Endobiliary Radiofrequency Ablation Combined with Gemcitabine and Cisplatin in Patients with Unresectable Extrahepatic Cholangiocarcinoma

 , , ,
, , ,
Abstract
:1. Introduction
2. Patients and Methods
2.1. Study Design and Patients
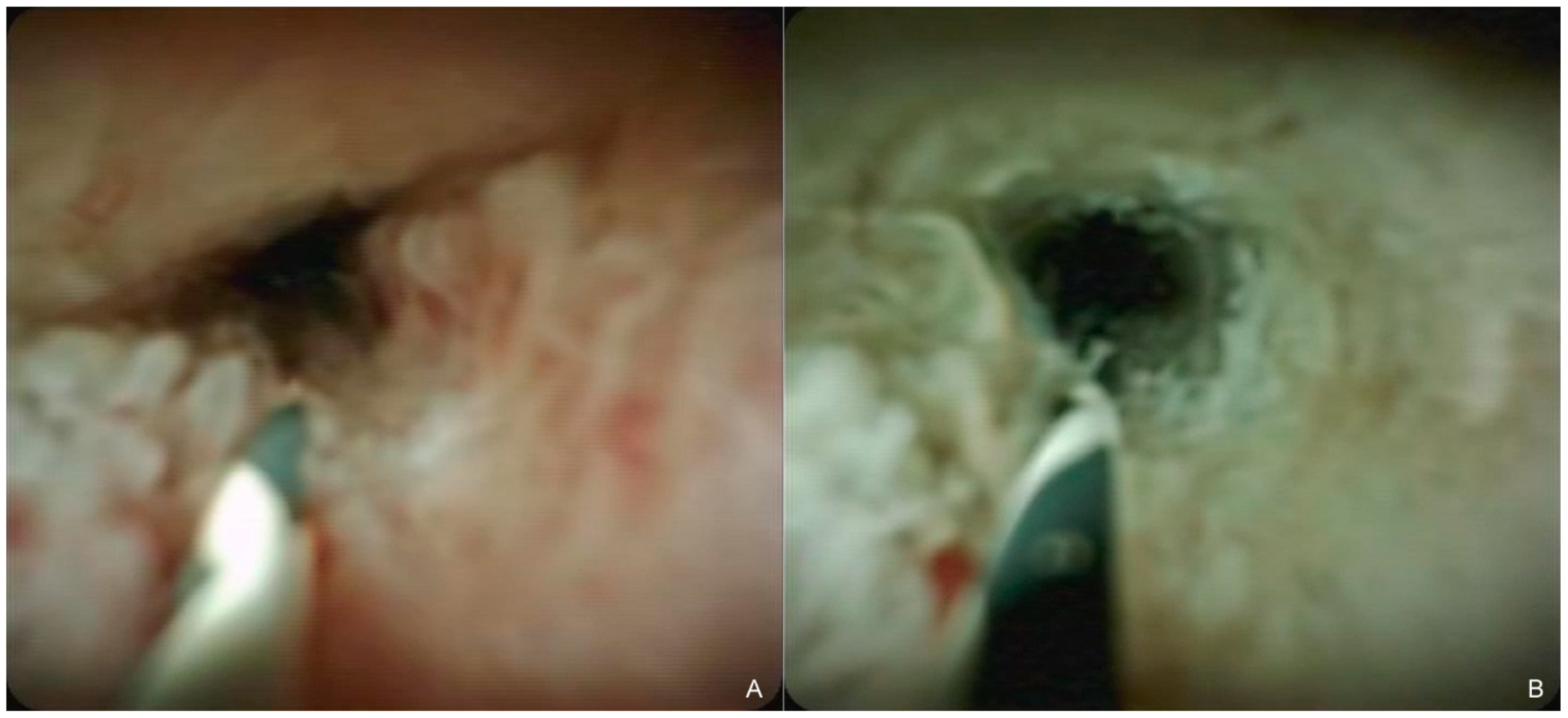
2.2. Endobiliary RFA with SEMS Placement
2.3. GC Therapy
2.4. Follow-Up
2.5. Outcomes and Definitions
2.6. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. SEMS Placement with/without Endobiliary RFA
3.3. Treatment Exposure
3.4. Efficacy
3.5. Safety
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Valle, J.W.; Borbath, I.; Khan, S.A.; Huguet, F.; Gruenberger, T.; Arnold, D. Biliary cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2016, 27, v28–v37. [Google Scholar] [CrossRef] [PubMed]
- Khan, S.A.; Davidson, B.R.; Goldin, R.D.; Heaton, N.; Karani, J.; Pereira, S.P.; Rosenberg, W.M.; Tait, P.; Taylor-Robinson, S.D.; Thillainayagam, A.V.; et al. Guidelines for the diagnosis and treatment of cholangiocarcinoma: An update. Gut 2012, 61, 1657–1669. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nagino, M.; Hirano, S.; Yoshitomi, H.; Aoki, T.; Uesaka, K.; Unno, M.; Ebata, T.; Konishi, M.; Sano, K.; Shimada, K.; et al. Clinical practice guidelines for the management of biliary tract cancers 2019: The 3rd English edition. J. Hepatobiliary Pancreat Sci. 2021, 28, 26–54. [Google Scholar] [CrossRef] [PubMed]
- Lauterio, A.; De Carlis, R.; Centonze, L.; Buscemi, V.; Incarbone, N.; Vella, I.; De Carlis, L. Current Surgical Management of Peri-Hilar and Intra-Hepatic Cholangiocarcinoma. Cancers 2021, 13, 3657. [Google Scholar] [CrossRef]
- Rizzo, A.; Brandi, G. Pitfalls, challenges, and updates in adjuvant systemic treatment for resected biliary tract cancer. Expert Rev. Gastroenterol. Hepatol. 2021, 15, 547–554. [Google Scholar] [CrossRef]
- Valle, J.; Wasan, H.; Palmer, D.H.; Cunningham, D.; Anthoney, A.; Maraveyas, A.; Madhusudan, S.; Iveson, T.; Hughes, S.; Pereira, S.P.; et al. Cisplatin plus gemcitabine versus gemcitabine for biliary tract cancer. N. Engl. J. Med. 2010, 362, 1273–1281. [Google Scholar] [CrossRef] [Green Version]
- Dumonceau, J.M.; Tringali, A.; Papanikolaou, I.S.; Blero, D.; Mangiavillano, B.; Schmidt, A.; Vanbiervliet, G.; Costamagna, G.; Devière, J.; García-Cano, J.; et al. Endoscopic biliary stenting: Indications, choice of stents, and results: European Society of Gastrointestinal Endoscopy (ESGE) Clinical Guideline—Updated October 2017. Endoscopy 2018, 50, 910–930. [Google Scholar] [CrossRef] [Green Version]
- Nakai, Y.; Isayama, H.; Wang, H.P.; Rerknimitr, R.; Khor, C.; Yasuda, I.; Kogure, H.; Moon, J.H.; Lau, J.; Lakhtakia, S.; et al. International consensus statements for endoscopic management of distal biliary stricture. J. Gastroenterol. Hepatol. 2020, 35, 967–979. [Google Scholar] [CrossRef] [Green Version]
- Togawa, O.; Isayama, H.; Tsujino, T.; Nakai, Y.; Kogure, H.; Hamada, T.; Sasaki, T.; Yashima, Y.; Yagioka, H.; Arizumi, T.; et al. Management of dysfunctional covered self-expandable metallic stents in patients with malignant distal biliary obstruction. J. Gastroenterol. 2013, 48, 1300–1307. [Google Scholar] [CrossRef]
- Inoue, T.; Naitoh, I.; Suzuki, Y.; Okumura, F.; Haneda, K.; Kitano, R.; Yoshida, M.; Hayashi, K.; Yoneda, M. Multi-center study of endoscopic revision after side-by-side metal stent placement for malignant hilar biliary obstruction. Dig. Endosc. 2021, 33, 807–814. [Google Scholar] [CrossRef]
- Sofi, A.A.; Khan, M.A.; Das, A.; Sachdev, M.; Khuder, S.; Nawras, A.; Lee, W. Radiofrequency ablation combined with biliary stent placement versus stent placement alone for malignant biliary strictures: A systematic review and meta-analysis. Gastrointest Endosc. 2018, 87, 944–951.e1. [Google Scholar] [CrossRef] [PubMed]
- Inoue, T.; Yoneda, M. Updated evidence on the clinical impact of endoscopic radiofrequency ablation in the treatment of malignant biliary obstruction. Dig. Endosc. 2022, 34, 345–358. [Google Scholar] [CrossRef] [PubMed]
- Inoue, T.; Ibusuki, M.; Kitano, R.; Kobayashi, Y.; Ohashi, T.; Nakade, Y.; Sumida, Y.; Ito, K.; Yoneda, M. Endobiliary radiofrequency ablation combined with bilateral metal stent placement for malignant hilar biliary obstruction. Endoscopy 2020, 52, 595–599. [Google Scholar] [CrossRef] [PubMed]
- Eisenhauer, E.A.; Therasse, P.; Bogaerts, J.; Schwartz, L.H.; Sargent, D.; Ford, R.; Dancey, J.; Arbuck, S.; Gwyther, S.; Mooney, M.; et al. New response evaluation criteria in solid tumours: Revised RECIST guideline (version 1.1). Eur. J. Cancer 2009, 45, 228–247. [Google Scholar] [CrossRef]
- Isayama, H.; Hamada, T.; Yasuda, I.; Itoi, T.; Ryozawa, S.; Nakai, Y.; Kogure, H.; Koike, K. Tokyo criteria 2014 for transpapillary biliary stenting. Dig. Endosc. 2015, 27, 259–264. [Google Scholar] [CrossRef]
- Kanda, Y. Investigation of the freely available easy-to-use software ‘EZR’ for medical statistics. Bone Marrow Transpl. 2013, 48, 452–458. [Google Scholar] [CrossRef] [Green Version]
- Almadi, M.A.; Barkun, A.; Martel, M. Plastic vs. self-expandable metal stents for palliation in malignant biliary obstruction: A series of meta-analyses. Am. J. Gastroenterol. 2017, 112, 260–273. [Google Scholar] [CrossRef]
- Xia, M.X.; Pan, Y.L.; Cai, X.B.; Wu, J.; Gao, D.J.; Ye, X.; Wang, T.T.; Hu, B. Comparison of endoscopic bilateral metal stent drainage with plastic stents in the palliation of unresectable hilar biliary malignant strictures: Large multicenter study. Dig. Endosc. 2021, 33, 179–189. [Google Scholar] [CrossRef]
- Steel, A.W.; Postgate, A.J.; Khorsandi, S.; Nicholls, J.; Jiao, L.; Vlavianos, P.; Habib, N.; Westaby, D. Endoscopically applied radiofrequency ablation appears to be safe in the treatment of malignant biliary obstruction. Gastrointest Endosc. 2011, 73, 149–153. [Google Scholar] [CrossRef]
- Kim, E.J.; Chung, D.H.; Kim, Y.J.; Kim, Y.S.; Park, Y.H.; Kim, K.K.; Cho, J.H. Endobiliary radiofrequency ablation for distal extrahepatic cholangiocarcinoma: A clinicopathological study. PLoS ONE 2018, 13, e0206694. [Google Scholar] [CrossRef]
- Haen, S.P.; Pereira, P.L.; Salih, H.R.; Rammensee, H.G.; Gouttefangeas, C. More than just tumor destruction: Immunomodulation by thermal ablation of cancer. Clin. Dev. Immunol. 2011, 2011, 160250. [Google Scholar] [CrossRef] [PubMed]
- Giardino, A.; Innamorati, G.; Ugel, S.; Perbellini, O.; Girelli, R.; Frigerio, I.; Regi, P.; Scopelliti, F.; Butturini, G.; Paiella, S.; et al. Immunomodulation after radiofrequency ablation of locally advanced pancreatic cancer by monitoring the immune response in 10 patients. Pancreatology 2017, 17, 962–966. [Google Scholar] [CrossRef] [PubMed]
- Llovet, J.M.; De Baere, T.; Kulik, L.; Haber, P.K.; Greten, T.F.; Meyer, T.; Lencioni, R. Locoregional therapies in the era of molecular and immune treatments for hepatocellular carcinoma. Nat. Rev. Gastroenterol. Hepatol. 2021, 18, 293–313. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.; Wang, J.; Zhou, H.; Zhou, Y.; Wang, Y.; Jin, H.; Lou, Q.; Zhang, X. Efficacy and safety of endoscopic radiofrequency ablation for unresectable extrahepatic cholangiocarcinoma: A randomized trial. Endoscopy 2018, 50, 751–760. [Google Scholar] [CrossRef]
- Gao, D.J.; Yang, J.F.; Ma, S.R.; Wu, J.; Wang, T.T.; Jin, H.B.; Xia, M.X.; Zhang, Y.C.; Shen, H.Z.; Ye, X.; et al. Endoscopic radiofrequency ablation plus plastic stent placement versus stent placement alone for unresectable extrahepatic biliary cancer: A multicenter randomized controlled trial. Gastrointest Endosc. 2021, 94, 91–100.e2. [Google Scholar] [CrossRef]
- Yang, J.; Wang, J.; Zhou, H.; Wang, Y.; Huang, H.; Jin, H.; Lou, Q.; Shah, R.J.; Zhang, X. Endoscopic radiofrequency ablation plus a novel oral 5-fluorouracil compound versus radiofrequency ablation alone for unresectable extrahepatic cholangiocarcinoma. Gastrointest Endosc. 2020, 92, 1204–1212.e1. [Google Scholar] [CrossRef]
- Inoue, T.; Ito, K.; Yoneda, M. Novel balloon catheter-based endobiliary radiofrequency ablation system: Ex-vivo experimental study. Dig. Endosc. 2020, 32, 974–978. [Google Scholar] [CrossRef]
- Laleman, W.; van der Merwe, S.; Verbeke, L.; Vanbeckevoort, D.; Aerts, R.; Prenen, H.; Van Cutsem, E.; Verslype, C. A new intraductal radiofrequency ablation device for inoperable biliopancreatic tumors complicated by obstructive jaundice: The IGNITE-1 study. Endoscopy 2017, 49, 977–982. [Google Scholar] [CrossRef]
- Lee, Y.N.; Jeong, S.; Choi, H.J.; Cho, J.H.; Cheon, Y.K.; Park, S.W.; Kim, Y.S.; Lee, D.H.; Moon, J.H. The safety of newly developed automatic temperature-controlled endobiliary radiofrequency ablation system for malignant biliary strictures: A prospective multicenter study. J. Gastroenterol. Hepatol. 2019, 34, 1454–1459. [Google Scholar] [CrossRef]
- Inoue, T.; Kutsumi, H.; Ibusuki, M.; Yoneda, M. Feasibility of balloon-based endobiliary radiofrequency ablation under cholangioscopy guidance in a swine model. Sci. Rep. 2021, 11, 14254. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| With-RFA Group | Without-RFA Group | p Value | ||
|---|---|---|---|---|
| Number of patients, n | 25 | 25 | ||
| Sex (male/female), n | 10/15 | 17/8 | 0.088 | |
| Mean age, years (range) | 78 (50–86) | 74 (48–85) | 0.073 | |
| ECOG performance status, n (%) | 0.242 | |||
| 0 | 9 (36) | 12 (48) | ||
| 1 | 13 (52) | 13 (52) | ||
| 2 | 3 (12) | 0 | ||
| Diagnosis, n (%) | ||||
| Extrahepatic cholangiocaricinoma (adenocarcinoma) | 25 (100) | 25 (100) | 1.000 | |
| Location of tumor, n (%) | 1.000 | |||
| Hilar | 21 (84) | 22 (88) | ||
| Distal | 4 (16) | 3 (12) | ||
| Metastatic, n (%) | 12 (48) | 15 (60) | 0.571 | |
| Metastatic site †, n (%) | ||||
| Peritoneum | 6 (24) | 2 (8) | 0.247 | |
| Liver | 5 (20) | 5 (20) | 1.000 | |
| Lymph nodes | 4 (16) | 5 (20) | 1.000 | |
| Bone | 1 (4) | 4 (16) | 0.349 | |
| Lung | 0 | 4 (16) | 0.110 | |
| Adrenal | 0 | 1 (4) | 1.000 | |
| Cholangitis ‡, n (%) | 5 (20) | 3 (12) | 0.702 | |
| Mean bilirubin level ‡, mg/dL (range) | 1.76 (0.41–20.74) | 2.69 (0.31–18.60) | 0.146 | |
| Mean alkaline phosphatase level ‡, U/L (range) | 864 (276–3772) | 888 (197–3372) | 0.091 | |
| Mean CEA, ng/mL | 10.1 (1–862) | 9.8 (1–1120) | 0.745 | |
| Mean CA19-9, U/mL (range) | 1086 (2–140054) | 912 (2–152510) | 0.564 | |
| With-RFA Group | Without-RFA Group | p Value | ||
|---|---|---|---|---|
| Clinical success, n (%) | 25/25 (100) | 25/25 (100) | 1.000 | |
| Procedure-related adverse events besides RBO, n (%) | 2/25 (8) | 2/25 (8) | 1.000 | |
| Cholangitis | 1 | 1 | ||
| Pancreatitis | 1 | 0 | ||
| Bleeding | 0 | 1 | ||
| Incidence of RBO, n (%) | 12/25 (44) | 15/25 (60) | 0.571 | |
| Median time to RBO, months (95% CI) | 10.7 (5.1-NA) | 5.2 (3.0-NA) | 0.048 | |
| 6-month non-RBO rate | 71% | 39% | ||
| 1-year non-RBO rate | 46% | 33% | ||
| With-RFA Group | Without-RFA Group | p Value | ||
|---|---|---|---|---|
| Best overall response, n (%) | ||||
| Complete response | 0 | 0 | 1.000 | |
| Partial response | 4/22 (18) | 4/23 (17) | 1.000 | |
| Stable disease | 14/22 (64) | 13/23 (57) | 0.763 | |
| Progressive disease | 4/22 (18) | 6/23 (26) | 0.722 | |
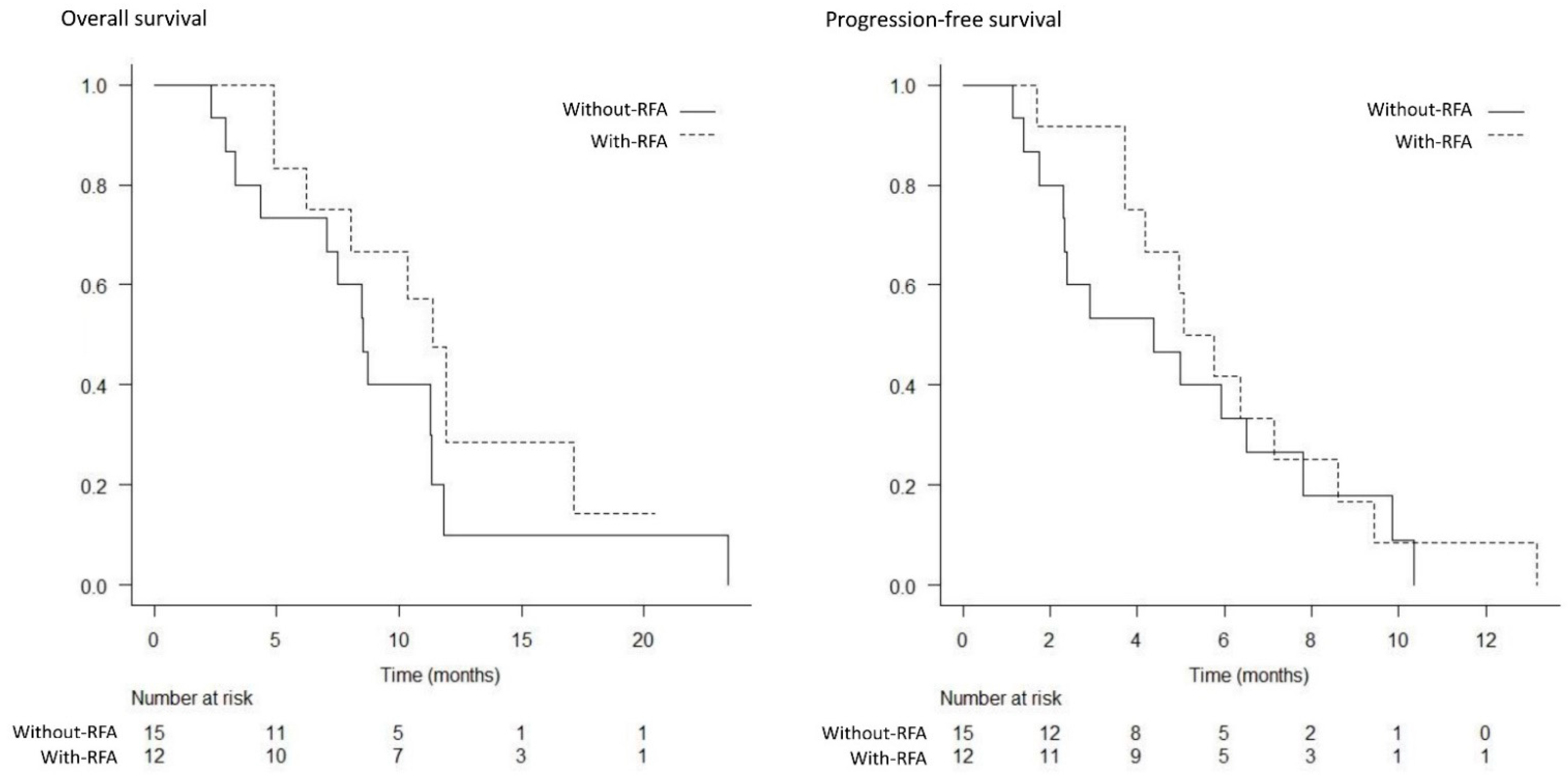
| Median overall survival, months (95% CI) | ||||
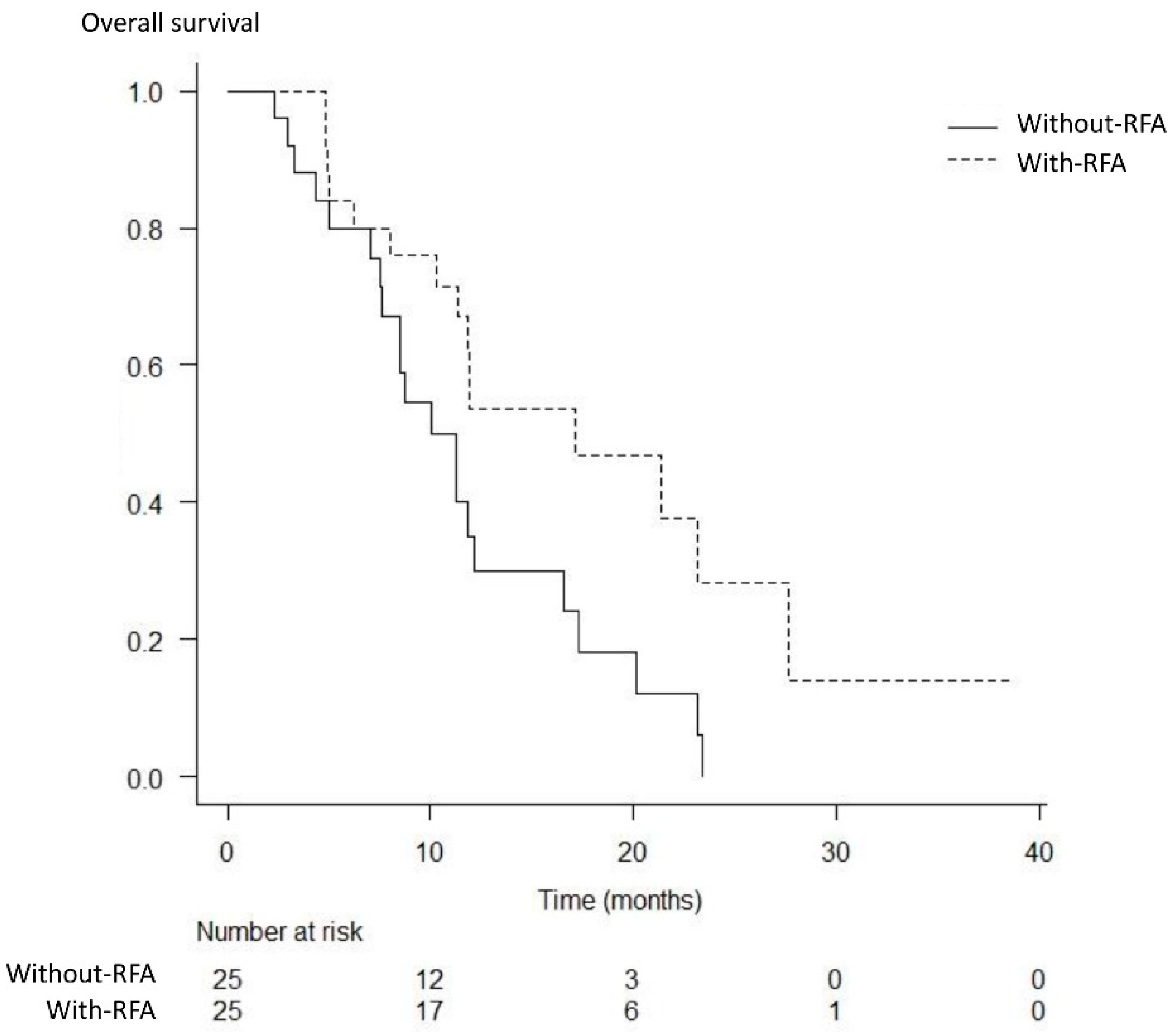
| Total population | 17.1 (10.3–27.6) | 11.3 (7.5–12.1) | 0.017 | |
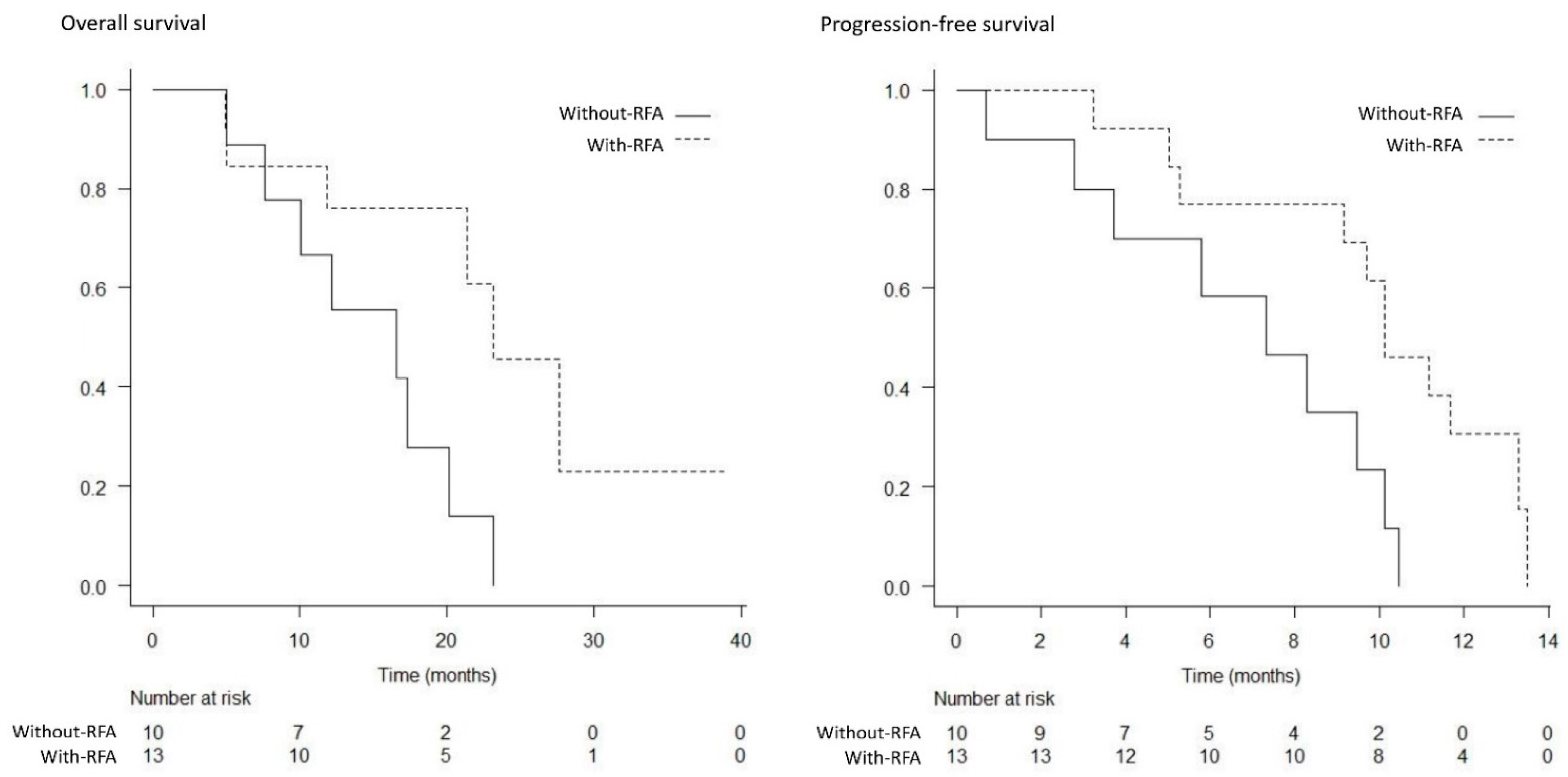
| Locally advanced | 23.1 (11.8–NA) | 16.6 (5.0–20.1) | 0.032 | |
| Metastatic | 11.4 (4.9–17.1) | 8.5 (3.3–11.3) | 0.180 | |
| Progression-free survival, months (95% CI) | ||||
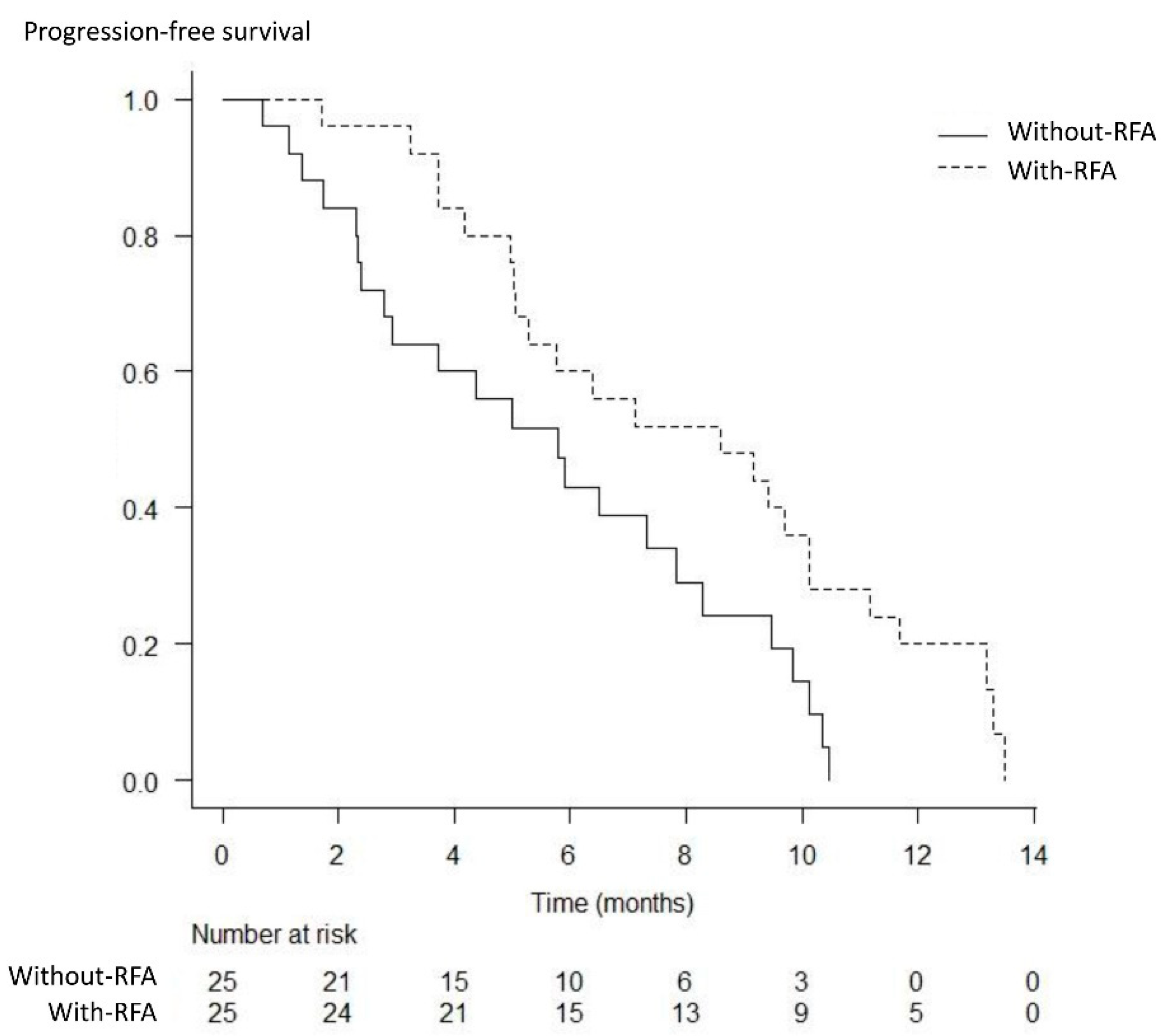
| Total population | 8.6 (5.1–10.1) | 5.8 (2.8–7.8) | 0.014 | |
| Locally advanced | 10.1 (5.3–13.3) | 7.3 (0.7–10.1) | 0.015 | |
| Metastatic | 5.4 (3.7–8.6) | 4.4 (1.7–6.5) | 0.529 | |
| With-RFA Group | Without-RFA Group | p Value | |
|---|---|---|---|
| Hematological toxicities, n (%) | |||
| Anemia | 8/25 (32) | 7/25 (28) | 1.000 |
| Thrombocytopenia | 5/25 (20) | 7/25 (28) | 0.742 |
| Leukopenia | 8/25 (32) | 8/25 (32) | 1.000 |
| Neutropenia | 13/25 (52) | 11/25 (44) | 0.778 |
| Febrile neutropenia | 0 | 0 | |
| Non-hematological toxicities *, n (%) | |||
| Biliary tract infection | 2/25 (8) | 1/25 (4) | 1.000 |
| Appetite loss | 1/25 (4) | 0 | 1.000 |
| Urticaria | 1/25 (4) | 1/25 (4) | 1.000 |
| Constipation | 0 | 1/25 (4) | 1.000 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Inoue, T.; Naitoh, I.; Kitano, R.; Ibusuki, M.; Kobayashi, Y.; Sumida, Y.; Nakade, Y.; Ito, K.; Yoneda, M. Endobiliary Radiofrequency Ablation Combined with Gemcitabine and Cisplatin in Patients with Unresectable Extrahepatic Cholangiocarcinoma. Curr. Oncol. 2022, 29, 2240-2251. https://doi.org/10.3390/curroncol29040182
Inoue T, Naitoh I, Kitano R, Ibusuki M, Kobayashi Y, Sumida Y, Nakade Y, Ito K, Yoneda M. Endobiliary Radiofrequency Ablation Combined with Gemcitabine and Cisplatin in Patients with Unresectable Extrahepatic Cholangiocarcinoma. Current Oncology. 2022; 29(4):2240-2251. https://doi.org/10.3390/curroncol29040182
Chicago/Turabian StyleInoue, Tadahisa, Itaru Naitoh, Rena Kitano, Mayu Ibusuki, Yuji Kobayashi, Yoshio Sumida, Yukiomi Nakade, Kiyoaki Ito, and Masashi Yoneda. 2022. "Endobiliary Radiofrequency Ablation Combined with Gemcitabine and Cisplatin in Patients with Unresectable Extrahepatic Cholangiocarcinoma" Current Oncology 29, no. 4: 2240-2251. https://doi.org/10.3390/curroncol29040182