
Contemporary Trends in Malignant Peritoneal Mesothelioma: Incidence and Survival in the United States
Abstract
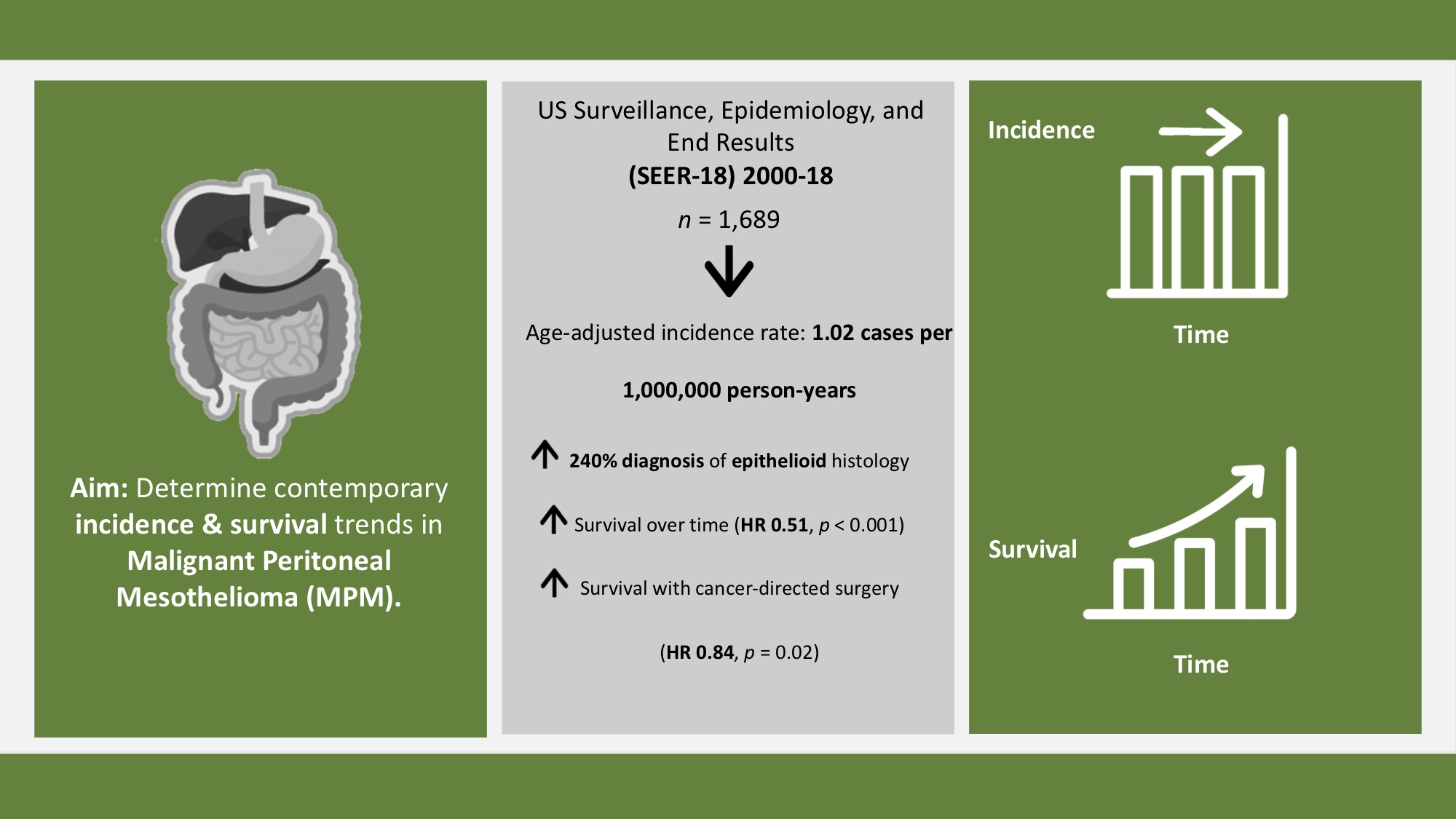
:Simple Summary
Abstract

1. Introduction
2. Materials and Methods
2.1. Data Source
2.2. Study Population-Malignant Peritoneal Mesothelioma
2.3. Clinical and Demographic Variables
2.4. Statistical Analysis
3. Results
3.1. Incidence Trends
3.2. Survival Trends
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Broeckx, G.; Pauwels, P. Malignant peritoneal mesothelioma: A review. Transl. Lung Cancer Res. 2018, 7, 537–542. [Google Scholar] [CrossRef] [PubMed]
- Moolgavkar, S.H.; Meza, R.; Turim, J. Pleural and peritoneal mesotheliomas in SEER: Age effects and temporal trends, 1973–2005. Cancer Causes Control 2009, 20, 935–944. [Google Scholar] [CrossRef] [PubMed]
- Shavelle, R.; Vavra-Musser, K.; Lee, J.; Brooks, J. Life Expectancy in Pleural and Peritoneal Mesothelioma. Lung Cancer Int. 2017, 2017, 2782590. [Google Scholar] [CrossRef] [Green Version]
- Roggli, V.L.; Sharma, A.; Butnor, K.J.; Sporn, T.; Vollmer, R.T. Malignant Mesothelioma and Occupational Exposure to Asbestos: A Clinicopathological Correlation of 1445 Cases. Ultrastruct. Pathol. 2002, 26, 55–65. [Google Scholar] [CrossRef] [PubMed]
- Hodgson, J.T.; Darnton, A. The quantitative risks of mesothelioma and lung cancer in relation to asbestos exposure. Ann. Occup. Hyg. 2000, 44, 565–601. [Google Scholar] [CrossRef] [PubMed]
- Lacourt, A.; Gramond, C.; Rolland, P.; Ducamp, S.; Audignon, S.; Astoul, P.; Chamming, S.; Ilg, A.G.S.; Rinaldo, M.; Raherison, C.; et al. Occupational and non-occupational attributable risk of asbestos exposure for malignant pleural mesothelioma. Thorax 2014, 69, 532–539. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iwatsubo, Y.; Pairon, J.C.; Boutin, C.; Menard, O.; Massin, N.; Caillaud, D.; Orlowski, E.; Galateau-Salle, F.; Bignon, J.; Brochard, P. Pleural Mesothelioma: Dose-Response Relation at Low Levels of Asbestos Exposure in a French Population-based Case-Control Study. Am. J. Epidemiol. 1998, 148, 133–142. [Google Scholar] [CrossRef] [Green Version]
- LE Stang, N.; Bouvier, V.; Glehen, O.; Villeneuve, L.; Galateau-Sallé, F.; Clin, B. Incidence and survival of peritoneal malignant mesothelioma between 1989 and 2015: A population-based study. Cancer Epidemiol. 2019, 60, 106–111. [Google Scholar] [CrossRef]
- Gatta, G.; van der Zwan, J.M.; Casali, P.G.; Siesling, S.; Tos, A.P.D.; Kunkler, I.; Otter, R.; Licitra, L.; Mallone, S.; Tavilla, A.; et al. Rare cancers are not so rare: The rare cancer burden in Europe. Eur. J. Cancer 2011, 47, 2493–2511. [Google Scholar] [CrossRef]
- Chicago Consensus Working Group; Schuitevoerder, D.; Izquierdo, F.J.; Plana, A.; Nash, G.M.; Fernandez, L.J.; Kluger, M.D.; Mack, L.A.; Mammen, J.M.V.; Pameijer, C.R.; et al. The Chicago Consensus on peritoneal surface malignancies: Management of peritoneal mesothelioma. Cancer 2020, 126, 2547–2552. [Google Scholar] [CrossRef]
- Edwards, J.G.; Abrams, K.R.; Leverment, J.N.; Spyt, T.J.; Waller, D.A.; O’Byrne, K.J. Prognostic factors for malignant mesothelioma in 142 patients: Validation of CALGB and EORTC prognostic scoring systems. Thorax 2000, 55, 731–735. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Verma, V.; Sleightholm, R.L.; Rusthoven, C.G.; Koshy, M.; Sher, D.J.; Grover, S.; Simone, C.B. Malignant Peritoneal Mesothelioma: National Practice Patterns, Outcomes, and Predictors of Survival. Ann. Surg. Oncol. 2018, 25, 2018–2026. [Google Scholar] [CrossRef] [PubMed]
- Henley, S.J.; Larson, T.C.; Wu, M.; Antao, V.; Lewis, M.; Pinheiro, G.A.; Eheman, C. Mesothelioma incidence in 50 states and the District of Columbia, United States, 2003–2008. Int. J. Occup. Environ. Health 2013, 19, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beal, E.W.; Ahmed, A.; Grotz, T.; Leiting, J.; Fournier, K.F.; Lee, A.J.; Dineen, S.; Dessureault, S.; Baumgartner, J.M.; Veerapong, J.; et al. Trends in the indications for and short-term outcomes of cytoreductive surgery with hyperthermic intraperitoneal chemotherapy. Am. J. Surg. 2020, 219, 478–483. [Google Scholar] [CrossRef]
- Helm, J.H.; Miura, J.T.; Glenn, J.A.; Marcus, R.K.; Larrieux, G.; Jayakrishnan, T.T.; Donahue, A.E.; Gamblin, T.C.; Turaga, K.K.; Johnston, F.M. Cytoreductive Surgery and Hyperthermic Intraperitoneal Chemotherapy for Malignant Peritoneal Mesothelioma: A Systematic Review and Meta-analysis. Ann. Surg. Oncol. 2014, 22, 1686–1693. [Google Scholar] [CrossRef]
- Surveillance, Epidemiology, and End Results (SEER) Program. SEER*Stat Database: Mortality-All COD, Aggregated with State, Total U.S. (1969–2018) <Katrina/Rita Population Adjustment>, National Cancer Institute, DCCPS, Surveillance Research Program. Available online: www.seer.cancer.gov (accessed on 26 January 2022).
- SEER*Stat Databases: November 2020 Submission. Available online: https://seer.cancer.gov/data-software/documentation/seerstat/nov2020/ (accessed on 26 January 2022).
- SEER ICD-O-3 Coding Materials. Available online: https://seer.cancer.gov/icd-o-3/ (accessed on 26 January 2022).
- Taioli, E.; Wolf, A.S.; Camacho-Rivera, M.; Kaufman, A.; Lee, D.-S.; Nicastri, D.; Rosenzweig, K.; Flores, R.M. Determinants of Survival in Malignant Pleural Mesothelioma: A Surveillance, Epidemiology, and End Results (SEER) Study of 14,228 Patients. PLoS ONE 2015, 10, e0145039. [Google Scholar] [CrossRef] [Green Version]
- Surveillance Research Program, National Cancer Institute SEER*Stat Software. Available online: Seer.cancer.gov/seerstat (accessed on 26 January 2022).
- National Cancer Institute. Joinpoint Regression Program, Version 4.8.0.1; Statistical Methodology and Applications Branch, Surveillance Research Program, National Cancer Institute: Bethesda, MD, USA, April 2020. [Google Scholar]
- StataCorp. Stata Statistical Software: Release 16; StataCorp LLC: College Station, TX, USA, 2019. [Google Scholar]
- Spirtas, R.; Heineman, E.F.; Bernstein, L.; Beebe, G.W.; Keehn, R.J.; Stark, A.; Harlow, B.L.; Benichou, J. Malignant mesothelioma: Attributable risk of asbestos exposure. Occup. Environ. Med. 1994, 51, 804–811. [Google Scholar] [CrossRef] [Green Version]
- Beebe-Dimmer, J.L.; Fryzek, J.P.; Yee, C.L.; Dalvi, T.B.; Garabrant, D.H.; Schwartz, A.G.; Gadgeel, S. Mesothelioma in the United States: A Surveillance, Epidemiology, and End Results (SEER)–Medicare investigation of treatment patterns and overall survival. Clin. Epidemiol. 2016, 8, 743–750. [Google Scholar] [CrossRef] [Green Version]
- Larson, T.; Melnikova, N.; Davis, S.I.; Jamison, P. Incidence and Descriptive Epidemiology of Mesothelioma in the United States, 1999–2002. Int. J. Occup. Environ. Health 2007, 13, 398–403. [Google Scholar] [CrossRef]
- Yan, T.D.; Deraco, M.; Baratti, D.; Kusamura, S.; Elias, D.; Glehen, O.; Gilly, F.N.; Levine, E.A.; Shen, P.; Mohamed, F.; et al. Cytoreductive Surgery and Hyperthermic Intraperitoneal Chemotherapy for Malignant Peritoneal Mesothelioma: Multi-Institutional Experience. J. Clin. Oncol. 2009, 27, 6237–6242. [Google Scholar] [CrossRef]
- Bijelic, L.; Darcy, K.; Do, J.S.; Tian, C.; Cannon, T. Predictors and Outcomes of Surgery in Peritoneal Mesothelioma: An Analysis of 2000 Patients from the National Cancer Database. Ann. Surg. Oncol. 2020, 27, 2974–2982. [Google Scholar] [CrossRef] [PubMed]
- Ullah, A.; Waheed, A.; Khan, J.; Mishra, A.; Tareen, B.; Nama, N.; Karki, N.R.; Panezai, M.S.; Zarate, L.V.; White, J.; et al. Incidence, Survival Analysis and Future Perspective of Primary Peritoneal Mesothelioma (PPM): A Population-Based Study from SEER Database. Cancers 2022, 14, 942. [Google Scholar] [CrossRef] [PubMed]
- Malgras, B.; Network, O.B.O.T.R.; Gayat, E.; Aoun, O.; Dico, R.L.; Eveno, C.; Pautrat, K.; Delhorme, J.-B.; Passot, G.; Marchal, F.; et al. Impact of Combination Chemotherapy in Peritoneal Mesothelioma Hyperthermic Intraperitoneal Chemotherapy (HIPEC): The RENAPE Study. Ann. Surg. Oncol. 2018, 25, 3271–3279. [Google Scholar] [CrossRef] [PubMed]
- Hassan, R.; Alexander, R.; Antman, K.; Boffetta, P.; Churg, A.; Coit, D.; Hausner, P.; Kennedy, R.; Kindler, H.; Metintas, M.; et al. Current treatment options and biology of peritoneal mesothelioma: Meeting summary of the first NIH peritoneal mesothelioma conference. Ann. Oncol. 2006, 17, 1615–1619. [Google Scholar] [CrossRef] [PubMed]
- Liu, S.; Staats, P.; Lee, M.; Alexander, H.R.; Burke, A.P. Diffuse mesothelioma of the peritoneum: Correlation between histological and clinical parameters and survival in 73 patients. Pathology 2014, 46, 604–609. [Google Scholar] [CrossRef]
- Robinson, B.W.; Lake, R.A. Advances in Malignant Mesothelioma. N. Engl. J. Med. 2005, 353, 1591–1603. [Google Scholar] [CrossRef] [Green Version]
- Louw, A.; Lee, Y.C.G.; Acott, N.; Creaney, J.; Vliet, C.; Chai, S.M. Diagnostic utility of BAP1 for malignant pleural mesothelioma in pleural fluid specimens with atypical morphology. Cytopathology 2021, 33, 84–92. [Google Scholar] [CrossRef]
- Baratti, D.; Kusamura, S.; Cabras, A.D.; Deraco, M. Cytoreductive Surgery with Selective Versus Complete Parietal Peritonectomy Followed by Hyperthermic Intraperitoneal Chemotherapy in Patients with Diffuse Malignant Peritoneal Mesothelioma: A Controlled Study. Ann. Surg. Oncol. 2012, 19, 1416–1424. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| MPM | |
|---|---|
| (n = 1689) | |
| Sex | |
| Male | 937 (55.4%) |
| Female | 752 (44.5%) |
| Age | |
| 0–19 | 5 (0.3%) |
| 20–34 | 71 (4.2%) |
| 35–49 | 259 (15.3%) |
| 50–64 | 530 (31.3%) |
| 65–79 | 621 (36.7%) |
| >80 | 203 (12.0%) |
| Race/Ethnicity | |
| White | 1271 (75.2%) |
| Black | 99 (5.8%) |
| Hispanic | 228 (13.5%) |
| Other | 86 (5.0%) |
| Year of Diagnosis | |
| 2000–2002 | 204 (12.1%) |
| 2003–2005 | 271 (16.0%) |
| 2006–2008 | 257 (15.2%) |
| 2009–2011 | 272 (16.1%) |
| 2012–2014 | 273 (16.2%) |
| 2015–2018 | 412 (24.4%) |
| Histology | |
| Epithelioid | 632 (37.4%) |
| Biphasic | 62 (3.6%) |
| Sarcomatoid | 54 (3.2%) |
| Undefined | 941 (55.7%) |
| Site | |
| Peritoneum and Retroperitoneum | 1641 (97.2%) |
| Abdomen and Soft tissue | 28 (1.6%) |
| Ovary | 20 (1.1%) |
| Stage | |
| Localized | 200 (11.8%) |
| Regional | 232 (13.7%) |
| Distant | 741 (43.8%) |
| Unknown | 516 (30.5%) |
| Extent of Resection | |
| Removal of Primary Site | 137 (8.0%) |
| Debulking | 270 (15.9%) |
| Radical | 145 (8.5%) |
| PC | APC (95% CI) | p Value | |
|---|---|---|---|
| Unadjusted Overall | 64.9 | 1.2 * (0.07, 2.31) | 0.038 |
| Adjusted Overall | 38.9 | 0.1 (−1.0, 1.3) | 0.850 |
| Unadjusted Sex | |||
| Male | 38.4 | 0.5 (−0.8, 1.8) | 0.451 |
| Female | 107.9 | 2.1 * (0.7, 3.4) | 0.005 |
| Adjusted Sex | |||
| Male | 10.5 | −0.9 (−2.2, 0.5) | 0.200 |
| Female | 88.6 | 1.3 (−0.0, 2.7) | 0.060 |
| Unadjusted Histology | |||
| Epithelioid | 292.5 | 3.7 * (1.9, 5.5) | <0.001 |
| Biphasic | 423.3 | 2.2 (−1.6, 6.2) | 0.238 |
| Undefined | −2.9 | −1.0 * (−2.0, −0.02) | 0.046 |
| Sarcomatoid | - | - | |
| Adjusted Histology | |||
| Epithelioid | 239.7 | 2.6 * (0.7, 4.5) | 0.010 |
| Biphasic | 325.1 | 1.1 (−2.8, 5.1) | 0.560 |
| Undefined | −19 | −2.1 * (−3.1, −1.1) | 0.001 |
| Sarcomatoid | - | - |
| HR | p-Value | 95% CI | |
|---|---|---|---|
| Sex | |||
| Male (reference) | - | ||
| Female | 0.66 | <0.001 | (0.58, 0.76) |
| Age a | 1.55 | <0.001 | (1.44, 1.67) |
| Race/Ethnicity | |||
| Other (reference) White Black Hispanic (all races) | - 0.97 0.86 1.11 | 0.821 0.472 0.539 | (0.72, 1.30) (0.57, 1.30) (0.80, 1.55) |
| Year of diagnosis | |||
| 2000–2002 (reference) 2003–2005 2006–2008 2009–2011 2012–2014 2015–2018 | - 0.73 0.66 0.58 0.60 0.51 | 0.008 0.003 <0.001 <0.001 <0.001 | (0.57, 0.92) (0.50, 0.87) (0.44, 0.76) (0.45, 0.79) (0.38, 0.67) |
| Histology | |||
| Epithelioid (reference) Undefined Biphasic Sarcomatoid | - 1.11 1.49 2.85 | 0.149 0.032 <0.001 | (0.96, 1.28) (1.03, 2.13) (1.99, 4.08) |
| Receipt of Surgery | 0.84 | 0.024 | (0.72, 0.98) |
| Stage | |||
| Localized Regional Distant | 0.88 1.01 1.10 | 0.359 0.925 0.336 | (0.68, 1.15) (0.79, 1.30) (0.91, 1.33) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Calthorpe, L.; Romero-Hernandez, F.; Miller, P.; Conroy, P.C.; Hirose, K.; Kim, A.; Kirkwood, K.; Nakakura, E.; Corvera, C.; Maker, A.V.; et al. Contemporary Trends in Malignant Peritoneal Mesothelioma: Incidence and Survival in the United States. Cancers 2023, 15, 229. https://doi.org/10.3390/cancers15010229
Calthorpe L, Romero-Hernandez F, Miller P, Conroy PC, Hirose K, Kim A, Kirkwood K, Nakakura E, Corvera C, Maker AV, et al. Contemporary Trends in Malignant Peritoneal Mesothelioma: Incidence and Survival in the United States. Cancers. 2023; 15(1):229. https://doi.org/10.3390/cancers15010229
Chicago/Turabian StyleCalthorpe, Lucia, Fernanda Romero-Hernandez, Phoebe Miller, Patricia C. Conroy, Kenzo Hirose, Alex Kim, Kimberly Kirkwood, Eric Nakakura, Carlos Corvera, Ajay V. Maker, and et al. 2023. "Contemporary Trends in Malignant Peritoneal Mesothelioma: Incidence and Survival in the United States" Cancers 15, no. 1: 229. https://doi.org/10.3390/cancers15010229