer Research Group Netherlands (HEBON); EMBRACE; Silvestri, V.; Barrowdale, D.; Mulligan, A.M.; Neuhausen, S.L.; Fox, S.; Karlan, B.Y.; Mitchell, G.; et al. Male Breast Cancer in BRCA1 and BRCA2 Mutation Carriers: Pathology Data from the Consortium of Investigators of Modifiers of BRCA1/2. Breast Cancer Res. 2016, 18, 15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ibrahim, M.; Yadav, S.; Ogunleye, F.; Zakalik, D. Male BRCA Mutation Carriers: Clinical Characteristics and Cancer Spectrum. BMC Cancer 2018, 18, 179. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stratton, M.R.; Ford, D.; Neuhasen, S.; Seal, S.; Wooster, R.; Friedman, L.S.; King, M.-C.; Egilsson, V.; Devilee, P.; McManus, R.; et al. Familial Male Breast Cancer Is Not Linked to the BRCA1 Locus on Chromosome 17q. Nat. Genet. 1994, 7, 103–107. [Google Scholar] [CrossRef] [PubMed]
- Tai, Y.C.; Domchek, S.; Parmigiani, G.; Chen, S. Breast Cancer Risk Among Male BRCA1 and BRCA2 Mutation Carriers. JNCI J. Natl. Cancer Inst. 2007, 99, 1811–1814. [Google Scholar] [CrossRef] [PubMed]
- Hassett, M.J.; Somerfield, M.R.; Baker, E.R.; Cardoso, F.; Kansal, K.J.; Kwait, D.C.; Plichta, J.K.; Ricker, C.; Roshal, A.; Ruddy, K.J.; et al. Management of Male Breast Cancer: ASCO Guideline. J. Clin. Oncol. 2020, 38, JCO.19.03120. [Google Scholar] [CrossRef]
- Arbeitsgemeinschaft der Wissenschaftlichen Medizinischen Fachgesellschaften (AWMF). Interdisziplinäre S3-Leitlinie Für Die Früherkennung, Diagnostik, Therapie Und Nachsorge Des Mammakarzinoms Version 4.3 AWMF-Registernummer: 032-045OL; Version 4.3; Deutsche Krebsgesellschaft: Berlin, Germany, 2020. [Google Scholar]
- Hauke, J.; Horvath, J.; Groß, E.; Gehrig, A.; Honisch, E.; Hackmann, K.; Schmidt, G.; Arnold, N.; Faust, U.; Sutter, C.; et al. Gene Panel Testing of 5589 BRCA1/2 -Negative Index Patients with Breast Cancer in a Routine Diagnostic Setting: Results of the German Consortium for Hereditary Breast and Ovarian Cancer. Cancer Med. 2018, 7, 1349–1358. [Google Scholar] [CrossRef]
- Pritzlaff, M.; Summerour, P.; McFarland, R.; Li, S.; Reineke, P.; Dolinsky, J.S.; Goldgar, D.E.; Shimelis, H.; Couch, F.J.; Chao, E.C.; et al. Male Breast Cancer in a Multi-Gene Panel Testing Cohort: Insights and Unexpected Results. Breast Cancer Res. Treat. 2017, 161, 575–586. [Google Scholar] [CrossRef] [Green Version]
- Rizzolo, P.; Zelli, V.; Silvestri, V.; Valentini, V.; Zanna, I.; Bianchi, S.; Masala, G.; Spinelli, A.M.; Tibiletti, M.G.; Russo, A.; et al. Insight into Genetic Susceptibility to Male Breast Cancer by Multigene Panel Testing: Results from a Multicenter Study in Italy: Multigene Panel Testing in Male Breast Cancer. Int. J. Cancer 2019, 145, 390–400. [Google Scholar] [CrossRef]
- Fostira, F.; Saloustros, E.; Apostolou, P.; Vagena, A.; Kalfakakou, D.; Mauri, D.; Tryfonopoulos, D.; Georgoulias, V.; Yannoukakos, D.; Fountzilas, G.; et al. Germline Deleterious Mutations in Genes Other than BRCA2 Are Infrequent in Male Breast Cancer. Breast Cancer Res. Treat. 2018, 169, 105–113. [Google Scholar] [CrossRef]
- Szwiec, M.; Tomiczek-Szwiec, J.; Kluźniak, W.; Wokołorczyk, D.; Osowiecka, K.; Sibilski, R.; Wachowiak, M.; Gronwald, J.; Gronwald, H.; Lubiński, J.; et al. Genetic Predisposition to Male Breast Cancer in Poland. BMC Cancer 2021, 21, 975. [Google Scholar] [CrossRef]
- Tedaldi, G.; Tebaldi, M.; Zampiga, V.; Cangini, I.; Pirini, F.; Ferracci, E.; Danesi, R.; Arcangeli, V.; Ravegnani, M.; Martinelli, G.; et al. Male Breast Cancer: Results of the Application of Multigene Panel Testing to an Italian Cohort of Patients. Diagnostics 2020, 10, 269. [Google Scholar] [CrossRef] [PubMed]
- Wappenschmidt, B.; Hauke, J.; Faust, U.; Niederacher, D.; Wiesmüller, L.; Schmidt, G.; Groß, E.; Gehrig, A.; Sutter, C.; Ramser, J.; et al. Criteria of the German Consortium for Hereditary Breast and Ovarian Cancer for the Classification of Germline Sequence Variants in Risk Genes for Hereditary Breast and Ovarian Cancer. Geburtshilfe Frauenheilkd. 2020, 80, 410–429. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- ACMG Laboratory Quality Assurance Committee; Richards, S.; Aziz, N.; Bale, S.; Bick, D.; Das, S.; Gastier-Foster, J.; Grody, W.W.; Hegde, M.; Lyon, E.; et al. Standards and Guidelines for the Interpretation of Sequence Variants: A Joint Consensus Recommendation of the American College of Medical Genetics and Genomics and the Association for Molecular Pathology. Genet. Med. 2015, 17, 405–423. [Google Scholar] [CrossRef] [Green Version]
- Plon, S.E.; Eccles, D.M.; Easton, D.; Foulkes, W.D.; Genuardi, M.; Greenblatt, M.S.; Hogervorst, F.B.L.; Hoogerbrugge, N.; Spurdle, A.B.; Tavtigian, S.V.; et al. Sequence Variant Classification and Reporting: Recommendations for Improving the Interpretation of Cancer Susceptibility Genetic Test Results. Hum. Mutat. 2008, 29, 1282–1291. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Plagnol, V.; Curtis, J.; Epstein, M.; Mok, K.Y.; Stebbings, E.; Grigoriadou, S.; Wood, N.W.; Hambleton, S.; Burns, S.O.; Thrasher, A.J.; et al. A Robust Model for Read Count Data in Exome Sequencing Experiments and Implications for Copy Number Variant Calling. Bioinformatics 2012, 28, 2747–2754. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Exome Aggregation Consortium; Lek, M.; Karczewski, K.J.; Minikel, E.V.; Samocha, K.E.; Banks, E.; Fennell, T.; O’Donnell-Luria, A.H.; Ware, J.S.; Hill, A.J.; et al. Analysis of Protein-Coding Genetic Variation in 60,706 Humans. Nature 2016, 536, 285–291. [Google Scholar] [CrossRef] [Green Version]
- Kääriäinen, H.; Muilu, J.; Perola, M.; Kristiansson, K. Genetics in an Isolated Population like Finland: A Different Basis for Genomic Medicine? J. Community Genet. 2017, 8, 319–326. [Google Scholar] [CrossRef] [Green Version]
- Tomasik, B.; Bieńkowski, M.; Jassem, J. PARP Inhibitors beyond BRCA-Mutated Cancers: Precision Medicine at the Crossroads. Precis. Cancer Med. 2021, 4, 19. [Google Scholar] [CrossRef]
- Rebbeck, T.R.; Friebel, T.M.; Friedman, E.; Hamann, U.; Huo, D.; Kwong, A.; Olah, E.; Olopade, O.I.; Solano, A.R.; Teo, S.-H.; et al. Mutational Spectrum in a Worldwide Study of 29,700 Families with BRCA1 or BRCA2 Mutations. Hum. Mutat. 2018, 39, 593–620. [Google Scholar] [CrossRef] [Green Version]
- Cardoso, F.; Bartlett, J.M.S.; Slaets, L.; van Deurzen, C.H.M.; van Leeuwen-Stok, E.; Porter, P.; Linderholm, B.; Hedenfalk, I.; Schröder, C.; Martens, J.; et al. Characterization of Male Breast Cancer: Results of the EORTC 10085/TBCRC/BIG/NABCG International Male Breast Cancer Program. Ann. Oncol. 2018, 29, 405–417. [Google Scholar] [CrossRef]
- Lee, A.; Yang, X.; Tyrer, J.; Gentry-Maharaj, A.; Ryan, A.; Mavaddat, N.; Cunningham, A.P.; Carver, T.; Archer, S.; Leslie, G.; et al. Comprehensive epithelial tubo-ovarian cancer risk prediction model incorporating genetic and epidemiological risk factors. J. Med. Genet. 2022, 59, 632–643. [Google Scholar] [CrossRef] [PubMed]
- Wu, S.; Zhou, J.; Zhang, K.; Chen, H.; Luo, M.; Lu, Y.; Sun, Y.; Chen, Y. Molecular Mechanisms of PALB2 Function and Its Role in Breast Cancer Management. Front. Oncol. 2020, 10, 301. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Silvestri, V.; Zelli, V.; Valentini, V.; Rizzolo, P.; Navazio, A.S.; Coppa, A.; Agata, S.; Oliani, C.; Barana, D.; Castrignanò, T.; et al. Whole-Exome Sequencing and Targeted Gene Sequencing Provide Insights into the Role of PALB2 as a Male Breast Cancer Susceptibility Gene: PALB2 Mutations in Male Breast Cancer. Cancer 2017, 123, 210–218. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ding, Y.C.; Steele, L.; Kuan, C.-J.; Greilac, S.; Neuhausen, S.L. Mutations in BRCA2 and PALB2 in Male Breast Cancer Cases from the United States. Breast Cancer Res. Treat. 2011, 126, 771–778. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aloraifi, F.; McCartan, D.; McDevitt, T.; Green, A.J.; Bracken, A.; Geraghty, J. Protein-Truncating Variants in Moderate-Risk Breast Cancer Susceptibility Genes: A Meta-Analysis of High-Risk Case-Control Screening Studies. Cancer Genet. 2015, 208, 455–463. [Google Scholar] [CrossRef] [PubMed]
- Zheng, G.; Leone, J.P. Male Breast Cancer: An Updated Review of Epidemiology, Clinicopathology, and Treatment. J. Oncol. 2022, 2022, 1734049. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Subgroup | Overall Study Sample (%) | BRCA1/2- Positive | BRCA1- Positive | BRCA2- Positive | BRCA1/2 Negative Patients Further Investigated | Carriers of Pathogenic Variants in 23 Non-BRCA1/2-Genes (%) |
|---|---|---|---|---|---|---|
| patients with mBC | 614 (100) | 170 | 28 | 142 | 340 | 32 (9.4) |
| unilateral BC | 586 (95.4) | 160 | 28 | 132 | 328 | 32 (9.8) |
| bilateral BC | 28 (4.6) | 10 | 0 | 10 | 12 | 0 (0) |
| BC/OC FH * | 460 (75.9) | 154 | 26 | 128 | 235 | 23 (9.8) |
| no BC/OC FH * | 146 (24.1) | 16 | 2 | 14 | 102 | 9 (8.8) |
| mean AAD (range) * | 60 (22–91) | 62 (33–83) | 62 (33–82) | 62 (37–83) | 60 (27–91) | 58 (30–83) |
| AAD < 40 years | 30 (4.9) | 4 (2.4) | 1 | 3 | 18 | 2 (11.2) |
| AAD 40–49 years | 90 (14.8) | 18 (10.6) | 4 | 14 | 55 | 8 (14.5) |
| AAD 50–59 years | 163 (26.8) | 42 (24.7) | 5 | 37 | 89 | 7 (7.9) |
| AAD 60–69 years | 183 (30.0) | 61 (35.9) | 9 | 52 | 97 | 7 (7.2) |
| AAD 70–79 years | 125 (20.5) | 40 (23.5) | 8 | 32 | 69 | 7 (10.1) |
| AAD > 80 years | 18 (3.0) | 5 [2.9] | 1 | 4 | 12 | 1 (8.3) |
| ER/PR-status available (%) | 407 (100) | 107 (100) | 17 (100) | 90 (100) | 243 (100) | 24 (100) |
| HER2-status available (%) | 323 (100) | 90 (100) | 15 (100) | 75 (100) | 200 (100) | 21 (100) |
| ER-positive (%) | 394 (96.8) | 105 (98.1) | 17 (100) | 88 (97.8) | 234 (96.3) | 24 (100) |
| ER-negative (%) | 13 (3.2) | 2 (1.9) | 0 (0) | 2 (2.2) | 9 (3.7) | 0 (0) |
| PR-positive (%) | 366 (89.9) | 94 (87.9) | 14 (82.4) | 80 (88.9) | 219 (90.1) | 23 (96.0) |
| PR-negative (%) | 41 (10.1) | 13 (12.1) | 3 (17.6) | 10 (11.1) | 24 (9.9) | 1 (4.2) |
| HER2-positive (%) | 38 (11.7) | 13 (14.4) | 2 (13.3) | 11 (14.7) | 20 (10.0) | 4 (19.0) |
| HER2-negative (%) | 285 (88.2) | 77 (85.6) | 13 (86.7) | 64 (85.3) | 180 (90.0) | 17 (81.0) |
| Gene | mBC PTVs (%) | Patients with mBC | ExAC Controls n = 27,173 (%) | mBC vs. ExAC | |
|---|---|---|---|---|---|
| OR (95% CI) | p * | ||||
| BRCA2 | 142 (23.13) | 614 | 105 (0.39) | 77.41 (58.71–102.33) | <10−5 |
| BRCA1 | 28 (4.56) | 614 | 76 (0.28) | 17.04 (10.54–26.82) | <10−5 |
| CHEK2 | 8 (2.35) | 340 | 172 (0.63) | 3.78 (1.59–7.71) | 0.002 |
| PALB2 | 6 (1.76) | 340 | 33 (0.12) | 14.77 (5.02–36.02) | <10−5 |
| ATM | 4 (1.18) | 340 | 96 (0.35) | 3.36 (0.89–8.96) | 0.04 |
| FANCM | 2 (0.59) | 340 | 184 (0.68) | - | - |
| BRIP1 | 1 (0.29) | 340 | 59 (0.22) | - | - |
| CDH1 | 1 (0.29) | 340 | 2 (0.00) | - | - |
| NBN ** | 1 (0.29) | 340 | 42 (0.15) | - | - |
| PTEN | 1 (0.29) | 340 | 1 (0.00) | - | - |
| RAD50 ** | 1 (0.29) | 340 | 84 (0.31) | - | - |
| RAD51C | 1 (0.29) | 340 | 34 (0.13) | - | - |
| Covariat | β | 95% CI | p |
|---|---|---|---|
| FH | 1.78 | −0.97–4.52 | 0.20 |
| ATM | −11.87 | −22.35–−1.39 | 0.03 |
| CHEK2 | −1.96 | −9.09–5.17 | 0.59 |
| PALB2 | 3.55 | −5.98–13.07 | 0.46 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rolfes, M.; Borde, J.; Möllenhoff, K.; Kayali, M.; Ernst, C.; Gehrig, A.; Sutter, C.; Ramser, J.; Niederacher, D.; Horváth, J.; et al. Prevalence of Cancer Predisposition Germline Variants in Male Breast Cancer Patients: Results of the German Consortium for Hereditary Breast and Ovarian Cancer. Cancers 2022, 14, 3292. https://doi.org/10.3390/cancers14133292
Rolfes M, Borde J, Möllenhoff K, Kayali M, Ernst C, Gehrig A, Sutter C, Ramser J, Niederacher D, Horváth J, et al. Prevalence of Cancer Predisposition Germline Variants in Male Breast Cancer Patients: Results of the German Consortium for Hereditary Breast and Ovarian Cancer. Cancers. 2022; 14(13):3292. https://doi.org/10.3390/cancers14133292
Chicago/Turabian StyleRolfes, Muriel, Julika Borde, Kathrin Möllenhoff, Mohamad Kayali, Corinna Ernst, Andrea Gehrig, Christian Sutter, Juliane Ramser, Dieter Niederacher, Judit Horváth, and et al. 2022. "Prevalence of Cancer Predisposition Germline Variants in Male Breast Cancer Patients: Results of the German Consortium for Hereditary Breast and Ovarian Cancer" Cancers 14, no. 13: 3292. https://doi.org/10.3390/cancers14133292