Dual-Energy Computed Tomography of the Lung in COVID-19 Patients: Mismatch of Perfusion Defects and Pulmonary Opacities


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. DECT Imaging Acquisition Parameters
2.3. DECT Imaging Analysis
2.4. Automatic Analysis of Lung Opacities
2.5. Statistical Analysis
3. Results
3.1. Characteristics of the Study Group
3.2. Image Quality Assessment
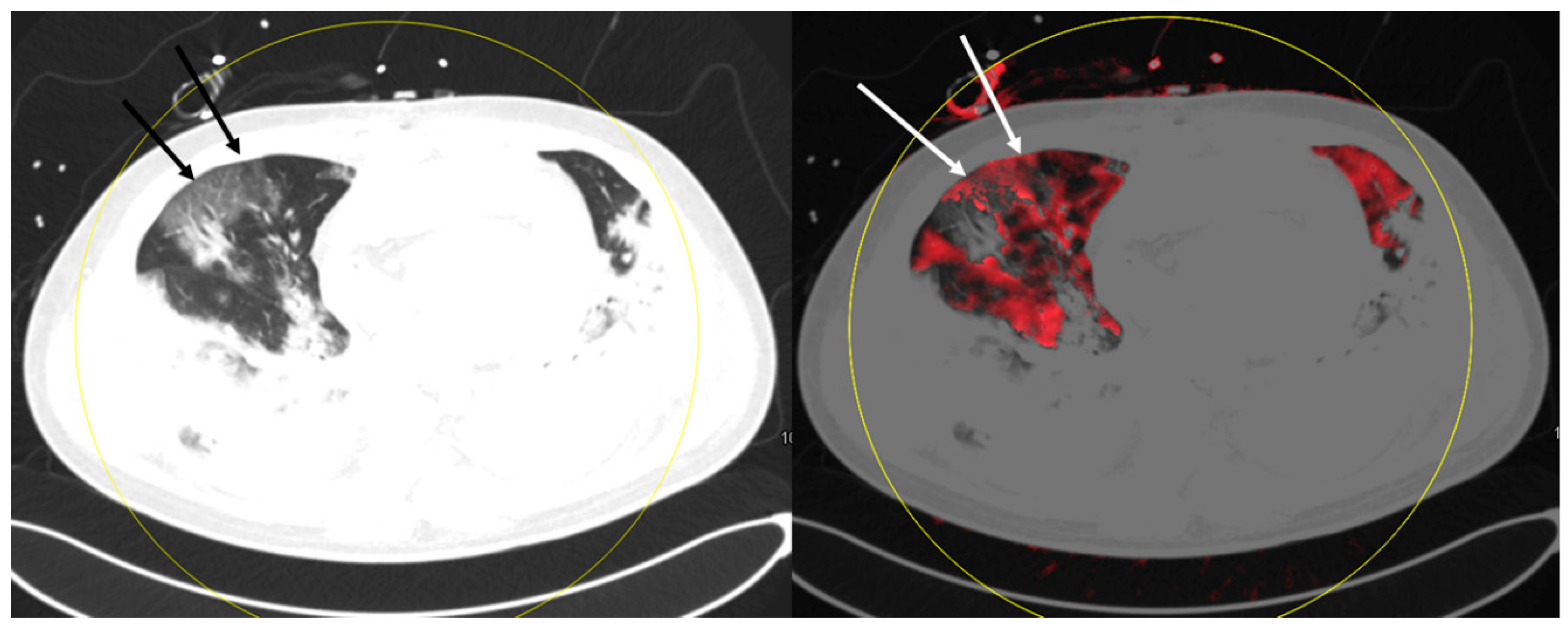
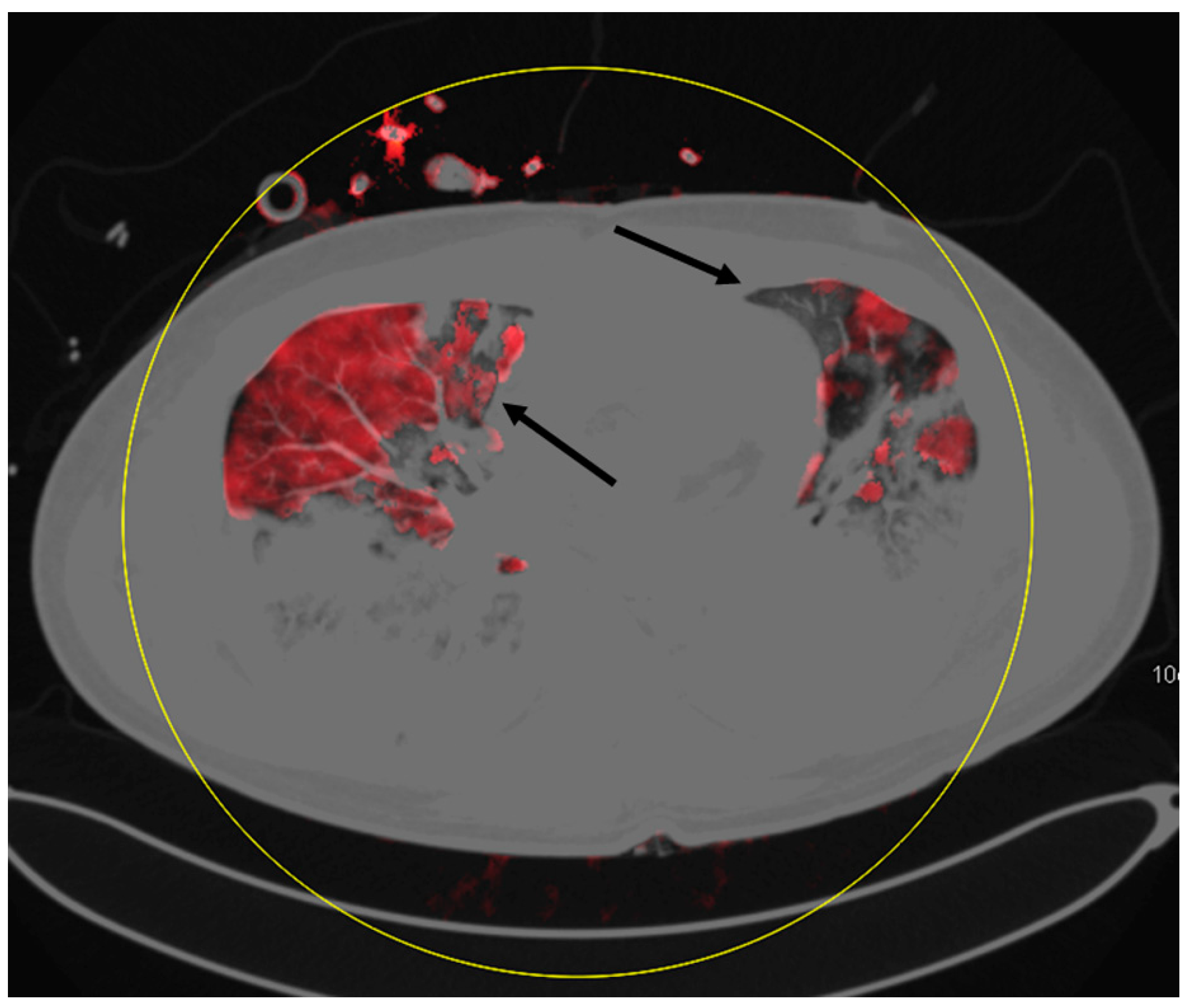
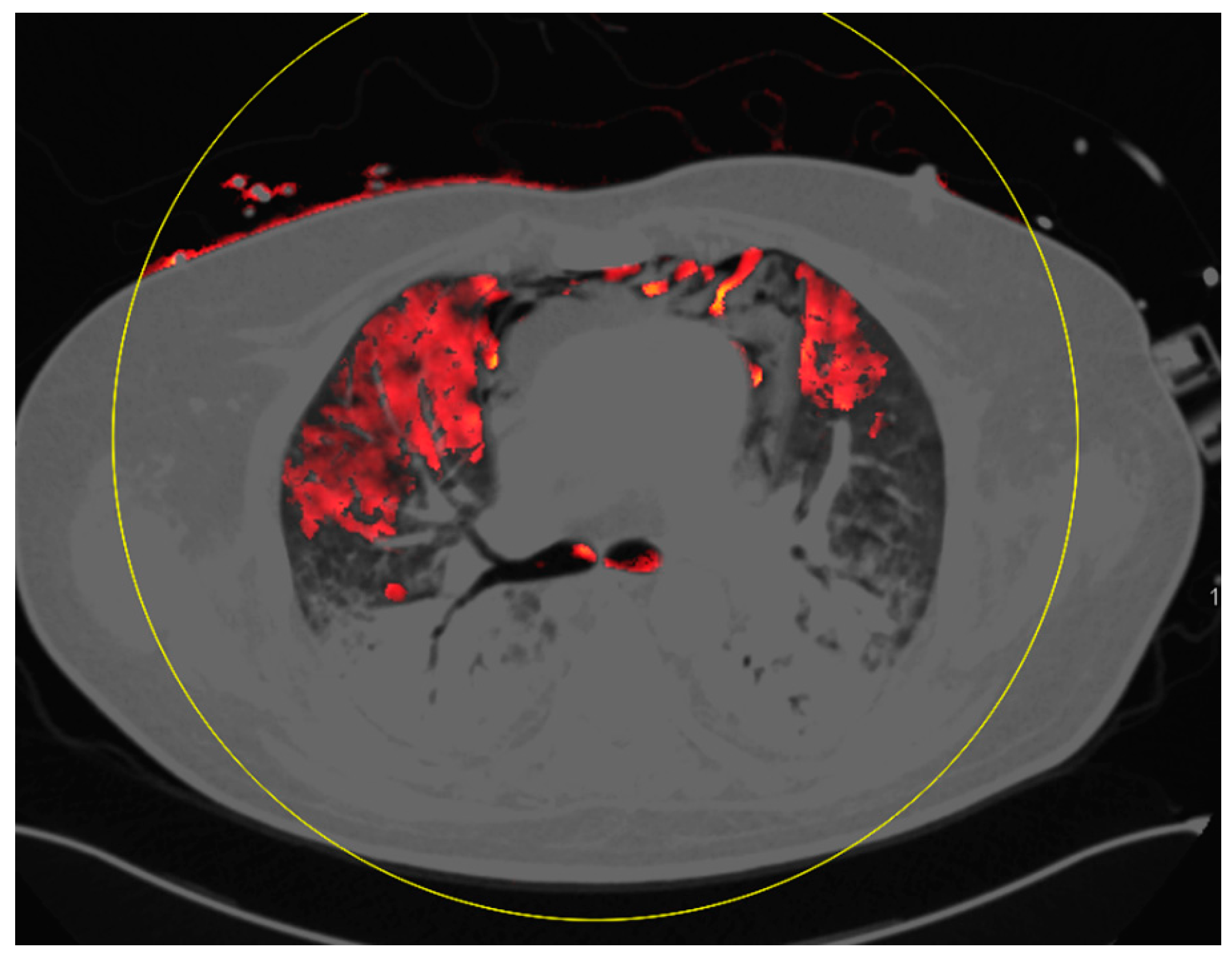
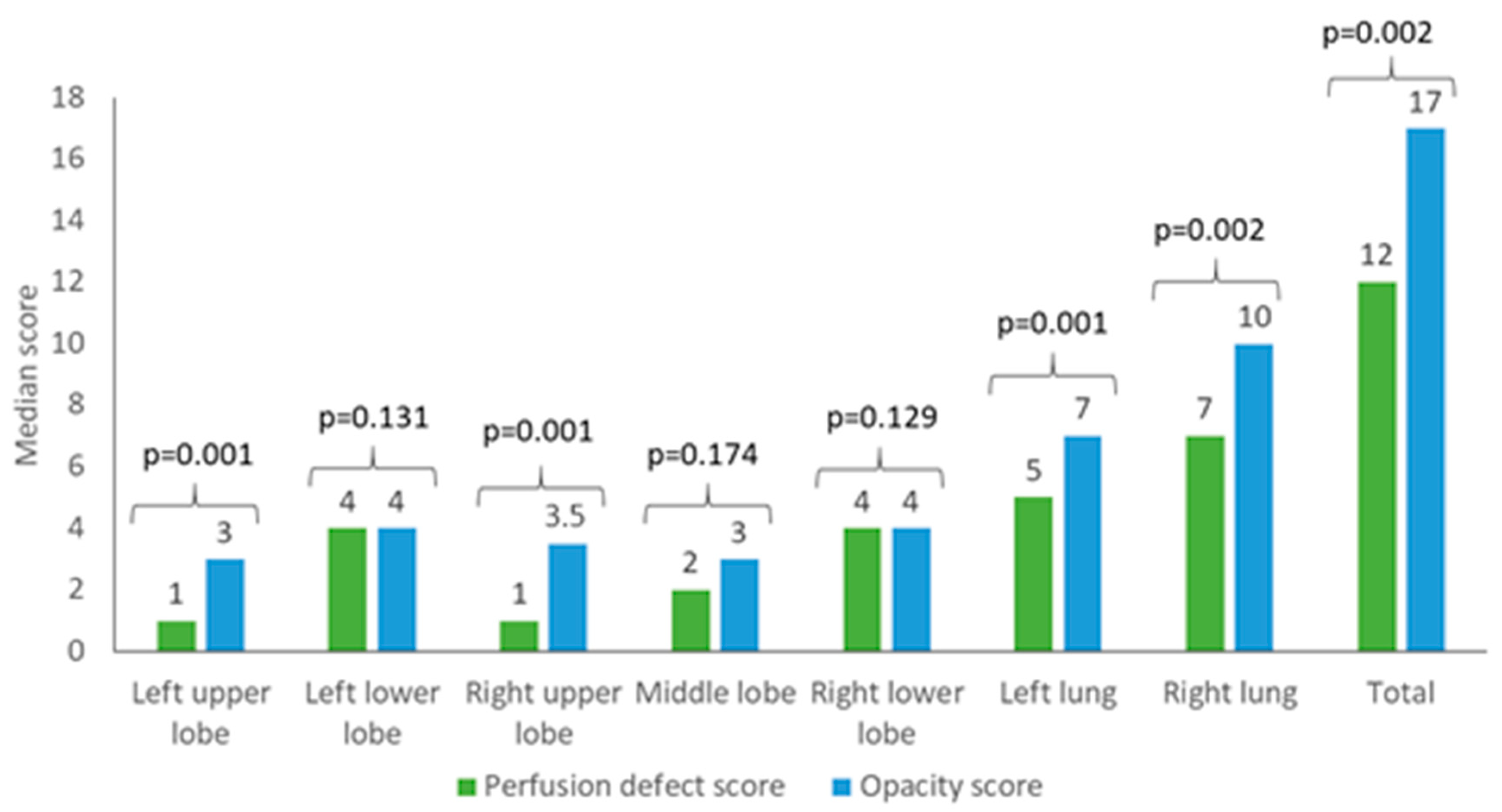
3.3. Perfusion Defects and Automatic Opacity Score Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- Zhu, N.; Zhang, D.; Wang, W.; Li, X.; Yang, B.; Song, J.; Zhao, X.; Huang, B.; Shi, W.; Lu, R.; et al. A Novel Coronavirus from Patients with Pneumonia in China, 2019. N. Engl. J. Med. 2020, 382, 727–733. [Google Scholar] [CrossRef] [PubMed]
- Mahase, E. China coronavirus: WHO declares international emergency as death toll exceeds 200. BMJ 2020, 368, m408. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van Kasteren, P.B.; van der Veer, B.; van den Brink, S.; Wijsman, L.; de Jonge, J.; van den Brandt, A.; Molenkamp, R.; Reusken, C.; Meijer, A. Comparison of seven commercial RT-PCR diagnostic kits for COVID-19. J. Clin. Virol. 2020, 128, 104412. [Google Scholar] [CrossRef]
- Li, Y.; Xia, L. Coronavirus Disease 2019 (COVID-19): Role of Chest CT in Diagnosis and Management. AJR Am. J. Roentgenol. 2020, 214, 1280–1286. [Google Scholar] [CrossRef]
- Xiong, Y.; Sun, D.; Liu, Y.; Fan, Y.; Zhao, L.; Li, X.; Zhu, W. Clinical and High-Resolution CT Features of the COVID-19 Infection: Comparison of the Initial and Follow-up Changes. Investig. Radiol. 2020, 55, 332–339. [Google Scholar] [CrossRef]
- Bernheim, A.; Mei, X.; Huang, M.; Yang, Y.; Fayad, Z.A.; Zhang, N.; Diao, K.; Lin, B.; Zhu, X.; Li, K.; et al. Chest CT Findings in Coronavirus Disease-19 (COVID-19): Relationship to Duration of Infection. Radiology 2020, 295, 200463. [Google Scholar] [CrossRef] [Green Version]
- Wu, J.; Wu, X.; Zeng, W.; Guo, D.; Fang, Z.; Chen, L.; Huang, H.; Li, C. Chest CT Findings in Patients With Coronavirus Disease 2019 and Its Relationship With Clinical Features. Investig. Radiol. 2020, 55, 257–261. [Google Scholar] [CrossRef]
- Pan, F.; Ye, T.; Sun, P.; Gui, S.; Liang, B.; Li, L.; Zheng, D.; Wang, J.; Hesketh, R.L.; Yang, L.; et al. Time Course of Lung Changes at Chest CT during Recovery from Coronavirus Disease 2019 (COVID-19). Radiology 2020, 295, 715–721. [Google Scholar] [CrossRef] [Green Version]
- Chung, M.; Bernheim, A.; Mei, X.; Zhang, N.; Huang, M.; Zeng, X.; Cui, J.; Xu, W.; Yang, Y.; Fayad, Z.A.; et al. CT Imaging Features of 2019 Novel Coronavirus (2019-nCoV). Radiology 2020, 295, 202–207. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, K.; Wu, J.; Wu, F.; Guo, D.; Chen, L.; Fang, Z.; Li, C. The Clinical and Chest CT Features Associated With Severe and Critical COVID-19 Pneumonia. Investig. Radiol. 2020, 55, 327–331. [Google Scholar] [CrossRef] [PubMed]
- Ye, Z.; Zhang, Y.; Wang, Y.; Huang, Z.; Song, B. Chest CT manifestations of new coronavirus disease 2019 (COVID-19): A pictorial review. Eur. Radiol. 2020, 30, 4381–4389. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Song, F.; Shi, N.; Shan, F.; Zhang, Z.; Shen, J.; Lu, H.; Ling, Y.; Jiang, Y.; Shi, Y. Emerging 2019 Novel Coronavirus (2019-nCoV) Pneumonia. Radiology 2020, 295, 210–217. [Google Scholar] [CrossRef] [Green Version]
- Guan, W.J.; Ni, Z.Y.; Hu, Y.; Liang, W.H.; Ou, C.Q.; He, J.X.; Liu, L.; Shan, H.; Lei, C.L.; Hui, D.S.C.; et al. Clinical Characteristics of Coronavirus Disease 2019 in China. N. Engl. J. Med. 2020, 382, 1708–1720. [Google Scholar] [CrossRef] [PubMed]
- Ai, T.; Yang, Z.; Hou, H.; Zhan, C.; Chen, C.; Lv, W.; Tao, Q.; Sun, Z.; Xia, L. Correlation of Chest CT and RT-PCR Testing for Coronavirus Disease 2019 (COVID-19) in China: A Report of 1014 Cases. Radiology 2020, 296, E32–E40. [Google Scholar] [CrossRef] [Green Version]
- Cui, S.; Chen, S.; Li, X.; Liu, S.; Wang, F. Prevalence of venous thromboembolism in patients with severe novel coronavirus pneumonia. J. Thromb. Haemost. 2020, 18, 1421–1424. [Google Scholar] [CrossRef]
- Ackermann, M.; Verleden, S.E.; Kuehnel, M.; Haverich, A.; Welte, T.; Laenger, F.; Vanstapel, A.; Werlein, C.; Stark, H.; Tzankov, A.; et al. Pulmonary Vascular Endothelialitis, Thrombosis, and Angiogenesis in Covid-19. N. Engl. J. Med. 2020, 383, 120–128. [Google Scholar] [CrossRef]
- Calabrese, F.; Pezzuto, F.; Fortarezza, F.; Hofman, P.; Kern, I.; Panizo, A.; von der Thüsen, J.; Timofeev, S.; Gorkiewicz, G.; Lunardi, F. Pulmonary pathology and COVID-19: Lessons from autopsy. The experience of European Pulmonary Pathologists. Virchows Arch. 2020, 477, 359–372. [Google Scholar] [CrossRef]
- Gervaise, A.; Bouzad, C.; Peroux, E.; Helissey, C. Acute pulmonary embolism in non-hospitalized COVID-19 patients referred to CTPA by emergency department. Eur. Radiol. 2020. [Google Scholar] [CrossRef]
- Oudkerk, M.; Buller, H.R.; Kuijpers, D.; van Es, N.; Oudkerk, S.F.; McLoud, T.C.; Gommers, D.; van Dissel, J.; Ten Cate, H.; van Beek, E.J. Diagnosis, Prevention, and Treatment of Thromboembolic Complications in COVID-19: Report of the National Institute for Public Health of the Netherlands. Radiology 2020, 201629. [Google Scholar] [CrossRef]
- Cellina, M.; Oliva, G. Acute pulmonary embolism in a patient with COVID-19 pneumonia. Diagn. Interv. Imaging 2020, 101, 325–326. [Google Scholar] [CrossRef] [PubMed]
- Roncon, L.; Zuin, M.; Barco, S.; Valerio, L.; Zuliani, G.; Zonzin, P.; Konstantinides, S.V. Incidence of acute pulmonary embolism in COVID-19 patients: Systematic review and meta-analysis. Eur. J. Intern. Med. 2020. [Google Scholar] [CrossRef] [PubMed]
- Lu, G.M.; Zhao, Y.; Zhang, L.J.; Schoepf, U.J. Dual-energy CT of the lung. AJR Am. J. Roentgenol. 2012, 199, S40–S53. [Google Scholar] [CrossRef] [PubMed]
- Masy, M.; Giordano, J.; Petyt, G.; Hossein-Foucher, C.; Duhamel, A.; Kyheng, M.; De Groote, P.; Fertin, M.; Lamblin, N.; Bervar, J.F.; et al. Dual-energy CT (DECT) lung perfusion in pulmonary hypertension: Concordance rate with V/Q scintigraphy in diagnosing chronic thromboembolic pulmonary hypertension (CTEPH). Eur. Radiol. 2018, 28, 5100–5110. [Google Scholar] [CrossRef]
- Nance, J.W., Jr.; Henzler, T.; Meyer, M.; Apfaltrer, P.; Braunagel, M.; Krissak, R.; Schoepf, U.J.; Schoenberg, S.O.; Fink, C. Optimization of contrast material delivery for dual-energy computed tomography pulmonary angiography in patients with suspected pulmonary embolism. Investig. Radiol. 2012, 47, 78–84. [Google Scholar] [CrossRef]
- Zhang, L.J.; Zhou, C.S.; Schoepf, U.J.; Sheng, H.X.; Wu, S.Y.; Krazinski, A.W.; Silverman, J.R.; Meinel, F.G.; Zhao, Y.E.; Zhang, Z.J.; et al. Dual-energy CT lung ventilation/perfusion imaging for diagnosing pulmonary embolism. Eur. Radiol. 2013, 23, 2666–2675. [Google Scholar] [CrossRef]
- Wu, H.W.; Cheng, J.J.; Li, J.Y.; Yin, Y.; Hua, J.; Xu, J.R. Pulmonary embolism detection and characterization through quantitative iodine-based material decomposition images with spectral computed tomography imaging. Investig. Radiol. 2012, 47, 85–91. [Google Scholar] [CrossRef]
- Krissak, R.; Henzler, T.; Reichert, M.; Krauss, B.; Schoenberg, S.O.; Fink, C. Enhanced visualization of lung vessels for diagnosis of pulmonary embolism using dual energy CT angiography. Investig. Radiol. 2010, 45, 341–346. [Google Scholar] [CrossRef]
- Lang, M.; Som, A.; Carey, D.; Reid, N.; Mendoza, D.P.; Flores, E.J.; Li, M.D.; Shepard, J.-A.O.; Little, B.P. Pulmonary Vascular Manifestations of COVID-19 Pneumonia. Radiol. Cardiothorac. Imaging 2020, 2, e200277. [Google Scholar] [CrossRef]
- Lang, M.; Som, A.; Mendoza, D.P.; Flores, E.J.; Reid, N.; Carey, D.; Li, M.D.; Witkin, A.; Rodriguez-Lopez, J.M.; Shepard, J.O.; et al. Hypoxaemia related to COVID-19: Vascular and perfusion abnormalities on dual-energy CT. Lancet Infect. Dis. 2020. [Google Scholar] [CrossRef]
- Grillet, F.; Behr, J.; Calame, P.; Aubry, S.; Delabrousse, E. Acute Pulmonary Embolism Associated with COVID-19 Pneumonia Detected with Pulmonary CT Angiography. Radiology 2020, 296, E186–E188. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pelosi, P.; de Abreu, M.G. Acute respiratory distress syndrome: We can’t miss regional lung perfusion! BMC Anesthesiol. 2015, 15, 35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mondal, R.; Lahiri, D.; Deb, S.; Bandyopadhyay, D.; Shome, G.; Sarkar, S.; Paria, S.R.; Thakurta, T.G.; Singla, P.; Biswas, S.C. COVID-19: Are we dealing with a multisystem vasculopathy in disguise of a viral infection? J. Thromb. Thrombolysis 2020. [Google Scholar] [CrossRef] [PubMed]
- Zhang, W.; Zhao, Y.; Zhang, F.; Wang, Q.; Li, T.; Liu, Z.; Wang, J.; Qin, Y.; Zhang, X.; Yan, X.; et al. The use of anti-inflammatory drugs in the treatment of people with severe coronavirus disease 2019 (COVID-19): The Perspectives of clinical immunologists from China. Clin. Immunol. 2020, 214, 108393. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Values |
|---|---|
| Opacity score | 1: ≤25% lung opacity |
| 2: 26–50% lung opacity | |
| 3: 51–75% lung opacity | |
| 4: ≥75% lung opacity | |
| Perfusion defect score | 1: ≤25% lung perfusion defect |
| 2: 26–50% lung perfusion defect | |
| 3: 51–75% lung perfusion defect | |
| 4: >75% lung perfusion defect |
| Characteristics | Values |
|---|---|
| Examinations | n = 24 |
| Patients | n =14 (male: n = 11) |
| Invasive ventilation | n = 20 |
| Mean age ± std | 55 ± 16 years |
| Range | 32–80 years |
| Median time RT-PCR—DECT | 8 days (3–16 days) |
| Median time between first CT and follow-up | 13 days (9–18 days) |
| Indications for imaging | |
| Clinical deterioration and search for inflammatory origin | n = 15 |
| Suspicion of bleeding | n = 4 |
| Follow-up of pulmonary status | n = 2 |
| Suspicion of cervical thrombosis | n = 1 |
| Trauma | n = 1 |
| Staging | n = 1 |
| Characteristics | Values |
|---|---|
| Main pulmonary findings | |
| Ground glass opacity | n = 24 |
| Consolidation | n = 22 |
| Mosaic perfusion pattern | n = 19 |
| Pleural effusion | n = 17 |
| Fibrotic streaks | n = 3 |
| Bronchiectasis | n = 2 |
| Pneumothorax | n = 1 |
| Mediastinal lymphadenopathy | n = 1 |
| Secondary non-pulmonary findings | |
| Thrombosis of jugular veins | n = 5 |
| Thoracic bleeding | n = 1 |
| Aortic aneurysm | n = 1 |
| Lung volume | |
| Left upper lobe | 829 ± 384 mL |
| Left lower lobe | 473 ± 310 mL |
| Right upper lobe | 662 ± 304 mL |
| Middle lobe | 324 ± 178 mL |
| Right lower lobe | 700 ± 253 mL |
| Left lung | 1302 ± 588 mL |
| Right lung | 1685 ± 615 mL |
| Total | 2988 ± 1178 ml |
| Characteristics | Reader 1 | Reader 2 |
|---|---|---|
| Artifacts | 4 (IQR 4–4) | 4 (IQR 4–4) |
| Sharpness of lung veseels | 4 (IQR 3–4) | 4 (IQR 3–4) |
| Overall image qualtiy | 4 (IQR 4–4) | 4 (IQR 4–4) |
| Perfusion Defects Reader 1 | Automatic Opacity Score | p-Value | |
|---|---|---|---|
| Reader 2 | |||
| Left upper lobe | 1 (IQR 1–4) | 3 (IQR 2–4) | 0.001 |
| 1 (IQR 1–4) | 0.001 | ||
| Left lower lobe | 4 (IQR 3–4) | 4 (IQR 4–4) | 0.131 |
| 4 (IQR 3–4) | 0.197 | ||
| Right upper lobe | 1 (IQR 1–3) | 3.5 (IQR 3–4) | 0.001 |
| 1 (IQR 1–3) | 0.001 | ||
| Middle lobe | 2 (IQR 1–3) | 3 (IQR 1–4) | 0.174 |
| 2 (IQR 1–3) | 0.174 | ||
| Right lower lobe | 4 (IQR 3–4) | 4 (IQR 4–4) | 0.129 |
| 4 (IQR 2.5–4) | 0.131 | ||
| Left lung | 5 (IQR 4–8) | 7 (IQR 6–8) | 0.001 |
| 5 (IQR 4–8) | 0.001 | ||
| Right lung | 7 (IQR 5–11) | 10 (IQR 8–11) | 0.002 |
| 7 (IQR 5–11) | 0.001 | ||
| Total | 12 (IQR 9–18) | 17 (IQR 15–19) | 0.002 |
| 12.5 (IQR 9–18) | 0.002 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Afat, S.; Othman, A.E.; Nikolaou, K.; Gassenmaier, S. Dual-Energy Computed Tomography of the Lung in COVID-19 Patients: Mismatch of Perfusion Defects and Pulmonary Opacities. Diagnostics 2020, 10, 870. https://doi.org/10.3390/diagnostics10110870
Afat S, Othman AE, Nikolaou K, Gassenmaier S. Dual-Energy Computed Tomography of the Lung in COVID-19 Patients: Mismatch of Perfusion Defects and Pulmonary Opacities. Diagnostics. 2020; 10(11):870. https://doi.org/10.3390/diagnostics10110870
Chicago/Turabian StyleAfat, Saif, Ahmed E. Othman, Konstantin Nikolaou, and Sebastian Gassenmaier. 2020. "Dual-Energy Computed Tomography of the Lung in COVID-19 Patients: Mismatch of Perfusion Defects and Pulmonary Opacities" Diagnostics 10, no. 11: 870. https://doi.org/10.3390/diagnostics10110870