
Factors Creating a Need for Repeated Drainage of Deep Neck Infections


1
Division of Chinese Internal Medicine, Center for Traditional Chinese Medicine, Chang Gung Memorial Hospital, Taoyuan 333, Taiwan
2
School of Medicine, Chang Gung University, Taoyuan 333, Taiwan
3
Department of Otorhinolaryngology & Head and Neck Surgery, New Taipei Municipal TuCheng Hospital (Built and Operated by Chang Gung Medical Foundation), New Taipei City 236, Taiwan
4
Department of Otorhinolaryngology & Head and Neck Surgery, Chang Gung Memorial Hospital, Linkou 333, Taiwan
5
Department of Medical Imaging and Intervention, Chang Gung Memorial Hospital, Linkou 333, Taiwan
*
Author to whom correspondence should be addressed.
Diagnostics 2022, 12(4), 940; https://doi.org/10.3390/diagnostics12040940
Submission received: 15 March 2022
/
Revised: 5 April 2022
/
Accepted: 8 April 2022
/
Published: 9 April 2022
(This article belongs to the Special Issue Diagnostic Infectious Disease and Microbiology)
Abstract
:Deep neck infection (DNI) is associated with morbidity and mortality. Surgical incision and drainage (I&D) of DNI abscesses are essential. Refractory abscesses require repeat I&D. Few studies have assessed the risk factors associated with repeat I&D; here, we investigated such factors. In total, 605 patients with DNI were enrolled between July 2016 and February 2022. Of these patients, 107 underwent repeat I&D. Clinical variables were assessed. On univariate analysis, a high blood sugar level (odds ratio (OR) = 1.006, p < 0.001), the involvement of at least four neck spaces (OR = 15.44, p < 0.001), and mediastinitis (OR = 1.787, p = 0.040) were significant risk factors for repeat I&D. On multivariate analysis, a high blood sugar level (OR = 1.005, p < 0.001) and the involvement of at least four neck spaces (OR = 14.79, p < 0.001) were significant independent risk factors for repeat I&D. Patients who required repeat I&D had longer hospital stays and a higher tracheostomy rate than did other patients (both p < 0.05). The pathogens did not differ between patients who did and did not require repeat surgical I&D (all p > 0.05), but the rates of pathogen non-growth from blood cultures were 19.47% (97/498) in the group without a need for repeat I&D and 0.93% (1/107) in the group with such a need (p < 0.001). DNI can be fatal; a higher blood sugar level and the involvement of at least four neck spaces were independent risk factors for repeat surgical I&D. If at least four neck spaces are involved, we recommend controlling the blood sugar level after admission. We found significant differences in the length of hospital stay and the need for tracheostomy between groups who did and did not require repeat surgical I&D. Although the pathogens did not differ between the groups, pathogen non-growth from blood cultures was less common in the group with for repeat surgical I&D than in the group without such a need.
1. Introduction
Deep neck infection (DNI) is a life-threatening bacterial infection [1]. Clinical manifestations of DNI include neck swelling and redness, localized heat, and shortness of breath; some patients exhibit airway obstruction. DNI can trigger severe sepsis, esophageal perforation, necrotizing fasciitis, descending necrotizing mediastinitis, disseminated intravascular coagulation, jugular vein thrombosis, and pericarditis [2,3,4,5,6,7,8,9]. In addition to antibiotics, surgical drainage and postoperative wound irrigation are required by patients with advanced DNI [10].
Surgery requires great care; the anatomical landmarks of DNI patients are not clearly evident [11,12]. Because major blood vessels such as the carotid artery and the jugular vein are located in the cervical region, precise abscess drainage is difficult [13]. Repeat surgery is required by some patients during the hospital stay [14,15]. Therapeutic management is complicated. However, few studies have sought risk factors associated with repeat surgical drainage; here, we investigated such factors.
2. Materials and Methods
We retrospectively reviewed the medical records of 605 patients with DNIs who were admitted to Chang Gung Memorial Hospital (Linkou, Taiwan) between July 2016 and February 2022. DNI was diagnosed by ultrasonography and computed tomography (CT) [7]. The involved deep neck spaces of CT images were identified retrospectively by at least one radiologist (S.-C.C.) and one otorhinolaryngologist (S.-L.C.). If there were situations where the involved deep neck spaces were difficult to identify, it would be decided by team discussion. Treatment included antibiotics and surgical incision and drainage (I&D). I&D was performed when the DNI compromised the airway, the abscess was large (≥2 cm), and when the DNI did not improve after 48 h of intravenous empirical antibiotics [16]. These antibiotics were ceftriaxone 1 g/12 h and metronidazole 500 mg/8 h; they reduced the levels of aerobic and anaerobic bacteria before culture results were available [17,18]. Postoperative irrigation was performed at intervals of 4–8 h depending on disease severity [19]. Repeat I&D was defined as more than one drainage procedure during the same hospital stay. We followed the patient’s clinical condition and laboratory data after the first open I&D. If the patient’s symptoms and data progressed seriously within 48–72 h, we further arranged a CT exam. If there were abscesses that must be drained, the clinician would arrange a repeated open I&D (Figure 1A,B).
2.1. Exclusion Criteria
The exclusion criteria were a swallowed foreign body, severe cardiopulmonary disease, previous head-and-neck tumor surgery, and prior head-and-neck chemoradiotherapy. Follow-up CT was used during hospitalization to exclude patients whose abscesses were initially ineffectively drained. In total, 605 patients were enrolled, of whom 107 required repeat drainage.
2.2. Data Collection
We recorded gender, age, C-reactive protein (CRP) and blood sugar levels, diabetes mellitus (DM) status, number of involved DNI spaces, mediastinitis status, length of hospital stay, tracheostomy status, all I&D procedures, and pathogens involved.
2.3. Statistical Analysis
All data were analyzed using MedCalc software (ver. 18.6; MedCalc, Ostend, Belgium). Because the Kolmogorov–Smirnov test showed that the data were not normally distributed, we used the chi-squared test to compare categorical variables and the Mann–Whitney U test to compare continuous variables. We employed logistic regression for univariate and multivariate analyses. We engaged in forward stepwise selection, which was followed by multivariate logistic regression; all variables included in univariate analysis were entered into the final multivariate model. For all analyses, p < 0.05 was considered to indicate statistical significance.
3. Results
Demographic and clinical data are listed in Table 1. In total, 605 DNI patients (397 men (65.62%) and 208 women (34.38%); mean age, 51.70 ± 18.66 years) were included. The mean CRP level was 147.96 ± 107.74 mg/L and the mean blood sugar level was 152.52 ± 79.34 mg/dL. Overall, 254 (41.98%) patients had DM. Involvement in all patients comprised one deep neck space in 153 (25.28%) patients, two spaces in 183 (30.24%) patients, three spaces in 156 (25.78%) patients, and at least four spaces in 113 (18.70%) patients.
Of those with deep neck space involvement, it involved the parapharyngeal space in 342 (56.52%) patients, the submandibular space in 243 (40.16%), the retropharyngeal space in 213 (35.20%), the masticator space in 124 (20.49%), the parotid space in 117 (19.33%), the carotid space in 58 (9.58%), the anterior cervical space in 57 (9.42%), the perivertebral space in 54 (8.92%), the visceral space in 53 (8.77%), and the posterior cervical space in 21 (3.47%). Mediastinitis was apparent in 85 (14.04%) patients. The mean length of hospital stay was 11.56 ± 9.18 days. Tracheostomy was performed on 120 (19.83%) patients. In total, 269 (44.46%) patients underwent I&D; 107 (17.68%) patients underwent at least two I&D procedures. Table 1 lists the cultured pathogens. The overall non-growth pathogen rate was 16.19% (98/605).
Table 2 shows the results of univariate analyses. A high blood sugar level (odds ratio (OR) = 1.006, 95% confidence interval (CI): 1.003–1.008, p < 0.001), the involvement of at least four spaces (OR = 15.44, 95% CI: 9.443–25.26, p < 0.001), and mediastinitis (OR = 1.787, 95% CI: 1.043–3.061, p = 0.040) were significant risk factors for repeat I&D. All factors were subjected to forward stepwise selection, which was followed by multivariate logistic regression. A high blood sugar level (OR = 1.005, 95% CI: 1.003–1.008, p < 0.001) and the involvement of at least four spaces (OR = 14.79, 95% CI: 8.931–24.49, p < 0.001) were significant independent risk factors for repeat I&D (Table 2).
Table 3 lists the hospital stays and tracheostomy statuses of the 107 patients who underwent repeat I&D and the 498 patients who did not. The hospital stay was significantly longer for patients who underwent repeat I&D (18.19 ± 9.06 days) than for patients who did not undergo repeat I&D (10.13 ± 8.56 days, p < 0.001). The tracheostomy rate was significantly higher for patients who underwent repeat I&D (66.35%, 71/107) than for patients who did not undergo repeat I&D (9.83%, 49/498).
Table 4 lists the pathogens in both groups; there were no significant differences (all p > 0.05). However, no pathogens grew from blood cultures for 0.93% (1/107) of patients who underwent repeat I&D and for 19.47% (97/498) of patients who did not require repeat I&D; this difference was statistically significant (p < 0.001).
4. Discussion
DNI can trigger life-threatening complications; management includes broad-spectrum intravenous antibiotics, timely surgical drainage, and airway protection (i.e., intubation and/or tracheostomy) [20]. The annual incidence of DNI is approximately 9–15/100,000; the most common etiology is dental [21,22]. Obregon-Guerrero reported that of 87 patients with DNIs, 21 (24%) required re-operation [14]. This burdens the healthcare system and increases medical costs [15,23]. Our rate of repeat I&D was 17.68%. A higher blood sugar level and the involvement of at least four spaces were independent risk factors associated with repeat I&D. Patients with such factors required longer hospital stays and a higher rate of tracheostomy than did other patients. Although the pathogens did not differ between groups, pathogen non-growth from blood was less common in the repeat I&D group (0.93%, 1/107) than in the other group (19.47%, 97/498). As shown in Table 2, a higher blood sugar level, the involvement of at least four spaces, and mediastinitis were risk factors for repeat I&D on univariate analysis.
Mediastinitis can be fatal; DNI spreads along the cervical fascia and the neck spaces down to the mediastinum [24]. The mortality rate was reportedly near 40% prior to the 1990s [25]. As diagnostic methods, surgical techniques, and intensive care unit protocols improved over the past 20 years, the outcomes and mortality have also improved. Multidisciplinary approaches and comprehensive medical treatments have significantly reduced mortality [9]. We found that the mediastinitis rate did not differ between the two groups on multivariate analysis. Mediastinitis indicates a severe infection. However, mediastinitis is not necessarily associated with incomplete surgical drainage. If mediastinitis did not occur in a site that was difficult to drain or irrigate, repeat I&D would be unnecessary.
We found that a higher blood sugar level and DNI involving at least four spaces were independent risk factors for repeat I&D on both univariate and multivariate analyses. Liu et al. reported that a high preoperative blood sugar was independently correlated with persistent discharge after operation to treat DNI [26]. Moreover, early blood sugar control has been shown to reduce infectious complications [27,28]. Importantly, we found that DNI involving at least four spaces was an independent risk factor for repeat I&D. The involvement of multiple spaces indicates an advanced infection [1] and increases mortality; elderly patients tend to exhibit more involved spaces than do patients aged <18 years [29]. Multiple-space DNI is associated with severe inflammation and increases the volume of cryptic space that is difficult to irrigate. Although blood sugar level can be the underlying reason for the repeat I&D, it can also be the effect of a more serious inflammatory response due to infection or even sepsis. We still recommend controlling the blood sugar level, especially in DNI patients who exhibit involvement of multiple spaces.
Table 3 shows that the length of hospital stay and tracheostomy rate were higher in the repeat I&D group than in the other group. Careful airway protection with close surveillance of respiratory function and adequate infection control are important considerations [30]. Ideally, airway specialists (otolaryngologists and anesthesiologists) should evaluate all patients early to prepare for airway security. The involvement of multiple spaces was previously identified as a risk factor for tracheostomy [31]. Patients undergoing repeat I&D should be closely monitored until airway signs and symptoms resolve [32]. Postoperative ventilation for >48 h was independently associated with unplanned re-operation [15], which is consistent with the findings of other studies: prolonged ventilation was a risk factor for re-operation and re-admission [33,34]. Older age and DM were correlated with a longer hospital stay [35].
Table 4 shows that the pathogens did not significantly differ between groups. The rate of specific pathogen non-growth from blood cultures was 19.47% (97/498) in the group that did not undergo repeat I&D, while it was only 0.93% (1/107) in the group that did undergo this procedure, which differed significantly. In addition, the overall rate of specific pathogen non-growth was 16.19% (98/605). Blood culture does not sensitively identify pathogens, especially when antibiotics have been administered [36,37].
Limitations of the Article
This study has some limitations. First, the retrospective nature of the study at a single institution resulted in a certain attrition rate. Furthermore, the repeated drainage for DNI is clinical and determined by the clinician. As such, while the independent variables are logical for repeated drainage, they do not mandate the requirement for repeated drainage. The bias occurred in this mode of data acquisition.
5. Conclusions
A higher blood sugar level and the involvement of at least four spaces were independent risk factors for repeat I&D. In such patients, the blood sugar level should be controlled after admission. The repeat I&D group exhibited a longer hospital stay and a higher tracheostomy rate than did the other group. Although the pathogens did not differ between the two groups, specific pathogen non-growth from blood was less common in the repeat I&D group than in the other group.
Author Contributions
Conceptualization, C.-Y.H., Y.-C.W., S.-C.C. and S.-L.C.; methodology, C.-Y.H. and S.-L.C.; validation, C.-Y.H. and S.-L.C.; data curation, C.-Y.H. and S.-L.C.; writing—original draft preparation, C.-Y.H. and S.-L.C.; writing—review and editing, S.-L.C.; visualization, C.-Y.H., S.-C.C. and S.-L.C.; supervision, C.-Y.H., Y.-C.W. and S.-L.C.; project administration, C.-Y.H., S.-C.C. and S.-L.C. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
This study was approved by the Institutional Review Board (IRB) of the Chang Gung Medical Foundation (IRB no. 202200298B0).
Informed Consent Statement
The data were collected retrospectively, and the patients were anonymized before data analysis. The IRB waived the need for informed consent.
Data Availability Statement
All data generated or analyzed during this study are included in this published article. The data are available on request.
Acknowledgments
The authors thank all of the members of Department of Otorhinolaryngology-Head and Neck Surgery, Chang Gung Memorial Hospital, Linkou, for their invaluable help.
Conflicts of Interest
The authors declare no conflict of interest.
Abbreviations
| CT | Computed tomography |
| CRP | C-reactive protein |
| DNI | Deep neck infection |
| DM | Diabetes mellitus |
| I&D | Incision and drainage |
| OR | Odds ratio |
References
- Velhonoja, J.; Laaveri, M.; Soukka, T.; Irjala, H.; Kinnunen, I. Deep neck space infections: An upward trend and changing characteristics. Eur. Arch. Otorhinolaryngol. 2020, 277, 863–872. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tapiovaara, L.; Back, L.; Aro, K. Comparison of intubation and tracheotomy in patients with deep neck infection. Eur. Arch. Otorhinolaryngol. 2017, 274, 3767–3772. [Google Scholar] [CrossRef] [PubMed]
- Rzepakowska, A.; Rytel, A.; Krawczyk, P.; Osuch-Wójcikiewicz, E.; Widłak, I.; Deja, M.; Niemczyk, K. The Factors Contributing to Efficiency in Surgical Management of Purulent Infections of Deep Neck Spaces. Ear Nose Throat J. 2021, 100, 354–359. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boscolo-Rizzo, P.; Marchiori, C.; Montolli, F.; Vaglia, A.; Da Mosto, M.C. Deep neck infections: A constant challenge. ORL J. Otorhinolaryngol. Relat. Spec. 2006, 68, 259–265. [Google Scholar] [CrossRef] [PubMed]
- Prado-Calleros, H.M.; Jimenez-Fuentes, E.; Jimenez-Escobar, I. Descending necrotizing mediastinitis: Systematic review on its treatment in the last 6 years, 75 years after its description. Head Neck 2016, 38 (Suppl. 1), E2275–E2283. [Google Scholar] [CrossRef]
- Aizawa, N.; Tsuchiya, A.; Takahashi, S. Two cases of deep neck infection with esophageal perforation. J.-STAGE 2013, 26, 149–154. [Google Scholar] [CrossRef]
- Ho, C.-Y.; Wang, Y.-C.; Chin, S.-C.; Chen, S.-L. Factors Affecting Patients with Concurrent Deep Neck Infection and Acute Epiglottitis. Diagnostics 2022, 12, 29. [Google Scholar] [CrossRef]
- Chen, S.-L.; Chin, S.-C.; Wang, Y.-C.; Ho, C.-Y. Factors Affecting Patients with Concurrent Deep Neck Infection and Cervical Necrotizing Fasciitis. Diagnostics 2022, 12, 443. [Google Scholar] [CrossRef]
- Ho, C.Y.; Chin, S.C.; Chen, S.L. Management of Descending Necrotizing Mediastinitis, a Severe Complication of Deep Neck Infection, Based on Multidisciplinary Approaches and Departmental Co-Ordination. Ear Nose Throat J. 2022, 1455613211068575. [Google Scholar] [CrossRef]
- Tsai, M.-S.; Chang, G.-H.; Chen, W.-M.; Liu, C.-Y.; Lin, M.-H.; Chang, P.-J.; Huang, T.-Y.; Tsai, Y.-T.; Wu, C.-Y.; Hsu, C.-M.; et al. The Association between Decompensated Liver Cirrhosis and Deep Neck Infection: Real-World Evidence. Int. J. Environ. Res. Public Health 2019, 16, 3863. [Google Scholar] [CrossRef] [Green Version]
- Cable, B.B.; Brenner, P.; Bauman, N.M.; Mair, E.A. Image-guided surgical drainage of medial parapharyngeal abscesses in children: A novel adjuvant to a difficult approach. Ann. Otol. Rhinol. Laryngol. 2004, 113, 115–120. [Google Scholar] [CrossRef]
- Nagy, M.; Pizzuto, M.; Backstrom, J.; Brodsky, L. Deep neck infections in children: A new approach to diagnosis and treatment. Laryngoscope 1997, 107, 1627–1634. [Google Scholar] [CrossRef] [PubMed]
- Han, S.M.; Chae, H.S.; Lee, H.N.; Jeon, H.J.; Bong, J.P.; Kim, J.H. Computed tomography-guided navigation assisted drainage for inaccessible deep neck abscess: A case report. Medicine 2019, 98, e14674. [Google Scholar] [CrossRef] [PubMed]
- Obregon-Guerrero, G.; Martinez-Ordaz, J.L.; Moreno-Aguilera, E.; Ramirez-Martinez, M.; Pena-Garcia, J.F.; Perez-Alvarez, C. Deep neck abscess. Factors related to reoperation and mortality. Cir. Cir. 2013, 81, 299–306. [Google Scholar]
- Sangal, N.R.; Nishimori, K.; Zhao, E.; Siddiqui, S.H.; Baredes, S.; Chan Woo Park, R. Understanding Risk Factors Associated with Unplanned Reoperation in Major Head and Neck Surgery. JAMA Otolaryngol. Head Neck Surg. 2018, 144, 1044–1051. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.L.; Young, C.K.; Liao, C.T.; Tsai, T.Y.; Kang, C.J.; Huang, S.F. Parotid Space, a Different Space from Other Deep Neck Infection Spaces. Microorganisms 2021, 9, 2361. [Google Scholar] [CrossRef]
- Yang, S.W.; Lee, M.H.; See, L.C.; Huang, S.H.; Chen, T.M.; Chen, T.A. Deep neck abscess: An analysis of microbial etiology and the effectiveness of antibiotics. Infect. Drug Resist. 2008, 1, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, M.K.; Wen, Y.S.; Chang, C.C.; Lee, H.S.; Huang, M.T.; Hsiao, H.C. Deep neck infections in diabetic patients. Am. J. Otolaryngol. 2000, 21, 169–173. [Google Scholar] [CrossRef]
- Ding, M.C.; Lee, C.Y.; Wang, Y.T.; Hsu, C.M.; Tsai, Y.T.; Tsai, M.S. Innovative continuous-irrigation approach for wound care after deep neck infection surgery: A case report. Int. J. Surg. Case Rep. 2021, 80, 105620. [Google Scholar] [CrossRef]
- Ferzli, G.; Sukato, D.C.; Mourad, M.; Kadakia, S.; Gordin, E.A.; Ducic, Y. Aggressive Necrotizing Fasciitis of the Head and Neck Resulting in Massive Defects. Ear Nose Throat J. 2019, 98, 197–200. [Google Scholar] [CrossRef]
- Boscolo-Rizzo, P.; Stellin, M.; Muzzi, E.; Mantovani, M.; Fuson, R.; Lupato, V.; Trabalzini, F.; DA Mosto, M.C. Deep neck infections: A study of 365 cases highlighting recommendations for management and treatment. Eur. Arch. Otorhinolaryngol. 2012, 269, 1241–1249. [Google Scholar] [CrossRef] [PubMed]
- Staffieri, C.; Fasanaro, E.; Favaretto, N.; La Torre, F.B.; Sanguin, S.; Giacomelli, L.; Marino, F.; Ottaviano, G.; Staffieri, A.; Marioni, G. Multivariate approach to investigating prognostic factors in deep neck infections. Eur. Arch. Otorhinolaryngol. 2014, 271, 2061–2067. [Google Scholar] [CrossRef] [PubMed]
- Palmer, S.J.; Parker, M.J.; Hollingworth, W. The cost and implications of reoperation after surgery for fracture of the hip. J. Bone Jt. Surg. Br. 2000, 82, 864–866. [Google Scholar] [CrossRef]
- Sokouti, M.; Nezafati, S. Descending necrotizing mediastinitis of oropharyngeal infections. J. Dent. Res. Dent. Clin. Dent. Prospect. 2009, 3, 82–85. [Google Scholar] [CrossRef]
- Dzian, A.; Malík, M.; Fučela, I.; Skaličanová, M.; Stiegler, P.; Hajtman, A.; Bugová, G.; Sániová, B.D. A multidisciplinary approach to the management of descending necrotizing mediastinitis—Case series. Neuro. Endocrinol. Lett. 2019, 40, 284–288. [Google Scholar]
- Liu, S.-A.; Liang, M.-T.; Wang, C.-P.; Lin, W.-D.; Ho, H.-C.; Chiu, Y.-T. Preoperative blood sugar and C-reactive protein associated with persistent discharge after incision and drainage for patients with deep neck abscesses. Clin. Otolaryngol. 2009, 34, 336–342. [Google Scholar] [CrossRef] [PubMed]
- Bochicchio, G.V.; Joshi, M.; Bochicchio, K.M.; Pyle, A.; Johnson, S.B.; Meyer, W.; Lumpkins, K.; Scalea, T.M. Early hyperglycemic control is important in critically injured trauma patients. J. Trauma 2007, 63, 1353–1358. [Google Scholar] [CrossRef]
- Hemmila, M.R.; Taddonio, M.A.; Arbabi, S.; Maggio, P.M.; Wahl, W.L. Intensive insulin therapy is associated with reduced infectious complications in burn patients. Surgery. 2008, 144, 629–635. [Google Scholar] [CrossRef] [Green Version]
- Maharaj, S.; Ahmed, S.; Pillay, P. Deep Neck Space Infections: A Case Series and Review of the Literature. Clin. Med. Insights Ear Nose Throat 2019, 12, 1179550619871274. [Google Scholar] [CrossRef] [Green Version]
- Pineau, P.M.; Gautier, J.; Pineau, A.; Emam, N.; Laccourreye, L.; Boucher, S. Intubation decision criteria in adult epiglottitis. Eur. Ann. Otorhinolaryngol. Head Neck Dis. 2021, 138, 329–332. [Google Scholar] [CrossRef]
- Chen, S.-L.; Young, C.-K.; Tsai, T.-Y.; Chien, H.-T.; Kang, C.-J.; Liao, C.-T.; Huang, S.-F. Factors Affecting the Necessity of Tracheostomy in Patients with Deep Neck Infection. Diagnostics 2021, 11, 1536. [Google Scholar] [CrossRef] [PubMed]
- Dowdy, R.A.E.; Cornelius, B.W. Medical Management of Epiglottitis. Anesth. Prog. 2020, 67, 90–97. [Google Scholar] [CrossRef] [PubMed]
- Kang, Y.A. Risk Factors and Outcomes Associated with Readmission to the Intensive Care Unit after Cardiac Surgery. AACN Adv. Crit Care 2016, 27, 29–39. [Google Scholar] [CrossRef] [PubMed]
- Algattas, H.; Kimmell, K.T.; Vates, G.E. Risk of Reoperation for Hemorrhage in Patients After Craniotomy. World Neurosurg. 2016, 87, 531–539. [Google Scholar] [CrossRef]
- O’Brien, K.J.; Snapp, K.R.; Dugan, A.J.; Westgate, P.M.; Gupta, N. Risk Factors Affecting Length of Stay in Patients with Deep Neck Space Infection. Laryngoscope 2020, 130, 2133–2137. [Google Scholar] [CrossRef]
- Islam, A.; Oko, M. Cervical necrotising fasciitis and descending mediastinitis secondary to unilateral tonsillitis: A case report. J. Med. Case Rep. 2008, 2, 368. [Google Scholar] [CrossRef] [Green Version]
- Guardiani, E.; Bliss, M.; Harley, E. Supraglottitis in the era following widespread immunization against Haemophilus influenzae type B: Evolving principles in diagnosis and management. Laryngoscope 2010, 120, 2183–2188. [Google Scholar] [CrossRef]
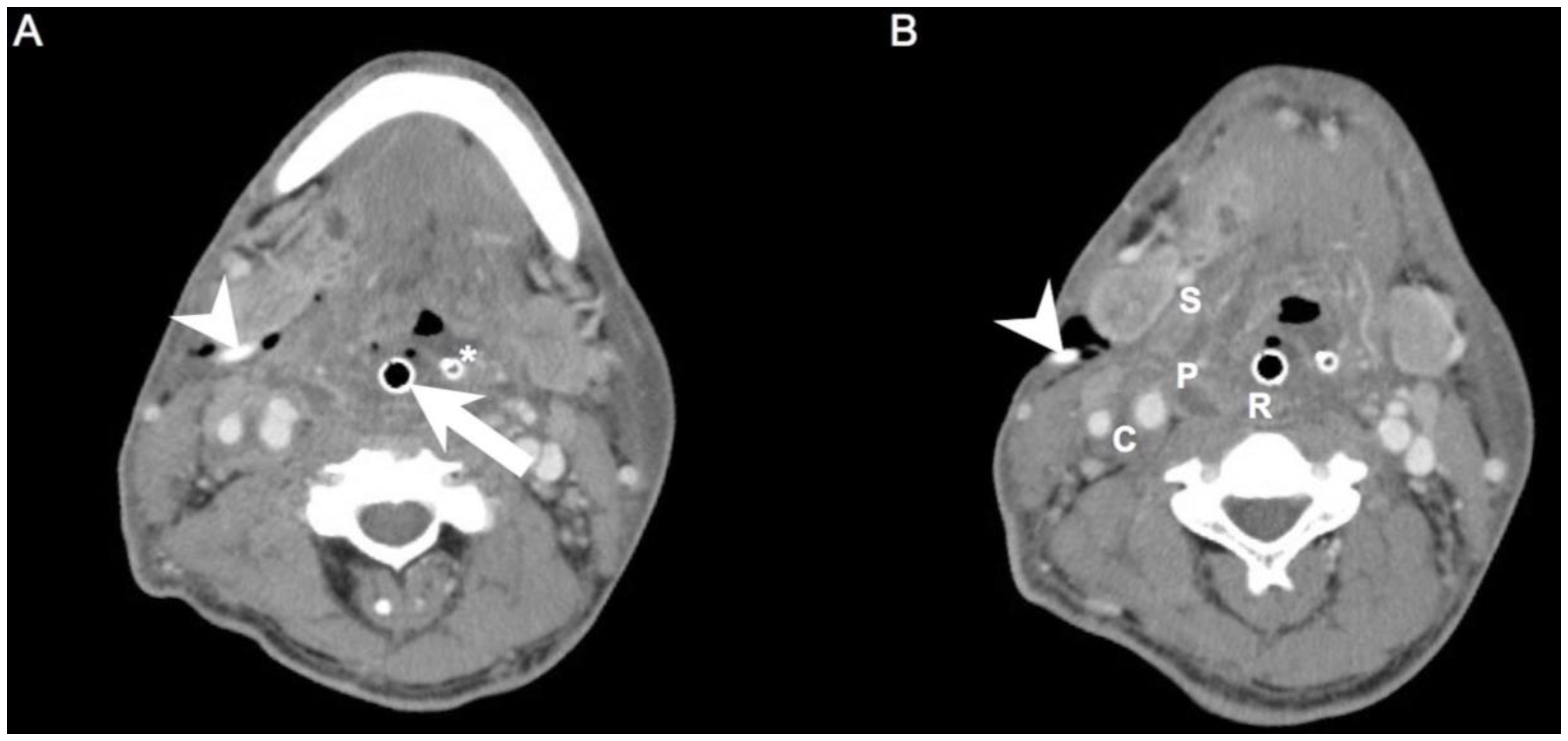
Figure 1.
(A,B). Axial views of a patient who required repeat I&D. Arrowhead: drainage tube of the first surgery; Arrow: endotracheal tube; Asterisk: nasogastric tube; C: carotid space; P: parapharyngeal space; R: retropharyngeal space; S: submandibular space.
Figure 1.
(A,B). Axial views of a patient who required repeat I&D. Arrowhead: drainage tube of the first surgery; Arrow: endotracheal tube; Asterisk: nasogastric tube; C: carotid space; P: parapharyngeal space; R: retropharyngeal space; S: submandibular space.


{kind=link}
Table 1.
Clinical characteristics of the 605 DNI patients undergoing surgical drainage.
| Characteristics | N (%) |
|---|---|
| Gender | 605 (100.00) |
| Male | 397 (65.62) |
| Female | 208 (34.38) |
| Age, years (SD) | 51.70 ± 18.66 |
| CRP, mg/L (SD) | 147.96 ± 107.74 |
| Blood sugar, mg/dL (SD) | 152.52 ± 79.34 |
| Diabetes mellitus | 254 (41.98) |
| Number of deep neck space involvement | |
| Single space | 153 (25.28) |
| Double spaces | 183 (30.24) |
| Triple spaces | 156 (25.78) |
| Multiple spaces, ≥4 | 113 (18.70) |
| Deep neck space involvement | |
| Parapharyngeal space | 342 (56.52) |
| Submandibular space | 243 (40.16) |
| Retropharyngeal space | 213 (35.20) |
| Masticator space | 124 (20.49) |
| Parotid space | 117 (19.33) |
| Carotid space | 58 (9.58) |
| Anterior cervical space | 57 (9.42) |
| Perivertebral space | 54 (8.92) |
| Visceral space | 53 (8.77) |
| Posterior cervical space | 21 (3.47) |
| Mediastinitis | 85 (14.04) |
| Length of hospital stay, days (SD) | 11.56 ± 9.18 |
| Tracheostomy | 120 (19.83) |
| Surgical I&D | 269 (44.46) |
| Repeated surgical I&D, ≥2 | 107 (17.68) |
| Pathogens | |
| Streptococcus constellatus | 122 (20.16) |
| Prevotella intermedia | 76 (12.56) |
| Parvimonas micra | 73 (12.06) |
| Klebsiella pneumoniae | 70 (11.57) |
| Streptococcus anginosus | 66 (10.90) |
| Prevotella buccae | 65 (10.74) |
| Staphylococcus aureus | 37 (6.11) |
| Streptococcus salivarius | 28 (4.62) |
| Streptococcus pneumoniae | 25 (4.13) |
| Gemella morbillorum | 24 (3.96) |
| Staphylococcus epidemidis | 22 (3.63) |
| Serratia marcescens | 22 (3.63) |
| Eikenella corrodens | 19 (3.14) |
| Streptococcus oralis | 17 (2.80) |
| Salmonella enterica | 16 (2.64) |
| Pseudomonas aeruginosa | 15 (2.47) |
| Slackia exigua | 13 (2.14) |
| Rothia amarae | 11 (1.81) |
| Stenotrophomonas maltophilia | 11 (1.81) |
| No growth | 98 (16.19) |
DNI = deep neck infection; N = numbers; SD = standard deviation; CRP = C-reactive protein (normal range <5 mg/L); Blood sugar (normal range: 70–100 mg/dL); Incision and drainage = I&D.
Table 2.
Univariate and multivariate analyses of data concerning 107 patients who required repeat I&D and 498 patients who did not.
Table 2.
Univariate and multivariate analyses of data concerning 107 patients who required repeat I&D and 498 patients who did not.
| Variable | Repeated Surgical I&D | Univariate Analysis | Multivariate Analysis | |||||
|---|---|---|---|---|---|---|---|---|
| Yes | No | OR | 95% CI | p-Value | OR | 95% CI | p-Value | |
| Gender | 107 | 498 | 0.875 | |||||
| Male | 71 | 326 | 1.040 | 0.643–1.555 | ||||
| Female | 36 | 172 | 1.000 | |||||
| Age, years | 0.912 | |||||||
| >60 | 40 | 189 | 0.976 | 0.634–1.502 | ||||
| ≤60 | 67 | 309 | 1.000 | |||||
| CRP, mg/L (SD) | 160.18 ± 106.54 | 145.34 ± 107.92 | 1.001 | 0.999–1.003 | 0.199 | |||
| Blood sugar, mg/dL (SD) | 191.69 ± 91.45 | 144.10 ± 73.92 | 1.006 | 1.003–1.008 | <0.001 * | 1.005 | 1.003–1.008 | <0.001 * |
| Diabetes mellitus | 0.082 | |||||||
| Yes | 53 | 201 | 1.450 | 0.953–2.205 | ||||
| No | 54 | 297 | 1.000 | |||||
| Multiple spaces, ≥4 | <0.001 * | <0.001 * | ||||||
| Yes | 66 | 47 | 15.44 | 9.443–25.26 | 14.79 | 8.931–24.49 | ||
| No | 41 | 451 | 1.000 | 1.000 | ||||
| Parapharyngeal space | 0.588 | |||||||
| Yes | 63 | 279 | 1.123 | 0.654–1.527 | ||||
| No | 44 | 219 | 1.000 | |||||
| Submandibular space | 0.660 | |||||||
| Yes | 45 | 198 | 1.099 | 0.719–1.679 | ||||
| No | 62 | 300 | 1.000 | |||||
| Retropharyngeal space | 0.293 | |||||||
| Yes | 33 | 180 | 0.787 | 0.502–1.234 | ||||
| No | 74 | 318 | 1.000 | |||||
| Masticator space | 0.182 | |||||||
| Yes | 27 | 97 | 1.395 | 0.855–2.276 | ||||
| No | 80 | 401 | 1.000 | |||||
| Parotid space | 0.724 | |||||||
| Yes | 22 | 95 | 1.098 | 0.653–1.845 | ||||
| No | 85 | 403 | 1.000 | |||||
| Carotid space | 0.101 | |||||||
| Yes | 15 | 43 | 1.725 | 0.919–3.236 | ||||
| No | 92 | 455 | 1.000 | |||||
| Anterior cervical space | 0.689 | |||||||
| Yes | 9 | 48 | 0.861 | 0.408–1.813 | ||||
| No | 98 | 450 | 1.000 | |||||
| Perivertebral space | 0.214 | |||||||
| Yes | 13 | 41 | 1.541 | 0.795–2.989 | ||||
| No | 94 | 457 | 1.000 | |||||
| Visceral space | 0.096 | |||||||
| Yes | 14 | 39 | 1.771 | 0.924–3.394 | ||||
| No | 93 | 459 | 1.000 | |||||
| Posterior cervical space | 0.211 | |||||||
| Yes | 6 | 15 | 1.912 | 0.724–5.049 | ||||
| No | 101 | 483 | 1.000 | |||||
| Mediastinitis | 0.040 * | - | - | - | ||||
| Yes | 22 | 63 | 1.787 | 1.043–3.061 | ||||
| No | 85 | 435 | 1.000 | |||||
DNI = deep neck infection; Incision and drainage = I&D; SD = standard deviation; OR = odds ratio; CI = confidence intervals; CRP = C-reactive protein; * p < 0.05 shown in bold.
Table 3.
Hospital stay lengths and tracheostomy statuses concerning 107 patients who required repeat I&D and 498 patients who did not.
Table 3.
Hospital stay lengths and tracheostomy statuses concerning 107 patients who required repeat I&D and 498 patients who did not.
| Characteristics | Repeated, N = 107 (%) | Non-Repeated, N = 498 (%) | p-Value |
|---|---|---|---|
| Length of hospital stay, days (SD) | 18.19 ± 9.06 | 10.13 ± 8.56 | <0.001 * |
| Tracheostomy | <0.001 * | ||
| Yes | 71 (66.35) | 49 (9.83) | |
| No | 36 (33.65) | 449 (90.17) |
I&D = incision and drainage; DNI = deep neck infection; N = number; * p < 0.05 shown in bold.
Table 4.
Pathogens concerning 107 patients who required repeat I&D and 498 patients who did not.
| Pathogens | Repeated, N = 107 (%) | Non-Repeated, N = 498 (%) | p-Value |
|---|---|---|---|
| Streptococcus constellatus | 24 (22.42) | 98 (19.67) | 0.520 |
| Prevotella intermedia | 15 (14.01) | 61 (12.24) | 0.630 |
| Parvimonas micra | 11 (10.28) | 62 (12.44) | 0.511 |
| Klebsiella pneumoniae | 12 (11.21) | 58 (11.64) | 0.907 |
| Streptococcus anginosus | 9 (8.41) | 57 (11.44) | 0.346 |
| Prevotella buccae | 10 (9.34) | 55 (11.04) | 0.587 |
| Staphylococcus aureus | 9 (8.41) | 28 (5.62) | 0.296 |
| Streptococcus salivarius | 8 (7.47) | 20 (4.01) | 0.148 |
| Streptococcus pneumoniae | 2 (1.86) | 23 (4.61) | 0.156 |
| Gemella morbillorum | 2 (1.86) | 22 (4.41) | 0.179 |
| Staphylococcus epidemidis | 6 (5.60) | 16 (3.21) | 0.259 |
| Serratia marcescens | 4 (3.73) | 18 (3.61) | 0.950 |
| Eikenella corrodens | 4 (3.73) | 15 (3.01) | 0.704 |
| Streptococcus oralis | 2 (1.86) | 15 (3.01) | 0.491 |
| Salmonella enterica | 3 (2.80) | 13 (2.61) | 0.910 |
| Pseudomonas aeruginosa | 5 (4.67) | 10 (2.00) | 0.140 |
| Slackia exigua | 2 (1.86) | 11 (2.20) | 0.818 |
| Rothia amarae | 2 (1.86) | 9 (1.80) | 0.965 |
| Stenotrophomonas maltophilia | 4 (3.73) | 7 (1.40) | 0.136 |
| No growth | 1 (0.93) | 97 (19.47) | <0.001 * |
I&D = incision and drainage; DNI = deep neck infection; N = number. * p < 0.05 shown in bold.
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Ho, C.-Y.; Wang, Y.-C.; Chin, S.-C.; Chen, S.-L. Factors Creating a Need for Repeated Drainage of Deep Neck Infections. Diagnostics 2022, 12, 940. https://doi.org/10.3390/diagnostics12040940
AMA Style
Ho C-Y, Wang Y-C, Chin S-C, Chen S-L. Factors Creating a Need for Repeated Drainage of Deep Neck Infections. Diagnostics. 2022; 12(4):940. https://doi.org/10.3390/diagnostics12040940
Chicago/Turabian StyleHo, Chia-Ying, Yu-Chien Wang, Shy-Chyi Chin, and Shih-Lung Chen. 2022. "Factors Creating a Need for Repeated Drainage of Deep Neck Infections" Diagnostics 12, no. 4: 940. https://doi.org/10.3390/diagnostics12040940
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.