The Impact and Consequences of SARS-CoV-2 Pandemic on a Single University Dermatology Outpatient Clinic in Germany

 , , , and
, , , and 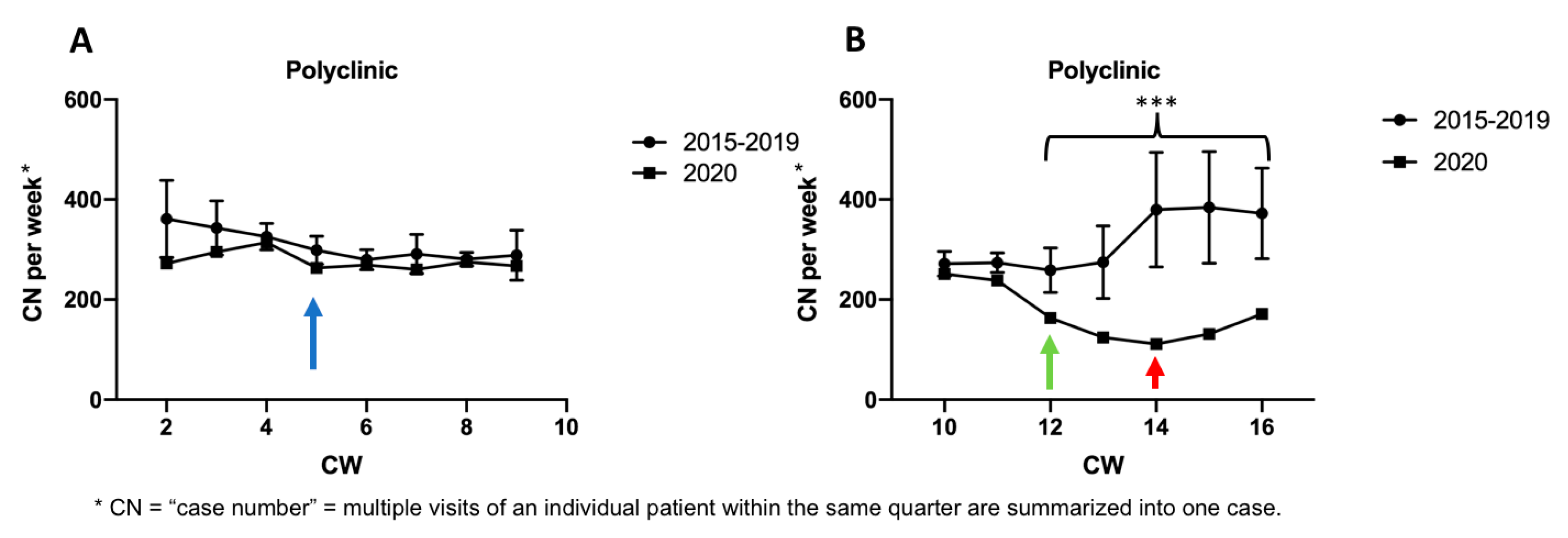{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Methods
Statistical Analyses
3. Results
3.1. Number of Outpatient Cases Declined Significantly as a Consequence of the SARS-CoV-2 Pandemic
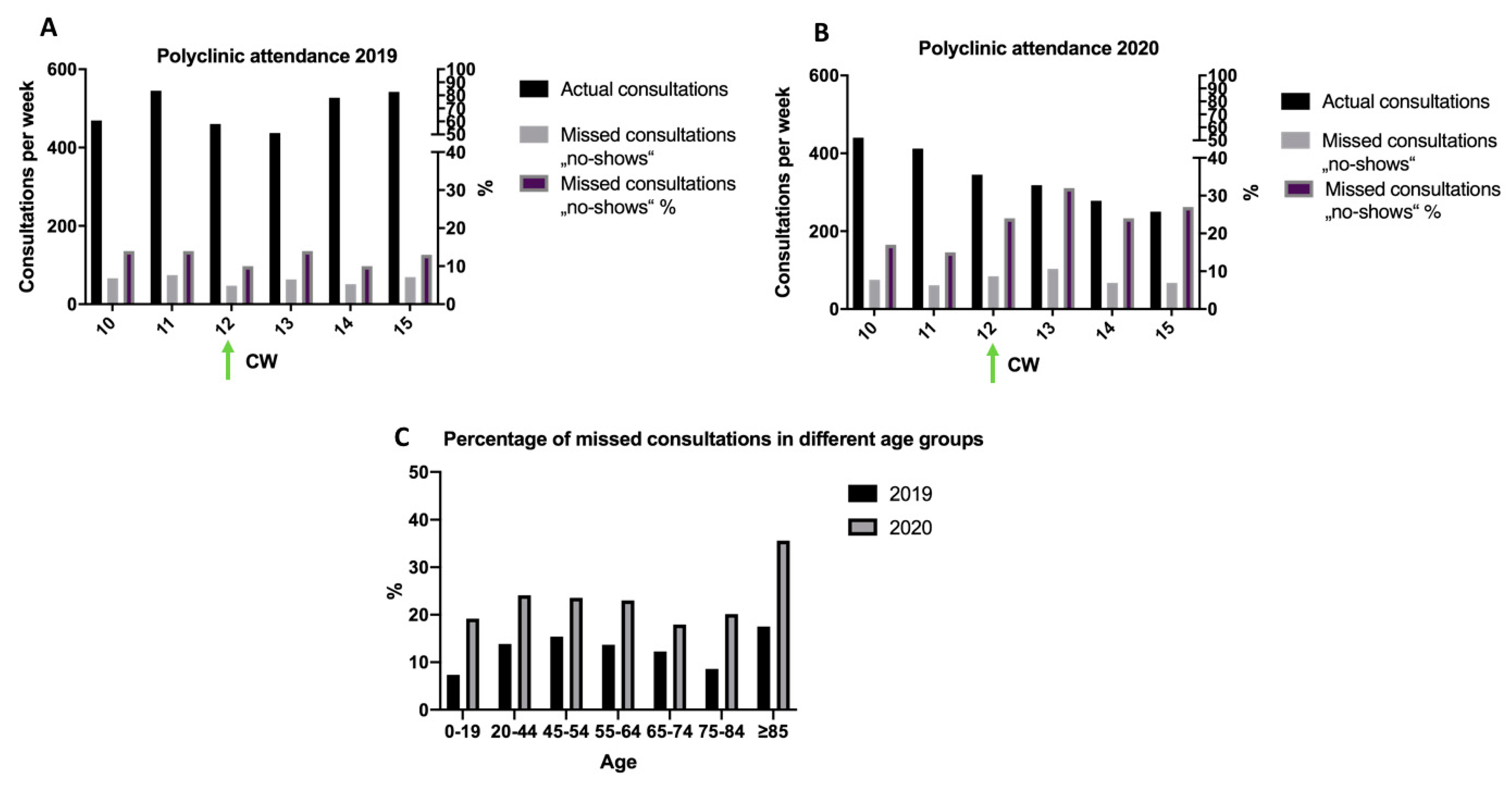
3.2. Substantial Increase of Missed Consultations during the Peak of SARS-CoV-2 Pandemic
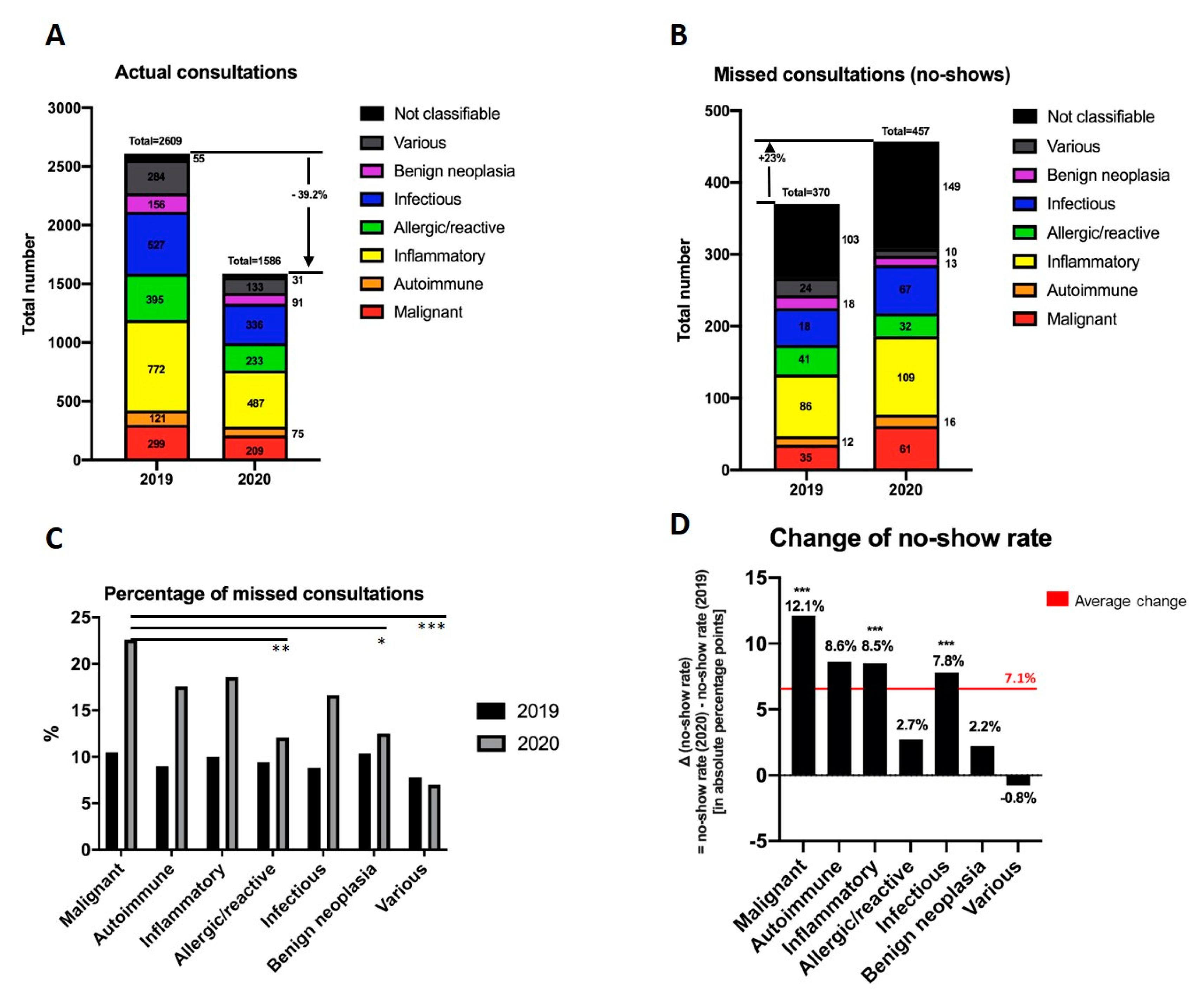
3.3. Patient Groups Were Differently Influenced by SARS-CoV-2 Pandemic
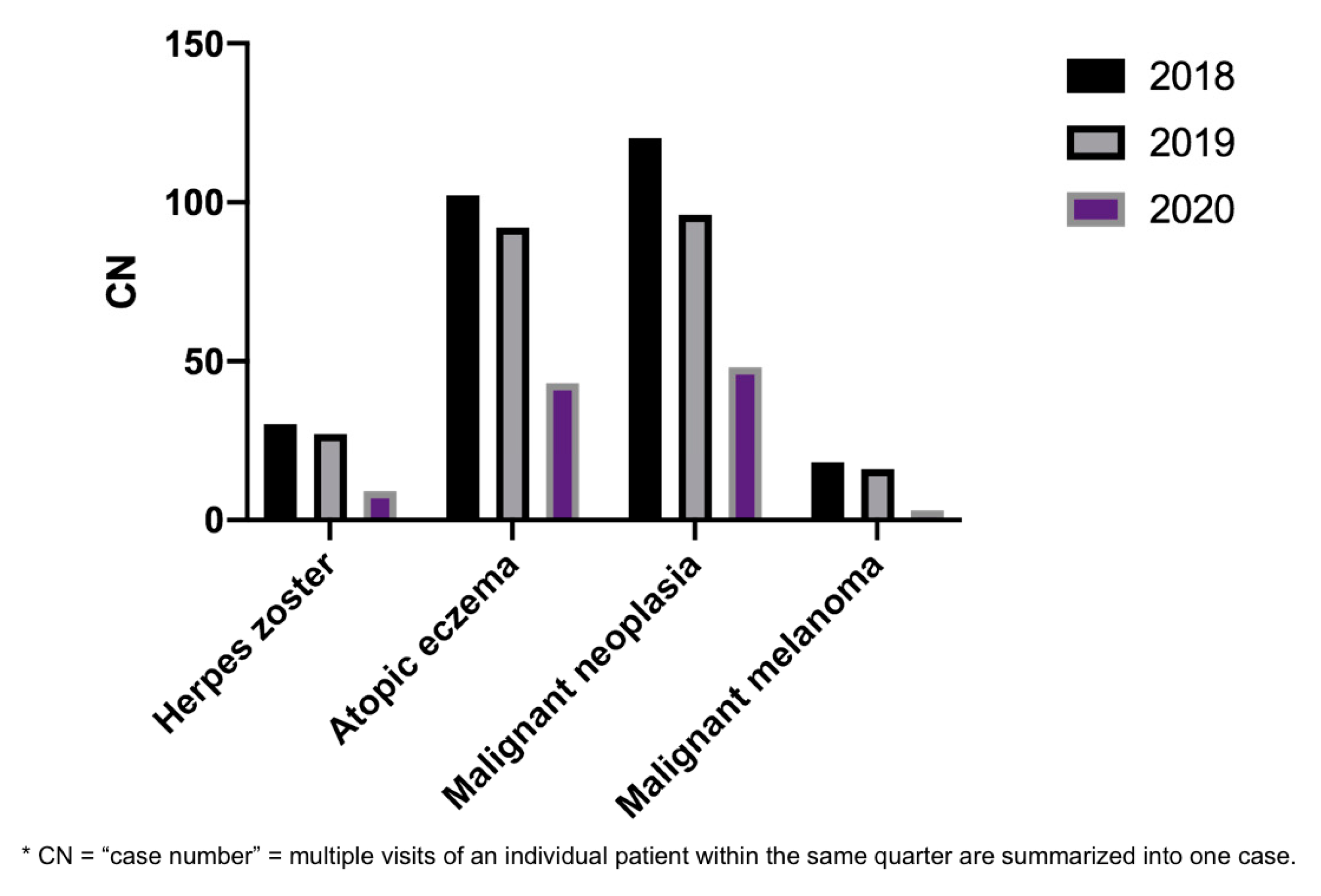
3.4. Absolute Case Numbers of Certain Diagnoses in Our PC Decreased during SARS-CoV-2 Pandemic
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Lu, H.-Z.; Stratton, C.W.; Tang, Y.-W. Outbreak of pneumonia of unknown etiology in Wuhan, China: The mystery and the miracle. J. Med. Virol. 2020, 92, 401–402. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Du Toit, A. Outbreak of a novel coronavirus. Nat. Rev. Microbiol. 2020, 18, 123. [Google Scholar] [CrossRef] [PubMed]
- Emanuel, E.J.; Persad, G.; Upshur, R.; Thome, B.; Parker, M.; Glickman, A.; Zhang, C.; Boyle, C.; Smith, M.; Phillips, J.P. Fair Allocation of Scarce Medical Resources in the Time of Covid-19. N. Engl. J. Med. 2020, 382, 2049–2055. [Google Scholar] [CrossRef] [PubMed]
- Corona-Pandemie/Bayern Ruft den Katastrophenfall aus/Veranstaltungsverbote und Betriebsuntersagungen. 2020. Available online: https://www.bayern.de/corona-pandemie-bayern-ruft-den-katastrophenfall-aus-veranstaltungsverbote-und-betriebsuntersagungen/ (accessed on 25 August 2020).
- Wargon, M.; Guidet, B.; Hoang, T.D.; Hejblum, G. A systematic review of models for forecasting the number of emergency department visits. Emerg. Med. J. 2009, 26, 395–399. [Google Scholar] [CrossRef] [PubMed]
- Diehl, A.K.; Morris, M.D.; Mannis, S.A. Use of Calendar and Weather Data to Predict Walk-In Attendance. South. Med. J. 1981, 74, 709–712. [Google Scholar] [CrossRef] [PubMed]
- Holleman, D.R.; Bowling, R.L.; Gathy, C. Predicting daily visits to a waik-in clinic and emergency department using calendar and weather data. J. Gen. Intern. Med. 1996, 11, 237–239. [Google Scholar] [CrossRef] [PubMed]
- Batal, H.; Tench, J.; McMillan, S.; Adams, J.; Mehler, P.S. Predicting patient visits to an urgent care clinic using calendar variables. Acad. Emerg. Med. 2001, 8, 48–53. [Google Scholar] [CrossRef]
- Allocca, M.; Fiorino, G.; Furfaro, F.; Gilardi, D.; Radice, S.; D’Amico, F.; Zilli, A.; Danese, S. Maintaining the Quality Standards of Care for Inflammatory Bowel Disease Patients During the COVID-19 Pandemic. Clin. Gastroenterol. Hepatol. 2020, 18, 1882–1883. [Google Scholar] [CrossRef]
- Metzler, B.; Siostrzonek, P.; Binder, R.K.; Bauer, A.; Reinstadler, S.J. Decline of acute coronary syndrome admissions in Austria since the outbreak of COVID-19: The pandemic response causes cardiac collateral damage. Eur. Heart J. 2020, 41, 1852–1853. [Google Scholar] [CrossRef] [Green Version]
- Schwarz, V.; Mahfoud, F.; Lauder, L.; Reith, W.; Behnke, S.; Smola, S.; Rissland, J.; Pfuhl, T.; Scheller, B.; Böhm, M.; et al. Decline of emergency admissions for cardiovascular and cerebrovascular events after the outbreak of COVID-19. Clin. Res. Cardiol. 2020, 1–7. [Google Scholar] [CrossRef]
- Garfin, D.R.; Silver, R.C.; Holman, E.A. The novel coronavirus (COVID-2019) outbreak: Amplification of public health consequences by media exposure. Health Psychol. 2020, 39, 355–357. [Google Scholar] [CrossRef]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Li, X.; Xu, S.; Yu, M.; Wang, K.; Tao, Y.; Zhou, Y.; Shi, J.; Zhou, M.; Wu, B.; Yang, Z.; et al. Risk factors for severity and mortality in adult COVID-19 inpatients in Wuhan. J. Allergy Clin. Immunol. 2020, 146, 110–118. [Google Scholar] [CrossRef] [PubMed]
- Bialek, S.; Boundy, E.; Bowen, V.; Chow, N.; Cohn, A.; Dowling, N.; Ellington, S.; Gierke, R.; Hall, A.; MacNeil, J.; et al. Severe Outcomes Among Patients with Coronavirus Disease 2019 (COVID-19)—United States, February 12–March 16, 2020. MMWR. Morb. Mortal. Wkly. Rep. 2020, 69, 343–346. [Google Scholar] [CrossRef]
- Wang, H.; Zhang, L. Risk of COVID-19 for patients with cancer. Lancet Oncol. 2020, 21, e181. [Google Scholar] [CrossRef]
- Xia, Y.; Jin, R.; Zhao, J.; Li, W.; Shen, H. Risk of COVID-19 for patients with cancer. Lancet Oncol. 2020, 21, e180. [Google Scholar] [CrossRef]
- Wu, P.-H.; Chuang, Y.-S.; Lin, Y.-T. Does Herpes Zoster Increase the Risk of Stroke and Myocardial Infarction? A Comprehensive Review. J. Clin. Med. 2019, 8, 547. [Google Scholar] [CrossRef] [Green Version]
- Johnson, R.W.; Rice, A.S. Postherpetic neuralgia. N. Engl. J. Med. 2014, 371, 1526–1533. [Google Scholar] [CrossRef] [PubMed]
- Cormier, J.N.; Voss, R.K.; Woods, T.N.; Cromwell, K.D.; Nelson, K.C. Improving outcomes in patients with melanoma: Strategies to ensure an early diagnosis. Patient Relat. Outcome Meas. 2015, 6, 229–242. [Google Scholar] [CrossRef] [Green Version]
- Pennie, M.L.; Soon, S.L.; Risser, J.B.; Veledar, E.; Culler, S.D.; Chen, S.C. Melanoma outcomes for Medicare patients: Association of stage and survival with detection by a dermatologist vs a nondermatologist. Arch. Dermatol. 2007, 143, 488–494. [Google Scholar] [CrossRef]
- Maringe, C.; Spicer, J.; Morris, M.; Purushotham, A.; Nolte, E.; Sullivan, R.; Rachet, B.; Aggarwal, A. The impact of the COVID-19 pandemic on cancer deaths due to delays in diagnosis in England, UK: A national, population-based, modelling study. Lancet Oncol. 2020, 21, 1023–1034. [Google Scholar] [CrossRef]




© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, R.; Helf, C.; Tizek, L.; Neuhauser, R.; Eyerich, K.; Zink, A.; Eberlein, B.; Biedermann, T.; Brockow, K.; Boehner, A. The Impact and Consequences of SARS-CoV-2 Pandemic on a Single University Dermatology Outpatient Clinic in Germany. Int. J. Environ. Res. Public Health 2020, 17, 6182. https://doi.org/10.3390/ijerph17176182
Wang R, Helf C, Tizek L, Neuhauser R, Eyerich K, Zink A, Eberlein B, Biedermann T, Brockow K, Boehner A. The Impact and Consequences of SARS-CoV-2 Pandemic on a Single University Dermatology Outpatient Clinic in Germany. International Journal of Environmental Research and Public Health. 2020; 17(17):6182. https://doi.org/10.3390/ijerph17176182
Chicago/Turabian StyleWang, Rosi, Charlotte Helf, Linda Tizek, Ruth Neuhauser, Kilian Eyerich, Alexander Zink, Bernadette Eberlein, Tilo Biedermann, Knut Brockow, and Alexander Boehner. 2020. "The Impact and Consequences of SARS-CoV-2 Pandemic on a Single University Dermatology Outpatient Clinic in Germany" International Journal of Environmental Research and Public Health 17, no. 17: 6182. https://doi.org/10.3390/ijerph17176182