Association between Age of Menopause and Thickness of Crestal Cortical Bone at Dental Implant Site: A Cross-Sectional Observational Study

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. CBCT Examinations of Patients and Implant Sites
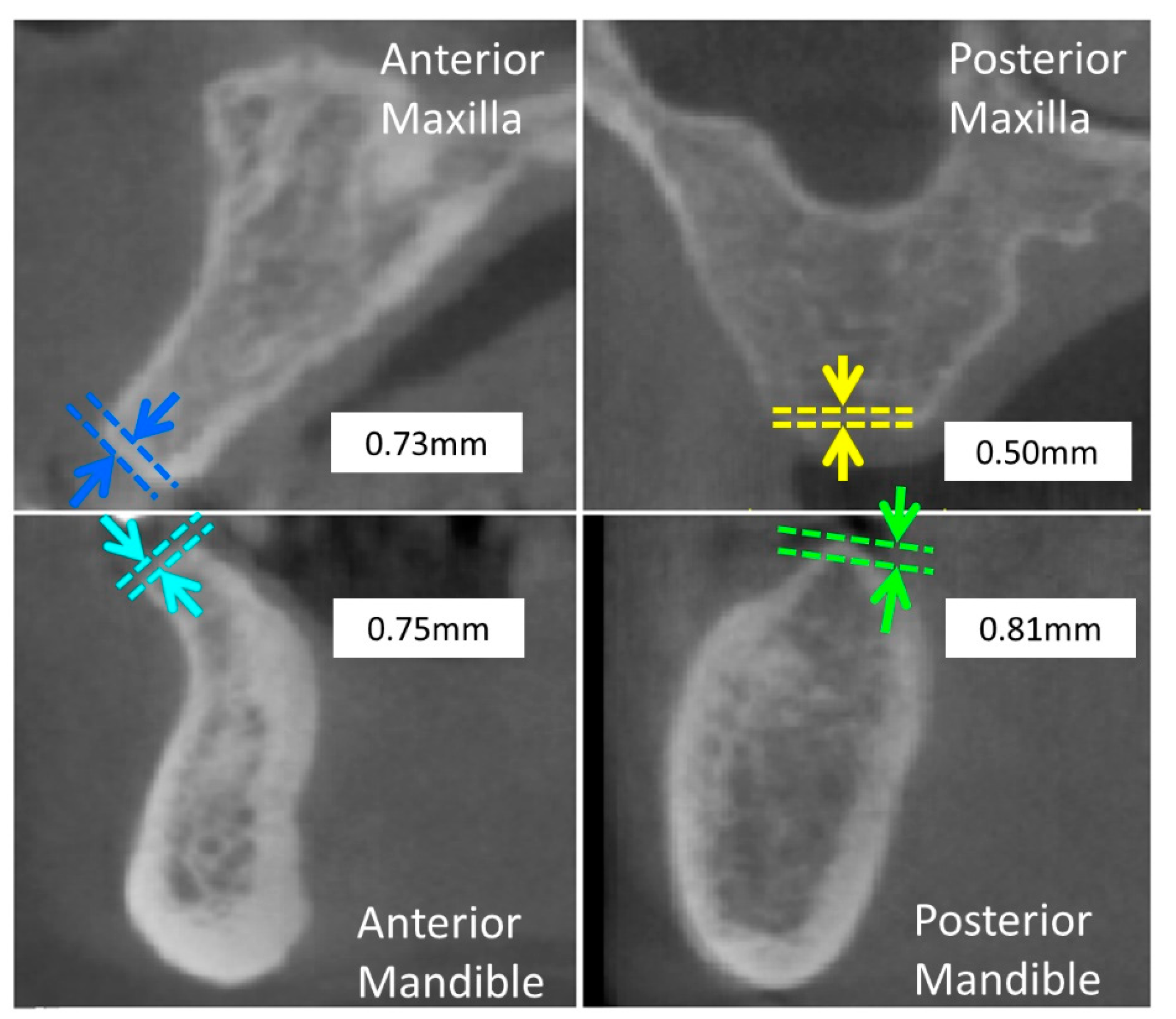
2.2. Measurement of Thickness of Crestal Cortical Bone at Prospective Dental Implant Sites
2.3. Statistical Analysis
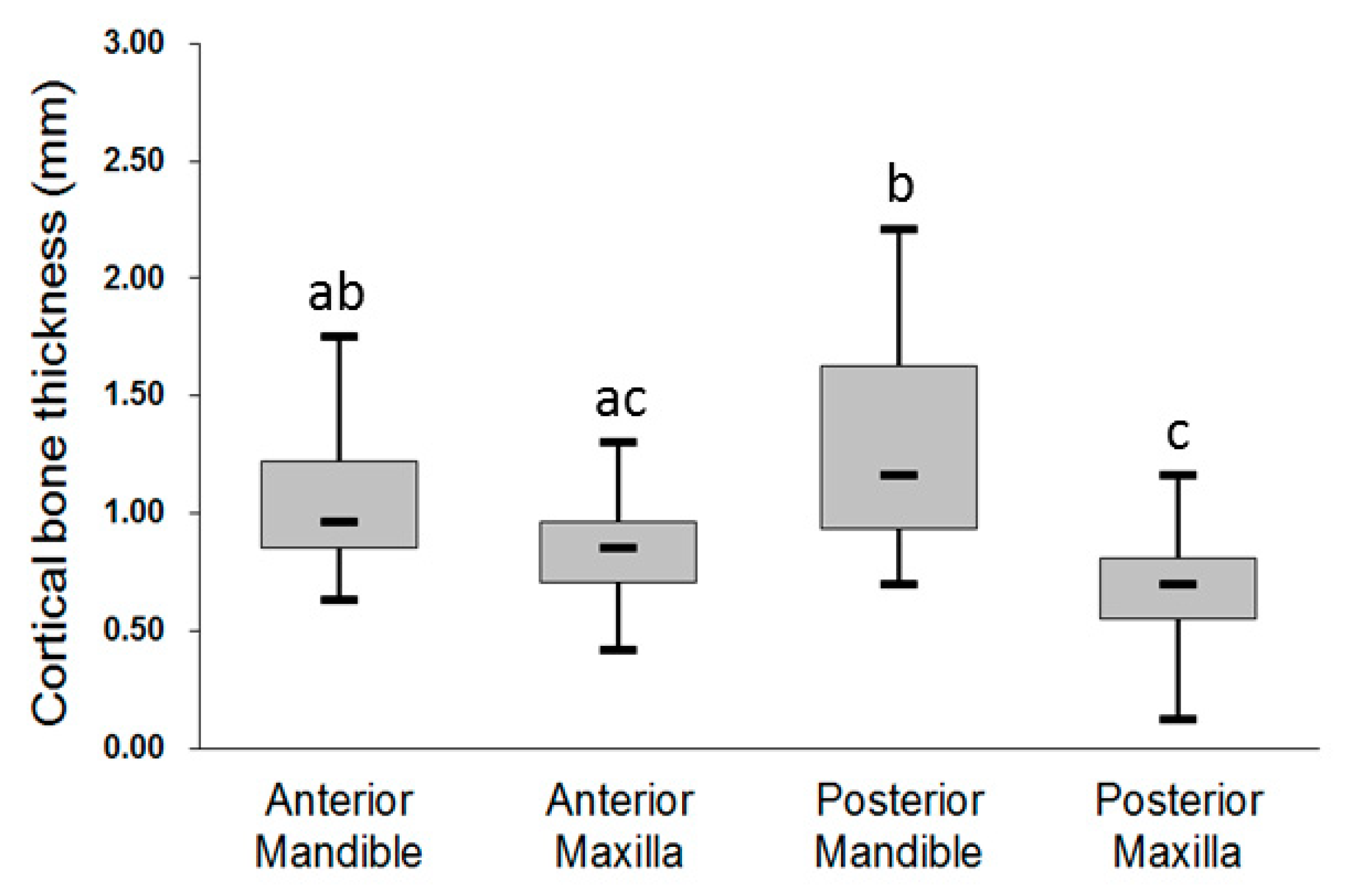
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Kanis, J.A.; Melton, L.J., III; Christiansen, C.; Johnston, C.C.; Khaltaev, N. The diagnosis of osteoporosis. J. Bone Miner. Res. 1994, 9, 1137–1141. [Google Scholar] [CrossRef]
- Melton, J.L., III. Perspectives: How many women have osteoporosis now? J. Bone Miner. Res. 1995, 10, 175–177. [Google Scholar] [CrossRef]
- Iwasaki, M.; Nakamura, K.; Yoshihara, A.; Miyazaki, H. Change in bone mineral density and tooth loss in Japanese community-dwelling postmenopausal women: A 5-year cohort study. J. Bone Miner. Metab. 2012, 30, 447–453. [Google Scholar] [CrossRef]
- Branemark, P.-I. Osseointegrated implants in the treatment of the edentulous jaw. Experience from a 10-year period. Scand. J. Plast. Reconstr. Surg. Suppl. 1977, 16, 1–132. [Google Scholar]
- Alsaadi, G.; Quirynen, M.; Komárek, A.; Van Steenberghe, D. Impact of local and systemic factors on the incidence of oral implant failures, up to abutment connection. J. Clin. Periodontol. 2007, 34, 610–617. [Google Scholar] [CrossRef]
- Hsu, J.T.; Fuh, L.J.; Tu, M.G.; Li, Y.F.; Chen, K.T.; Huang, H.L. The effects of cortical bone thickness and trabecular bone strength on noninvasive measures of the implant primary stability using synthetic bone models. Clin. Implant. Dent. Relat. Res. 2013, 15, 251–261. [Google Scholar] [CrossRef]
- Moy, P.K.; Medina, D.; Shetty, V.; Aghaloo, T.L. Dental implant failure rates and associated risk factors. Int. J. Oral Maxillofac. Implant. 2005, 20, 569–577. [Google Scholar]
- Alamri, H.; Sadrameli, M.; Alshalhoob, M.; Alshehri, M. Applications of CBCT in dental practice: A review of the literature. Gen. Dent. 2012, 60, 390–400. [Google Scholar]
- de Oliveira, R.C.G.; Leles, C.R.; Normanha, L.M.; Lindh, C.; Ribeiro-Rotta, R.F. Assessments of trabecular bone density at implant sites on CT images. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2008, 105, 231–238. [Google Scholar] [CrossRef]
- Fuh, L.J.; Huang, H.L.; Chen, C.S.; Fu, K.L.; Shen, Y.W.; Tu, M.G.; Shen, W.C.; Hsu, J.T. Variations in bone density at dental implant sites in different regions of the jawbone. J. Oral Rehabil. 2010, 37, 346–351. [Google Scholar] [CrossRef]
- Shapurian, T.; Damoulis, P.D.; Reiser, G.M.; Griffin, T.J.; Rand, W.M. Quantitative evaluation of bone density using the Hounsfield index. Int. J. Oral Maxillofac. Implant. 2006, 21, 290–297. [Google Scholar]
- Turkyilmaz, I.; McGlumphy, E.A. Influence of bone density on implant stability parameters and implant success: A retrospective clinical study. BMC Oral Health 2008, 8, 32. [Google Scholar] [CrossRef] [Green Version]
- Gerlach, N.L.; Meijer, G.J.; Borstlap, W.A.; Bronkhorst, E.M.; Bergé, S.J.; Maal, T.J.J. Accuracy of bone surface size and cortical layer thickness measurements using cone beam computerized tomography. Clin. Oral Implant. Res. 2013, 24, 793–797. [Google Scholar] [CrossRef]
- Miyamoto, I.; Tsuboi, Y.; Wada, E.; Suwa, H.; Iizuka, T. Influence of cortical bone thickness and implant length on implant stability at the time of surgery—Clinical, prospective, biomechanical, and imaging study. Bone 2005, 37, 776–780. [Google Scholar] [CrossRef]
- Sugiura, T.; Yamamoto, K.; Kawakami, M.; Horita, S.; Murakami, K.; Kirita, T. Influence of bone parameters on peri-implant bone strain distribution in the posterior mandible. Med. Oral Patol. Oral Y Cir. Bucal 2015, 20, e66. [Google Scholar] [CrossRef]
- Lekholm, U.; Zarb, G.A. Patient selection and preparation. In Tissue-Integr. Prostheses: Osseointegration Clinical Dentistry; Brånemark, P.I., Zarb, G.A., Albrektsson, T., Eds.; Quintessence: Milan, Italy, 1985; pp. 199–209. [Google Scholar]
- Norton, M.R.; Gamble, C. Bone classification: An objective scale of bone density using the computerized tomography scan. Clin. Oral Implant. Res. 2001, 12, 79–84. [Google Scholar] [CrossRef]
- Vercellotti, T.; Vercellotti, G. New bone classification for analysis of the single surgical site. In Essentials in Piezosurgery: Clinical Advantages in Dentistry; Quintessence: Milan, Italy, 2009; pp. 91–93. [Google Scholar]
- David, O.; Leretter, M.; Neagu, A. The quality of trabecular bone assessed using cone-beam computed tomography. Rom. J. Biophys 2014, 24, 227–241. [Google Scholar]
- González-García, R.; Monje, F. The reliability of cone-beam computed tomography to assess bone density at dental implant recipient sites: A histomorphometric analysis by micro-CT. Clin. Oral Implant. Res. 2013, 24, 871–879. [Google Scholar] [CrossRef]
- Hao, Y.; Zhao, W.; Wang, Y.; Yu, J.; Zou, D. Assessments of jaw bone density at implant sites using 3D cone-beam computed tomography. Eur. Rev. Med Pharmacol. Sci. 2014, 18, 1398–1403. [Google Scholar]
- Gupta, A.; Rathee, S.; Agarwal, J.; Pachar, R. Measurement of Crestal Cortical Bone Thickness at Implant Site: A Cone Beam Computed Tomography Study. J. Contemp. Dent. Pract. 2017, 18, 785–789. [Google Scholar] [CrossRef]
- Ko, Y.C.; Huang, H.L.; Shen, Y.W.; Cai, J.Y.; Fuh, L.J.; Hsu, J.T. Variations in crestal cortical bone thickness at dental implant sites in different regions of the jawbone. Clin. Implant. Dent. Relat. Res. 2017, 19, 440–446. [Google Scholar] [CrossRef]
- Jacobs, R.; Salmon, B.; Codari, M.; Hassan, B.; Bornstein, M.M. Cone beam computed tomography in implant dentistry: Recommendations for clinical use. BMC Oral Heal. 2018, 18, 88. [Google Scholar] [CrossRef] [Green Version]
- Fanning, B. CBCT—The justification process, audit and review of the recent literature. J. Ir. Dent. Assoc. 2011, 57, 256–261. [Google Scholar]
- Frederiksen, N.L. Diagnostic imaging in dental implantology. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 1995, 80, 540–554. [Google Scholar] [CrossRef]
- Guerrero, M.E.; Jacobs, R.; Loubele, M.; Schutyser, F.; Suetens, P.; van Steenberghe, D. State-of-the-art on cone beam CT imaging for preoperative planning of implant placement. Clin. Oral Investig. 2006, 10, 1–7. [Google Scholar] [CrossRef]
- Sumer, A.; Caliskan, A.; Uzun, C.; Karoz, T.; Sumer, M.; Cankaya, S. The evaluation of palatal bone thickness for implant insertion with cone beam computed tomography. Int. J. Oral Maxillofac. Surg. 2016, 45, 216–220. [Google Scholar] [CrossRef]
- Tsutsumi, K.; Chikui, T.; Okamura, K.; Yoshiura, K. Accuracy of linear measurement and the measurement limits of thin objects with cone beam computed tomography: Effects of measurement directions and of phantom locations in the fields of view. Int. J. Oral Maxillofac. Implant. 2011, 26, 91–100. [Google Scholar]
- Borrud, L.G.; Dawson-Hughes, B.; Looker, A.C.; Shepherd, J.A.; Wright, N.C. Osteoporosis or low bone mass at the femur neck or lumbar spine in older adults, United States, 2005–2008. NCHS Data Brief. 2012, 93, 1–8. [Google Scholar]
- Gulsahi, A. Osteoporosis and jawbones in women. J. Int. Soc. Prev. Community Dent. 2015, 5, 263. [Google Scholar] [CrossRef] [Green Version]
- Daan, N.M.; Fauser, B.C. Menopause prediction and potential implications. Maturitas 2015, 82, 257–265. [Google Scholar] [CrossRef]
- Greendale, G.A.; Lee, N.P.; Arriola, E.R. The menopause. Lancet 1999, 353, 571–580. [Google Scholar] [CrossRef]
- Chen, C.-H.; Nakano, H.; Liou, E.J.; Maki, K. A cone beam computer tomographic study of the cortical bone thickness in different class II facial patterns. Orthod. Waves 2010, 69, 131–137. [Google Scholar] [CrossRef]
- Farnsworth, D.; Rossouw, P.E.; Ceen, R.F.; Buschang, P.H. Cortical bone thickness at common miniscrew implant placement sites. Am. J. Orthod. Dentofac. Orthop. 2011, 139, 495–503. [Google Scholar] [CrossRef]
- Nucera, R.; Lo Giudice, A.; Bellocchio, A.M.; Spinuzza, P.; Caprioglio, A.; Perillo, L.; Matarese, G.; Cordasco, G. Bone and cortical bone thickness of mandibular buccal shelf for mini-screw insertion in adults. Angle Orthod. 2017, 87, 745–751. [Google Scholar] [CrossRef] [Green Version]
- Poon, Y.-C.; Chang, H.-P.; Tseng, Y.-C.; Chou, S.-T.; Cheng, J.-H.; Liu, P.-H.; Pan, C.-Y. Palatal bone thickness and associated factors in adult miniscrew placements: A cone-beam computed tomography study. Kaohsiung J. Med. Sci. 2015, 31, 265–270. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Region | Younger Group | Older Group | p† | ||
|---|---|---|---|---|---|
| Number of Patient/Dental Implant Site | Mean ± SD (mm) | Number of Patient/Dental Implant Site | Mean ± SD (mm) | ||
| Anterior maxilla | 11/26 | 0.89 ± 0.26 | 6/19 | 0.85 ± 0.21 | 0.589 |
| Posterior maxilla | 18/48 | 0.77 ± 0.24 | 30/84 | 0.66 ± 0.29 | 0.008 * |
| Anterior mandible | 6/16 | 1.13 ± 0.20 | 6/24 | 1.08 ± 0.33 | 0.615 |
| Posterior mandible | 26/59 | 1.29 ± 0.46 | 20/64 | 1.27 ± 0.40 | 0.823 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ko, Y.-C.; Tsai, M.-T.; Fuh, L.-J.; Tsai, M.-J.; Wang, X.-H.; Huang, H.-L.; Hsu, J.-T. Association between Age of Menopause and Thickness of Crestal Cortical Bone at Dental Implant Site: A Cross-Sectional Observational Study. Int. J. Environ. Res. Public Health 2020, 17, 5868. https://doi.org/10.3390/ijerph17165868
Ko Y-C, Tsai M-T, Fuh L-J, Tsai M-J, Wang X-H, Huang H-L, Hsu J-T. Association between Age of Menopause and Thickness of Crestal Cortical Bone at Dental Implant Site: A Cross-Sectional Observational Study. International Journal of Environmental Research and Public Health. 2020; 17(16):5868. https://doi.org/10.3390/ijerph17165868
Chicago/Turabian StyleKo, Yi-Chun, Ming-Tzu Tsai, Lih-Jyh Fuh, Min-Jia Tsai, Xuan-Hui Wang, Heng-Li Huang, and Jui-Ting Hsu. 2020. "Association between Age of Menopause and Thickness of Crestal Cortical Bone at Dental Implant Site: A Cross-Sectional Observational Study" International Journal of Environmental Research and Public Health 17, no. 16: 5868. https://doi.org/10.3390/ijerph17165868