
Subclinical Myocardial Dysfunction in Patients with Persistent Dyspnea One Year after COVID-19

 , , , , , and
, , , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. TTE
2.2. Speckle Tracking Echocardiography (STE)
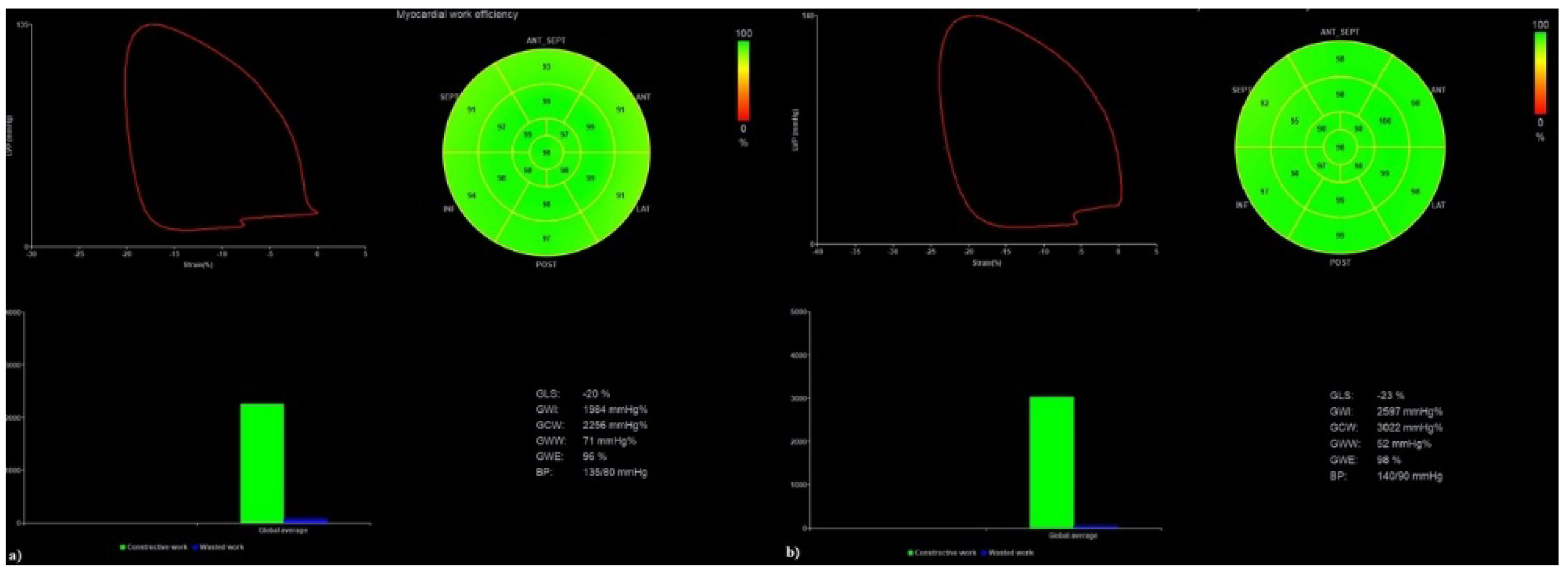
2.3. Myocardial Work (MW)
2.4. Statistical Analysis
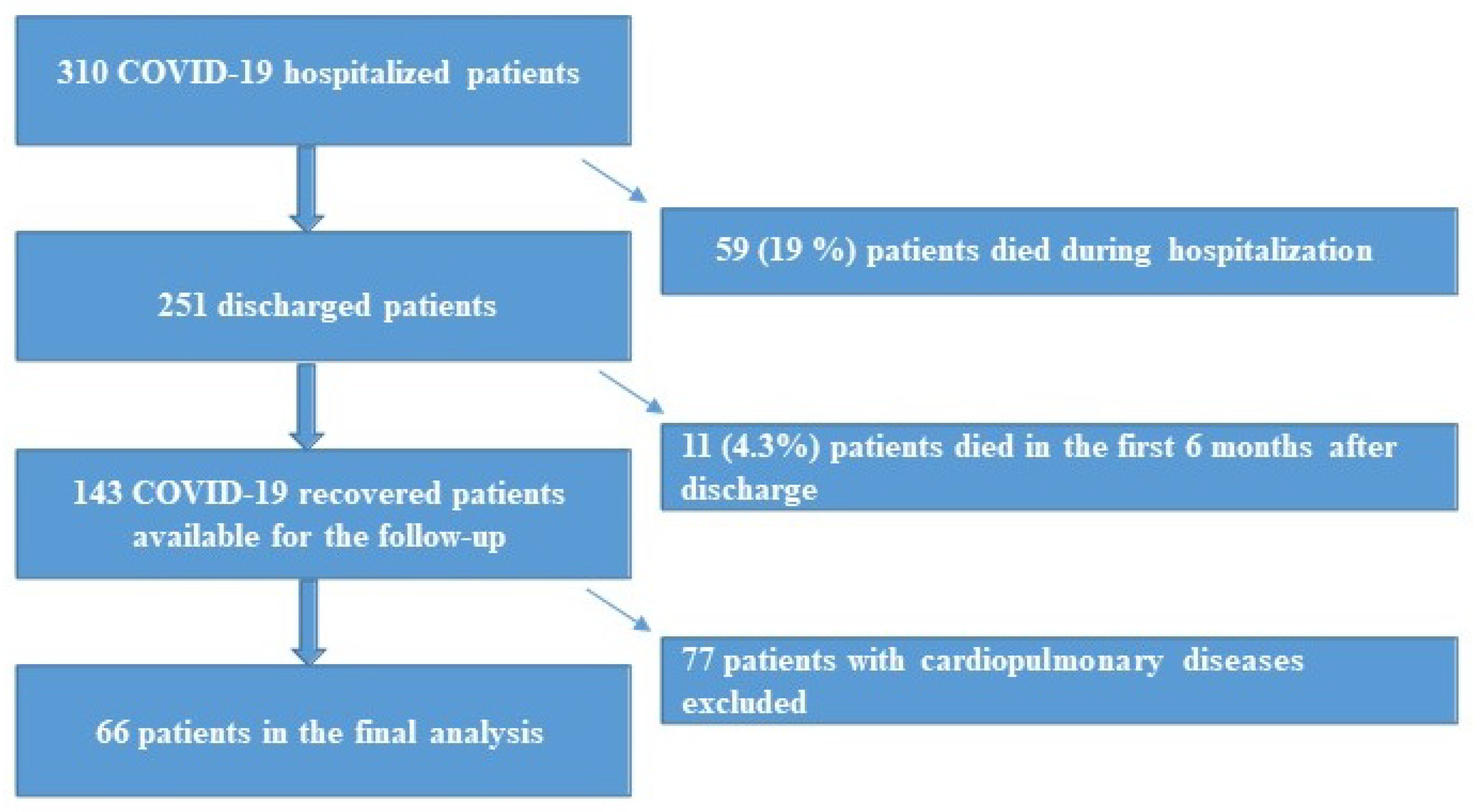
3. Results
Predictors of Persistent Dyspnea
4. Discussion
Study Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Nishiga, M.; Wang, D.W.; Han, Y.; Lewis, D.B.; Wu, J.C. COVID-19 and cardiovascular disease: From basic mechanisms to clinical perspectives. Nat. Rev. Cardiol. 2020, 17, 543–558. [Google Scholar] [CrossRef] [PubMed]
- Xu, H.; Hou, K.; Xu, R.; Li, Z.; Fu, H.; Wen, L.; Xie, L.; Liu, H.; Selvanayagam, J.B.; Zhang, N.; et al. Clinical Characteristics and Risk Factors of Cardiac Involvement in COVID-19. J. Am. Heart Assoc. 2020, 9, e016807. [Google Scholar] [CrossRef] [PubMed]
- WHO. COVID-19 Weekly Epidemiological Update; World Health Organization: Geneva, Switzerland, 2021; pp. 1–23.
- Pesaresi, M.; Pirani, F.; Tagliabracci, A.; Valsecchi, M.; Procopio, A.D.; Busardò, F.P.; Graciotti, L. SARS-CoV-2 identification in lungs, heart and kidney specimens by transmission and scanning electron microscopy. Eur. Rev. Med Pharmacol. Sci. 2020, 24, 5186–5188. [Google Scholar] [PubMed]
- Núñez-Gil, I.J.J.; Fernández-Ortiz, A.; Eid, C.M.; Huang, J.; Romero, R.; Becerra-Muñoz, V.M.; Uribarri, A.; Feltes, G.; Trabatoni, D.; Fernandez-Rozas, I.; et al. Underlying heart diseases and acute COVID-19 outcomes. Cardiol. J. 2021, 28, 202–214. [Google Scholar] [CrossRef]
- He, X.W.; Lai, J.S.; Cheng, J.; Wang, M.W.; Liu, Y.J.; Xiao, Z.C.; Xu, C.; Li, S.S.; Zeng, H.S. Impact of complicated myocardial injury on the clinical outcome of severe or critically ill COVID-19 patients. Zhonghua Xin Xue Guan Bing Za Zhi 2020, 48, E011. [Google Scholar]
- Grant, M.C.; Geoghegan, L.; Arbyn, M.; Mohammed, Z.; McGuinness, L.; Clarke, E.L.; Wade, R.G. The prevalence of symptoms in 24,410 adults infected by the novel coronavirus (SARS-CoV-2; COVID-19): A systematic review and meta-analysis of 148 studies from 9 countries. PLoS ONE 2020, 15, e0234765. [Google Scholar] [CrossRef]
- Li, X.; Guan, B.; Su, T.; Liu, W.; Chen, M.; Waleed, K.B.; Guan, X.; Gary, T.; Zhu, Z. Impact of cardiovascular disease and cardiac injury on in-hospital mortality in patients with COVID-19: A systematic review and meta-analysis. Heart 2020, 106, 1142–1147. [Google Scholar] [CrossRef]
- Hamming, I.; Timens, W.; Bulthuis, M.L.C.; Lely, A.T.; Navis, G.J.; van Goor, H. Tissue distribution of ACE2 protein, the functional receptor for SARS coronavirus. A first step in understanding SARS pathogenesis. J. Pathol. 2004, 203, 631–637. [Google Scholar] [CrossRef] [PubMed]
- Siripanthong, B.; Nazarian, S.; Muser, D.; Deo, R.; Santangeli, P.; Khanji, M.Y.; Cooper, L.T.; Chahal, C.A.A. Recognizing COVID-19–related myocarditis: The possible pathophysiology and proposed guideline for diagnosis and management. Heart Rhythm. 2020, 17, 1463–1471. [Google Scholar] [CrossRef] [PubMed]
- Lala, A.; Johnson, K.W.; Januzzi, J.L.; Russak, A.J.; Paranjpe, I.; Richter, F.; Zhao, S.; Somani, S.; Van Vleck, T.; Vaid, A.; et al. Prevalence and Impact of Myocardial Injury in Patients Hospitalized With COVID-19 Infection. J. Am. Coll. Cardiol. 2020, 76, 533–546. [Google Scholar] [CrossRef]
- Deng, Q.; Hu, B.; Zhang, Y.; Wang, H.; Zhou, X.; Hu, W.; Cheng, Y.; Yan, J.; Ping, H.; Zhou, Q. Suspected myocardial injury in patients with COVID-19: Evidence from front-line clinical observation in Wuhan, China. Int. J. Cardiol. 2020, 311, 116–121. [Google Scholar] [CrossRef] [PubMed]
- Messina, A.; Sanfilippo, F.; Milani, A.; Calabrò, L.; Negri, K.; García, M.I.M.; Astuto, M.; Vieillard-Baron, A.; Cecconi, M. COVID-19-related echocardiographic patterns of cardiovascular dysfunction in critically ill patients: A systematic review of the current literature. J. Crit. Care 2021, 65, 26–35. [Google Scholar] [CrossRef]
- Barman, H.A.; Atici, A.; Tekin, E.A.; Baycan, O.F.; Alici, G.; Meric, B.K.; Sit, O.; Genc, O.; Er, F.; Gungor, B.; et al. Echocardiographic features of patients with COVID-19 infection: A cross-sectional study. Int. J. Cardiovasc. Imag. 2021, 37, 825–834. [Google Scholar] [CrossRef] [PubMed]
- Mahmoud-Elsayed, H.M.; Moody, W.E.; Bradlow, W.M.; Khan-Kheil, A.M.; Hudsmith, L.E.; Steeds, R.P. Echocardiographic Findings in Covid-19 Pneumonia. Can. J. Cardiol. 2020, 36, 1203–1207. [Google Scholar] [CrossRef]
- Varghese, J.; Sandmann, S.; Ochs, K.; Schrempf, I.-M.; Frömmel, C.; Dugas, M.; Schmidt, H.H.; Vollenberg, R.; Tepasse, P.-R. Persistent symptoms and lab abnormalities in patients who recovered from COVID-19. Sci. Rep. 2021, 11, 1–8. [Google Scholar] [CrossRef]
- Moulson, N.; Petek, B.J.; Drezner, J.A.; Harmon, K.G.; Kliethermes, S.A.; Patel, M.R.; Baggish, A.L.; Asif, I.M.; Borchers, J.; Edenfield, K.M.; et al. SARS-CoV-2 Cardiac Involvement in Young Competitive Athletes. Circulation 2021, 144, 256–266. [Google Scholar] [CrossRef]
- Brito, D.; Meester, S.; Yanamala, N.; Patel, H.B.; Balcik, B.J.; Casaclang-Verzosa, G.; Seetharam, K.; Riveros, D.; Beto, R.J.; Balla, S.; et al. High Prevalence of Pericardial Involvement in College Student Athletes Recovering From COVID-19. JACC: Cardiovasc. Imag. 2021, 14, 541–555. [Google Scholar] [CrossRef] [PubMed]
- Ricci, F.; Aung, N.; Gallina, S.; Zemrak, F.; Fung, K.; Bisaccia, G.; Paiva, J.M.; Khanji, M.Y.; Mantini, C.; Palermi, S.; et al. Cardiovascular magnetic resonance reference values of mitral and tricuspid annular dimensions: The UK Biobank cohort. J. Cardiovasc. Magn. Reson. 2021, 23, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Palermi, S.; Serio, A.; Vecchiato, M.; Sirico, F.; Gambardella, F.; Ricci, F.; Iodice, F.; Radmilovic, J.; Russo, V.; D’Andrea, A. Potential role of an athlete-focused echocardiogram in sports eligibility. World J. Cardiol. 2021, 13, 271–297. [Google Scholar] [CrossRef]
- Puntmann, V.O.; Carerj, M.L.; Wieters, I.; Fahim, M.; Arendt, C.; Hoffmann, J.; Shchendrygina, A.; Escher, F.; Vasa-Nicotera, M.; Zeiher, A.M.; et al. Outcomes of Cardiovascular Magnetic Resonance Imaging in Patients Recently Recovered From Coronavirus Disease 2019 (COVID-19). JAMA Cardiol. 2020, 5, 1265. [Google Scholar] [CrossRef]
- Daniels, C.J.; Rajpal, S.; Greenshields, J.T.; Rosenthal, G.L.; Chung, E.H.; Terrin, M.; Jeudy, J.; Mattson, S.E.; Law, I.H.; Borchers, J.; et al. Prevalence of Clinical and Subclinical Myocarditis in Competitive Athletes with Recent SARS-CoV-2 Infection. JAMA Cardiol. 2021, 6, 1078. [Google Scholar] [CrossRef]
- Fayol, A.; Livrozet, M.; Boutouyrie, P.; Khettab, H.; Betton, M.; Tea, V.; Blanchard, A.; Bruno, R.; Hulot, J. French COVID cohort study group Cardiac performance in patients hospitalized with COVID-19: A 6 month follow-up study. ESC Heart Fail. 2021, 8, 2232–2239. [Google Scholar] [CrossRef]
- Daher, A.; Balfanz, P.; Cornelissen, C.; Müller, A.; Bergs, I.; Marx, N.; Müller-Wieland, D.; Hartmann, B.; Dreher, M.; Müller, T. Follow up of patients with severe coronavirus disease 2019 (COVID-19): Pulmonary and extrapulmonary disease sequelae. Respir. Med. 2020, 174, 106197. [Google Scholar] [CrossRef]
- Moody, W.E.; Liu, B.; Mahmoud-Elsayed, H.M.; Senior, J.; Lalla, S.S.; Khan-Kheil, A.M.; Brown, S.; Saif, A.; Moss, A.; Bradlow, W.M.; et al. Persisting Adverse Ventricular Remodeling in COVID-19 Survivors: A Longitudinal Echocardiographic Study. J. Am. Soc. Echocardiogr. 2021, 34, 562–566. [Google Scholar] [CrossRef] [PubMed]
- Lancellotti, P.; Zamorano, J.L.; Habib, G.; Badano, L. The EACVI Textbook of Echocardiography; Oxford University Press: Oxford, UK, 2016; ISBN 9780191792991. [Google Scholar]
- Lang, R.M.; Badano, L.P.; Mor-Avi, V.; Afilalo, J.; Armstrong, A.; Ernande, L.; Flachskampf, F.A.; Foster, E.; Goldstein, S.A.; Kuznetsova, T.; et al. Recommendations for Cardiac Chamber Quantification by Echocardiography in Adults: An Update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J. Am. Soc. Echocardiogr. 2015, 28, 1–39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Farsalinos, K.E.; Daraban, A.M.; Ünlü, S.; Thomas, J.D.; Badano, L.; Voigt, J.-U. Head-to-Head Comparison of Global Longitudinal Strain Measurements among Nine Different Vendors. J. Am. Soc. Echocardiogr. 2015, 28, 1171–1181.e2. [Google Scholar] [CrossRef]
- Papadopoulos, K.; Özden Tok, Ö.; Mitrousi, K.; Ikonomidis, I. Myocardial Work: Methodology and Clinical Applications. Diagnostics 2021, 11, 573. [Google Scholar] [CrossRef] [PubMed]
- Russell, K.; Eriksen, M.; Aaberge, L.; Wilhelmsen, N.; Skulstad, H.; Remme, E.W.; Haugaa, K.H.; Opdahl, A.; Fjeld, J.G.; Gjesdal, O.; et al. A novel clinical method for quantification of regional left ventricular pressure–strain loop area: A non-invasive index of myocardial work. Eur. Heart J. 2012, 33, 724–733. [Google Scholar] [CrossRef] [Green Version]
- Russell, K.; Eriksen, M.; Aaberge, L.; Wilhelmsen, N.; Skulstad, H.; Gjesdal, O.; Edvardsen, T.; Smiseth, O.A. Assessment of wasted myocardial work: A novel method to quantify energy loss due to uncoordinated left ventricular contractions. Am. J. Physiol. Heart Circ. Physiol. 2013, 305, H996–H1003. [Google Scholar] [CrossRef]
- Manganaro, R.; Marchetta, S.; Dulgheru, R.; Ilardi, F.; Sugimoto, T.; Robinet, S.; Cimino, S.; Go, Y.Y.; Bernard, A.; Kacharava, G.; et al. Echocardiographic reference ranges for normal non-invasive myocardial work indices: Results from the EACVI NORRE study. Eur. Heart J. Cardiovasc. Imag. 2019, 20, 582–590. [Google Scholar] [CrossRef]
- Maestrini, V.; Birtolo, L.I.; Francone, M.; Galardo, G.; Galea, N.; Severino, P.; Alessandri, F.; Colaiacomo, M.C.; Cundari, G.; Chimenti, C.; et al. Cardiac involvement in consecutive unselected hospitalized COVID-19 population: In-hospital evaluation and one-year follow-up. Int. J. Cardiol. 2021, 339, 235–242. [Google Scholar] [CrossRef]
- Ahmed, H.; Patel, K.; Greenwood, D.; Halpin, S.; Lewthwaite, P.; Salawu, A.; Eyre, L.; Breen, A.; O’Connor, R.; Jones, A.; et al. Long-term clinical outcomes in survivors of severe acute respiratory syndrome and Middle East respiratory syndrome coronavirus outbreaks after hospitalisation or ICU admission: A systematic review and meta-analysis. J. Rehabil. Med. 2020, 52, 63. [Google Scholar] [CrossRef]
- Madjid, M.; Safavi-Naeini, P.; Solomon, S.D.; Vardeny, O. Potential Effects of Coronaviruses on the Cardiovascular System: A Review. JAMA Cardiol. 2020, 5, 831–840. [Google Scholar] [CrossRef] [Green Version]
- Parry, A.H.; Wani, A.H.; Shah, N.N.; Jehangir, M. Medium-term chest computed tomography (CT) follow-up of COVID-19 pneumonia patients after recovery to assess the rate of resolution and determine the potential predictors of persistent lung changes. Egypt. J. Radiol. Nucl. Med. 2021, 52, 1–9. [Google Scholar] [CrossRef]
- Han, X.; Fan, Y.; Alwalid, O.; Li, N.; Jia, X.; Yuan, M.; Li, Y.; Cao, Y.; Gu, J.; Wu, H.; et al. Six-month Follow-up Chest CT Findings after Severe COVID-19 Pneumonia. Radiol. 2021, 299, E177–E186. [Google Scholar] [CrossRef]
- Özer, S.; Candan, L.; Özyıldız, A.G.; Turan, O.E. Evaluation of left ventricular global functions with speckle tracking echocardiography in patients recovered from COVID-19. Int. J. Cardiovasc. Imag. 2021, 37, 2227–2233. [Google Scholar] [CrossRef] [PubMed]
- Kotecha, T.; Knight, D.S.; Razvi, Y.; Kumar, K.; Vimalesvaran, K.; Thornton, G.; Patel, R.; Chacko, L.; Brown, J.T.; Coyle, C.; et al. Patterns of myocardial injury in recovered troponin-positive COVID-19 patients assessed by cardiovascular magnetic resonance. Eur. Heart J. 2021, 42, 1866–1878. [Google Scholar] [CrossRef] [PubMed]
- Heuvel, F.M.A.V.D.; Vos, J.L.; Koop, Y.; van Dijk, A.P.J.; Duijnhouwer, A.L.; de Mast, Q.; van de Veerdonk, F.L.; Bosch, F.; Kok, B.; Netea, M.G.; et al. Cardiac function in relation to myocardial injury in hospitalised patients with COVID-19. Neth. Heart J. 2020, 28, 410–417. [Google Scholar] [CrossRef]
- Minhas, A.S.; Gilotra, N.A.; Goerlich, E.; Metkus, T.; Garibaldi, B.T.; Sharma, G.; Bavaro, N.; Phillip, S.; Michos, E.D.; Hays, A.G. Myocardial Work Efficiency, A Novel Measure of Myocardial Dysfunction, Is Reduced in COVID-19 Patients and Associated With In-Hospital Mortality. Front. Cardiovasc. Med. 2021, 8, 667721. [Google Scholar] [CrossRef]
- Jaglan, A.; Roemer, S.; Jan, M.F.; Khandheria, B.K. Myocardial work index: A glimmer of hope in COVID-19. Eur. Heart J. Cardiovasc. Imag. 2021, 22, 228. [Google Scholar] [CrossRef]
- Hubert, A.; Le Rolle, V.; Leclercq, C.; Galli, E.; Samset, E.; Casset, C.; Mabo, P.; Hernandez, A.; Donal, E. Estimation of myocardial work from pressure–strain loops analysis: An experimental evaluation. Eur. Heart J. Cardiovasc. Imaging 2018, 19, 1372–1379. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Echocardiographic Parameters | Total Population (n = 66) | Dyspnea+ (n = 23) | Dyspne− (n = 43) | p Value |
|---|---|---|---|---|
| LVEF (%) | 56.9 ± 4.6 | 55.7 ± 4.6 | 57.6 ± 4.5 | 0.131 |
| LA volume (mL/m2) | 27.1 ± 7.5 | 27.1 ± 9.9 | 27.1 ± 6.0 | 0.986 |
| FAC (%) | 41.2 ± 8.8 | 40.8 ± 7.4 | 41.3 ± 9.6 | 0.838 |
| TAPSE (mm) | 24.8 ± 4.3 | 24.5 ± 4.9 | 25.0 ± 4.0 | 0.672 |
| E/A | 0.9 ± 0.2 | 1.0 ± 0.2 | 1.1 ± 0.3 | 0.046 |
| E/E’ | 9.1 ± 3.1 | 7.8 ± 2.4 | 7.2 ± 2.1 | 0.323 |
| S’ (cm/s) | 12.9 ± 2.1 | 12.3 ± 2.3 | 13.3 ± 1.8 | 0.077 |
| PAP (mmHg) | 16.5 ± 14.5 | 17.9 ± 14.1 | 15.7 ± 14.8 | 0.562 |
| GLS LV (%) | −20.9 ± 2.3 | −19.9 ± 2.1 | −21.3 ± 2.3 | 0.039 |
| GCW (mmHg%) | 2381.4 ± 463.6 | 2183.7 ± 487.9 | 2483.1 ± 422.4 | 0.024 |
| GWW (mmHg%) | 64.9 ± 33.1 | 60.9 ± 34.4 | 67.0 ± 32.7 | 0.530 |
| GWE (%) | 96.8 ± 2.5 | 96.4 ± 1.7 | 97.0 ± 2.8 | 0.425 |
| GWI (mmHg%) | 2132.5 ± 419.2 | 1960.0 ± 396.2 | 2221.1 ± 407.9 | 0.030 |
| GLS RV (%) | −21.9 ± 3.2 | −21.3 ± 2.9 | −22.3 ± 3.4 | 0.375 |
| GLS RV free wall (%) | −24.4 ± 4.2 | −25.2 ± 3.0 | −25.5 ± 4.8 | 0.831 |
| LV echocardiographic abnormalities in 66 patients | ||||
| LV systolic global dysfunction (n,%) | 1 (1.6%) | 1 (4.8%) | 0 (0%) | 0.181 |
| LV type 1 diastolic dysfunction (n,%) | 11 (16.7%) | 3 (14.3%) | 8 (21.6%) | 0.493 |
| LV type 2 diastolic dysfunction (n,%) | 1 (1.5%) | 1 (4.8%) | 0 (0%) | 0.181 |
| Parameter | Univariable Analysis | Multivariable Analysis | |||||||
|---|---|---|---|---|---|---|---|---|---|
| OR | 95% CI | p Value | OR | 95% CI | p Value | OR | 95% CI | p Value | |
| GLS LV | 1.321 | 1.004–1.738 | 0.047 | 1.171 | 0.848–1.616 | 0.338 | 1.179 | 0.853–1.628 | 0.318 |
| GCW | 0.998 | 0.997–1.000 | 0.035 | 0.998 | 0.997–1.000 | 0.035 | |||
| GWI | 0.998 | 0.997–1.000 | 0.040 | 0.998 | 0.997–1.000 | 0.040 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Luchian, M.-L.; Motoc, A.; Lochy, S.; Magne, J.; Belsack, D.; De Mey, J.; Roosens, B.; Van den Bussche, K.; Boeckstaens, S.; Chameleva, H.; et al. Subclinical Myocardial Dysfunction in Patients with Persistent Dyspnea One Year after COVID-19. Diagnostics 2022, 12, 57. https://doi.org/10.3390/diagnostics12010057
Luchian M-L, Motoc A, Lochy S, Magne J, Belsack D, De Mey J, Roosens B, Van den Bussche K, Boeckstaens S, Chameleva H, et al. Subclinical Myocardial Dysfunction in Patients with Persistent Dyspnea One Year after COVID-19. Diagnostics. 2022; 12(1):57. https://doi.org/10.3390/diagnostics12010057
Chicago/Turabian StyleLuchian, Maria-Luiza, Andreea Motoc, Stijn Lochy, Julien Magne, Dries Belsack, Johan De Mey, Bram Roosens, Karen Van den Bussche, Sven Boeckstaens, Hadischat Chameleva, and et al. 2022. "Subclinical Myocardial Dysfunction in Patients with Persistent Dyspnea One Year after COVID-19" Diagnostics 12, no. 1: 57. https://doi.org/10.3390/diagnostics12010057