The Initial Factors with Strong Predictive Value in Relation to Six-Month Outcome among Patients Operated due to Extra-Axial Hematomas

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
Statistical Analysis
3. Results
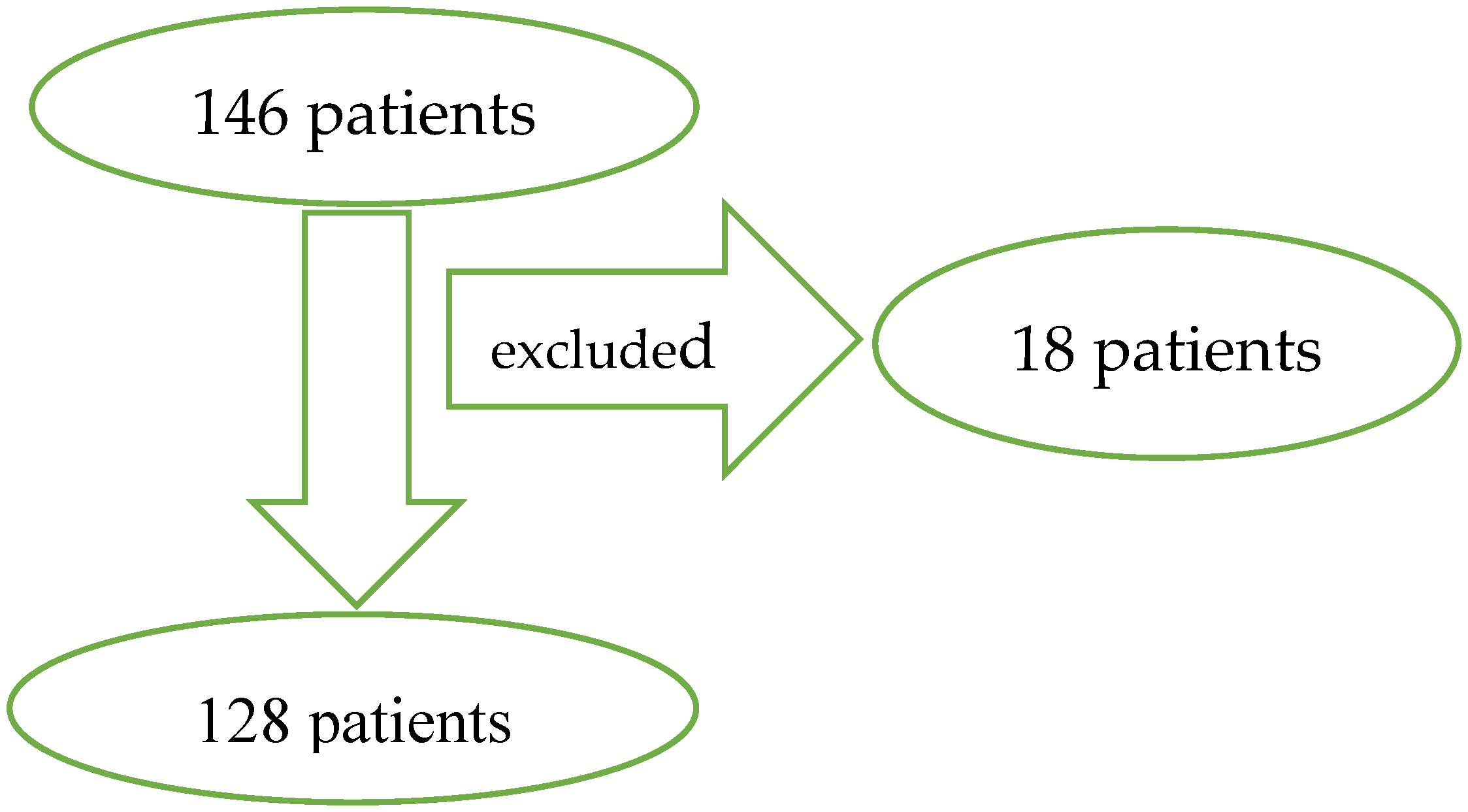
3.1. Group Presentation
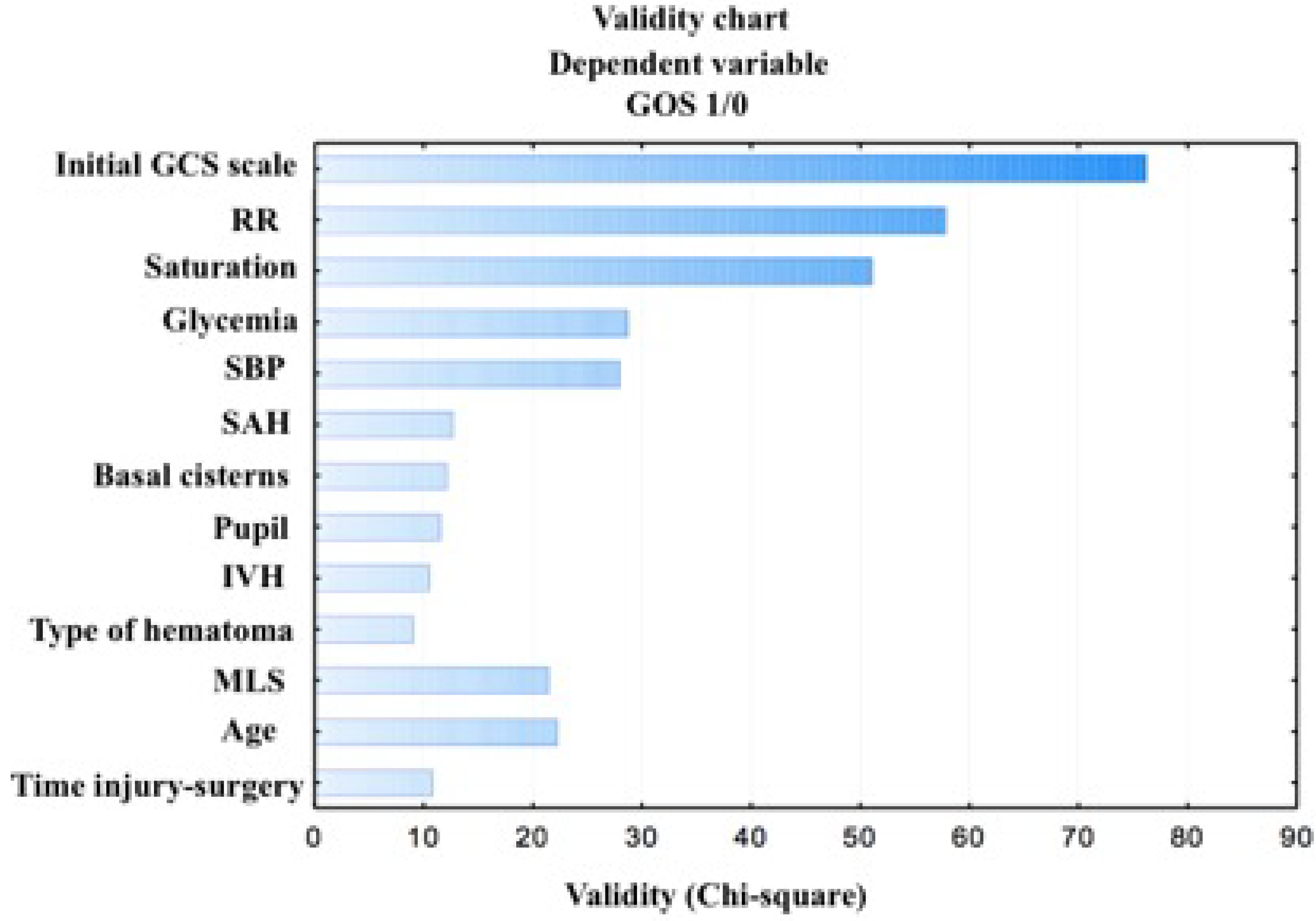
3.2. Logistic Regression Analysis (Multivariate Analysis)
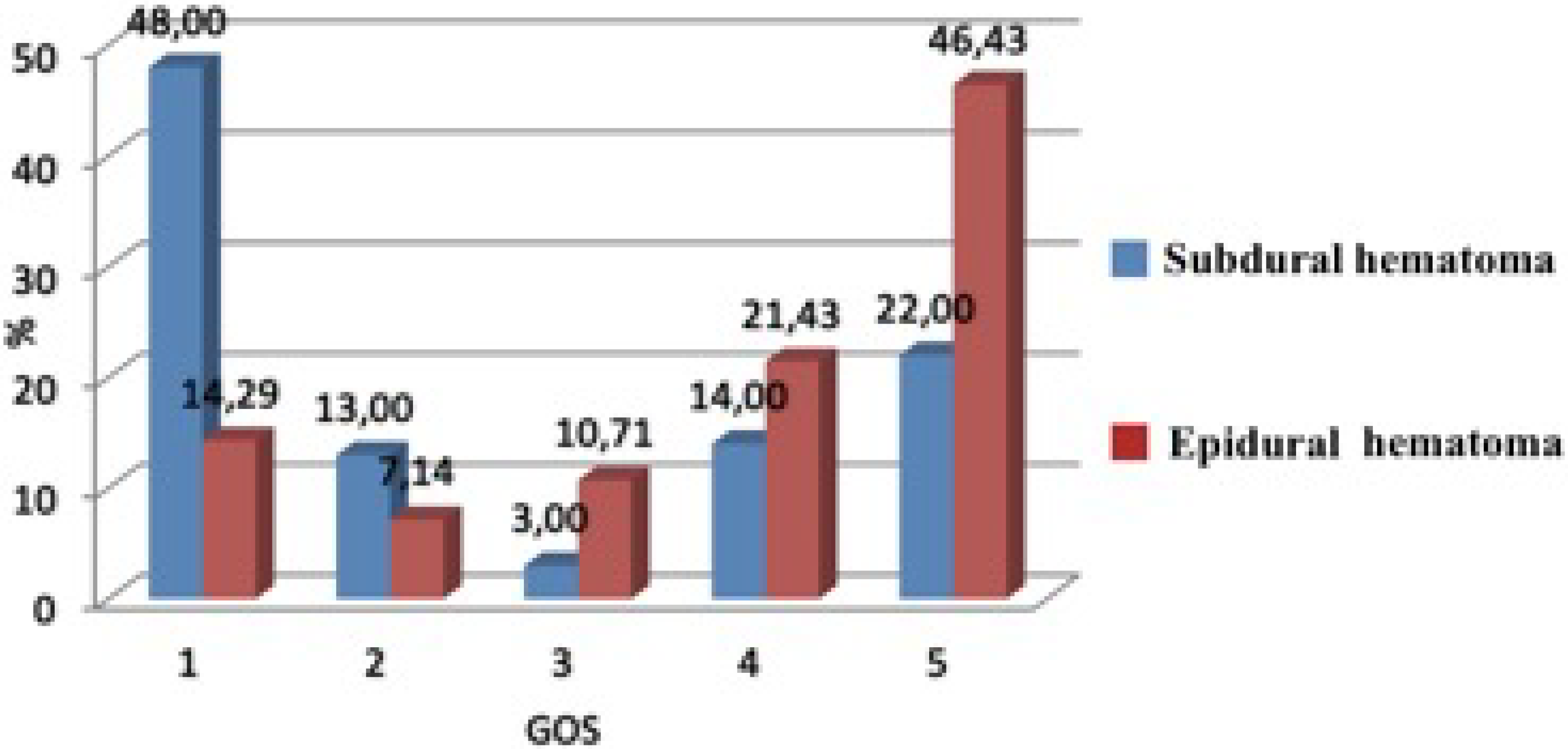
3.3. Six-Month Outcome (Univariate Analysis)
4. Discussion
4.1. Demographic Data
4.2. Physiological Factors
4.3. Laboratory Factors
4.4. Computer Tomography (CT) Scan Characteristics
4.5. Time Injury-Operation
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Krishna, G.; Beitchman, J.A.; Bromberg, C.E.; Currier Thomas, T. Approaches to Monitor Circuit Disruption after Traumatic Brain Injury: Frontiers in Preclinical Research. Int. J. Mol. Sci. 2020, 21, 588. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hukkelhoven, C.W.P.M.; Steyerberg, E.W.; Habbema, J.D.F.; Farace, E.; Marmarou, A.; Murray, G.D.; Marshall, L.F.; Mass, A.I.R. Predicting Outcome after Traumatic Brain Injury: Development and International Validation of Prognostic Scores Based on Admission Characteristics. J. Neurotrauma 2005, 22, 1025–1039. [Google Scholar] [CrossRef] [PubMed]
- Lingsma, H.F.; Roozenbeek, B.; Steyerberg, E.W.; Murray, G.D.; Maas, A.I. Early prognosis in traumatic brain injury: From prophecies to predictions. Lancet Neurol. 2010, 9, 543–554. [Google Scholar] [CrossRef]
- Murray, G.D.; Butcher, I.; McHugh, G.S.; Lu, J.; Mushkudiani, N.A.; Mass, A.I.R.; Marmarou, A.; Steyerberg, E.W. Multivariable prognostic analysis in traumatic brain injury: results from the IMPACT study. J. Neurotrauma 2007, 24, 329–337. [Google Scholar] [CrossRef] [PubMed]
- Collaborators, M.C.T.; Perel, P.; Arango, M.; Clayton, T.; Edwards, P.; Komolafe, E.; Poccock, S.; Roberts, I.; Shakur, H.; Steyerberg, E.; et al. Predicting outcome after traumatic brain injury: practical prognostic models based on large cohort of international patients. BMJ 2008, 336, 425–429. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mushkudiani, N.A.; Engel, D.C.; Steyerberg, E.W.; Butcher, I.; Lu, J.; Marmarou, A.; Slieker, F.; McHugh, G.S.; Murray, G.D.; Mass, A.I.R. Prognostic value of demographic characteristics in traumatic brain injury: Results from the IMPACT study. J. Neurotrauma 2007, 24, 259–269. [Google Scholar] [CrossRef]
- Taussky, P.; Widmer, H.R.; Takala, J.; Fandino, J. Outcome after acute traumatic subdural and epidural haematoma in Switzerland: a single-centre experience. Swiss Med. Wkly. 2008, 138, 281–285. [Google Scholar]
- Jeong, Y.H.; Oh, J.W.; Cho, S. Clinical Outcome of Acute Epidural Hematoma in Korea: Preliminary Report of 285 Cases Registered in the Korean Trauma Data Bank System. Korean J. Neurotrauma 2016, 12, 47–54. [Google Scholar] [CrossRef] [Green Version]
- Leitgeb, J.; Mauritz, W.; Brazinova, A.; Janciak, I.; Majdan, M.; Wilbacher, I.; Rusnak, M. Outcome after severe brain trauma due to acute subdural hematoma. J. Neurosurg. 2012, 117, 324–333. [Google Scholar] [CrossRef]
- Saadat, S.; Akbari, H.; Khorramirouz, R.; Mofid, R.; Rahimi-Movaghar, V. Determinants of mortality in patients with traumatic brain injury. Ulus. Travma. Acil. Cerrahi. Derg. 2012, 18, 219–224. [Google Scholar] [CrossRef] [Green Version]
- Khaled, C.N.; Raihan, M.Z.; Chowdhury, F.H. Surgical management of traumatic extradural hematoma: Experiences with 610 patients and prospective analysis. Ind. J. Neurotrauma 2008, 2, 75–79. [Google Scholar] [CrossRef]
- Ndoumbe, A.; Ekeme, M.P.; Jemea, B. Epidemiological Analysis of Surgically Treated Acute Traumatic Epidural Hematoma. Open J. Mod. Neurosurg. 2016, 6, 89–97. [Google Scholar] [CrossRef] [Green Version]
- Leitgeb, J.; Mauritz, W.; Brazinova, A.; Majdan, M.; Wilbacher, I. Outcome after severe brain trauma associated with epidural hematoma. ArchOrthop. Trauma. Surg. 2013, 133, 199–207. [Google Scholar] [CrossRef]
- Tian, H.L.; Chen, S.W.; Xu, T.; Hu, J.; Rong, B.Y.; Wang, G. Risk factors related to hospital mortality in patients with isolated traumatic acute subdural haematoma: Analysis of 308 patients undergone surgery. Chin. Med. J. (Engl.) 2008, 121, 1080–1084. [Google Scholar] [CrossRef]
- Gurer, B.; Kertmen, H.; Yilmaz, E.R.; Dolgun, H.; Hasturk, A.E.; Sekerci, Z. The Surgical Outcome of Traumatic Extraaxial Hematomas Causing Brain Herniation. Turk. Neurosurg. 2017, 27, 37–52. [Google Scholar] [CrossRef] [Green Version]
- Hamed, M.; Schuss, P.; Daher, F.H.; Borger, V.; Güresir, Á. Acute traumatic subdural hematoma: Surgical management in the presence of cerebral herniation—A singlecenter series and multivariate analysis. World Neurosurg. 2016, 94, 501–506. [Google Scholar] [CrossRef]
- McHugh, G.S.; Engel, D.C.; Butcher, I.; Steyerberg, E.W.; Lu, J.; Mushkudiani, N.; Hernandez, A.V.; Marmarou, A.; Maas, A.I.R.; Murray, G.D. Prognostic value of secondary insults in traumatic brain injury: Results from the IMPACT study. J. Neurotrauma 2007, 24, 287–293. [Google Scholar] [CrossRef]
- Honda, M.; Ichibayashi, R.; Yokomuro, H.; Yoshihara, K.; Masuda, H.; Haga, D.; Seiki, Y.; Kudoh, C.; Kishi, T. Early cerebral circulation disturbance in patients suffering from severe traumatic brain injury (TBI): A Xenon CT and perfusion CT study. Neurol. Med. Chir. 2016, 56, 501–509. [Google Scholar] [CrossRef] [Green Version]
- Okonkwo, D.O.; Shutter, L.A.; Moore, C.; Temkin, N.R.; Puccio, A.M.; Madden, C.J.; Andaluz, N.; Chesnut, R.M.; Bullock, M.R.; Grant, G.A.; et al. Brain tissue oxygen monitoring and management in severe traumatic brain injury phase-II: A phase II randomized trial. Crit. Care Med. 2017, 45, 1907–1914. [Google Scholar] [CrossRef]
- Petroni, G.; Quaglino, M.; Lujan, S.; Kovalevski, L.; Rondina, C.; Videtta, W. Early prognosis of severe traumatic brain injury in an urban argentinian trauma center. J. Trauma 2010, 68, 564–570. [Google Scholar] [CrossRef] [Green Version]
- Zuhroidah, I.; Dewi Nastiti, A.; Huda, N.; Rahmania, N. Correlation between respiratory frequency (rr) and outcome in head injury patients in emergency room of bangil hospital, pasuruan district. Nurse Health J. Keperawatan 2018, 7, 148–151. [Google Scholar]
- Chakraborty, S.; Skolnick, B.; Narayan, R.K. Neuroprotection trials in traumatic brain injury. Curr. Neurol. Neurosci. Rep. 2016, 16, 29. [Google Scholar] [CrossRef] [PubMed]
- Krishnamoorthy, V.; Chaikittisilpa, N.; Kiatchai, T.; Vavilala, M. Hypertension after severe traumatic brain injury: Friend or foe? J. Neurosurg. Anesth. 2017, 29, 382. [Google Scholar] [CrossRef]
- Kalayci, M.; Aktunç, E.; Gül, S. Decompressive craniectomy for acute subdural haematoma: An overview of current prognostic factors and a discussion about some novel prognostic parametres. J. Pak. Med. Assoc. 2013, 63, 34–49. [Google Scholar]
- Van Beek, J.G.; Mushkudiani, N.A.; Steyerberg, E.W.; Butcher, I.; Mchugh, G.S.; Lu, J.; Marmarou, A.; Murray, G.D.; Mass, A.I.R. Prognostic value of admission laboratory parameters in traumatic brain injury: Results from the IMPACT study. J. Neurotrauma 2007, 24, 315–328. [Google Scholar] [CrossRef]
- Cely, C.M.; Arora, P.; Quartin, A.A. Relationship of baseline glucose homeostasis to hyperglycemia during medical critical illness. Chest 2004, 126, 879–887. [Google Scholar] [CrossRef]
- Joseph, B.; Aziz, H.; Zangbar, B.; Kulvatunyou, N.; Pandit, V.; O’Keeffe, T.; Tang, A.; Wynne, J.; Randall, S.; Rhee, P. Acquired coagulopathy of traumatic brain injury defined by routine laboratory tests: Which laboratory values matter? J. Trauma Acute Care Surg. 2014, 76, 121–125. [Google Scholar] [CrossRef]
- Wafaisade, A.; Lefering, R.; Tjardes, T.; Wutzler, S.; Simanski, C.; Paffrath, T.; Fischer, P.; Bouillon, B.; Maegele, B.; Trauma Registry of DGU. Acute coagulopathy in isolated blunt traumatic brain injury. Neurocrit. Care 2010, 12, 211–219. [Google Scholar] [CrossRef]
- Rejeb, I.; Chakroun, O.; Chtara, K.; Meriam, B.; Hichem, K.; Adel, C.; Mabrouk, B.; Noureddine. Factors predicting early outcome in patients admitted at emergencydepartment with severe head trauma. J. Acute Dis. 2015, 4, 68–72. [Google Scholar]
- Gürkanlar, D.; Lakadamyali, H.; Ergun, T.; Yilmaz, C.; Yücel, E.; Altinörs, N. Predictive value of leucocytosis in head trauma. Turk. Neurosurg. 2009, 19, 211–215. [Google Scholar]
- Bernier, R.; Hillary, F. Trends in alcohol use during moderate and severe traumatic brain injury: 18 years of neurotrauma in Pennsylvania. Brain Inj. 2016, 30, 414–421. [Google Scholar] [CrossRef]
- Pandit, V.; Patel, N.; Rhee, P.; Kulvatunyou, N.; Aziz, H.; Green, D.J.; MbChB, T.O.; Zangbar, B.; Tang, A.; Gries, L.; et al. Effect of alcohol in traumatic brain injury: Is it really protective? J. Surg. Res. 2014, 190, 634–639. [Google Scholar] [CrossRef]
- Plurad, D.; Demetriades, D.; Gruzinski, G.; Preston, C.; Chan, L.; Gaspard, D.; Margulies, D.; Cryer, G. Motor vehicle crashes: the association of alcohol consumption with the type and severity of injuries and outcomes. J. Emerg. Med. 2010, 38, 12–17. [Google Scholar] [CrossRef]
- Maas, A.I.; Steyerberg, E.W.; Butcher, I.; Dammers, R.; Lu, J.; Marrmarou, A.; Mushkudiani, N.A.; McHugh, G.S.; Murray, G.D. Prognostic Value of Computerized Tomography Scan Characteristics in Traumatic Brain Injury: Results from the IMPACT Study. J. Neurotrauma 2007, 24, 303–314. [Google Scholar] [CrossRef]
- Hiler, M.; Czosnyka, M.; Hutchinson, P.; Balestreri, M.; Smielewski, P.; Matta, B. Predictive value of initial computerized tomography scan, intracranial pressure, and state of autoregulation in patients with traumatic brain injury. J. Neurosurg. 2006, 104, 731–737. [Google Scholar] [CrossRef]
- Yurt, I.; Bezircioglu, H.; Erşahin, Y. Extadural haematoma: Analysis of 190 cases. Turk. Neurosurg. 1996, 6, 63–67. [Google Scholar]
- Balik, V.; Lehto, H.; Hoza, D.; Phornsuwannapha, S.; Toninelli, S.; Romani, R.; Sulla, I.; Hernesniemi, J. Post-traumatic frontal and parieto-occipital extradural haematomas: A retrospective analysis of 41 patients and review of the literature. Cent. Eur. Neurosurg. 2011, 72, 169–175. [Google Scholar] [CrossRef]
- Munoz-Sánchez, M.A.; Murillo-Cabezas, F.; Cayuela-Domínguez, A.; Rincón-Ferrari, M.D.; Amaya-Villar, R.; León-Carrión, J. Skull fracture, with or without clinical signs, in mTBI is an independent risk marker for neurosurgically relevant intracranial lesion: A cohort study. Brain Inj. 2009, 23, 39–44. [Google Scholar] [CrossRef]
- Fabbri, A.; Servadei, F.; Marchesini, G.; Stein, S.C.; Vandelli, A. Early predictors of unfavourable outcome in subjects with moderate head injury in the emergency department. J. Neurol. Neurosurg. Psychiatry 2008, 79, 567–573. [Google Scholar] [CrossRef]
- Wood, R.L.; Eames, R. Application of behaviour modifi cation in the rehabilitation of traumatically brain-injured patients. In Applications of Conditioning Theory, 1st ed.; Routledge: New York, NY, USA, 1981; pp. 81–101. [Google Scholar]
- Servadei, F.; Nasi, M.T.; Giuliani, G.; Cremonini, A.M.; Cenni, P.; Zappi, D.; Taylor, S. CT prognostic factors in acute subdural haematomas: The value of the ‘worst’ CT scan. Br. J. Neurosurg. 2000, 14, 110–116. [Google Scholar] [CrossRef]
- Matsushima, K.; Inaba, K.; Siboni, S.; Skiada, D.; Strumwasser, A.M.; Magee, G.A.; Sung, G.Y.; Benjaminm, E.R.; Lam, L.; Demetriades, D. Emergent operation for isolated severe traumatic brain injury: Does time matter? J. Trauma Acute Care Surg. 2015, 79, 838–842. [Google Scholar] [CrossRef]
- Park, J.H.; Park, J.E.; Kim, S.H.; Lim, J.C.; You, N.K.; Ahn, Y.H. Outcomes of ultra-early decompressive craniectomy after severe traumatic brain injury-Treatment outcomes after severe TBI. Korean J. Neurotrauma 2014, 10, 112–118. [Google Scholar] [CrossRef]
- Seelig, J.M.; Becker, D.P.; Miller, J.D.; Greenberg, R.P.; Ward, J.D.; Choi, S.C. Traumatic acute subdural hematoma: major mortality reduction in comatose patients treated within four hours. N. Engl. J. Med. 1981, 304, 1511–1518. [Google Scholar] [CrossRef] [Green Version]
- Sergides, I.G.; Whiting, G.; Howarth, S.; Hutchinson, P.J. Is the recommended target of 4 hours from head injury to emergency craniotomy achievable? Br. J. Neurosurg. 2006, 20, 301–305. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Groups | |||||
|---|---|---|---|---|---|
| Demographic Data | ADH (n = 28) | SDH (n = 100) | |||
| Sex | N | % | N | % | |
| Famale | 2 | 7.14 | 14 | 14.00 | |
| Male | 26 | 92.86 | 86 | 86.00 | |
| Age | under 35 years | 10 | 35.71 | 14 | 14.00 |
| 36–60 years | 17 | 60.71 | 42 | 42.00 | |
| over 60 years | 1 | 3.57 | 44 | 44.00 | |
| Age | mean ± st.dev. | 38.82 | ±13.37 | 57.86 | ±18.26 |
| min–max | 14–69 | 18–93 | |||
| −95%CL | +95%CL | Chi2 Walda | Odd Ratio Unit | −95%CL | +95%CL | Rating | |
|---|---|---|---|---|---|---|---|
| Constant | −8.0112 | −0.7032 | 5.5722 | 0.0128 | 0.0003 | 0.4950 | −4.3572 |
| GCS | 0.3417 | 0.8976 | 19.4777 | 1.8583 | 1.4074 | 2.4537 | 0.6197 |
| Age | −0.1480 | −0.0256 | 7.8846 | 0.9169 | 0.8625 | 0.9747 | −0.0868 |
| SBP | 0.2635 | 2.4249 | 6.0629 | 3.8352 | 1.3015 | 11.3012 | 1.3442 |
| MLS | −0.2558 | −0.0324 | 6.5220 | 0.8658 | 0.7743 | 0.9681 | −0.1441 |
| Factors | Chi2 | p |
|---|---|---|
| Initial GCS scale | 76,044 | 0.000000 |
| RR | 57,863 | 0.000000 |
| Saturation | 51,060 | 0.000000 |
| Glycaemia | 28,605 | 0.000000 |
| SBP | 27,953 | 0.000000 |
| SAH | 12,665 | 0.0004 |
| State of basal cisterns | 12,069 | 0.0005 |
| Pupil reactive | 11,509 | 0.0007 |
| IVH | 10,514 | 0.001 |
| Type of hematoma | 9059 | 0.003 |
| MLS | 21,398 | 0.003 |
| Age | 22,231 | 0.008 |
| Time to surgery | 10,783 | 0.03 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kulesza, B.; Litak, J.; Grochowski, C.; Nogalski, A.; Rola, R. The Initial Factors with Strong Predictive Value in Relation to Six-Month Outcome among Patients Operated due to Extra-Axial Hematomas. Diagnostics 2020, 10, 174. https://doi.org/10.3390/diagnostics10030174
Kulesza B, Litak J, Grochowski C, Nogalski A, Rola R. The Initial Factors with Strong Predictive Value in Relation to Six-Month Outcome among Patients Operated due to Extra-Axial Hematomas. Diagnostics. 2020; 10(3):174. https://doi.org/10.3390/diagnostics10030174
Chicago/Turabian StyleKulesza, Bartłomiej, Jakub Litak, Cezary Grochowski, Adam Nogalski, and Radosław Rola. 2020. "The Initial Factors with Strong Predictive Value in Relation to Six-Month Outcome among Patients Operated due to Extra-Axial Hematomas" Diagnostics 10, no. 3: 174. https://doi.org/10.3390/diagnostics10030174