The Impact of COVID-19 on Telemedicine Utilization Across Multiple Service Lines in the United States



Abstract
:1. Introduction
1.1. Definition of Key Terms
1.2. Rationale
1.3. Significance
1.4. Objective
2. Methods
2.1. Protocol and Registration
2.2. Eligibility Criteria
2.3. Information Sources
2.4. Search
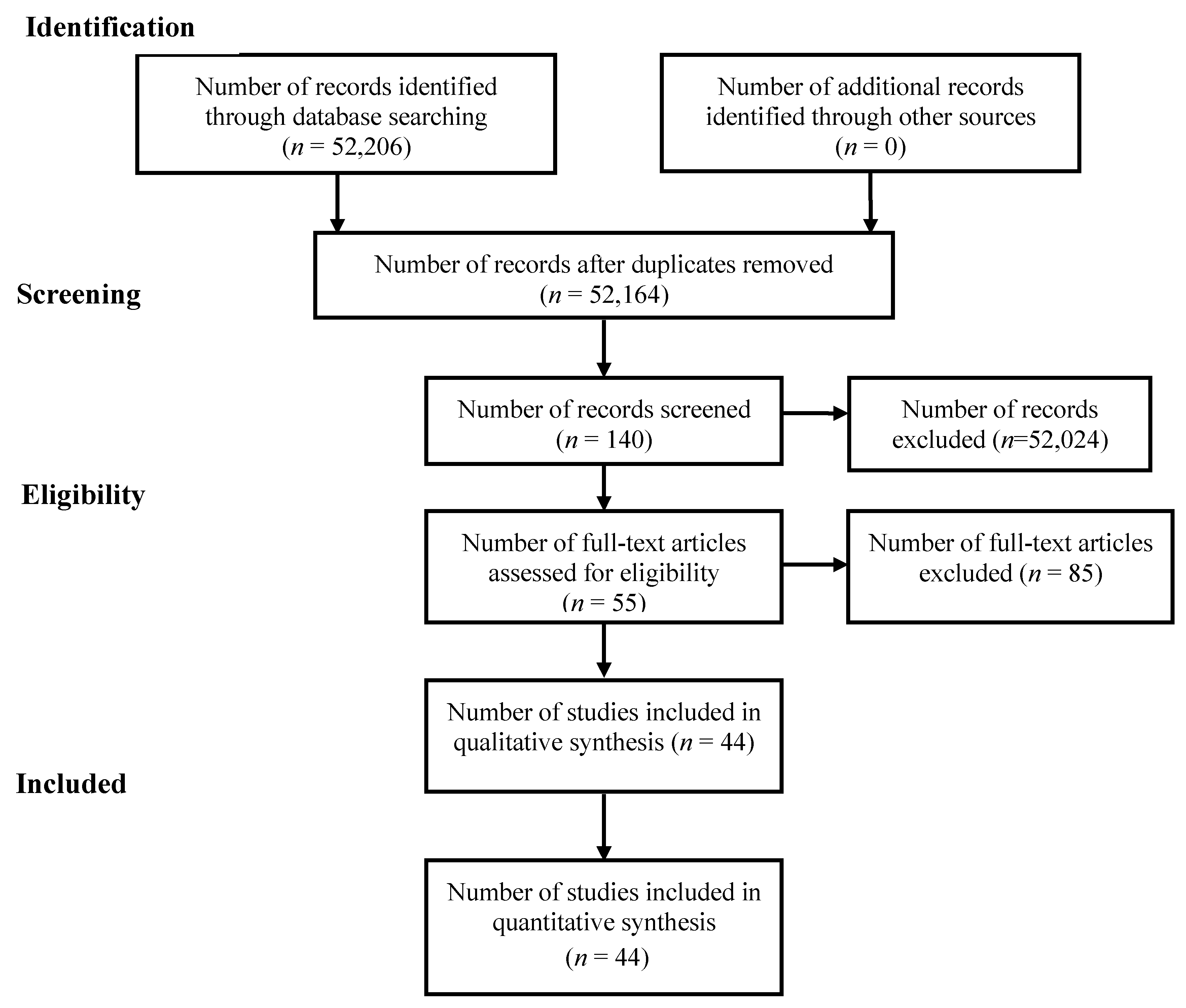
2.5. Study Selection
2.6. Data Collection Process
2.7. Data Items
2.8. Risk of Bias in Individual Studies
2.9. Summary Measures
2.10. Additional Analysis
3. Results
3.1. Results of Individual Studies and Synthesis of Results
3.2. Additional Analysis
4. Discussion
4.1. Summary of Evidence
4.2. Limitations
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Bashshur, R.; Shannon, G.W. History of Telemedicine: Evolution, Context, and Transformation; Mary Ann Liebert: New Rochelle, NY, USA, 2009. [Google Scholar]
- Telemedicine: A Guide to Assessing Telecommunications in Health Care. Available online: https://www.ncbi.nlm.nih.gov/books/NBK45445/ (accessed on 25 July 2020).
- The Evolution of Telemedicine. Available online: https://chironhealth.com/definitive-guide-to-telemedicine/about-telemedicine/evolution-of-telemedicine/ (accessed on 26 July 2020).
- Castro, F. The Roots of Telemedicine. Available online: https://athenetelehealth.com/the-roots-of-telemedicine/ (accessed on 26 July 2020).
- Nesbitt, T.S.; Katz-Bell, J. History of Telehealth. In Understanding Telehealth; McGraw-Hill Education: New York, NY, USA, 2008. [Google Scholar]
- Freiburger, G.; Holcomb, M.; Piper, D. The STARPAHC collection: Part of an archive of the history of telemedicine. J. Telemed. Telecare 2007, 13, 221–223. [Google Scholar] [CrossRef] [PubMed]
- Opportunities and Barriers for Telemedicine in the United States during the COVID-19 Emergency and Beyond. Available online: https://www.kff.org/womens-health-policy/issue-brief/opportunities-and-barriers-for-telemedicine-in-the-u-s-during-the-covid-19-emergency-and-beyond/ (accessed on 26 July 2020).
- Ludwig, S.; Zarbock, A. Coronaviruses and SARS-CoV-2: A Brief Overview. Anesthesia Analg. 2020, 131, 93–96. [Google Scholar] [CrossRef] [PubMed]
- One in 10 Americans Use Telehealth, But Nearly 75% Lack Awareness or Access, J.D. Power Finds. Retrieved. Available online: https://www.prnewswire.com/news-releases/one-in-10-americans-use-telehealth-but-nearly-75-lack-awareness-or-access-jd-power-finds-300892939.html (accessed on 29 July 2020).
- The Impact of the COVID-19 Pandemic on Outpatient Visits: A Rebound Emerges. Available online: https://www.commonwealthfund.org/publications/2020/apr/impact-covid-19-outpatient-visits (accessed on 23 September 2020).
- Nearly Half of Physicians Using Telehealth, up from Just 18% in 2018. Available online: https://www.healthcareitnews.com/news/nearly-half-physicians-using-telehealth-just-18-2018 (accessed on 23 April 2020).
- Survey: Physician Practice Patterns Changing as A Result Of COVID-19. Available online: https://link-gale-com.libproxy.txstate.edu/apps/doc/A621578229/BIC?u=txshracd2550&sid=BIC&xid=c2c99c3c (accessed on 23 April 2020).
- Telemedicine Options: The COVID-19 Pandemic Underscores the Role of Remote Patient Management. Podiatry Manag. 2020, 39, 79–80. Available online: https://eds-b-ebscohost-com.libproxy.txstate.edu/eds/pdfviewer/pdfviewer?vid=1&sid=c44ac7e7-793a-43d3-8dc5-842d219582de%40sessionmgr101 (accessed on 23 April 2020).
- Gondal, K.M.; Shaukat, S. Telemedicine in the Time of COVID-19 Pandemic. J. Coll. Phys. Surg. Pak. 2020, 30, 349–350. [Google Scholar] [CrossRef]
- Reynolds, R. Telehealth in pregnancy. Lancet Diabetes Endocrinol. 2020, 8, 459–461. [Google Scholar] [CrossRef]
- Machado, R.A.; De Souza, N.L.; Oliveira, R.M.; Júnior, H.M.; Bonan, P.R.F. Social media and telemedicine for oral diagnosis and counselling in the COVID-19 era. Oral Oncol. 2020, 105, 104685. [Google Scholar] [CrossRef]
- COVID-19 Shuts Down Nation; Family Planning Need Not Stop. Available online: https://www.reliasmedia.com/articles/146022-covid-19-shuts-down-nation-family-planning-need-not-stop (accessed on 6 July 2020).
- Canady, V.A. COVID-19 outbreak represents a new way of mental health service delivery. Ment. Heal. Wkly. 2020, 30, 1–4. [Google Scholar] [CrossRef]
- Wu, C.; Liu, Y.; Ohannessian, R.; Duong, T.A.; Odone, A. Global Telemedicine Implementation and Integration Within Health Systems to Fight the COVID-19 Pandemic: A Call to Action. JMIR Public Health Surveill. 2020, 6, e18810. [Google Scholar] [CrossRef]
- Telehealth: A New frontier in OB/GYN. Available online: https://www.contemporaryobgyn.net/view/telehealth-new-frontier-obgyn (accessed on 6 September 2020).
- COVID-19 Devastates At-Risk Populations. Available online: https://www.reliasmedia.com/articles/146066-covid-19-devastates-at-risk-populations (accessed on 6 July 2020).
- Romanick-Schmiedl, S.; Raghu, G. Telemedicine—Maintaining quality during times of transition. Nat. Rev. Dis. Prim. 2020, 6, 45. [Google Scholar] [CrossRef]
- Vidal-Alaball, J.; Acosta-Roja, R.; Hernández, N.P.; Luque, U.S.; Morrison, D.; Pérez, S.N.; Llano, J.P.; Vèrges, A.S.; Seguí, F.L.; Pastor, N.; et al. Telemedicine in the face of the COVID-19 pandemic. Atención Primaria 2020, 52, 418–422. [Google Scholar] [CrossRef]
- Wosik, J.; Fudim, M.; Cameron, B.; Gellad, Z.F.; Cho, A.; Phinney, D.; Curtis, S.; Roman, M.; Poon, E.G.; Ferranti, J.; et al. Telehealth transformation: COVID-19 and the rise of virtual care. J. Am. Med Inform. Assoc. 2020, 27, 957–962. [Google Scholar] [CrossRef] [PubMed]
- Bashshur, R.; Doarn, C.R.; Frenk, J.M.; Kvedar, J.C.; Woolliscroft, J.O. Telemedicine and the COVID-19 Pandemic, Lessons for the Future. Telemed. e-Health 2020, 26, 571–573. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spinelli, A.; Pellino, G. COVID-19 pandemic: Perspectives on an unfolding crisis. Br. J. Surg. 2020, 107, 785–787. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mann, D.; Chen, J.; Chunara, R.; A Testa, P.; Nov, O. COVID-19 transforms health care through telemedicine: Evidence from the field. J. Am. Med Informatics Assoc. 2020, 27, 1132–1135. [Google Scholar] [CrossRef]
- Aziz, A.; Zork, N.; Aubey, J.J.; Baptiste, C.D.; D’Alton, M.E.; Emeruwa, U.N.; Fuchs, K.M.; Goffman, D.; Gyamfi-Bannerman, C.; Haythe, J.H.; et al. Telehealth for High-Risk Pregnancies in the Setting of the COVID-19 Pandemic. Am. J. Perinatol. 2020, 37, 800–808. [Google Scholar] [CrossRef]
- Zhou, X.; Snoswell, C.L.; Harding, L.E.; Bambling, M.; Edirippulige, S.; Bai, X.; Smith, A.C. The Role of Telehealth in Reducing the Mental Health Burden from COVID-19. Telemed. e-Health 2020, 26, 377–379. [Google Scholar] [CrossRef] [Green Version]
- Freeman, M.P. COVID-19 From a Psychiatry Perspective: Meeting the Challenges. J. Clin. Psychiatry 2020, 81. [Google Scholar] [CrossRef]
- Shift to Telehealth Could Remain Trend After COVID-19. Available online: https://www.reliasmedia.com/articles/146176-shift-to-telehealth-could-remain-trend-after-covid-19 (accessed on 22 June 2020).
- Knopf, A. Telepsychiatry coming into its own with COVID-19. Brown Univ. Child Adolesc. Psychopharmacol. Child Adolesc. Psychopharmacol. Updat. 2020, 22, 1–3. [Google Scholar] [CrossRef] [Green Version]
- Parikh, A.; Kumar, A.A.; Jahangir, E. Cardio-Oncology Care in the Time of COVID-19 and the Role of Telehealth. JACC CardioOncol. 2020, 2, 356–358. [Google Scholar] [CrossRef]
- Rodler, S.; Apfelbeck, M.; Stief, C.; Heinemann, V.; Casuscelli, J. Lessons from the coronavirus disease 2019 pandemic: Will virtual patient management reshape uro-oncology in Germany? Eur. J. Cancer 2020, 132, 136–140. [Google Scholar] [CrossRef]
- Steingass, S.K.; Maloney-Newton, S. Telehealth Triage and Oncology Nursing Practice. Semin. Oncol. Nurs. 2020, 36, 151019. [Google Scholar] [CrossRef] [PubMed]
- Hospitals Use Telemedicine to Limit Exposures, Preserve PPE, Guide Patients to Right Setting. Available online: https://www.reliasmedia.com/articles/146050-hospitals-use-telemedicine-to-limit-exposures-preserve-ppe-guide-patients-to-right-setting (accessed on 22 June 2020).
- Jnr, B.A. Use of Telemedicine and Virtual Care for Remote Treatment in Response to COVID-19 Pandemic. J. Med Syst. 2020, 44, 1–9. [Google Scholar] [CrossRef]
- Portnoy, J.M.; Waller, M.; Elliott, T. Telemedicine in the Era of COVID-19. J. Allergy Clin. Immunol. Pract. 2020, 8, 1489–1491. [Google Scholar] [CrossRef]
- Contreras, C.M.; Metzger, G.A.; Beane, J.D.; Dedhia, P.H.; Ejaz, A.; Pawlik, T.M. Telemedicine: Patient-Provider Clinical Engagement During the COVID-19 Pandemic and Beyond. J. Gastrointest. Surg. 2020, 24, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Boxer, R.J.; Ellimoottil, C. Advantages and utilization of telemedicine. mHealth 2019, 5, 12. [Google Scholar] [CrossRef] [PubMed]
- Jobes, D.A.; Crumlish, J.A.; Evans, A.D. The COVID-19 pandemic and treating suicidal risk: The telepsychotherapy use of CAMS. J. Psychother. Integr. 2020, 30, 226–237. [Google Scholar] [CrossRef]
- Elkaddoum, R.; Haddad, F.G.; Eid, R.; Kourie, H.R. Telemedicine for cancer patients during COVID-19 pandemic: Between threats and opportunities. Future Oncol. 2020, 16, 1225–1227. [Google Scholar] [CrossRef]
- Trinidad, J.; Kroshinksy, D.; Kaffenberger, B.H.; Rojek, N. Telemedicine for inpatient dermatology consultations in response to the COVID-19 pandemic. J. Am. Acad. Dermatol. 2020, 83, e69–e71. [Google Scholar] [CrossRef]
- Incorporating telemedicine as part of COVID-19 outbreak response systems. Am. J. Manag. Care 2020, 26, 147–148. [CrossRef]
- Teledermatology and HIPAA Compliance in the Era of COVID-19. Available online: dermatologytimes.com/view/teledermatology-and-hipaa-compliance-era-covid-19 (accessed on 22 June 2020).
- Prasad, A.; Brewster, R.; Newman, J.G.; Rajasekaran, K. Optimizing your telemedicine visit during the COVID-19 pandemic: Practice guidelines for patients with head and neck cancer. Head Neck 2020, 42, 1317–1321. [Google Scholar] [CrossRef]
- Badeli, H.; Nejad, A.T.; Rad, A.H. Utilizing Telemedicine for Managing COVID-19. J. Pediatr. Nephrol. 2020, 8. [Google Scholar] [CrossRef]
- Cosic, K.; Popovic, S.; Sarlija, M.; Kesedzic, I. Impact of Human Disasters and COVID-19 Pandemic on Mental Health: Potential of Digital Psychiatry. Psychiatr. Danub. 2020, 32, 25–31. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| User | Prior to 2020 COVID-19 Pandemic | Following 2020 COVID-19 Pandemic |
|---|---|---|
| Patients |
|
|
| Providers |
|
|
| First Author, Date, Reference | Title | Publication | Observations | Themes | Service Line Addressed |
|---|---|---|---|---|---|
| Ludwig, 2020 [8] | Coronaviruses and SARS-CoV-2: A Brief Overview | Anesthesia and Analgesia |
| Infectious Disease | |
| J.D. Power, 2019 [9] | One in 10 Americans Use Telehealth, But Nearly 75% Lack Awareness or Access, J.D. Power Finds | PR Newswire |
| Multiple Specialties | |
| Eddy, 2020 [10] | Nearly half of physicians using telehealth, up from just 18% in 2018 | Healthcare IT News |
| Multiple Specialties | |
| Lehrman, 2020 [13] | Telemedicine Options: The COVID-19 pandemic underscores the role of remote patient management | Podiatry Management |
| HIPAA compliance; rapid expansion | Multiple Specialties |
| Gondal, 2020 [14] | Telemedicine in the time of COVID-19 Pandemic | Journal of the College of Physicians and Surgeons |
| “Telemedicine education; risk mitigation; convenience; lower cost; social distancing promotion; improved access” | Multiple Specialties |
| Reynolds, 2020 [15] | Telehealth in Pregnancy (Editorial) | Lancet Diabetes and Endocrinology |
| Social distancing; Self-Isolation; Risk mitigation | OB/GYN OB/GYN |
| Machado, 2020 [16] | Social Media and Telemedicine for Oral Diagnosis and Counselling in the COVID-19 Era (Editorial) | Oral Oncology |
| Social distancing; Self-Isolation; Risk mitigation | Dentistry |
| AHC Media, 2020 [17] | COVID-19 Shuts Down Nation; Family Planning Need Not Stop: Clinics resort to remote care. | Relias Media |
| “Improved access; increased reimbursements; social distancing; risk mitigation; telemedicine education” | OB/GYN |
| Canady, 2020 [18] | COVID-19 outbreak represents a new way of mental health service delivery. (Editorial) | Mental Health Weekly |
| “Telemedicine education; Social distancing promotion; improved access” | Mental Health |
| Ohannessian, 2020 [19] | Global Telemedicine Implementation and Integration Within Health Systems to Fight the COVID-19 Pandemic: A Call to Action (Editorial) | JMIR Public Health and Surveillance |
| “Improved access; telemedicine education” | Multiple Specialties |
| Lowery, 2020 [20] | Telehealth: A new frontier in OB/GYN | Contemporary OB/GYN |
| “Social distancing; convenience; lower costs; risk mitigation” | OB/GYN |
| AHC Media, 2020 [21] | COVID-19 Devastates At-Risk Populations: Telemedicine could be new normal | Relias Media |
| Risk mitigation; social distancing | Multiple Specialties |
| Romanick-Schmied, 2020 [22] | Telemedicine Maintaining Quality During Times of Transition | Nature Reviews Disease Primers |
| Improved access; rapid expansion; social distancing; convenience; risk mitigation | Multiple Specialties |
| Vidal-Alaball, 2020 [23] | Telemedicine in the Face of the COVID-19 Pandemic | Atencion Primaria |
| Improved access; rapid expansion; social distancing; lower cost; convenience | Multiple Specialties |
| Wosik, 2020 [24] | Telehealth transformation: COVID-19 and the rise of virtual care | Journal of the American Medical Informatics Association |
| Rapid expansion; social distancing | Multiple Specialties |
| Bashshur, 2020 [25] | Telemedicine and the COVID-19 Pandemic, Lessons for the Future (Editorial) | Telemedicine Journal and e-health |
| “Improved access; increased reimbursement; rapid expansion; social distancing; convenience; lower cost; risk mitigation; telemedicine education; relaxed regulations” | Multiple Specialties |
| Spinelli, 2020 [26] | COVID-19 Pandemic: Perspectives on an Unfolding Crisis | British Journal of Surgery |
| Risk mitigation; social distancing | Multiple Specialties |
| Mann, 2020 [27] | COVID-19 Transforms Health Care Through Telemedicine: Evidence From the Field | Journal of the American Medical Informatics Association |
| HIPAA compliance; increased reimbursement; rapid expansion; social distancing; patient satisfaction; risk mitigation; telemedicine education | Multiple Specialties |
| Aziz, 2020 [28] | Telehealth for High-Risk Pregnancies in the Setting of the COVID-19 Pandemic | American Journal of Perinatology |
| Mitigate risk for COVID-19 exposure; minimize patient travel | OB/GYN |
| Zhou, 2020 [29] | The Role of Telehealth in Reducing the Mental Health Burden from COVID-19 (Editorial) | Telemedicine Journal and e-health |
| Increased access; infection risk mitigation | Mental Health |
| Freeman, 2020 [30] | COVID-19 From a Psychiatry Perspective: Meeting the Challenges | The Journal of Clinical Psychiatry |
| Regulatory barrier removal, rapid expansion, improved access | Mental Health |
| AHC Media, 2020 [31] | Shift to Telehealth Could Remain Trend After COVID-19: Reproductive health remains priority. | Relias Media |
| HIPAA compliance; lower costs; patient satisfaction | OB/GYN |
| Knoph, 2020 [32] | Telepsychiatry Coming Into Its Own With COVID-19 (Editorial) | Brown University Child and Adolescent Pharmacology Update |
| “Patient satisfaction; reimbursement; improved access” | Mental Health |
| Parikh, 2020 [33] | Cardio-Oncology Care In the Time of COVID-19 and the Role of Telehealth | JACC CardioOncology |
| “Improved access; risk mitigation; convenience” | Oncology |
| Rodler, 2020 [34] | Lessons from the coronavirus disease 2019 pandemic: Will virtual patient management reshape uro-oncology in Germany? | European Journal of Cancer |
| Risk mitigation | Oncology |
| Steingass, 2020 [35] | Telehealth Triage and Oncology Nursing Practice | Seminars in Oncology Nursing |
| Telemedicine education | Oncology |
| AHC Media, 2020 [36] | Hospitals Use Telemedicine to Limit Exposures, Preserve Personal Protective Equipment (PPE), Guide Patients to Right Setting | Relias Media |
| “Improved access; HIPAA compliance; increased reimbursement; rapid expansion” | Multiple Specialties |
| Bokolo, 2020 [37] | Use of Telemedicine and Virtual Care for Remote Treatment in Response to COVID-19 Pandemic | Journal of Medical Systems |
| Rapid expansion; risk mitigation | Multiple Specialties |
| Portnoy, 2020 [38] | Telemedicine in the Era of COVID-19 (Editorial) | The Journal of Allergy and Clinical Immunology |
| “Risk mitigation; improved access; increased reimbursement; HIPAA compliance” | Multiple Specialties |
| Contreras, 2020 [39] | Telemedicine: Patient-Provider Clinical Engagement During the COVID-19 Pandemic and Beyond | Journal of Gastrointestinal Surgery |
| Increased reimbursement; relaxed regulations; improved access | Multiple Specialties |
| Boxer, 2019 [40] | Advantages and utilization of telemedicine | mHealth |
| Improved access; relaxed regulations; increased reimbursement | Multiple Specialties |
| Jobes, 2020 [41] | The COVID-19 pandemic and treating suicidal risk: The telepsychotherapy use of CAMS | Journal of Psychotherapy |
| Telemedicine education | Mental Health |
| Elkaddoum, 2020 [42] | Telemedicine for cancer patients during COVID-19 pandemic: between threats and opportunities | Future Oncology |
| Improved access; risk mitigation | Oncology |
| Trinidad, 2020 [43] | Telemedicine for inpatient dermatology consultations in response to the COVID-19 pandemic (Editorial) | Journal of the American Academy of Dermatology |
| Improved access; risk mitigation | Dermatology |
| Lovett, 2020 [44] | Incorporating Telemedicine as part of COVID-19 Outbreak Response Systems | The American Journal of Managed Care |
| “Improved access; increased reimbursement; rapid expansion; risk mitigation, relaxed regulations” | Multiple Specialties |
| Goldberg, 2020 [45] | Tele-dermatology and HIPAA compliance in the era of COVID-19. | Dermatology Times |
| HIPAA compliance | Dermatology |
| Prasad, 2020 [46] | Optimizing Your Telemedicine Visit During the COVID-19 Pandemic: Practice Guidelines for Patients With Head and Neck Cancer | Head and Neck |
| Patient/Provider Telemedicine Education | Oncology |
| Badeli, 2020 [47] | Utilizing Telemedicine for Managing COVID-19 | Journal of Pediatric Nephrology |
| “Improved access; social distancing; lower cost; patient satisfaction” | Oncology |
| Cosic, 2020 [48] | Impact of Human Disasters and COVID-19 Pandemic on Mental Health: Potential of Digital Psychiatry | Psychiatria Danubina |
| Improved access; telemedicine education | Mental Health |
| Effectiveness Themes | Article Citation Number | Incidence of Occurrence (n = 43) | Probability of Occurrence |
|---|---|---|---|
| Improved Access | [1,13,17,20,23,24,25,29,30,31,32,33,35,37,38,39,40,41,42,44,47] | 21 | 48% |
| Risk Mitigation | [1,13,15,16,17,20,21,22,23,25,27,28,29,33,34,36,37,39,43] | 19 | 43% |
| Social Distancing Promotion | [13,15,16,17,20,21,23,24,27,35,36,37,41,44] | 14 | 32% |
| Rapid Telemedicine Expansion | [13,22,23,24,25,26,30,32,33,35,37,44] | 12 | 27% |
| HIPAA Compliance/Relaxed Regulations | [13,25,26,30,31,37,38,39,40,47,48] | 11 | 25% |
| Telemedicine Education | [13,17,19,20,35,37,38,44,45,46] | 10 | 23% |
| Increased or Similar Reimbursements | [13,17,25,37,38] [39,40,47] | 8 | 18% |
| Convenience | [13,20,21,23,24,31,33] | 7 | 16% |
| Lower Cost | [13,20,21,24,38,41] | 6 | 14% |
| Patient Satisfaction | [31,32,37,41] | 4 | 9% |
| Service Line | Implementation Successes |
|---|---|
| Dermatology | Rapid diagnosis and treatment, increased access, reduced risk of infection, minimization of PPE and medical supply utilization, addressed health care disparities for underserved and rural populations. |
| OB/GYN | A typical virtual visit includes the pregnant woman utilizing home monitoring supplies to track measures such as fetal heart rate, maternal blood pressure, and fundal height. Specialists are able to view ultrasounds and other examinations through available technology, often in real-time. Home monitoring is also possible for certain high-risk conditions. Clinics quickly shifted to phone screening and initial consultations, as well as videoconferences with patients. Some clinics provided contraception renewals and new prescriptions through telemedicine. From a family planning perspective, telehealth visits have been a positive experience that both patients and providers favor. Clinics can phone triage patients before a scheduled visit to determine whether the visit can be done by telephone visit, or synchronous or asynchronous telemedicine. GLOW was a randomized trial of a weight management intervention delivered by telephone during a pregnancy with an aim of reducing gestational weight gain in women with overweight or obesity—goals of implementation were to consolidate in-person prenatal screening, surveillance, and examinations into fewer in-person visits while maintaining patient access to ongoing antenatal care and subspecialty consultations via telehealth virtual visits. |
| Oncology | Less consumption of PPE, can ensure patients are adhering to given recommendations, patients can address new symptoms, fears, or questions with providers. Cardio-oncology patients can be evaluated regularly, e.g., blood pressure readings, weight scales, or Cardio Micro Electro Mechanical System (CardioMEMS). Strict quarantine observation, reduced clinic visits, survivorship care planning, patient education. |
| Mental Health | Supporting both physical and psychosocial needs irrespective of geographic locations. Children with anxiety or significant trauma feel more comfortable than they would with in-person therapy. In response to the sudden need to provide tele-psychotherapy services, organizations quickly developed and offered free resources, clinical guidance, and synchronous and asynchronous access to online presentations to thousands of mental health providers around the world. Prescriptions can now be made (but not for other controlled substances, such as ADHD medications) after a thorough assessment through a live interactive video. Collaborative Assessment and Management of Suicidality (CAMS) protocols were created to provide support, guidance, and resources. Increase in patient and provider satisfaction rates. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Betancourt, J.A.; Rosenberg, M.A.; Zevallos, A.; Brown, J.R.; Mileski, M. The Impact of COVID-19 on Telemedicine Utilization Across Multiple Service Lines in the United States. Healthcare 2020, 8, 380. https://doi.org/10.3390/healthcare8040380
Betancourt JA, Rosenberg MA, Zevallos A, Brown JR, Mileski M. The Impact of COVID-19 on Telemedicine Utilization Across Multiple Service Lines in the United States. Healthcare. 2020; 8(4):380. https://doi.org/10.3390/healthcare8040380
Chicago/Turabian StyleBetancourt, Jose A., Matthew A. Rosenberg, Ashley Zevallos, Jon R. Brown, and Michael Mileski. 2020. "The Impact of COVID-19 on Telemedicine Utilization Across Multiple Service Lines in the United States" Healthcare 8, no. 4: 380. https://doi.org/10.3390/healthcare8040380