
Comparison of the Ability to Predict Mortality between the Injury Severity Score and the New Injury Severity Score: A Meta-Analysis


Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy and Study Selection
2.2. Inclusion and Exclusion Criteria
2.3. Data Extraction and Quality Assessment
2.4. Statistical Analysis
3. Results
3.1. Search Results and Characteristics of Studies
3.2. Test of the Threshold Effect and Heterogeneity
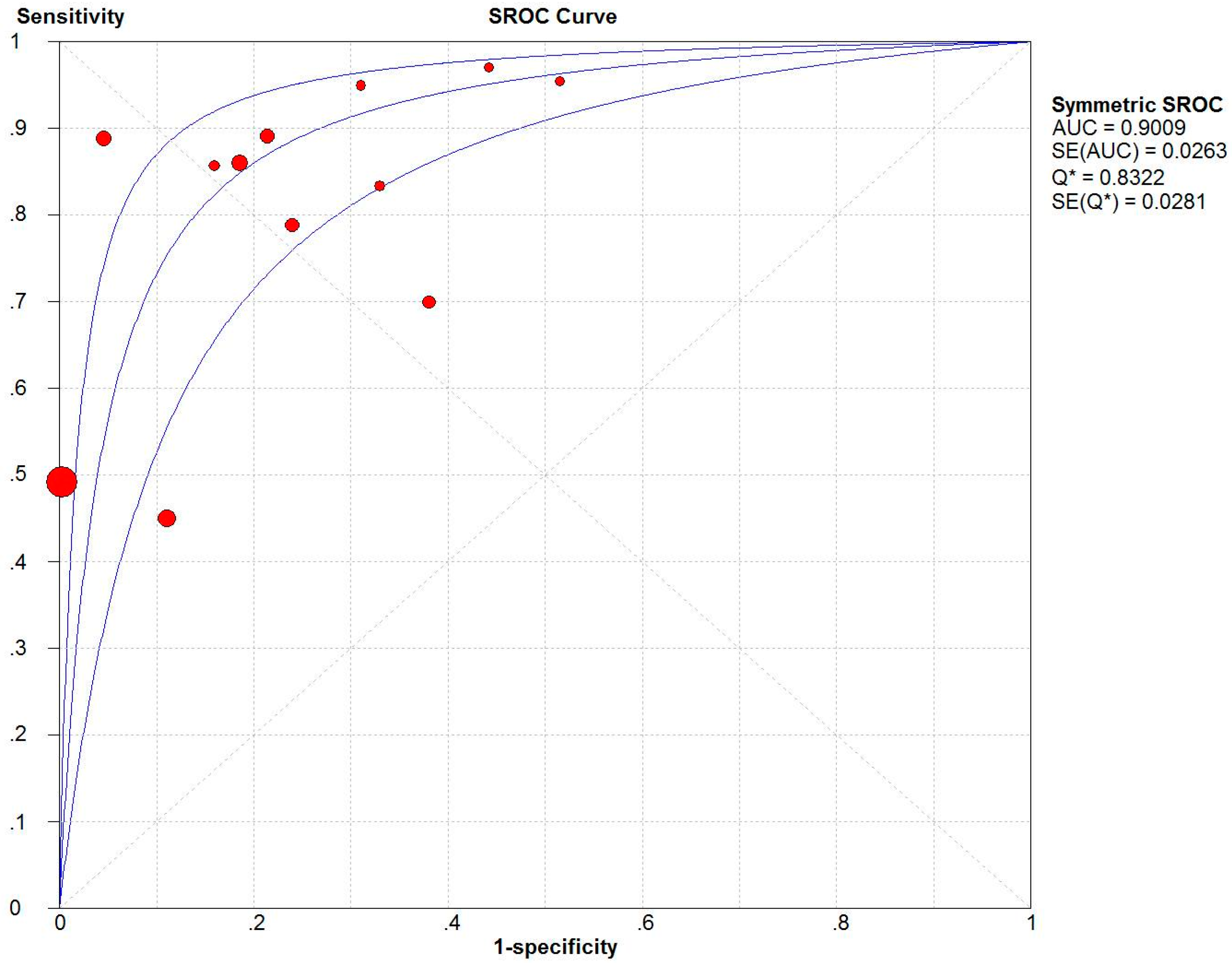
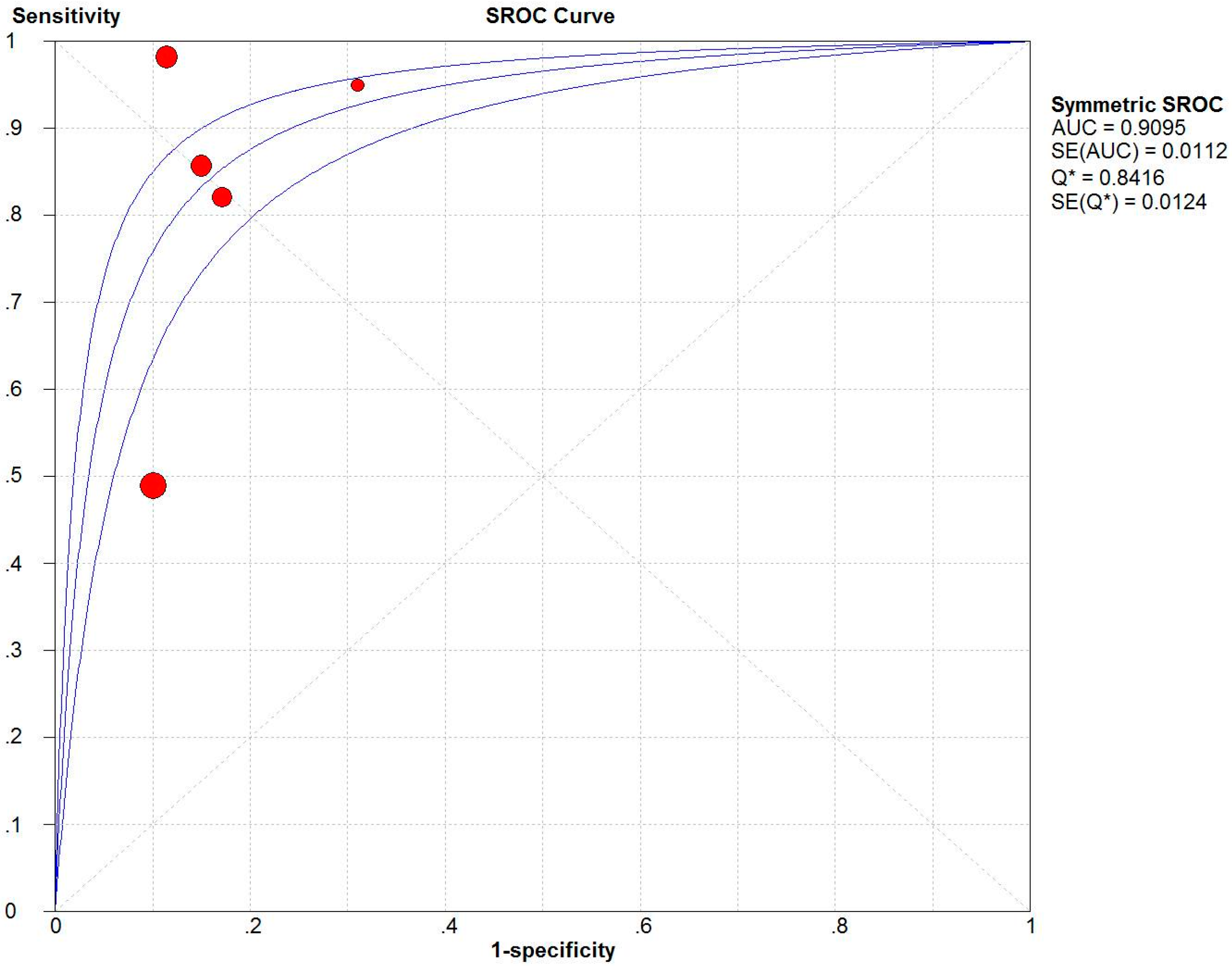
3.3. Overall Analysis
3.4. Meta-Regression and Sensitivity Analyses
3.5. Subgroup Meta-Analysis
4. Discussion
4.1. ISS vs. NISS
4.2. Factors Affecting the Accuracy of the ISS
4.3. Source of Heterogeneity
4.4. Limitations
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Salehi, O.; Tabibzadeh Dezfuli, S.A.; Namazi, S.S.; Dehghan Khalili, M.; Saeedi, M. A New Injury Severity Score for predicting the length of hospital stay in multiple trauma patients. Trauma Mon. 2016, 21, e20349. [Google Scholar] [CrossRef] [PubMed]
- Chiang, W.K.; Huang, S.T.; Chang, W.H.; Huang, M.Y.; Chien, D.K.; Tsai, C.H. Mortality factors regarding the Injury Severity Score in elderly trauma patients. Int. J. Gerontol. 2012, 6, 192–195. [Google Scholar] [CrossRef]
- WHO Global Alliance for Care of the Injured. Available online: http://www.who.int/emergencycare/gaci/gaci_flyer_web.pdf?ua=1 (accessed on 13 August 2016).
- Husum, H.; Strada, G. Injury Severity Score versus New Injury Severity Score for penetrating injuries. Prehospital Dis. Med. 2002, 17, 27–32. [Google Scholar]
- Baker, S.P.; O’Neill, B.; Haddon, W., Jr.; Long, W.B. The Injury Severity Score: A method for describing patients with multiple injuries and evaluating emergency care. J. Trauma 1974, 14, 187–196. [Google Scholar] [CrossRef] [PubMed]
- Osler, T.; Baker, S.P.; Long, W. A modification of the Injury Severity Score that both improves accuracy and simplifies scoring. J. Trauma Inj. Infect. Crit. Care 1997, 43, 922–926. [Google Scholar] [CrossRef]
- Balogh, Z.; Offner Pj Fau-Moore, E.E.; Moore Ee Fau-Biffl, W.L.; Biffl, W.L. NISS predicts postinjury multiple organ failure better than the ISS. J. Trauma 2000, 48, 624–627. [Google Scholar] [CrossRef] [PubMed]
- Whitaker, I.Y.; Gennari Td Fau-Whitaker, A.L.; Whitaker, A.L. The difference between ISS and NISS in a series of trauma patients in Brazil. Annu. Proc. Assoc. Adv. Automot. Med. 2003, 47, 301–309. [Google Scholar] [PubMed]
- Jamulitrat, S.; Sangkerd, P.; Thongpiyapoom, S.; Na Narong, M. A comparison of mortality predictive abilities between NISS and ISS in trauma patients. J. Med. Assoc. Thail. Chotmaihet Thangphaet 2001, 84, 1416–1421. [Google Scholar]
- Harwood, P.J.; Giannoudis Pv Fau-Probst, C.; Probst C Fau-Van Griensven, M.; Van Griensven, M.; Fau-Krettek, C.; Krettek, C.; Fau-Pape, H.-C.; Pape, H.C. Which AIS based scoring system is the best predictor of outcome in orthopaedic blunt trauma patients? J. Trauma 2006, 60, 334–340. [Google Scholar] [CrossRef] [PubMed]
- Sutherland, A.G.; Johnston, A.T.; Hutchison, J.D. The new injury severity score: Better prediction of functional recovery after musculoskeletal injury. Value Health J. Int. Soc. Pharm. Outcomes Res. 2006, 9, 24–27. [Google Scholar] [CrossRef] [PubMed]
- Hwang, J.Y.; Lee, K.H.; Kim, O.H.; Cha, K.C.; Cha, Y.S.; Kim, H.; Hwang, S.O. Validity of mortality prediction of ISS andnewinjury severity score in the severe trauma patients by injury mechanism. J. Emerg. Med. 2012, 43, 939–940. [Google Scholar] [CrossRef]
- Domingues Cde, A.; de Sousa, R.M.; Nogueira Lde, S.; Poggetti, R.S.; Fontes, B.; Munoz, D. The role of the New Trauma and Injury Severity Score (NTRISS) for survival prediction. Rev. Esc. Enferm. USP 2011, 45, 1353–1358. [Google Scholar] [CrossRef] [PubMed]
- Tohira, H.; Jacobs, I.; Mountain, D.; Gibson, N.; Yeo, A. Systematic review of predictive performance of injury severity scoring tools. Scand. J. Trauma Resusc. Emerg. Med. 2012, 20. [Google Scholar] [CrossRef] [PubMed]
- Kuhls, D.A.; Malone, D.L.; McCarter, R.J.; Napolitano, L.M. Predictors of mortality in adult trauma patients: the physiologic trauma score is equivalent to the Trauma and Injury Severity Score. J. Am. Coll. Surg. 2002, 194, 695–704. [Google Scholar] [CrossRef]
- Sullivan, T.; Haider, A.; DiRusso, S.M.; Nealon, P.; Shaukat, A.; Slim, M.; Michel, M.D. Prediction of mortality in pediatric trauma patients: New Injury Severity Score outperforms Injury Severity Score in the severely injured. J. Trauma Inj. Infect. Crit. Care 2003, 55, 1083–1088. [Google Scholar] [CrossRef] [PubMed]
- Tay, S.Y.; Sloan, E.P.; Zun, L.; Zaret, P. Comparison of the New Injury Severity Score and the Injury Severity Score. J. Trauma Inj. Infect. Crit. Care 2004, 56, 162–164. [Google Scholar] [CrossRef] [PubMed]
- Bulut, M.; Koksal, O.; Korkmaz, A.; Turan, M.; Ozguc, H. Childhood falls: Characteristics, outcome, and comparison of the Injury Severity Score and New Injury Severity Score. Emerg. Med. J. 2006, 23, 540–545. [Google Scholar] [CrossRef] [PubMed]
- Zhao, X.G.; Ma, Y.F.; Zhang, M.; Gan, J.X.; Xu, S.W.; Jiang, G.Y. Comparison of the New Injury Severity Score and the Injury Severity Score in multiple trauma patients. Chin. J. Traumatol. Engl. Ed. 2008, 11, 368–371. [Google Scholar] [CrossRef]
- Moore, L.; Lavoi, A.; Le Sage, N.; Bergeron, E.; Emond, M.; Abdous, B. Consensus or data-derived anatomic injury severity scoring? J. Trauma Inj. Infect. Crit. Care 2008, 64, 420–426. [Google Scholar] [CrossRef] [PubMed]
- Tamim, H.; Al Hazzouri, A.Z.; Mahfoud, Z.; Atoui, M.; El-Chemaly, S. The Injury Severity Score or the New Injury Severity Score for predicting mortality, intensive care unit admission and length of hospital stay: Experience from a university hospital in a developing country. Injury 2008, 39, 115–120. [Google Scholar] [CrossRef] [PubMed]
- Whiting, P.; Rutjes, A.W.; Reitsma, J.B.; Bossuyt, P.M.; Kleijnen, J. The development of QUADAS: A tool for the quality assessment of studies of diagnostic accuracy included in systematic reviews. BMC Med. Res. Methodol. 2003, 3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zamora, J.; Abraira, V.; Muriel, A.; Khan, K.; Coomarasamy, A. Meta-DiSc: A software for meta-analysis of test accuracy data. BMC Med. Res. Methodol. 2006, 6. [Google Scholar] [CrossRef] [PubMed]
- Turina, D.; Sustic, A.; Ticac, Z.; Dirlic, A.; Krstulovic, B.; Glavas, A.; Orlic, V. War head injury score: An outcome prediction model in war casualties with acute penetrating head injury. Mil. Med. 2001, 166, 331–334. [Google Scholar] [PubMed]
- Schiff, M.A.; Holt, V.L. The Injury Severity Score in pregnant trauma patients: Predicting placental abruption and fetal death. J. Trauma 2002, 53, 946–949. [Google Scholar] [CrossRef] [PubMed]
- Lefering, R. Development and validation of the revised injury severity classification score for severely injured patients. Eur. J. Trauma Emerg. Surg. 2009, 35, 437–447. [Google Scholar] [CrossRef] [PubMed]
- Eftekhar, B.; Zarei, M.R.; Ghodsi, M.; MoezArdalan, K.; Zargar, M.; Ketabchi, E. Comparing logistic models based on modified GCS motor component with other prognostic tools in prediction of mortality: Results of study in 7226 trauma patients. Injury 2005, 36, 900–904. [Google Scholar] [CrossRef] [PubMed]
- Woodford, M.R.; Mackenzie, C.F.; DuBose, J.; Hu, P.; Kufera, J.; Hu, E.Z.; Dutton, R.P.; Scalea, T.M. Continuously recorded oxygen saturation and heart rate during prehospital transport outperform initial measurement in prediction of mortality after trauma. J. Trauma Acute Care Surg. 2012, 72, 1006–1011. [Google Scholar] [CrossRef] [PubMed]
- Aydin, S.A.; Bulut, M.; Ozguc, H.; Ercan, I.; Turkmen, N.; Eren, B.; Esen, M. Should the New Injury Severity Score replace the Injury Severity Score in the trauma and Injury Severity Score? Ulus. Travma Acil Cerrahi Derg.-Turk. J. Trauma Emerg. Surg. TJTES 2008, 14, 308–312. [Google Scholar]
- Eryllmaz, M.; Durusu, M.; Mentes, O.; Ozer, T.; Killc, S.; Ersoy, G.; Altlnel, O.; Kalemoglu, M.; Torer, N. Comparison of trauma scores for adults who fell from height as survival predictivity. Turk. J. Med. Sci. 2009, 39, 247–252. [Google Scholar]
- Ahun, E.; Koksal, O.; Sigirli, D.; Torun, G.; Donmez, S.S.; Armagan, E. Value of the Glasgow coma scale, age, and arterial blood pressure score for predicting the mortality of major trauma patients presenting to the emergency department. Ulus. Travma Acil Cerrahi Derg.-Turk. J. Trauma Emerg. Surg. TJTES 2014, 20, 241–247. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, M.D. Validation of the summary ROC for diagnostic test meta-analysis: A Monte Carlo simulation. Acad. Radiol. 2003, 10, 25–31. [Google Scholar] [CrossRef]
- Lijmer, J.G.; Bossuyt, P.M.; Heisterkamp, S.H. Exploring sources of heterogeneity in systematic reviews of diagnostic tests. Stat. Med. 2002, 21, 1525–1537. [Google Scholar] [CrossRef] [PubMed]
- Gallagher, E.J. Clinical utility of likelihood ratios. Ann. Emerg. Med. 1998, 31, 391–397. [Google Scholar] [CrossRef]
- Glas, A.S.; Lijmer, J.G.; Prins, M.H.; Bonsel, G.J.; Bossuyt, P.M.M. The diagnostic odds ratio: A single indicator of test performance. J. Clin. Epidemiol. 2003, 56, 1129–1135. [Google Scholar] [CrossRef]
- Champion, H.R.; Copes, W.S.; Sacco, W.J.; Lawnick, M.M.; Bain, L.W.; Gann, D.S.; Gennarelli, T.; Mackenzie, E. A new characterization of injury severity. J. Trauma 1990, 30, 539–545; discussion 45–46. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| First Author | Country | Sample Size | Mortality | Year | Age (Years) | Male (%) | Tool | Cut-Off Value | TP | FP | FN | TN | AUC | Sen (%) | Spe (%) | Quality |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Chiang [2] | China (Taiwan) | 955 | 0.0450 | 2012 | ≥18 | 59.8 | ISS | 15 | 37 | 169 | 6 | 743 | 0.877 | 85.70 | 81.50 | 11 |
| Eftekhar [27] | Iran | 7208 | 0.0380 | 2005 | Mean, 32.5 | 76.0 | ISS | 44 a | 135 | 14 | 139 | 6920 | 0.944 | 49.20 | 99.80 | 10 |
| Lefering [26] | Germany | 1206 | 0.1660 | 2009 | Mean, 38.2 | 74.0 | ISS | 40 | 90 | 111 | 110 | 895 | 0.786 | 45.00 | 89.00 | 10 |
| NISS | 49 | 98 | 101 | 102 | 905 | 0.804 | 49.00 | 90.00 | ||||||||
| Bulut [18] | Turkey | 749 | 0.0360 | 2006 | <14 | 64.0 | ISS | 22 | 24 | 33 | 3 | 689 | 0.962 | 90.50 | 95.40 | 9 |
| NISS | 22 | 27 | 82 | 0 | 640 | 0.950 | 100.00 | 88.70 | ||||||||
| Woodford [28] | America | 120 | 0.0700 | 2012 | Mean, 42 | 63.0 | ISS | 44 a | 7 | 18 | 1 | 94 | 0.910 | 88.00 | 84.00 | 8 |
| Aydin [29] | Turkey | 550 | 0.2160 | 2008 | >16 | 78.0 | ISS | 21 | 106 | 92 | 13 | 339 | 0.907 | 89.10 | 78.70 | 10 |
| NISS | 25 | 102 | 76 | 17 | 431 | 0.914 | 85.70 | 82.40 | ||||||||
| Turina [24] | Croatia | 43 b | 0.2300 | 2001 | Mean, 30 | 93.0 | ISS | 20 | 10 | 17 | 0 | 16 | 0.750 | 100.00 | 49.00 | 8 |
| 41 c | 0.3900 | 2001 | Mean, 38 | 90.2 | ISS | 24 | 16 | 11 | 0 | 14 | 0.780 | 100.00 | 56.00 | |||
| Schiff [25] | America | 294 | 0.0340 | 2002 | Mean, 27.6 | 0.0 | ISS | 4 | 7 | 108 | 3 | 176 | 0.740 | 70.00 | 62.00 | 9 |
| Domingues [13] | Brazil | 533 | 0.2310 | 2011 | Mean, 38 | 80.5 | ISS | 44 a | 97 | 98 | 26 | 312 | 0.900 | 79.00 | 76.00 | 10 |
| NISS | 54 a | 101 | 70 | 22 | 340 | 0.920 | 82.00 | 83.00 | ||||||||
| Eryllmaz [30] | Turkey | 87 | 0.1034 | 2009 | Mean, 25 | 67.0 | ISS | 31.5 | 9 | 24 | 0 | 54 | 0.910 | 100.00 | 69.20 | 10 |
| NISS | 31.5 | 9 | 24 | 0 | 54 | 0.915 | 100.00 | 69.20 | ||||||||
| Ahun [31] | Turkey | 100 | 0.1200 | 2014 | Mean, 40.35 | 77.0 | ISS | 16 | 10 | 29 | 2 | 59 | 0.816 | 83.33 | 67.05 | 10 |
| Tool | Spearman Correlation Coefficient | p-Value |
|---|---|---|
| ISS | 0.517 | 0.085 |
| NISS | 0.300 | 0.624 |
| Tool | Sensitivity (95% CI) | Specificity (95% CI) | PLR (95% CI) | NLR (95% CI) | DOR (95% CI) |
|---|---|---|---|---|---|
| ISS | 0.64 (0.61–0.68) | 0.93 (0.93–0.94) | 5.11 (3.12–8.37) | 0.27 (0.19–0.40) | 27.75 (9.93–77.53) |
| NISS | 0.71 (0.66–0.75) | 0.87 (0.86–0.88) | 5.22 (3.84–7.08) | 0.20 (0.08–0.52) | 24.74 (10.19–60.07) |
| Variables | Coefficient | p-Value | RDOR (95% CI) |
|---|---|---|---|
| Mortality | −4.271 | 0.4823 | 0.01 (0.00–16,071.86) |
| Cut-off value | 0.022 | 0.6215 | 1.02 (0.92–1.13) |
| Quality | −0.191 | 0.6542 | 0.83 (0.31–2.23) |
| Number | 0.001 | 0.0805 | 1.00 (1.00–1.00) |
| First Author | Sensitivity | I2 of Sensitivity (%) |
|---|---|---|
| None a | 0.64 | 93.2 |
| Turina [24] b | 0.64 | 93.4 |
| Domingues [13] | 0.62 | 93.2 |
| Lefering [26] | 0.70 | 91.6 |
| Bulut [18] | 0.64 | 93.4 |
| Schiff [25] | 0.64 | 93.8 |
| Subgroup | I2 of Sensitivity (%) | I2 of Specificity (%) |
|---|---|---|
| All | 0.64 (93.2) | 0.93 (99.3) |
| Mortality < 0.1 | 0.58 (90.0) | 0.96 (99.6) |
| Mortality ≥ 0.1 | 0.69 (94.5) | 0.82 (93.7) |
| Sample size < 100 | 1.00 (0.0) | 0.62 (56.8) |
| Sample size ≥ 100 | 0.63 (93.8) | 0.94 (99.5) |
| Cut-off value < 44 | 0.69 (93.1) | 0.83 (97.0) |
| Cut-off value ≥ 44 | 0.59 (94.2) | 0.98 (99.6) |
| Developed country | 0.47 (71.6) | 0.83 (98.0) |
| Developing country | 0.70 (93.3) | 0.95 (99.4) |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Deng, Q.; Tang, B.; Xue, C.; Liu, Y.; Liu, X.; Lv, Y.; Zhang, L. Comparison of the Ability to Predict Mortality between the Injury Severity Score and the New Injury Severity Score: A Meta-Analysis. Int. J. Environ. Res. Public Health 2016, 13, 825. https://doi.org/10.3390/ijerph13080825
Deng Q, Tang B, Xue C, Liu Y, Liu X, Lv Y, Zhang L. Comparison of the Ability to Predict Mortality between the Injury Severity Score and the New Injury Severity Score: A Meta-Analysis. International Journal of Environmental Research and Public Health. 2016; 13(8):825. https://doi.org/10.3390/ijerph13080825
Chicago/Turabian StyleDeng, Qiangyu, Bihan Tang, Chen Xue, Yuan Liu, Xu Liu, Yipeng Lv, and Lulu Zhang. 2016. "Comparison of the Ability to Predict Mortality between the Injury Severity Score and the New Injury Severity Score: A Meta-Analysis" International Journal of Environmental Research and Public Health 13, no. 8: 825. https://doi.org/10.3390/ijerph13080825