Comparative Effectiveness of Published Interventions for Elderly Fall Prevention: A Systematic Review and Network Meta-Analysis

 ,
,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
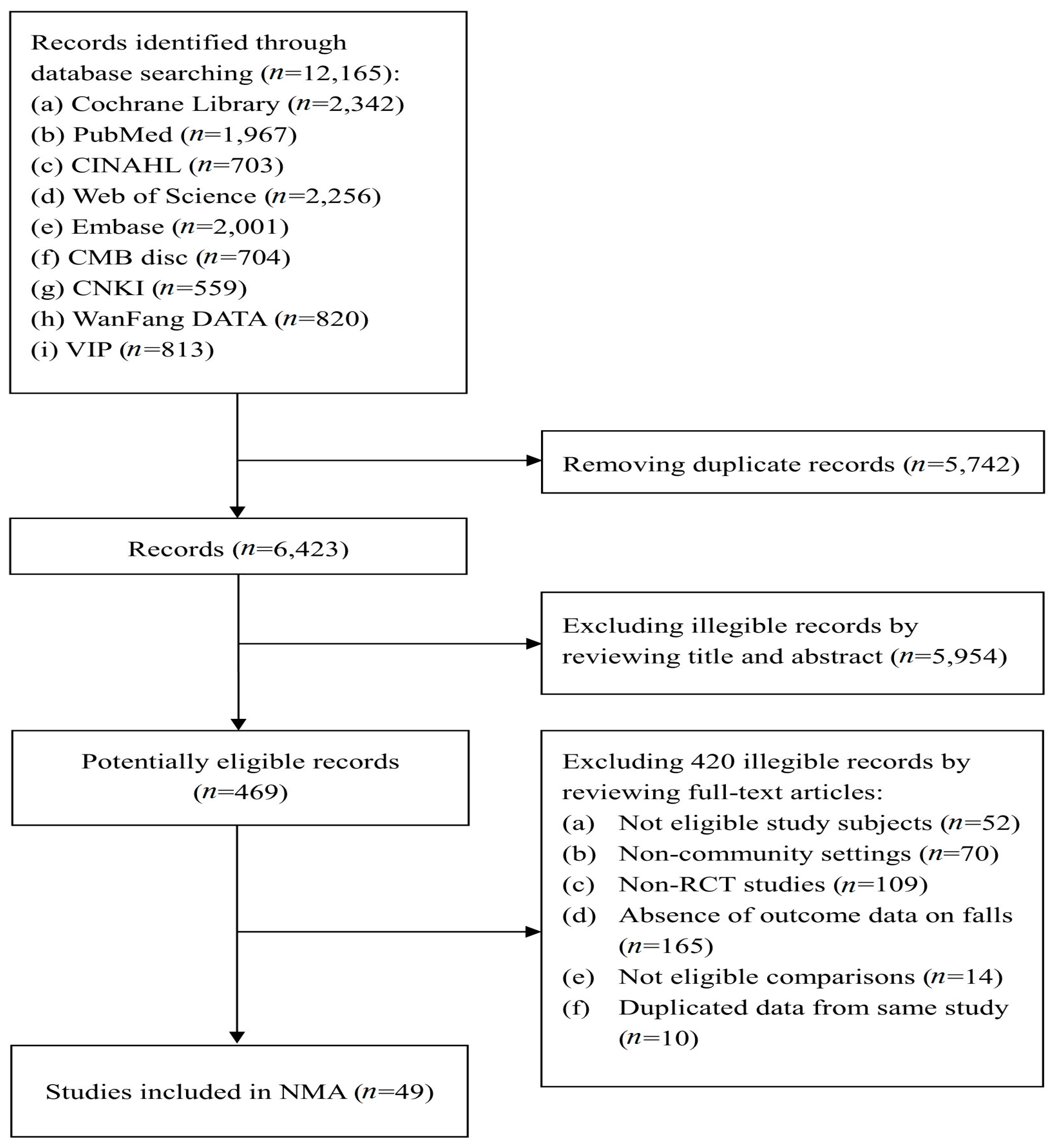
2.1. Search Strategy and Selection Criteria
2.2. Data Analysis
2.3. Role of the Funding Sources
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Conflicts of Interest
References
- WHO Global Report on Falls Prevention in Older Age. Available online: http://www.who.int/ageing/publications/Falls_prevention7March.pdf?ua=1 (accessed on 10 February 2018).
- Gelbard, R.; Inaba, K.; Okoye, O.T.; Morrell, M.; Saadi, Z.; Lam, L.; Talving, P.; Demetriades, D. Falls in the elderly: A modern look at an old problem. Am. J. Surg. 2014, 208, 249–253. [Google Scholar] [CrossRef] [PubMed]
- Campbell, A.J.; Reinken, J.; Allan, B.C.; Martinez, G.S. Falls in old age: A study of frequency and related clinical factors. Age Ageing 1981, 10, 264–270. [Google Scholar] [CrossRef] [PubMed]
- Carty, C.P.; Cronin, N.J.; Nicholson, D.; Lichtwark, G.A.; Mills, P.M.; Kerr, G.; Cresswell, A.G.; Barrett, R.S. Reactive stepping behaviour in response to forward loss of balance predicts future falls in community-dwelling older adults. Age Ageing 2015, 44, 109–115. [Google Scholar] [CrossRef] [PubMed]
- Chang, V.C.; Do, M.T. Risk factors for falls among seniors: Implications of gender. Am. J. Epidemiol. 2015, 181, 521–531. [Google Scholar] [CrossRef] [PubMed]
- Prudham, D.; Evans, J.G. Factors associated with falls in the elderly: A community study. Age Ageing 1981, 10, 141–146. [Google Scholar] [CrossRef] [PubMed]
- Alexander, B.H.; Rivara, F.P.; Wolf, M.E. The cost and frequency of hospitalization for fall-related injuries in older adults. Am. J. Public Health 1992, 82, 1020–1023. [Google Scholar] [CrossRef] [PubMed]
- Preventing Falls: How to Develop Community-Based Fall Prevention Programs for Older Adults. Available online: http://www.mtpinnacle.com/pdfs/cdc_guide-a.pdf (accessed on 10 February 2018).
- Vieira, E.R.; Palmer, R.C.; Chaves, P.H. Prevention of falls in older people living in the community. BMJ 2016, 353, i1419. [Google Scholar] [CrossRef] [PubMed]
- Tricco, A.C.; Thomas, S.M.; Veroniki, A.A.; Hamid, J.S.; Cogo, E.; Strifler, L.; Khan, P.A.; Robson, R.; Sibley, K.M.; MacDonald, H.; et al. Comparisons of interventions for preventing falls in older adults: A systematic review and meta-analysis. JAMA 2017, 318, 1687–1699. [Google Scholar] [CrossRef] [PubMed]
- Petridou, E.T.; Manti, E.G.; Ntinapogias, A.G.; Negri, E.; Szczerbinska, K. What works better for community-dwelling older people at risk to fall? A meta-analysis of multifactorial versus physical exercise-alone interventions. J. Aging Health 2009, 21, 713–729. [Google Scholar] [CrossRef] [PubMed]
- Goodwin, V.A.; Abbott, R.A.; Whear, R.; Bethel, A.; Ukoumunne, O.C.; Thompson-Coon, J.; Stein, K. Multiple component interventions for preventing falls and fall-related injuries among older people: Systematic review and meta-analysis. BMC Geriatr. 2014, 14, 15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Campbell, A.J.; Robertson, M.C. Rethinking individual and community fall prevention strategies: A meta-regression comparing single and multifactorial interventions. Age Ageing 2007, 36, 656–662. [Google Scholar] [CrossRef] [PubMed]
- EI-Khoury, F.; Cassou, B.; Charles, M.A.; Dargent-Molina, P. The effect of fall prevention exercise programmes on fall induced injuries in community dwelling older adults: Systematic review and meta-analysis of randomised controlled trials. BMJ 2013, 347, f6234. [Google Scholar] [CrossRef]
- Robertson, M.C.; Gillespie, L.D. Fall Prevention in Community-Dwelling Older Adults. JAMA 2013, 309, 1406–1407. [Google Scholar] [CrossRef] [PubMed]
- Stubbs, B.; Brefka, S.; Denkinger, M.D. What works to prevent falls in community-dwelling older adults? Umbrella review of meta-analyses of randomized controlled trials. Phys. Ther. 2015, 95, 1095–1110. [Google Scholar] [CrossRef] [PubMed]
- Glenny, A.M.; Altman, D.G.; Song, F.; Sakarovitch, C.; Deeks, J.J.; D’Amico, R.; Bradburn, M.; Eastwood, A.J. Indirect comparisons of competing interventions. Health Technol. Assess. 2005, 9, 1–134. [Google Scholar] [CrossRef] [PubMed]
- Hubbard, S.; Cooper, N.; Kendrick, D.; Young, B.; Wynn, P.M.; He, Z.; Miller, P.; Achana, F.; Sutton, A. Network meta-analysis to evaluate the effectiveness of interventions to prevent falls in children under age 5 years. Inj. Prev. 2015, 21, 98–108. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Carlin, B.P.; Neaton, J.D.; Soon, G.G.; Nie, L.; Kane, R.; Virnig, B.A.; Chu, H. Network meta-analysis of randomized clinical trials: Reporting the proper summaries. Clin. Trials 2014, 11, 246–262. [Google Scholar] [CrossRef] [PubMed]
- Gillespie, L.D.; Robertson, M.C.; Gillespie, W.J.; Sherrington, C.; Gates, S.; Clemson, L.M.; Lamb, S.E. Interventions for preventing falls in older people living in the community. Cochrane Database Syst. Rev. 2012, 9, CD007146. [Google Scholar] [CrossRef] [PubMed]
- Vlaeyen, E.; Coussement, J.; Leysens, G.; Van der Elst, E.; Delbaere, K.; Cambier, D.; Denhaerynck, K.; Goemaere, S.; Wertelaers, A.; Dobbels, F.; et al. Characteristics and effectiveness of fall prevention programs in nursing homes: A systematic review and meta-analysis of randomized controlled trials. J. Am. Geriatr. Soc. 2015, 63, 211–221. [Google Scholar] [CrossRef] [PubMed]
- Hill-Westmoreland, E.E.; Soeken, K.; Spellbring, A.M. A meta-analysis of fall prevention programs for the elderly: How effective are they? Nurs. Res. 2002, 51, 1–8. [Google Scholar] [CrossRef] [PubMed]
- The Effectiveness of Interventions to Prevent Falls in Elderly People over Age 60 Years: A Network Meta-Analysis. Available online: http://www.crd.york.ac.uk/PROSPERO/display_record.asp?ID=CRD42016027779 (accessed on 27 September 2017).
- Hutton, B.; Salanti, G.; Caldwell, D.M.; Chaimani, A.; Schmid, C.H.; Cameron, C.; Ioannidis, J.P.; Straus, S.; Thorlund, K.; Jansen, J.P.; et al. The PRISMA extension statement for reporting of systematic reviews incorporating network meta-analyses of health care interventions: Checklist and explanations. Ann. Intern. Med. 2015, 162, 777–784. [Google Scholar] [CrossRef] [PubMed]
- Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0. Available online: http://handbook.cochrane.org (accessed on 10 September 2017).
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials. Control. Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef]
- Dias, S.; Sutton, A.J.; Ades, A.E.; Welton, N.J. Evidence synthesis for decision making 2: A generalized linear modeling framework for pairwise and network meta-analysis of randomized controlled trials. Med. Decis. Mak. 2013, 33, 607–617. [Google Scholar] [CrossRef] [PubMed]
- Hong, H.; Chu, H.; Zhang, J.; Carlin, B.P. A Bayesian missing data framework for generalized multiple outcome mixed treatment comparisons. Res. Synth. Methods 2016, 7, 6–22. [Google Scholar] [CrossRef] [PubMed]
- Chaimani, A.; Higgins, J.P.; Mavridis, D.; Spyridonos, P.; Salanti, G. Graphical Tools for Network Meta-Analysis in STATA. PLoS ONE 2013, 8, e76654. [Google Scholar] [CrossRef] [PubMed]
- Salanti, G.; Ades, A.E.; Ioannidis, J.P. Graphical methods and numerical summaries for presenting results from multiple-treatment meta-analysis: An overview and tutorial. J. Clin. Epidemiol. 2011, 64, 163–171. [Google Scholar] [CrossRef] [PubMed]
- Lu, G.B.; Ades, A.E. Assessing evidence inconsistency in mixed treatment comparisons. J. Am. Stat. Assoc. 2006, 101, 447–459. [Google Scholar] [CrossRef]
- Measure the Fit of the Model in R. Available online: http://www.mtm.uoi.gr/images/5.BayesDiagnoshelp.pdf (accessed on 12 August 2017).
- Spiegelhalter, D.J.; Best, N.G.; Carlin, B.K.; van der Linde, A. Bayesian measures of model complexity and fit. J. R. Statist. Soc. B 2002, 64, 583–639. [Google Scholar] [CrossRef]
- Salanti, G.; Marinho, V.; Higgins, J.P. A case study of multiple-treatments meta-analysis demonstrates that covariates should be considered. J. Clin. Epidemiol. 2009, 62, 857–864. [Google Scholar] [CrossRef] [PubMed]
- White, I.R.; Barrett, J.K.; Jackson, D.; Higgins, J.P. Consistency and inconsistency in network meta-analysis: Model estimation using multivariate meta-regression. Res. Synth. Methods 2012, 3, 111–125. [Google Scholar] [CrossRef] [PubMed]
- Ansai, J.H.; Aurichio, T.R.; Gonçalves, R.; Rebelatto, J.R. Effects of two physical exercise protocols on physical performance related to falls in the oldest old: A randomized controlled trial. Geriatr. Gerontol. Int. 2016, 16, 429. [Google Scholar] [CrossRef] [PubMed]
- Barker, A.L.; Talevski, J.; Bohensky, M.A.; Brand, C.A.; Cameron, P.A.; Morello, R.T. Feasibility of Pilates exercise to decrease falls risk: A pilot randomized controlled trial in community-dwelling older people. Clin. Rehabil. 2016, 30, 984–996. [Google Scholar] [CrossRef] [PubMed]
- Bischoff-Ferrari, H.A.; Orav, E.J.; Dawson-Hughes, B. Effect of cholecalciferol plus calcium on falling in ambulatory older men and women: A 3-year randomized controlled trial. Arch. Intern. Med. 2006, 166, 424–430. [Google Scholar] [CrossRef] [PubMed]
- Blalock, S.J.; Casteel, C.; Roth, M.T.; Ferreri, S.; Demby, K.B.; Shankar, V. Impact of enhanced pharmacologic care on the prevention of falls: A randomized controlled trial. Am. J. Geriatr. Pharmacother. 2010, 8, 428–440. [Google Scholar] [CrossRef] [PubMed]
- Cai, Y. Observation on the Effect of nursing intervention for fall among elderly adults in rural community. Med. Inf. 2014, 27, 375. [Google Scholar] [CrossRef]
- Clemson, L.; Cumming, R.G.; Kendig, H.; Swann, M.; Heard, R.; Taylor, K. The Effectiveness of a Community-based program for reducing the incidence of falls in the elderly: A Randomized Trial. J. Am. Geriatr. Soc. 2004, 52, 1487–1494. [Google Scholar] [CrossRef] [PubMed]
- Clemson, L.; Singh, M.F.; Bundy, A.; Cumming, R.G.; Weissel, E.; Munro, J.; Manollaras, K.; Black, D. LiFE Pilot Study: A randomised trial of balance and strength training embedded in daily life activity to reduce falls in older adults. Aust. Occup. Ther. J. 2010, 57, 42–50. [Google Scholar] [CrossRef] [PubMed]
- Close, J.; Ellis, M.; Hooper, R.; Glucksman, E.; Jackson, S.; Swift, C. Prevention of falls in the elderly trial (PROFET): A randomised controlled trial. Lancet 1999, 353, 93–97. [Google Scholar] [CrossRef]
- Cornillon, E.; Blanchon, M.A.; Ramboatsisetraina, P.; Braize, C.; Beauchet, O.; Dubost, V.; Blanc, P.; Gonthier, R. Effectiveness of falls prevention strategies for elderly subjects who live in the community with performance assessment of physical activities (before-after). Ann. Readapt. Med. Phys. 2002, 45, 493–504. [Google Scholar] [CrossRef]
- Cumming, R.G.; Thomas, M.; Szonyi, G.; Salkeld, G.; O’Neill, E.; Westbury, C.; Frampton, G. Home visits by an occupational therapist for assessment and modification of environmental hazards: A randomized trial of falls prevention. J. Am. Geriatr. Soc. 1999, 47, 1397–1402. [Google Scholar] [CrossRef] [PubMed]
- Cumming, R.G.; Ivers, R.; Clemson, L.; Cullen, J.; Hayes, M.F.; Tanzer, M.; Mitchell, P. Improving vision to prevent falls in frail older people: A randomized trial. J. Am. Geriatr. Soc. 2007, 55, 175–181. [Google Scholar] [CrossRef] [PubMed]
- Dorresteijn, T.A.; Zijlstra, G.A.; Ambergen, A.W.; Delbaere, K.; Vlaeyen, J.W.; Kempen, G.I. Effectiveness of a home-based cognitive behavioral program to manage concerns about falls in community-dwelling, frail older people: Results of a randomized controlled trial. BMC Geriatr. 2016, 16, 2. [Google Scholar] [CrossRef] [Green Version]
- Dukas, L.; Bischoff, H.A.; Lindpaintner, L.S.; Schacht, E.; Birkner-Binder, D.; Damm, T.N.; Thalmann, B.; Stähelin, H.B. Alfacalcidol reduces the number of fallers in a community-dwelling elderly population with a minimum calcium intake of more than 500 mg daily. J. Am. Geriatr. Soc. 2004, 52, 230–236. [Google Scholar] [CrossRef] [PubMed]
- Elley, C.R.; Robertson, M.C.; Garrett, S.; Kerse, N.M.; McKinlay, E.; Lawton, B.; Moriarty, H.; Moyes, S.A.; Campbell, A.J. Effectiveness of a falls-and-fracture nurse coordinator to reduce falls: A randomized, controlled trial of at-risk older adults. J. Am. Geriatr. Soc. 2008, 56, 1383–1389. [Google Scholar] [CrossRef] [PubMed]
- Fairhall, N.; Sherrington, C.; Lord, S.R.; Kurrle, S.E.; Langron, C.; Lockwood, K.; Monaghan, N.; Aggar, C.; Cameron, I.D. Effect of a multifactorial, interdisciplinary intervention on risk factors for falls and fall rate in frail older people: A randomised controlled trial. Age Ageing 2014, 43, 616–622. [Google Scholar] [CrossRef] [PubMed]
- Fitzharris, M.P.; Day, L.; Lord, S.R.; Gordon, I.; Fildes, B. The Whitehorse NoFalls trial: Effects on fall rates and injurious fall rates. Age Ageing 2010, 39, 728–733. [Google Scholar] [CrossRef] [PubMed]
- Freiberger, E.; Menz, H.B.; Abu-Omar, K.; Rutten, A. Preventing falls in physically active community-dwelling older people: A comparison of two intervention techniques. Gerontology 2007, 53, 298–305. [Google Scholar] [CrossRef] [PubMed]
- Gawler, S.; Skelton, D.A.; Dinan-Young, S.; Masud, T.; Morris, R.W.; Griffin, M.; Kendrick, D.; Iliffe, S. Reducing falls among older people in general practice: The ProAct65+ exercise intervention trial. Arch. Gerontol. Geriatr. 2016, 67, 46–54. [Google Scholar] [CrossRef] [PubMed]
- Gianoudis, J.; Bailey, C.A.; Ebeling, P.R.; Nowson, C.A.; Sanders, K.M.; Hill, K.; Daly, R.M. Effects of a targeted multimodal exercise program incorporating high-speed power training on falls and fracture risk factors in older adults: A community-based randomized controlled trial. J. Bone Miner. Res. 2014, 29, 182–191. [Google Scholar] [CrossRef] [PubMed]
- Helbostad, J.L.; Sletvold, O.; Moe-Nilssen, R. Effects of home exercises and group training on functional abilities in home-dwelling older persons with mobility and balance problems: A randomized study. Aging Clin. Exp. Res. 2004, 16, 113–121. [Google Scholar] [CrossRef] [PubMed]
- Hogan, D.B.; MacDonald, F.A.; Betts, J.; Bricker, S.; Ebly, E.M.; Delarue, B.; Fung, T.S.; Harbidge, C.; Hunter, M.; Maxwell, C.J.; et al. A randomized controlled trial of a community-based consultation service to prevent falls. CMAJ 2001, 165, 537–543. [Google Scholar] [PubMed]
- Hornbrook, M.C.; Stevens, V.J.; Wingfield, D.J.; Hollis, J.F.; Greenlick, M.R.; Ory, M.G. Preventing falls among community-dwelling older persons: Results from a randomized trial. Gerontologist 1994, 34, 16–23. [Google Scholar] [CrossRef] [PubMed]
- Huang, T.T.; Yang, L.H.; Liu, C.Y. Reducing the fear of falling among community-dwelling elderly adults through cognitive-behavioural strategies and intense Tai Chi exercise: A randomized controlled trial. J. Adv. Nurs. 2011, 67, 961–971. [Google Scholar] [CrossRef] [PubMed]
- Jin, X.; Wang, S. The results analysis of intervention on fall among the elderly in Niujie area of Beijing. Chin. J. Geriatr. 2009, 28, 777–779. [Google Scholar] [CrossRef]
- Logghe, I.H.; Zeeuwe, P.E.; Verhagen, A.P.; Wijnen-Sponselee, R.M.; Willemsen, S.P.; Bierma-Zeinstra, S.M.; van Rossum, E.; Faber, M.J.; Koes, B.W. Lack of effect of Tai Chi Chuan in preventing falls in elderly people living at home: A randomized clinical trial. J. Am. Geriatr. Soc. 2009, 57, 70–75. [Google Scholar] [CrossRef] [PubMed]
- Lord, S.R.; Tiedemann, A.; Chapman, K.; Munro, B.; Murray, S.M.; Gerontology, M.; Ther, G.R.; Sherrington, C. The effect of an individualized fall prevention program on fall risk and falls in older people: A randomized, controlled trial. J. Am. Geriatr. Soc. 2005, 53, 1296–1304. [Google Scholar] [CrossRef] [PubMed]
- Luukinen, H.; Lehtola, S.; Jokelainen, J.; Väänänen-Sainio, R.; Lotvonen, S.; Koistinen, P. Pragmatic exercise-oriented prevention of falls among the elderly: A population-based, randomized, controlled trial. Prev. Med. 2007, 44, 265–271. [Google Scholar] [CrossRef] [PubMed]
- McMurdo, M.E.; Millar, A.M.; Daly, F. A randomized controlled trial of fall prevention strategies in old peoples’ homes. Gerontology 2000, 46, 83–87. [Google Scholar] [CrossRef] [PubMed]
- Palvanen, M.; Kannus, P.; Piirtola, M.; Niemi, S.; Parkkari, J.; Järvinen, M. Effectiveness of the Chaos Falls Clinic in preventing falls and injuries of home-dwelling older adults: A randomised controlled trial. Injury 2014, 45, 265–271. [Google Scholar] [CrossRef] [PubMed]
- Pérula, L.A.; Varas-Fabra, F.; Rodríguez, V.; Ruiz-Moral, R.; Fernández, J.A.; González, J.; Pérula, C.J.; Roldán, A.M.; de Dios, C. Effectiveness of a multifactorial intervention program to reduce falls incidence among community-living older adults: A randomized controlled trial. Arch. Phys. Med. Rehabil. 2012, 93, 1677–1684. [Google Scholar] [CrossRef] [PubMed]
- Pighills, A.C.; Torgerson, D.J.; Sheldon, T.A.; Drummond, A.E. Environmental assessment and modification to prevent falls in older people. J. Am. Geriatr. Soc. 2011, 59, 26–33. [Google Scholar] [CrossRef] [PubMed]
- Robson, E.; Edwards, J.; Gallagher, E.; Baker, D. Steady as you go (SAYGO): A falls-prevention program for seniors living in the community. Can. J. Aging 2003, 22, 207–216. [Google Scholar] [CrossRef]
- Salminen, M.J.; Vahlberg, T.J.; Salonoja, M.T.; Aarnio, P.T.; Kivelä, S.L. Effect of a risk-based multifactorial fall prevention program on the incidence of falls. J. Am. Geriatr. Soc. 2009, 57, 612–619. [Google Scholar] [CrossRef] [PubMed]
- Shumway-Cook, A.; Silver, I.F.; Lemier, M.; York, S.; Cummings, P.; Koepsell, T.D. Effectiveness of a community-based multifactorial intervention on falls and fall risk factors in community-living older adults: A randomized controlled trial. J. Gerontol. A Biol. Sci. Med. Sci. 2007, 6, 1420–1427. [Google Scholar] [CrossRef]
- Siegrist, M.; Freiberger, E.; Geilhof, B.; Salb, J.; Hentschke, C.; Landendoerfer, P.; Linde, K.; Halle, M.; Blank, W.A. Fall Prevention in a Primary Care Setting. Dtsch. Arztebl. Int. 2016, 113, 365–372. [Google Scholar] [CrossRef] [PubMed]
- Spice, C.L.; Morotti, W.; George, S.; Dent, T.H.; Rose, J.; Harris, S.; Gordon, C.J. The Winchester falls project: A randomised controlled trial of secondary prevention of falls in older people. Age Ageing 2009, 38, 33–40. [Google Scholar] [CrossRef] [PubMed]
- Tinetti, M.E.; Baker, D.I.; Mcavay, G.; Claus, E.B.; Garrett, P.; Gottschalk, M.; Koch, M.L.; Trainor, K.; Horwitz, R.I. A multifactorial intervention to reduce the risk of falling among elderly people living in the community. N. Engl. J. Med. 1994, 331, 821–827. [Google Scholar] [CrossRef] [PubMed]
- Trivedi, D.P.; Doll, R.; Khaw, K.T. Effect of four monthly oral vitamin D3 (cholecalciferol) supplementation on fractures and mortality in men and women living in the community: Randomised double blind controlled trial. BMJ 2003, 326, 469. [Google Scholar] [CrossRef] [PubMed]
- Trombetti, A.; Hars, M.; Herrmann, F.R.; Kressig, R.W.; Ferrari, S.; Rizzoli, R. Effect of music-based multitask training on gait, balance, and fall risk in elderly people: A randomized controlled trial. Arch. Intern. Med. 2011, 171, 525–533. [Google Scholar] [CrossRef] [PubMed]
- Voukelatos, A.; Cumming, R.G.; Lord, S.R.; Rissel, C. A randomized, controlled trial of tai chi for the prevention of falls: The Central Sydney tai chi trial. J. Am. Geriatr. Soc. 2007, 55, 1185–1191. [Google Scholar] [CrossRef] [PubMed]
- Voukelatos, A.; Merom, D.; Sherrington, C.; Rissel, C.; Cumming, R.G.; Lord, S.R. The impact of a home-based walking programme on falls in older people: The Easy Steps randomised controlled trial. Age Ageing 2015, 44, 377–383. [Google Scholar] [CrossRef] [PubMed]
- Wagner, E.H.; LaCroix, A.Z.; Grothaus, L.; Leveille, S.G.; Hecht, J.A.; Artz, K.; Odle, K.; Buchner, D.M. Preventing disability and falls in older adults: A population-based randomized trial. Am. J. Public Health 1994, 84, 1800–1806. [Google Scholar] [CrossRef] [PubMed]
- Weerdesteyn, V.; Rijken, H.; Geurts, A.C.; Smits-Engelsman, B.C.; Mulder, T.; Duysens, J. A five-week exercise program can reduce falls and improve obstacle avoidance in the elderly. Gerontology 2006, 52, 131–141. [Google Scholar] [CrossRef] [PubMed]
- Wolf, S.L.; Sattin, R.W.; Kutner, M.; O’Grady, M.; Greenspan, A.I.; Gregor, R.J. Intense tai chi exercise training and fall occurrences in older, transitionally frail adults: A randomized, controlled trial. J. Am. Geriatr. Soc. 2003, 51, 1693–1701. [Google Scholar] [CrossRef] [PubMed]
- Wu, C.; Wang, K.; He, Y.; Wang, Y.; Li, M.; Jin, P.; Wu, Y.; Hu, Y. A randomized controlled trial to prevent community elder falling and related factor analysis. Chin. J. Rehabilit. Med. 2010, 25, 986–988. [Google Scholar] [CrossRef]
- Xia, Q.; Jiang, Y.; Niu, C.; Xia, Z. Study on the effect of comprehensive intervention for fall among elderly adults in community. Chin. J. Prev. Control Chronic Dis. 2010, 18, 515–517. [Google Scholar]
- Xie, X.; Huang, Z.; Zhang, H. Application of Community Intervention Combined Health Education in Preventing Falls in older people. Chin. J. Ethno-Med. Ethno-Pharm. 2016, 25, 161–162. [Google Scholar]
- Zhan, J. Observation on the effect of family prevention and prevention of falls in the elderly. Med. Inf. 2015, 28, 226. [Google Scholar] [CrossRef]
- Zhan, P.; Liu, J. Application of CSPDCA mode in the design of exercises for the prevention of falls in the elderly. Pract. Clin. Med. 2010, 11, 98–99. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
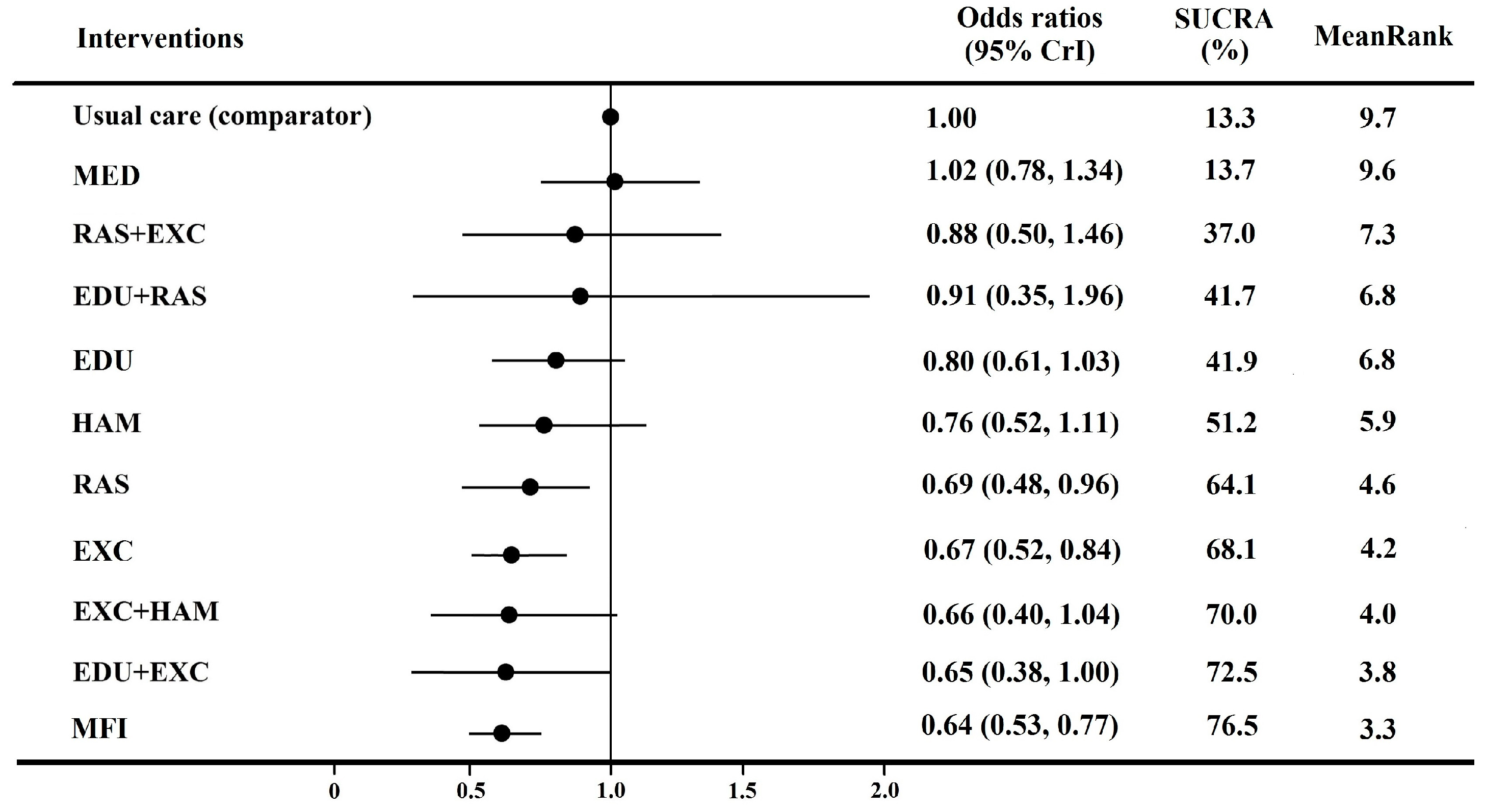
| (1) Usual Care | 0.80 (0.61, 1.03) | 0.69 (0.48, 0.96) * | 0.67 (0.52, 0.84) * | 1.02 (0.78, 1.34) | 0.76 (0.52, 1.11) | 0.91 (0.35, 1.96) | 0.65 (0.38, 1.00) | 0.88 (0.50, 1.46) | 0.66 (0.40, 1.04) | 0.64 (0.53, 0.77) * |
| (2) Education (EDU) | 0.88 (0.56, 1.33) | 0.85 (0.60, 1.12) | 1.30 (0.89, 1.80) | 0.97 (0.63, 1.51) | 1.14 (0.48, 2.40) | 0.81 (0.50, 1.21) | 1.12 (0.60, 2.04) | 0.84 (0.48, 1.40) | 0.81 (0.64, 1.00) * | |
| (3) Risk assessment and suggestions (RAS) | 1.00 (0.65, 1.50) | 1.53 (0.98, 2.32) | 1.14 (0.65, 1.80) | 1.37 (0.53, 2.97) | 0.96 (0.50, 1.74) | 1.32 (0.67, 2.38) | 0.98 (0.52, 1.67) | 0.95 (0.64, 1.39) | ||
| (4) Exercise (EXC) | 1.55 (1.10, 2.18) | 1.16 (0.74, 1.76) | 1.38 (0.55, 3.07) | 0.98 (0.56, 1.57) | 1.33 (0.75, 2.29) | 0.99 (0.59, 1.57) | 0.97 (0.73, 1.30) | |||
| (5) Medical care (MED) | 0.76 (0.48, 1.14) | 0.91 (0.35, 2.03) | 0.64 (0.35, 1.06) | 0.88 (0.46, 1.51) | 0.65 (0.38, 1.07) | 0.63 (0.46, 0.84) * | ||||
| (6) Hazard assessment and modification (HAM) | 1.23 (0.43, 2.70) | 0.88 (0.44, 1.48) | 1.20 (0.57, 2.16) | 0.89 (0.48, 1.51) | 0.87 (0.55, 1.25) | |||||
| (7) EDU + RAS | 0.83 (0.30, 1.92) | 1.16 (0.39, 2.69) | 0.86 (0.30, 1.94) | 0.83 (0.33, 1.76) | ||||||
| (8) EDU + EXC | 1.46 (0.63, 2.98) | 1.09 (0.52, 2.12) | 1.04 (0.64, 1.66) | |||||||
| (9) RAS + EXC | 0.81 (0.37, 1.56) | 0.78 (0.42, 1.32) | ||||||||
| (10) EXC + HAM | 1.03 (0.60, 1.66) | |||||||||
| (11) Multifactorial interventions (MFI) |
| Analysis Strategies | EDU | RAS | EXC | MED | HAM | EDU + RAS | EDU + EXC | RAS + EXC | EXC + HAM | MFI |
|---|---|---|---|---|---|---|---|---|---|---|
| All 49 studies | 0.80 (0.61, 1.03) | 0.69 (0.48, 0.96) * | 0.67 (0.52, 0.84) * | 1.02 (0.78, 1.34) | 0.76 (0.52, 1.11) | 0.91 (0.35, 1.96) | 0.65 (0.38, 1.00) | 0.88 (0.50, 1.46) | 0.66 (0.40, 1.04) | 0.64 (0.53, 0.77) * |
| Exclude Ref. [36] | 0.80 (0.61, 1.02) | 0.68 (0.47, 0.96) * | 0.68 (0.54, 0.85) * | 1.02 (0.76, 1.36) | 0.76 (0.50, 1.10) | 0.89 (0.35, 1.85) | 0.65 (0.39, 1.06) | 0.90 (0.48, 1.54) | 0.65 (0.38, 1.02) | 0.64 (0.53, 0.77) * |
| Exclude Ref. [37] | 0.80 (0.60, 1.04) | 0.69 (0.47, 0.95) * | 0.67 (0.53, 0.82) * | 1.02 (0.75, 1.35) | 0.77 (0.51, 1.14) | 0.92 (0.35, 2.00) | 0.66 (0.36, 1.06) | 0.89 (0.48, 1.56) | 0.65 (0.39, 1.04) | 0.64 (0.52, 0.76) * |
| Exclude Ref. [43] | 0.80 (0.61, 1.03) | 0.82 (0.53, 1.20) | 0.67 (0.54, 0.82) * | 1.02 (0.79, 1.28) | 0.76 (0.52, 1.05) | 0.91 (0.37, 1.95) | 0.66 (0.39, 1.07) | 0.91 (0.49, 1.51) | 0.66 (0.39, 1.04) | 0.64 (0.53, 0.78) * |
| Exclude Ref. [74] | 0.80 (0.60, 1.03) | 0.69 (0.49, 0.96) * | 0.69 (0.54, 0.84) * | 1.03 (0.78, 1.34) | 0.77 (0.53, 1.08) | 0.92 (0.37, 1.90) | 0.64 (0.39, 1.06) | 0.90 (0.48, 1.54) | 0.66 (0.39, 1.05) | 0.64 (0.52, 0.77) * |
| Exclude Ref. [76] | 0.79 (0.60, 1.04) | 0.69 (0.48, 0.97) * | 0.65 (0.51, 0.82) * | 1.01 (0.75, 1.33) | 0.77 (0.52, 1.10) | 0.90 (0.37, 1.89) | 0.64 (0.38, 1.02) | 0.88 (0.47, 1.50) | 0.66 (0.39, 1.03) | 0.64 (0.53, 0.76) * |
| Exclude Refs. A | 0.80 (0.61, 1.05) | 0.81 (0.51, 1.21) | 0.68 (0.54, 0.87) * | 1.02 (0.77, 1.32) | 0.76 (0.52, 1.10) | 0.91 (0.36, 1.90) | 0.66 (0.39, 1.08) | 0.88 (0.48, 1.43) | 0.65 (0.38, 1.01) | 0.65 (0.54, 0.78) * |
| Exclude Refs. B | 0.90 (0.70, 1.14) | 0.71 (0.53, 0.92) * | 0.71 (0.60, 0.87) * | 1.04 (0.81, 1.27) | 0.78 (0.58, 1.06) | 0.97 (0.44, 1.88) | 0.75 (0.46, 1.12) | 0.89 (0.55, 1.39) | 0.68 (0.46, 1.02) | 0.77 (0.63, 0.92) * |
| Exclude Refs. C | 0.79 (0.62, 1.02) | 0.68 (0.48, 0.94) * | 0.68 (0.54, 0.84) * | 1.01 (0.75, 1.35) | 0.76 (0.50, 1.09) | 0.87 (0.36, 1.84) | 0.72 (0.40, 1.18) | 0.90 (0.49, 1.52) | 0.66 (0.38, 1.06) | 0.64 (0.53, 0.77) * |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cheng, P.; Tan, L.; Ning, P.; Li, L.; Gao, Y.; Wu, Y.; Schwebel, D.C.; Chu, H.; Yin, H.; Hu, G. Comparative Effectiveness of Published Interventions for Elderly Fall Prevention: A Systematic Review and Network Meta-Analysis. Int. J. Environ. Res. Public Health 2018, 15, 498. https://doi.org/10.3390/ijerph15030498
Cheng P, Tan L, Ning P, Li L, Gao Y, Wu Y, Schwebel DC, Chu H, Yin H, Hu G. Comparative Effectiveness of Published Interventions for Elderly Fall Prevention: A Systematic Review and Network Meta-Analysis. International Journal of Environmental Research and Public Health. 2018; 15(3):498. https://doi.org/10.3390/ijerph15030498
Chicago/Turabian StyleCheng, Peixia, Liheng Tan, Peishan Ning, Li Li, Yuyan Gao, Yue Wu, David C. Schwebel, Haitao Chu, Huaiqiong Yin, and Guoqing Hu. 2018. "Comparative Effectiveness of Published Interventions for Elderly Fall Prevention: A Systematic Review and Network Meta-Analysis" International Journal of Environmental Research and Public Health 15, no. 3: 498. https://doi.org/10.3390/ijerph15030498