
Evaluation of Membrane Ultrafiltration and Residual Chlorination as a Decentralized Water Treatment Strategy for Ten Rural Healthcare Facilities in Rwanda

 ,
,
Abstract
:1. Introduction
2. Experimental Section
2.1. Study Setting
2.2. Intervention
2.2.1. Inclusion Criteria and Site Selection
2.2.2. Water and Power Supply at Participating HCF
2.2.3. Water Purification Systems
2.2.4. Training and Start-Up
2.3. Program Monitoring
2.3.1. Data Collection and Monitoring
2.3.2. Data Analysis
2.3.3. Ethics
3. Results and Discussion
3.1. Water Purification System Performance
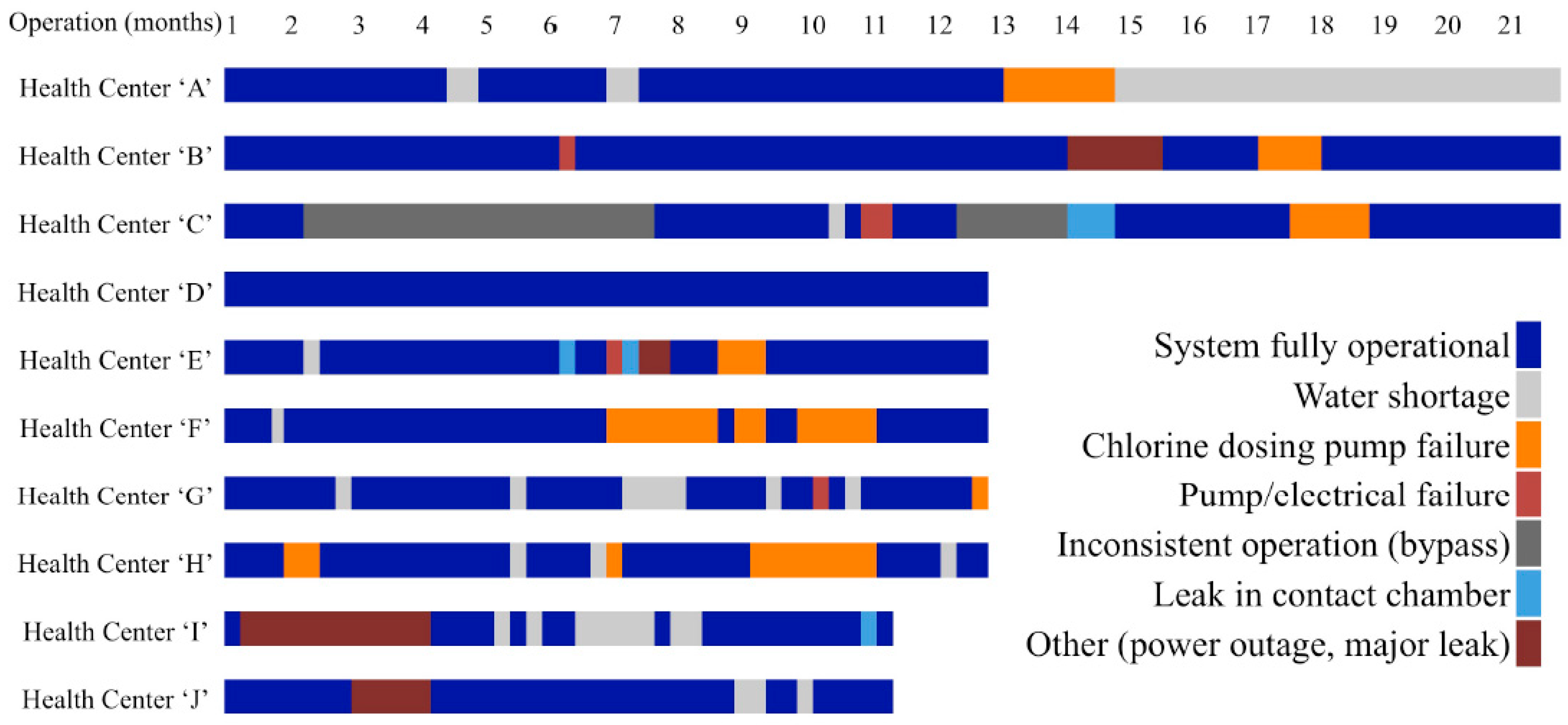
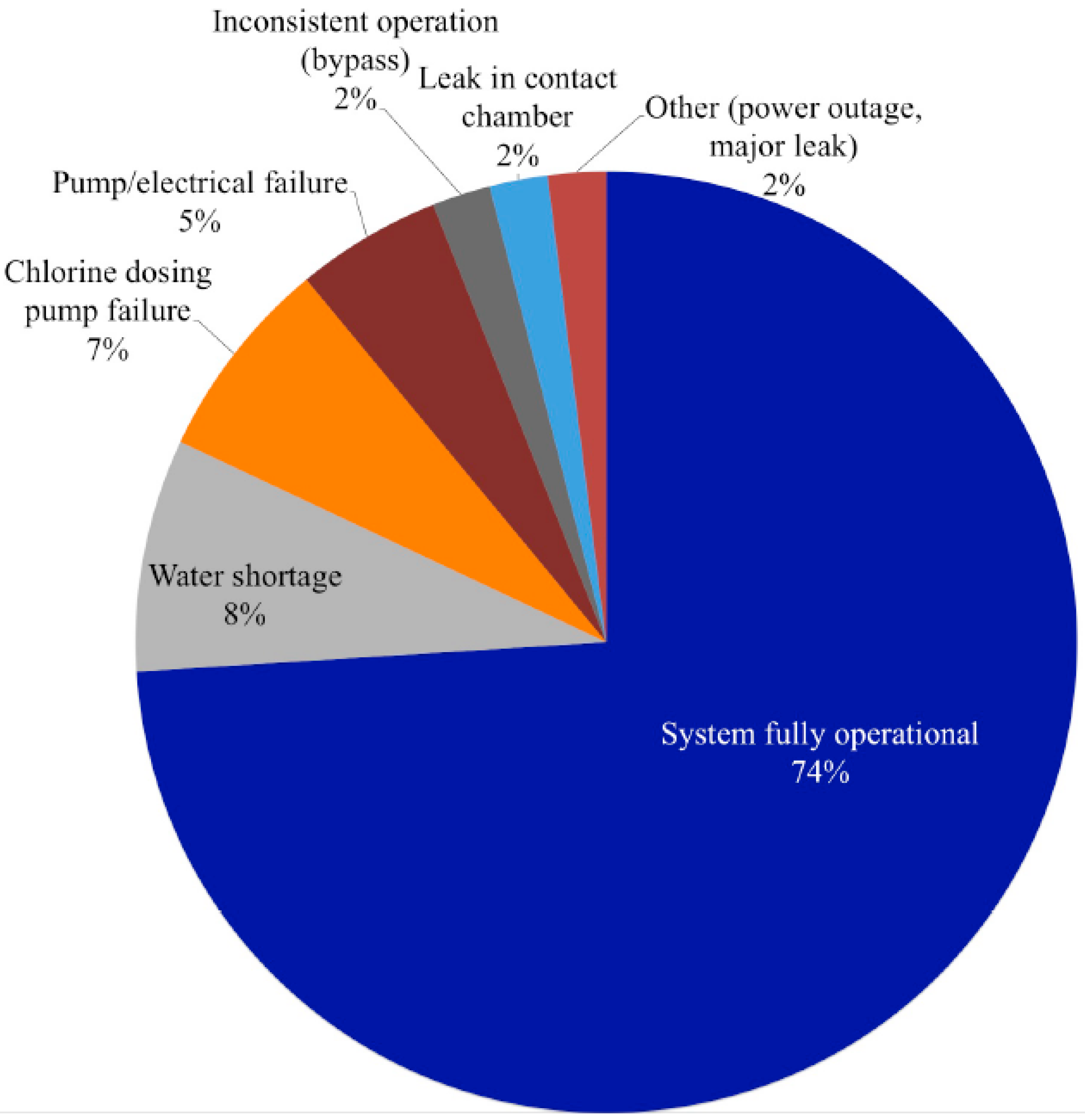
3.1.1. Operations and Maintenance


| Treatment Interruption * | Water Interruption ** | |||||
|---|---|---|---|---|---|---|
| Reason for service interruption | User bypass | Chlorine dosing pump failure | Water shortage | Pump/electric failure | Underground contact chamber leak | Other 1 |
| Number of events | 2 | 12 | 22 | 4 | 5 | 4 |
| Number of sites at which events occurred | 1 | 7 | 8 | 4 | 4 | 4 |
| Days of interruption (proportion of total observed interruption period) | 91 (0.08) | 315 (0.28) | 367 (0.32) | 218 (0.19) | 75 (0.07) | 64 (0.06) |
| Mean time to failure in days (range) 2 | N/A | 330 (61–542) | N/A | 161 (2–390) | 300 (171–427) | N/A |
| Mean time for repairs to be completed in days (range) 2 | N/A | 24 (1–37) | N/A | 55 (15–125) | 18 (4–53) | N/A |
3.1.2. Treatment Interruptions

3.1.3. Water Interruptions
3.1.4. Time to Resolve System Interruptions
3.2. Water Quality
3.2.1. Quality of Water in Samples of Chlorinated UF Permeate Collected Immediately Following the WTS
3.2.2. Quality of Water at Points of Use
| WTS Fully Operational n (%) | Treatment Interruption * n (%) | Water Interruption ** n (%) | |
|---|---|---|---|
| Number of samples | 446 | 96 | 50 |
| E. coli (MPN †/100 mL) | |||
| <1 | 432 (96.9) | 93 (96.9) | 39 (78.0) |
| 1–10 | 11 (2.5) | 1 (1.0) | 2 (4.0) |
| >10 | 3 (0.6) | 2 (1.2) | 9 (18.0) |
| Total Coliforms (MPN †/100 mL) | |||
| <1 | 397 (89.2) | 79 (82.3) | 31 (62.0) |
| 1–10 | 26 (5.8) | 7 (7.3) | 3 (6.0) |
| >10 | 22 (5.0) | 10 (10.4) | 16 (32.0) |
| Number of samples | 440 | 84 | 47 |
| Free chlorine residual (mg/L) †† | |||
| Mean | 0.12 | 0.02 | 0.03 |
| Median | 0.02 | 0.02 | 0.02 |
| Range | <0.02–2.20 | <0.02–0.17 | <0.02–0.35 |
| Total chlorine residual (mg/L) †† | |||
| Mean | 0.18 | 0.06 | 0.08 |
| Median | 0.06 | 0.04 | 0.04 |
| Range | <0.02–2.20 | <0.02–0.26 | <0.02–0.48 |
| Turbidity (NTU) | |||
| Mean | 1.13 | 1.22 | 3.36 |
| Median | 0.70 | 0.74 | 1.34 |
| Range | 0.02–26.63 | 0.05–6.92 | 0.39–49.61 |
| WTS Fully Operational | Treatment Interruption * | |||
|---|---|---|---|---|
| TAPS n (%) | Containers n (%) | Taps n (%) | Containers n (%) | |
| Number of samples | 369 | 77 | 83 | 13 |
| E. coli (MPN **/100 mL) | ||||
| <1 | 363 (98.4) | 69 (89.6) | 81 (97.6) | 12 (92.3) |
| 1–10 | 6 (1.6) | 5 (6.5) | 1 (1.2) | 0 (0) |
| >10 | 0 (0.0) | 3 (3.9) | 1 (1.2) | 1 (7.69) |
| Total Coliforms (MPN **/100 mL) | ||||
| <1 | 344 (93.5) † | 53 (68.8) | 70 (84.3) † | 9 (69.2) |
| 1–10 | 16 (4.4) | 10 (13.0) | 6 (7.23) | 1 (7.69) |
| >10 | 8 (2.1) | 14 (18.2) | 7 (8.43) | 3 (23.8) |
| Number of samples | 364 | 76 | 83 | 13 |
| Free chlorine residual (mg/L) †† | ||||
| Mean | 0.13 | 0.11 | 0.02 | <0.02 |
| Median | 0.02 | 0.02 | <0.02 | <0.02 |
| Range | <0.02–2.20 | <0.02–2.20 | <0.02–0.17 | <0.02–0.04 |
| Total chlorine residual (mg/L) †† | ||||
| Mean | 0.19 | 0.15 | 0.06 | 0.02 |
| Median | 0.07 | 0.04 | 0.04 | 0.02 |
| Range | <0.02–2.20 | <0.02–2.20 | <0.02–0.26 | <0.02–0.09 |
| Turbidity (NTU) | ||||
| Mean | 1.09 | 1.30 | 1.17 | 1.49 |
| Median | 0.71 | 0.62 | 0.74 | 0.74 |
| Range | 0.02–20.07 | 0.12–26.6 | 0.05–6.92 | 0.12–5.76 |
3.2.3. Quality of Water in Storage Containers
| ≥1 total coliform MPN †/100 mL | ≥ 1 E. coli MPN †/100 mL | |||
|---|---|---|---|---|
| Point of Use Type | n (%) | OR (95% CI) | n (%) | OR (95% CI) |
| Tap | 24 (6.5) | ref | 6 (1.6) | ref |
| Container * | 24 (31.2) | 6.49 (3.43–12.25) | 8 (10.4) | 7.01 (2.36–20.85) |
| ≥ 1 total coliform MPN † /100 mL | ≥ 1 E. coli MPN †/100 mL | |||
|---|---|---|---|---|
| System Status | n (%) | OR (95% CI) | n (%) | OR (95% CI) |
| WTS Fully Operational | 48 (11) | ref | 14 (3) | ref |
| Treatment Interruption ** | 17 (18) | 1.78 (0.97–3.25) | 3 (3) | 1.00 (0.28–3.53) |
| Water Interruption *** | 19 (38) | 5.07 (2.66–9.66) | 11 (22) | 8.70 (3.70–20.46) |
3.3. Discussion
3.3.1. Determinants of MF System Performance

{kind=link}
{kind=link}
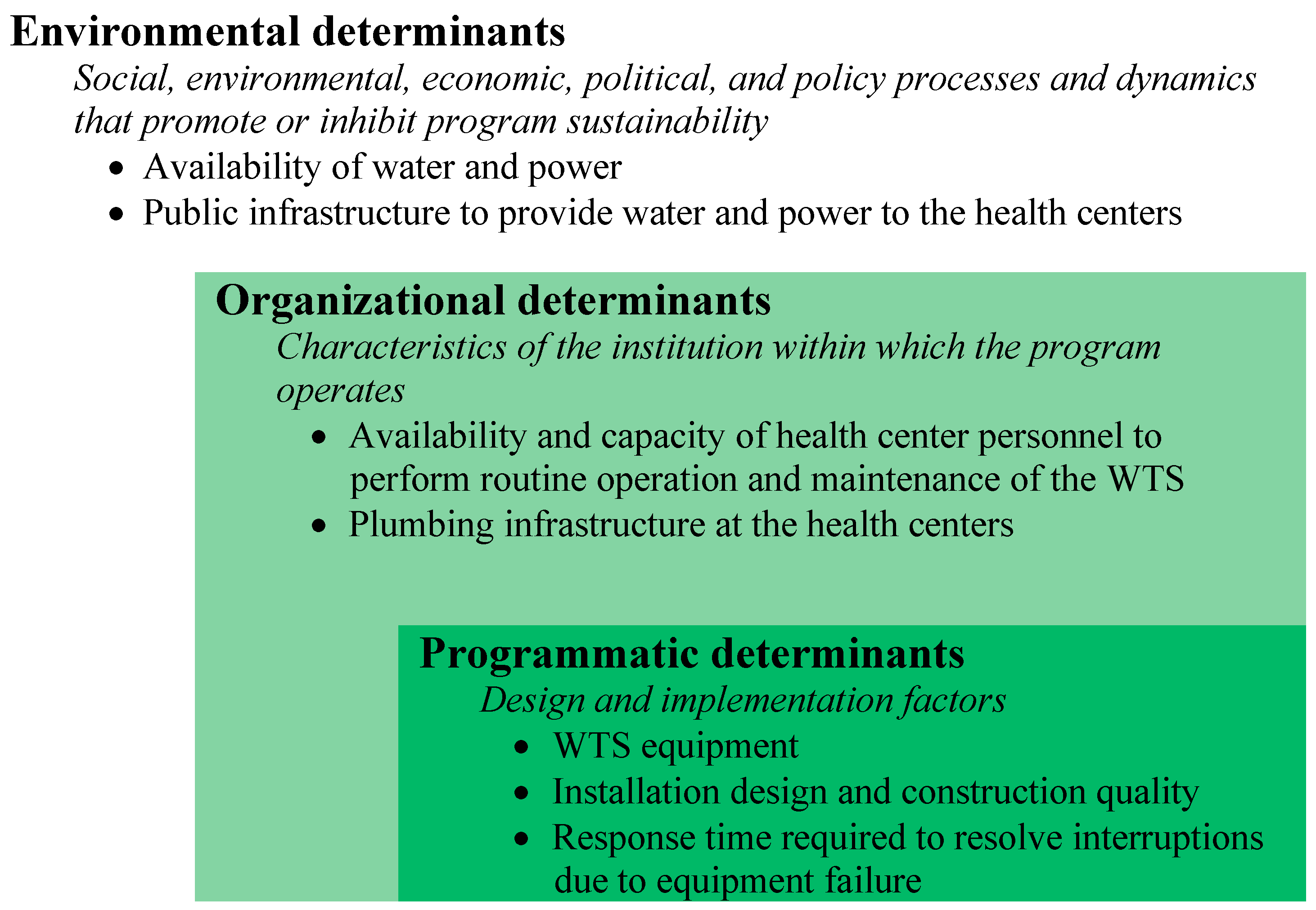{kind=link}
3.3.2. Factors Associated with Successful Operation of MF Systems
3.3.3. Factors Associated with Interruptions in Water Provision and Water Treatment
3.3.4 Factors Affecting Water Quality at Point of Use
3.3.5. Study Strengths and Limitations
4. Conclusions
Supplementary Files
Supplementary File 1Acknowledgments
Author Contributions
Conflicts of Interest
References
- Adams, J.; Bartram, J.; Chartier, Y. Essential Environmental Health Standards in Health Care; World Health Organization: Geneva, Switzerland, 2008; Available online: http://www.who.int/water_sanitation_health/hygiene/settings/ehs_health_care.pdf.pdf (accessed on 10 October 2015).
- Benova, L.; Cumming, O.; Campbell, O.M.R. Systematic review and meta-analysis: Association between water and sanitation environment and maternal mortality. Trop. Med. Int. Health 2014, 19, 368–387. [Google Scholar] [CrossRef] [PubMed]
- Hsia, R.Y.; Mbembati, N.A.; Macfarlane, S.; Kruk, M.E. Access to emergency and surgical care in sub-Saharan Africa: The infrastructure gap. Health Policy Plan. 2012, 27, 234–244. [Google Scholar] [CrossRef] [PubMed]
- Shordt, K.; Smet, E. Getting It Right: Improving Maternal Health Through Water, Sanitation & Hygiene; SIMAVI: 2012. Available online: http://simavi.org/wp-content/uploads/2015/03/Simavi-Publicatie-Getting-It-Right.pdf (accessed on 10 October 2015).
- Velleman, Y.; Mason, E.; Graham, W.; Benova, L.; Chopra, M.; Campbell, O.M.R.; Gordon, B.; Wijesekera, S.; Hounton, S.; Mills, J.E.; et al. From joint thinking to joint action: A call to action on improving water, sanitation, and hygiene for maternal and newborn health. PLoS Med. 2014, 11. [Google Scholar] [CrossRef] [PubMed]
- Campbell, O.M.R.; Benova, L.; Gon, G.; Afsana, K.; Cumming, O. Getting the basics right—The role of water, sanitation and hygiene in maternal and reproductive health: A conceptual framework. Trop. Med. Int. Health 2015, 20, 252–267. [Google Scholar] [CrossRef] [PubMed]
- Cronk, R.; Bartram, J.; Boisson, S.; Gordon, B.; Fewtrell, L.; Montgomery, M. Water, Sanitation and Hygiene in Health Care Facilities: Status in Low and Middle Income Countries and Way Forward; World Health Organization: Geneva, Switzerland, 2015; Available online: http://apps.who.int/iris/bitstream/10665/154588/1/9789241508476_eng.pdf?ua=1 (accessed on 10 October 2015).
- Lee, E.J.; Schwab, K.J. Deficiencies in drinking water distribution systems in developing countries. J. Water Health 2005, 3, 109–127. [Google Scholar] [PubMed]
- Moe, C.L.; Rheingans, R.D. Global challenges in water, sanitation and health. J. Water Health 2006, 4, 41–57. [Google Scholar] [PubMed]
- Bain, R.; Cronk, R.; Wright, J.; Yang, H.; Slaymaker, T.; Bartram, J. Fecal contamination of drinking-water in low- and middle-income countries: A systematic review and meta-analysis. PLOS Med. 2014, 11. [Google Scholar] [CrossRef] [PubMed]
- Wright, J.; Gundry, S.; Conroy, R. Household drinking water in developing countries: A systematic review of microbiological contamination between source and point-of-use. Trop. Med. Int. Health 2004, 9, 106–117. [Google Scholar] [CrossRef] [PubMed]
- Gunther, I.; Schipper, Y. Pumps, Germs and storage: The impact of improved water containers on water quality and health. Health Econ. 2013, 22, 757–774. [Google Scholar] [CrossRef] [PubMed]
- Peter-Varbanets, M.; Zurbruegg, C.; Swartz, C.; Pronk, W. Decentralized systems for potable water and the potential of membrane technology. Water Res. 2009, 43, 245–265. [Google Scholar] [CrossRef] [PubMed]
- Zheng, X.; Yu, M.; Liang, H.; Qi, L.; Zheng, H.; Exler, H.; Schier, W.; Frechen, F.-B. Membrane technology for municipal drinking water plants in China: Progress and prospects. Desalination Water Treat. 2012, 49, 281–295. [Google Scholar] [CrossRef]
- Sima, L.C.; Elimelech, M. More than a drop in the bucket: Decentralized membrane-based drinking water refill stations in Southeast Asia. Environ. Sci. Technol. 2013, 47, 7580–7588. [Google Scholar] [CrossRef] [PubMed]
- Schafer, A.I.; Hughes, G.; Richards, B.S. Renewable energy powered membrane technology: A leapfrog approach to rural water treatment in developing countries? Renew. Sustain. Energy Rev. 2014, 40, 542–556. [Google Scholar] [CrossRef]
- Lee, N.H.; Amy, G.; Croue, J.P.; Buisson, H. Identification and understanding of fouling in low-pressure membrane (MF/UF) filtration by natural organic matter (NOM). Water Res. 2004, 38, 4511–4523. [Google Scholar] [CrossRef] [PubMed]
- Huang, H.; Lee, N.; Young, T.; Gary, A.; Lozier, J.C.; Jacangelo, J.G. Natural organic matter fouling of low-pressure, hollow-fiber membranes: Effects of NOM source and hydrodynamic conditions. Water Res. 2007, 41, 3823–3832. [Google Scholar] [CrossRef] [PubMed]
- Howe, K.J.; Clark, M.M. Fouling of microfiltration and ultrafiltration membranes by natural waters. Environ. Sci. Technol. 2002, 36, 3571–3576. [Google Scholar] [CrossRef] [PubMed]
- Iannelli, R.; Ripari, S.; Casini, B.; Buzzigoli, A.; Privitera, G.; Verani, M.; Carducci, A. Feasibility assessment of surface water disinfection by ultrafiltration. Water Sci. Technol. Water Supply 2014, 14, 522–531. [Google Scholar] [CrossRef]
- Boulestreau, M.; Hoa, E.; Peter-Verbanets, M.; Pronk, W.; Rajagopaul, R.; Lesjean, B. Operation of gravity-driven ultrafiltration prototype for decentralised water supply. Desalination Water Treat. 2012, 42, 125–130. [Google Scholar] [CrossRef]
- Peter-Varbanets, M.; Gujer, W.; Pronk, W. Intermittent operation of ultra-low pressure ultrafiltration for decentralized drinking water treatment. Water Res. 2012, 46, 3272–3282. [Google Scholar] [CrossRef] [PubMed]
- Arnal, J.M.; Garcia-Fayos, B.; Sancho, M.; Verdu, G.; Lora, J. Design and Installation of a decentralized drinking water system based on ultrafiltration in Mozambique. Desalination 2010, 250, 613–617. [Google Scholar] [CrossRef]
- Arnal, J.M.; Sancho, M.; Garcia Fayos, B.; Lora, J.; Verdu, G. Aquapot: UF real applications for water potabilization in developing countries: Problems, location and solutions adopted. Desalination 2007, 204, 316–321. [Google Scholar] [CrossRef]
- Molelekwa, G.F.; Mukhola, M.S.; Van der Bruggen, B.; Luis, P. Preliminary studies on membrane filtration for the production of potable water: A case of tshaanda rural village in South Africa. PLoS ONE 2014, 9. [Google Scholar] [CrossRef] [PubMed]
- United Nations Children’s Fund (UNICEF). Final Report on WASH Survey for Households, Schools and Health Centres in the Districts of Burera, Musanze, Nyabihu and Rubavu, Rwanda; UNICEF Rwanda: Kigali, Rwanda, June 2011. [Google Scholar]
- General Electric Water & Process Technologies. Product Fact SHEET for ZeeWeed pressurized Ultrafiltration Model ZW1500-600; GE Corporation: Fairfield, CT, USA, 2013; p. 2. [Google Scholar]
- Water Aid Rwanda. Water Hygiene and Sanitation Baseline Study in Bugesera District, Rwanda; WaterAid: Kigali, Rwanda, November 2010. [Google Scholar]
- General Electric Water & Process Technologies. Filters and Membranes: Zeeweed Hollow-Fiber Membranes: Zeeweed 1500. Available online: http://www.gewater.com/products/zeeweed-1500-membrane.html (accessed on 23 October 2014).
- Huttinger, A.; Personal communication with General Electric Foundation and General Electric Water and Process Technologies, Kigali, Rwanda. 14 March 2012.
- Huttinger, A. Water, Sanitation and Hygiene Infrastructure and Quality in Rural Healthcare Facilities in Rwanda. J. Health Public Policy 2015. (submitted). [Google Scholar]
- Scheirer, M.A.; Dearing, J.W. An agenda for research on the sustainability of public health programs. Am. J. Public Health 2011, 101, 2059–2067. [Google Scholar] [CrossRef] [PubMed]
- Bossert, T.J. Can they get along without us—Sustainability of donor-supported health projects in Central-America and Africa. Soc. Sci. Med. 1990, 30, 1015–1023. [Google Scholar] [CrossRef]
- Sarriot, E.G.; Winch, P.J.; Ryan, L.J.; Bowie, J.; Kouletio, M.; Swedberg, E.; LeBan, K.; Edison, J.; Welch, R.; Pacque, M.C. A Methodological approach and framework for sustainability assessment in NGO-implemented primary health care programs. Int. J. Health Plann. Manage. 2004, 19, 23–41. [Google Scholar] [CrossRef] [PubMed]
- Olsen, I.T. Sustainability of health care: A framework for analysis. Health Policy Plann 1998, 13, 287–295. [Google Scholar] [CrossRef]
- United Nations Water (UN-Water). Global Annual Assessment of Sanitation and Drinking-water 2012 Report: The Challenge of Extending and Sustaining Services; World Health Organization: Geneva, Switzerland, 2012; Available online: http://apps.who.int//iris/bitstream/10665/44849/1/9789241503365_eng.pdf?ua=1 (accessed on 10 October 2015).
- Burr, P.; Fonseca, C. Applying a life-cycle costs approach to water: Costs and service levels in rural and small town areas in Andhra Pradesh (India), Burkina Faso, Ghana and Mozambique; IRC: The Hague, Netherlands, 2013; Available online: http://www.ircwash.org/sites/default/files/20130208_8_wp_water_web_2.pdf (accessed on 10 October 2015).
- Carter, R.; Harvey, E.; Casey, V. User financing of rural handpump water services. In Pumps, Pipes and Promises: Costs, Finances and Accountability for Sustainable WASH Services; IRC International Water and Sanitation Centre: The Hague, The Netherlands, 2010; Available online: http://www.ircwash.org/sites/default/files/Carter-2010-User.pdf (accessed on 10 October 2015).
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huttinger, A.; Dreibelbis, R.; Roha, K.; Ngabo, F.; Kayigamba, F.; Mfura, L.; Moe, C. Evaluation of Membrane Ultrafiltration and Residual Chlorination as a Decentralized Water Treatment Strategy for Ten Rural Healthcare Facilities in Rwanda. Int. J. Environ. Res. Public Health 2015, 12, 13602-13623. https://doi.org/10.3390/ijerph121013602
Huttinger A, Dreibelbis R, Roha K, Ngabo F, Kayigamba F, Mfura L, Moe C. Evaluation of Membrane Ultrafiltration and Residual Chlorination as a Decentralized Water Treatment Strategy for Ten Rural Healthcare Facilities in Rwanda. International Journal of Environmental Research and Public Health. 2015; 12(10):13602-13623. https://doi.org/10.3390/ijerph121013602
Chicago/Turabian StyleHuttinger, Alexandra, Robert Dreibelbis, Kristin Roha, Fidel Ngabo, Felix Kayigamba, Leodomir Mfura, and Christine Moe. 2015. "Evaluation of Membrane Ultrafiltration and Residual Chlorination as a Decentralized Water Treatment Strategy for Ten Rural Healthcare Facilities in Rwanda" International Journal of Environmental Research and Public Health 12, no. 10: 13602-13623. https://doi.org/10.3390/ijerph121013602