
Effect of Home Exercise Training in Patients with Nonspecific Low-Back Pain: A Systematic Review and Meta-Analysis


 , ,
, ,  , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
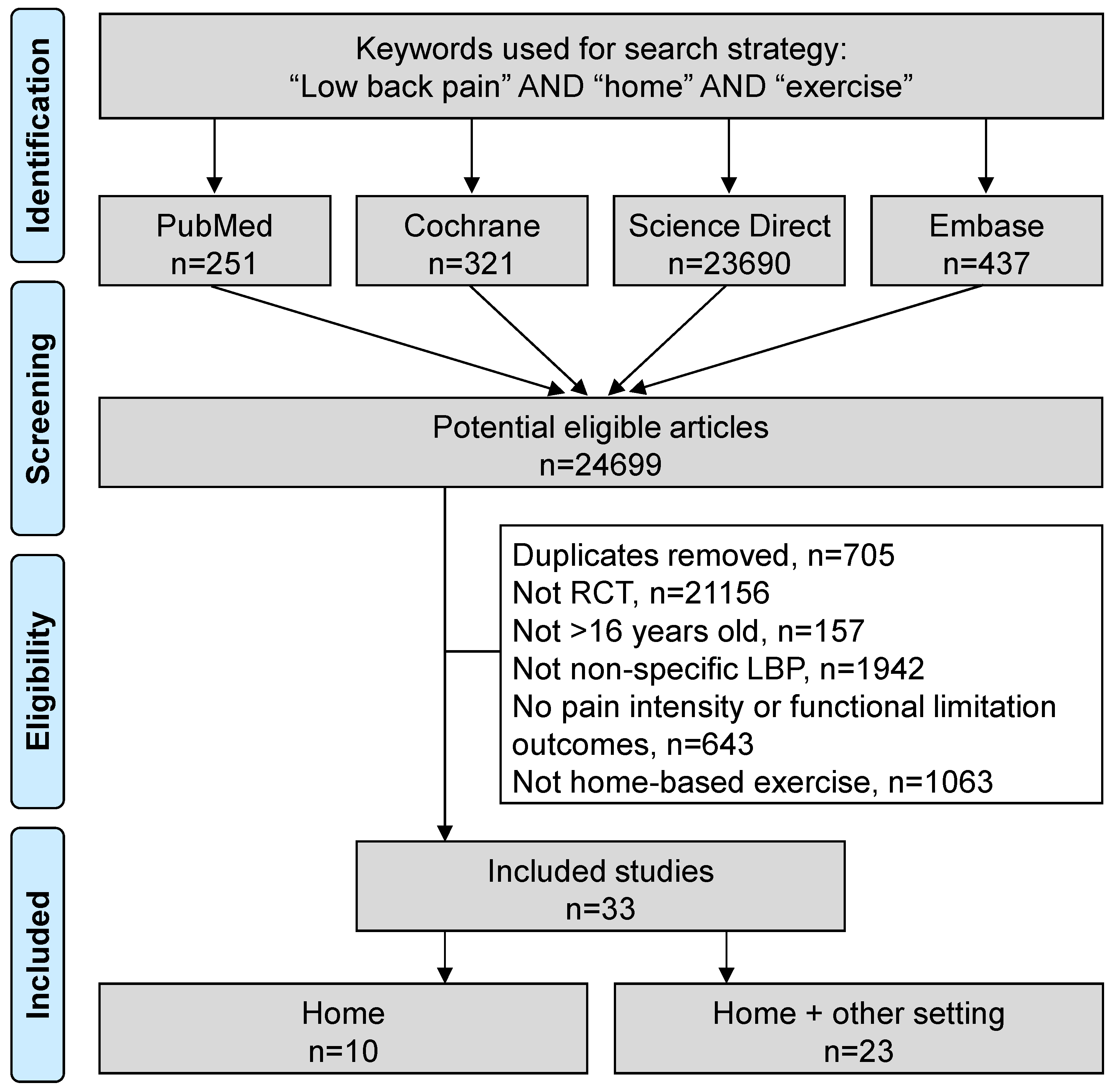
2.1. Literature Search
2.2. Data Extraction
2.3. Quality of Assessment
2.4. Statistical Considerations
3. Results
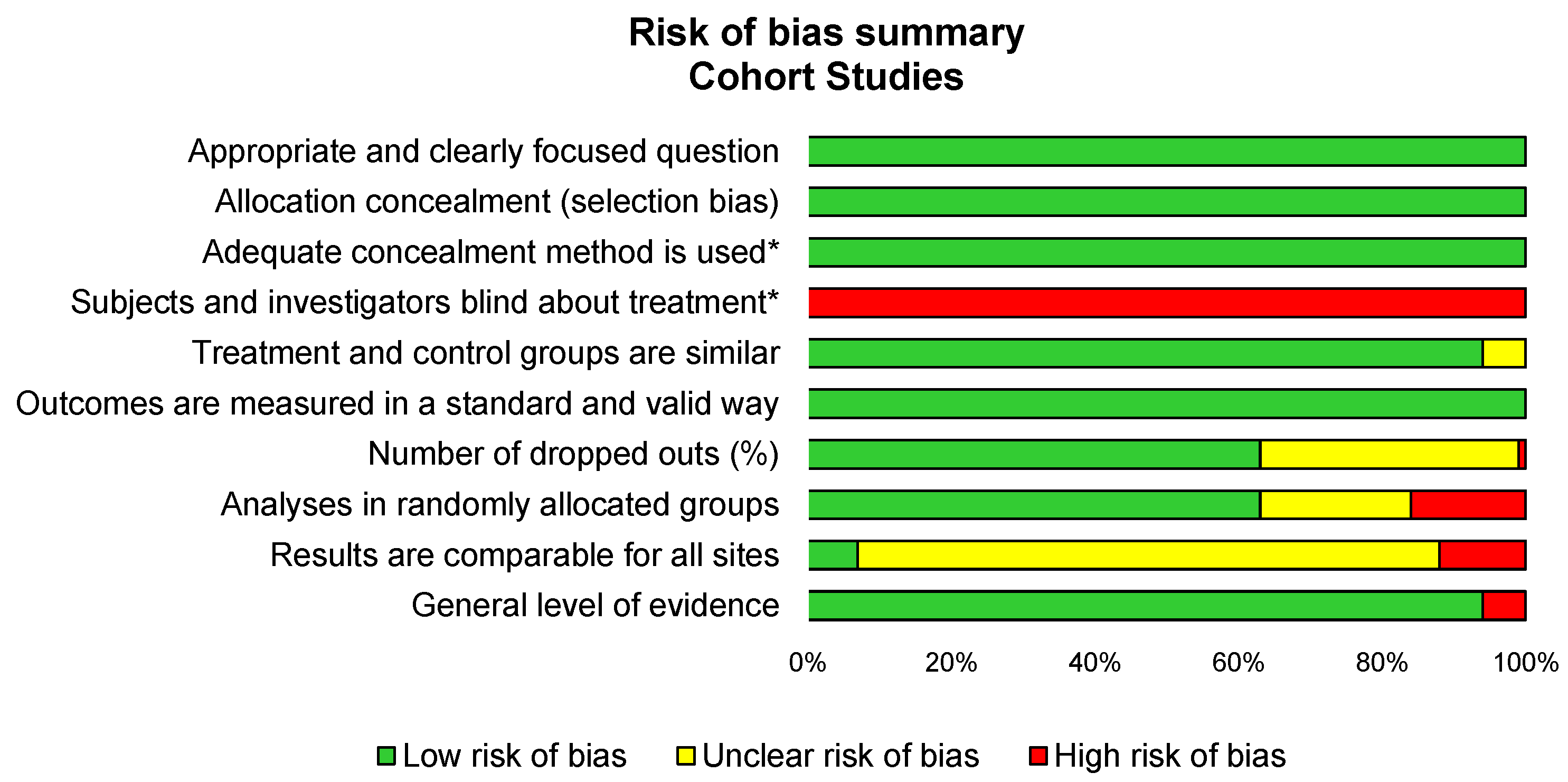
3.1. Quality of Assessment
3.2. Study Designs of Included Articles
3.3. Inclusion and Exclusion Criteria of Included Studies
3.4. Population
3.5. Intervention: Characteristics of Exercise
3.5.1. Type of Exercise
3.5.2. Duration of Intervention
3.5.3. Frequency and Duration of Sessions
3.5.4. Standardization
3.5.5. Supervision
3.5.6. Location
3.6. Outcomes-Pain Intensity and Functional Limitations
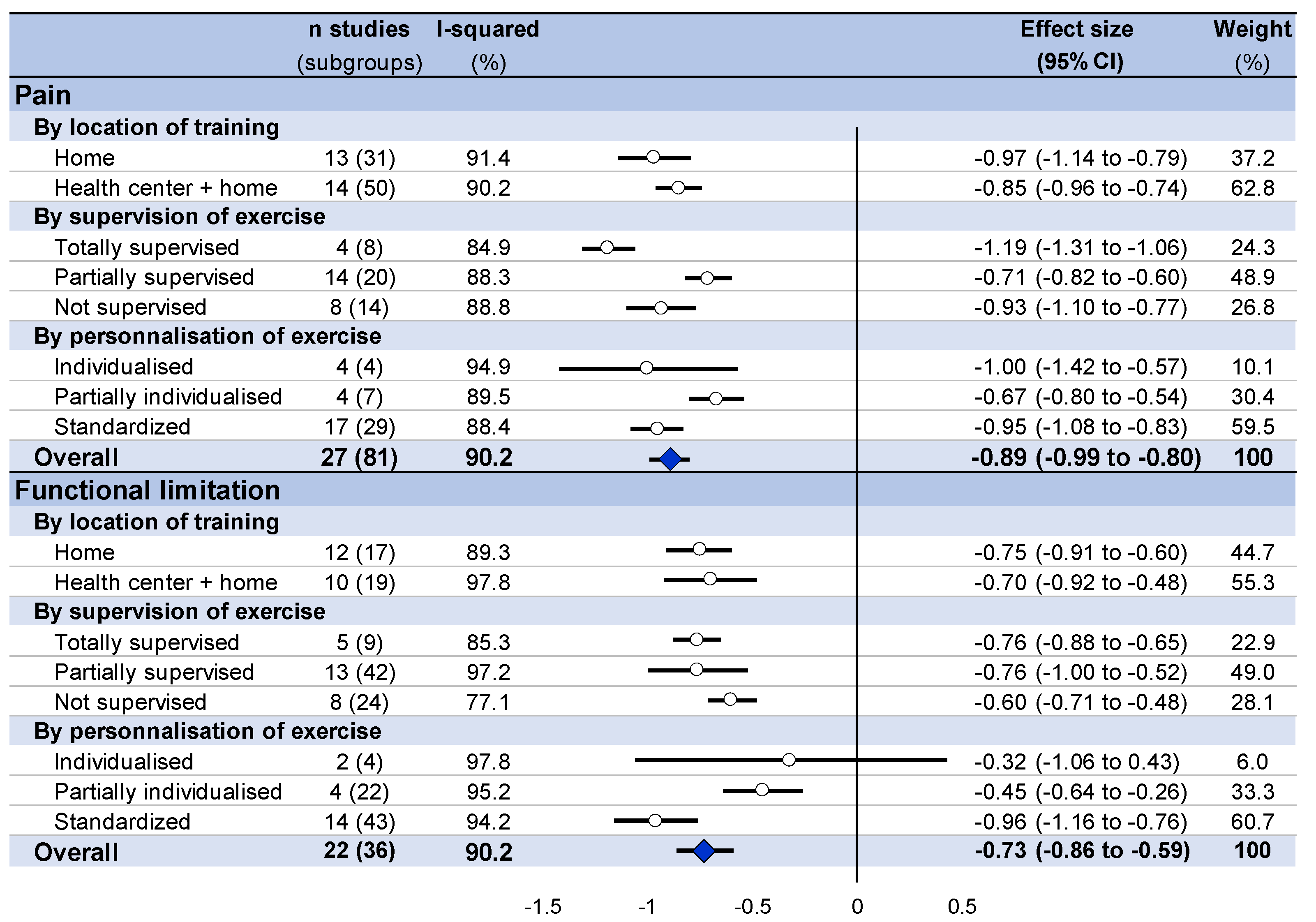
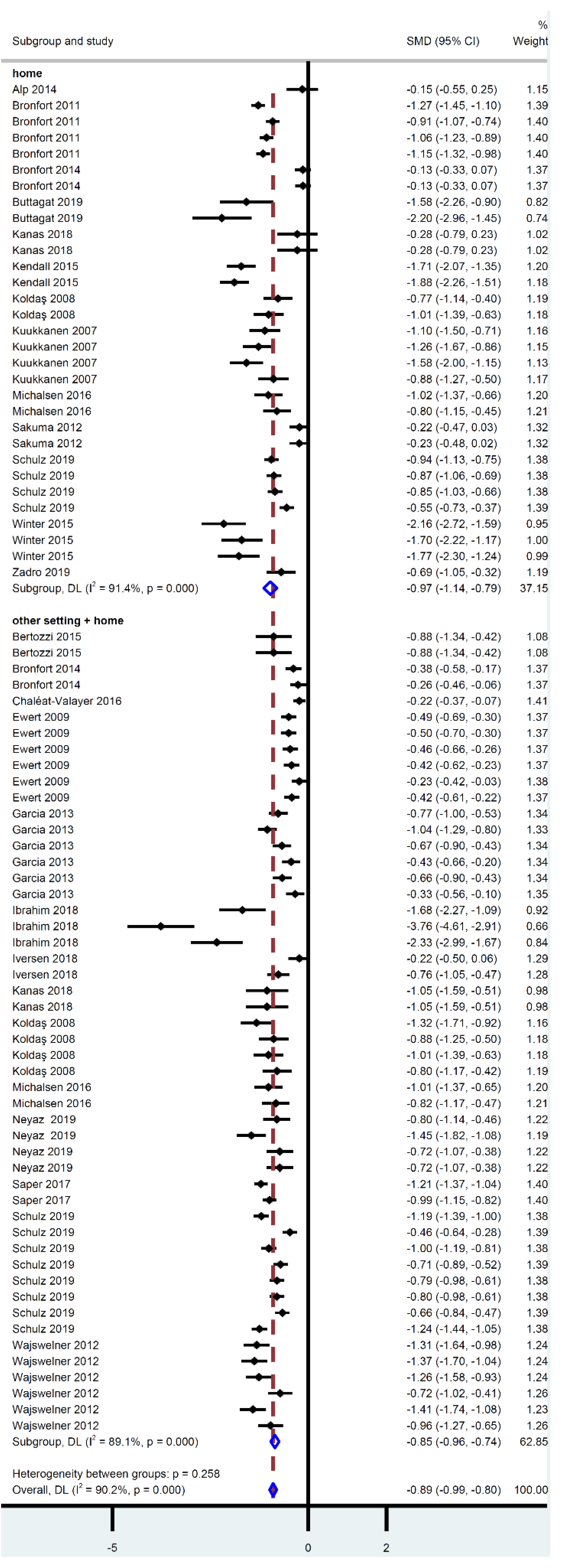
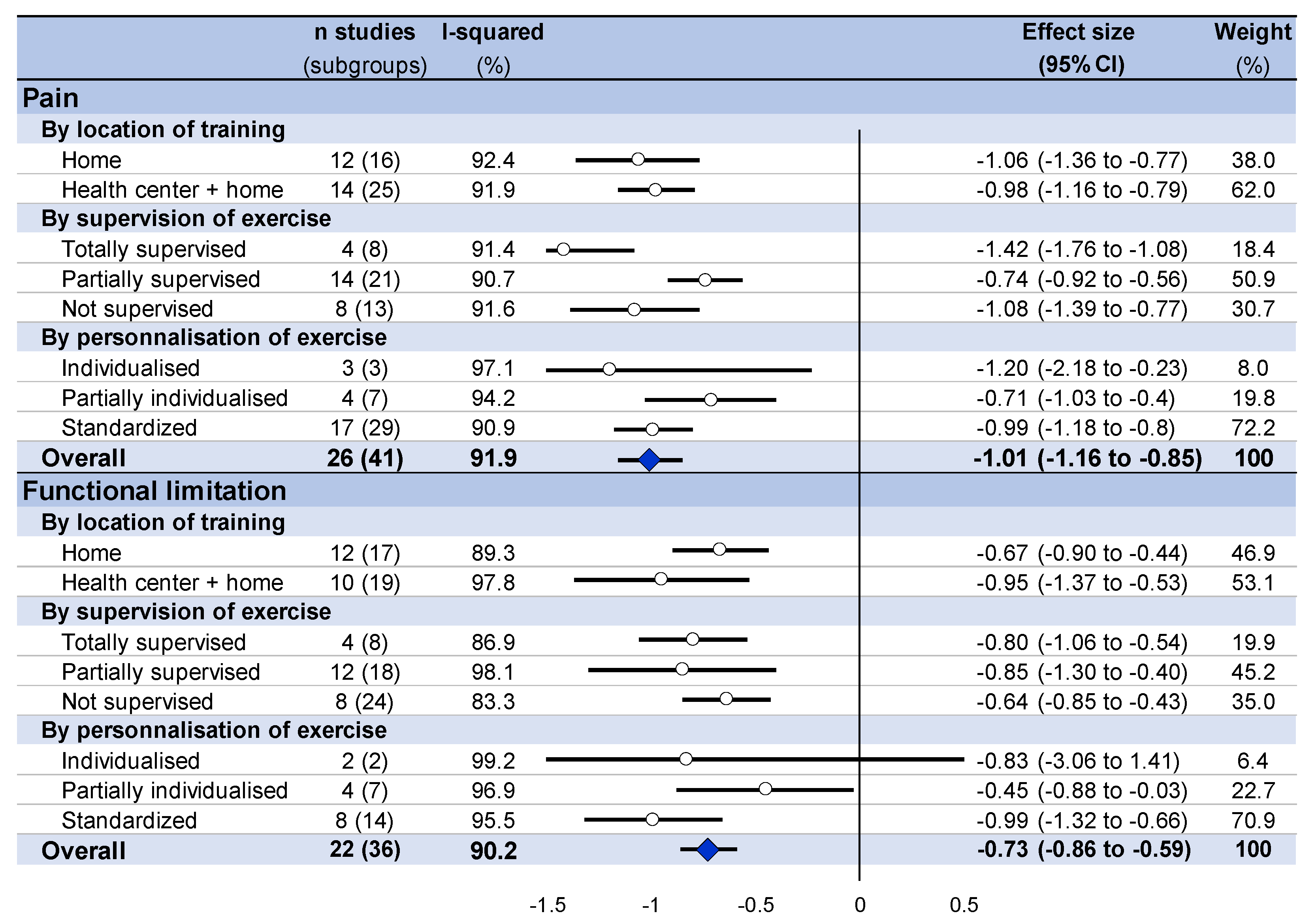
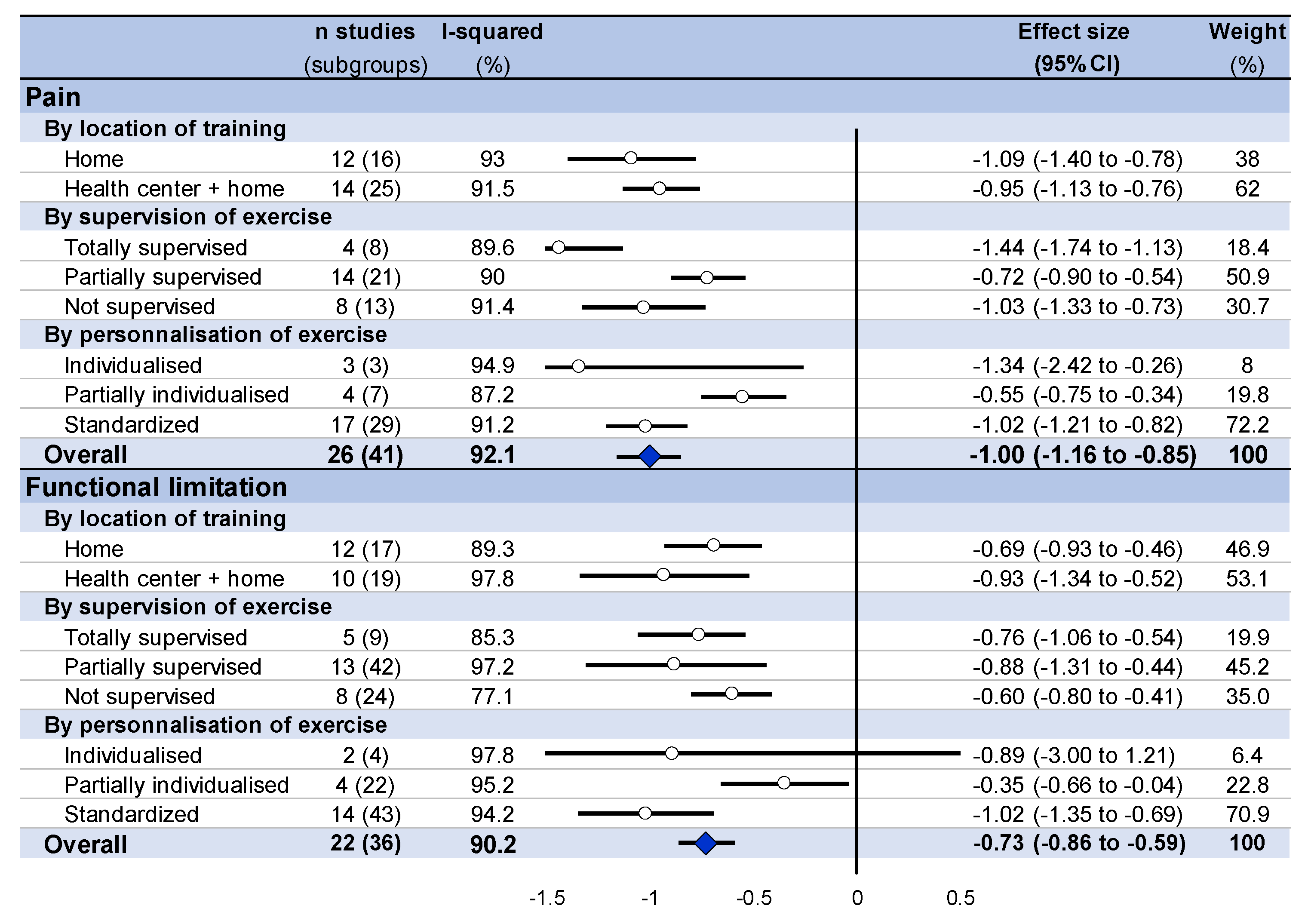
3.7. Meta-Analysis on the Effect of Home-Based Exercise
3.8. Stratification by Characteristics of Training
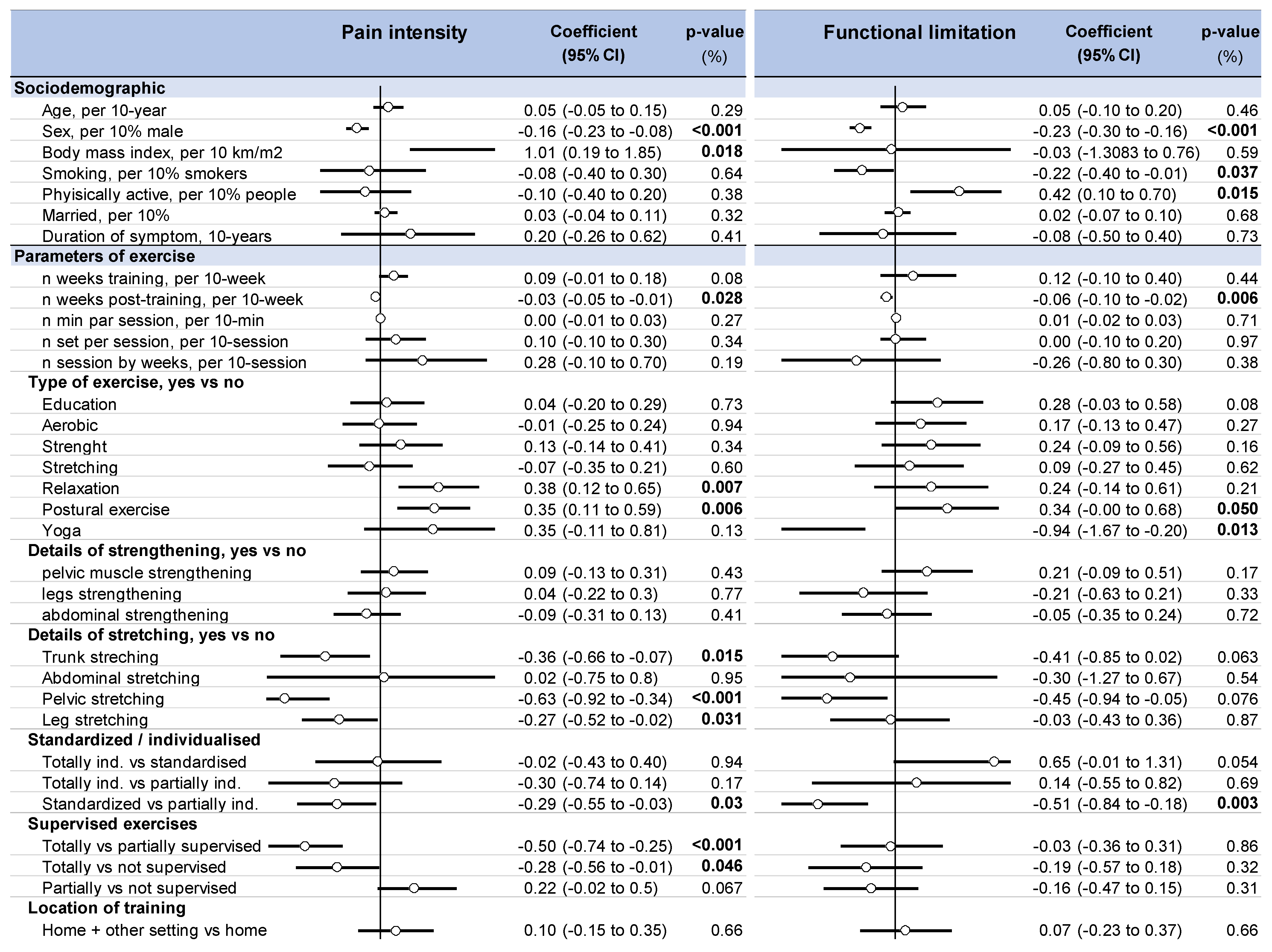
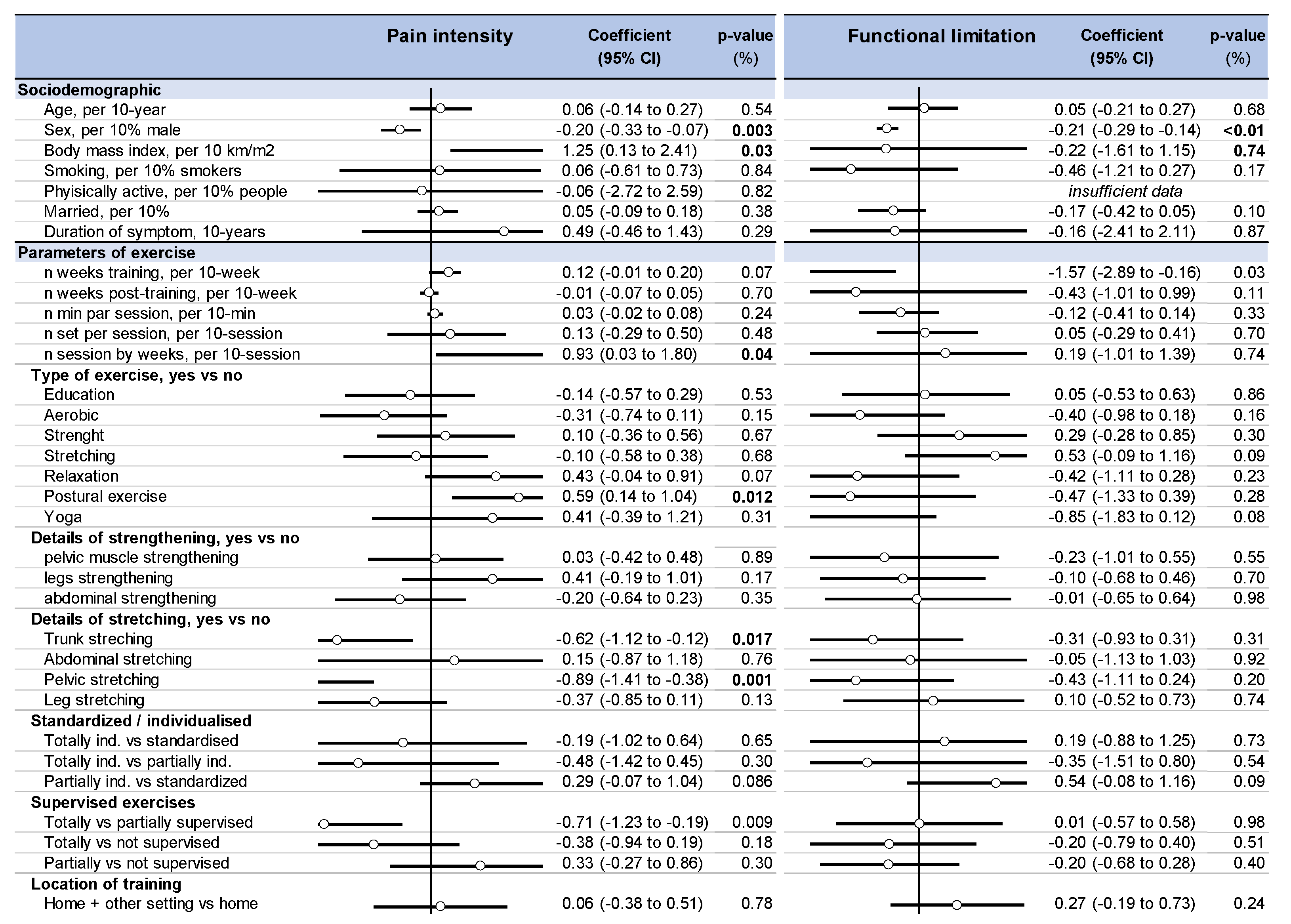
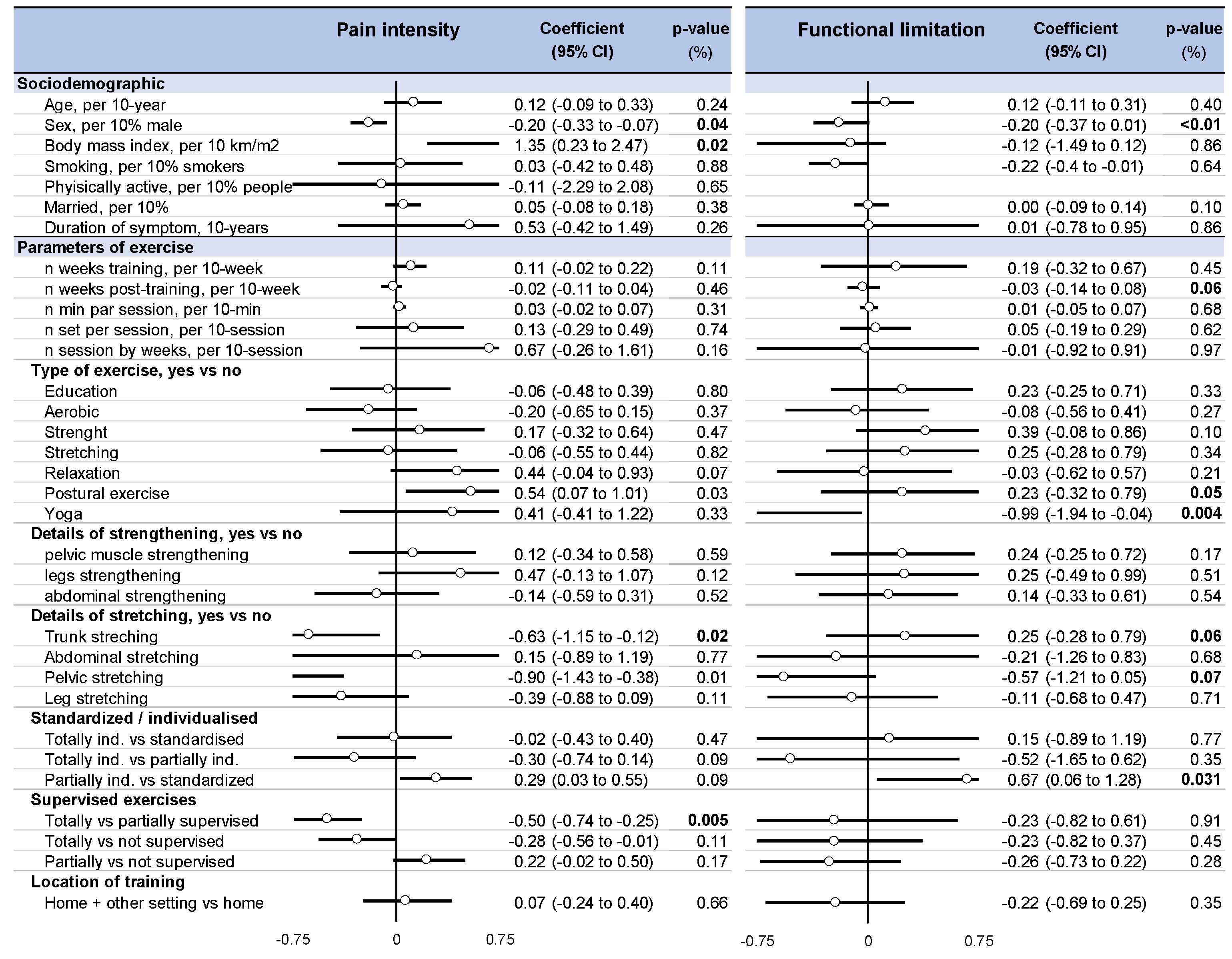
3.9. Metaregressions
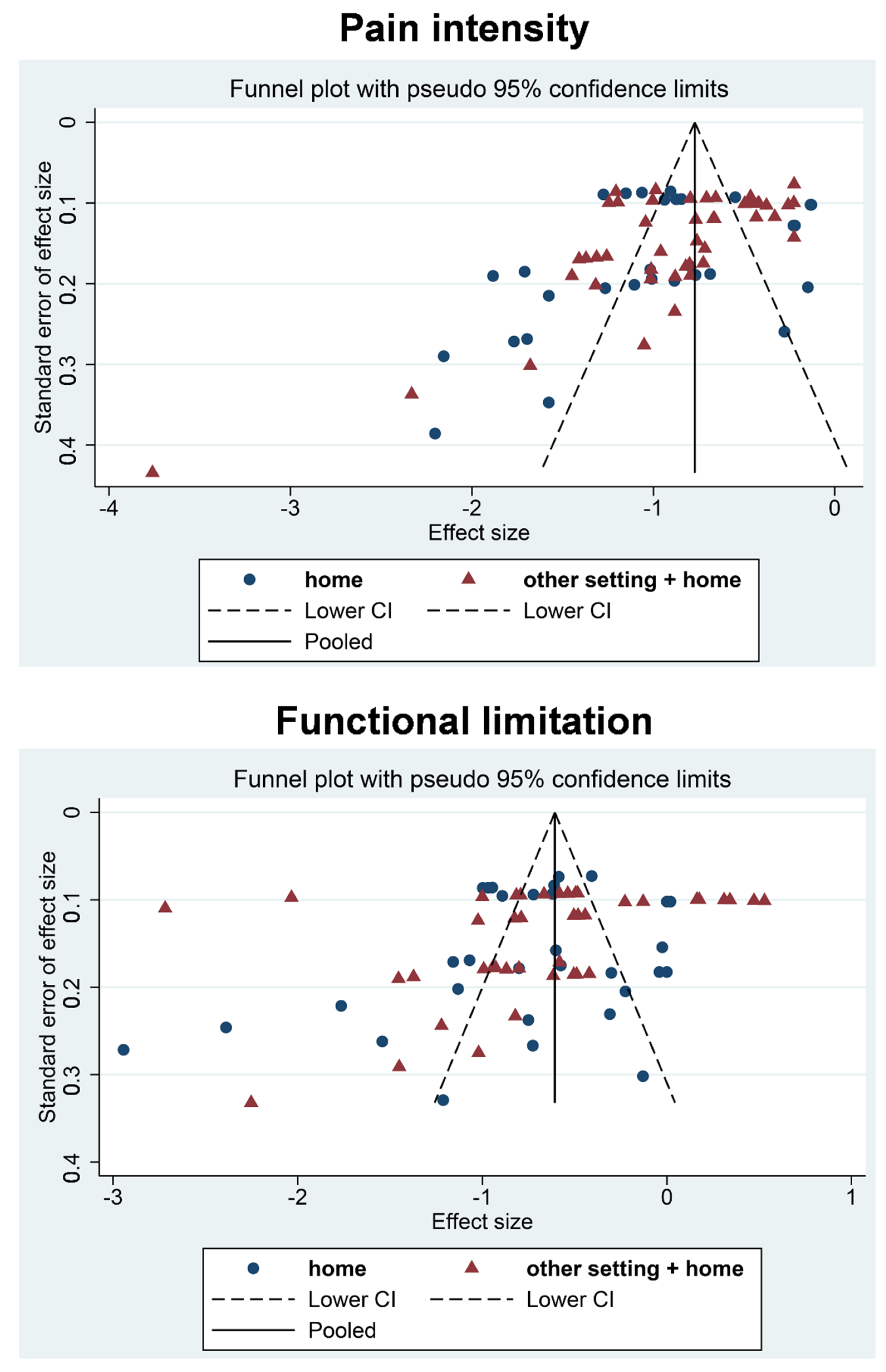
3.10. Sensitivity Analyses
4. Discussion
4.1. The Benefits of Home Exercise Training on LBP Patients
4.2. Which Type of Exercise Training?
4.3. Supervision, Standardization, Frequency, and Duration of Exercise Training
4.4. Predictors of Pain Intensity Improvements
4.5. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
Appendix B

Appendix C

Appendix D

Appendix E

Appendix F

Appendix G

References
- Hoy, D.; Brooks, P.; Blyth, F.; Buchbinder, R. The Epidemiology of low back pain. Best Pract. Res. Clin. Rheumatol. 2010, 24, 769–781. [Google Scholar] [CrossRef]
- Airaksinen, O.; Brox, J.I.; Cedraschi, C.; Hildebrandt, J.; Klaber-Moffett, J.; Kovacs, F.; Mannion, A.F.; Reis, S.; Staal, B.; Ursin, H.; et al. Chapter 4 European guidelines for the management of chronic nonspecific low back pain. Eur. Spine J. 2006, 15, s192–s300. [Google Scholar] [CrossRef] [Green Version]
- Searle, A.; Spink, M.; Ho, A.; Chuter, V. Exercise interventions for the treatment of chronic low back pain: A systematic review and meta-analysis of randomised controlled trials. Clin. Rehabil. 2015, 29, 1155–1167. [Google Scholar] [CrossRef]
- Hayden, J.A.; Wilson, M.N.; Riley, R.D.; Iles, R.; Pincus, T.; Ogilvie, R. Individual recovery expectations and prognosis of outcomes in non-specific low back pain: Prognostic factor review. Cochrane Database Syst. Rev. 2019. [Google Scholar] [CrossRef]
- Kanas, M.; Faria, R.S.; Salles, L.G.; Sorpreso, I.C.E.; Martins, D.; Da Cunha, R.A.; Wajchenberg, M. Home-based exercise therapy for treating non-specific chronic low back pain. Rev. Assoc. Médica Bras. 2018, 64, 824–831. [Google Scholar] [CrossRef]
- Balagué, F.; Mannion, A.F.; Pellise, F.; Cedraschi, C. Non-specific low back pain. Lancet 2012, 379, 482–491. [Google Scholar] [CrossRef] [Green Version]
- Opdenacker, J.; Delecluse, C.; Boen, F. A 2-Year Follow-Up of a Lifestyle Physical Activity Versus a Structured Exercise Intervention in Older Adults. J. Am. Geriatr. Soc. 2011, 59, 1602–1611. [Google Scholar] [CrossRef] [PubMed]
- Chiarotto, A.; Boers, M.; Deyo, R.A.; Buchbinder, R.; Corbin, T.P.; Costa, L.O.; Foster, N.E.; Grotle, M.; Koes, B.W.; Kovacs, F.M.; et al. Core outcome measurement instruments for clinical trials in nonspecific low back pain. Pain 2017, 159, 481–495. [Google Scholar] [CrossRef] [PubMed]
- Bombardier, C. Outcome Assessments in the Evaluation of Treatment of Spinal Disorders. Spine 2000, 25, 3100–3103. [Google Scholar] [CrossRef]
- Ostelo, R.W.J.G.; Deyo, R.A.; Stratford, P.; Waddell, G.; Croft, P.; Von Korff, M.; Bouter, L.M.; Henrica, C. Interpreting change scores for pain and functional status in low back pain: Towards international consensus regarding minimal important change. Spine 2008, 33, 90–94. [Google Scholar] [CrossRef] [Green Version]
- Owen, P.J.; Miller, C.T.; Mundell, N.L.; Verswijveren, S.J.J.M.; Tagliaferri, S.D.; Brisby, H.; Bowe, S.J.; Belavy, D.L. Which specific modes of exercise training are most effective for treating low back pain? Network meta-analysis. Br. J. Sports Med. 2019, 54, 1279–1287. [Google Scholar] [CrossRef]
- Harbour, R.; Miller, J. A new system for grading recommendations in evidence based guidelines. BMJ 2001, 323, 334–336. [Google Scholar] [CrossRef] [Green Version]
- D’Azy, C.B.; Pereira, B.; Chiambaretta, F.; Dutheil, F. Oxidative and Anti-Oxidative Stress Markers in Chronic Glaucoma: A Systematic Review and Meta-Analysis. PLoS ONE 2016, 11, e0166915. [Google Scholar] [CrossRef]
- Lanhers, C.; Pereira, B.; Naughton, G.; Trousselard, M.; Lesage, F.-X.; Dutheil, F. Creatine Supplementation and Upper Limb Strength Performance: A Systematic Review and Meta-Analysis. Sports Med. 2016, 47, 163–173. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Courtin, R.; Pereira, B.; Naughton, G.; Chamoux, A.; Chiambaretta, F.; Lanhers, C.; Dutheil, F. Prevalence of dry eye disease in visual display terminal workers: A systematic review and meta-analysis. BMJ Open 2016, 6, e009675. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- D’Azy, C.B.; Pereira, B.; Naughton, G.; Chiambaretta, F.; Dutheil, F. Antibioprophylaxis in Prevention of Endophthalmitis in Intravitreal Injection: A Systematic Review and Meta-Analysis. PLoS ONE 2016, 11, e0156431. [Google Scholar] [CrossRef]
- Lanhers, C.; Pereira, B.; Naughton, G.; Trousselard, M.; Lesage, F.-X.; Dutheil, F. Creatine Supplementation and Lower Limb Strength Performance: A Systematic Review and Meta-Analyses. Sports Med. 2015, 45, 1285–1294. [Google Scholar] [CrossRef] [PubMed]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.; Colquhoun, H.; Kastner, M.; Levac, D.; Ng, C.; Sharpe, J.P.; Wilson, K.; et al. A scoping review on the conduct and reporting of scoping reviews. BMC Med. Res. Methodol. 2016, 16, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Alp, A.; Mengi, G.; Avsaroglu, A.H.; Mert, M.; Sigirli, D. Efficacy of Core-Stabilization Exercise and Its Comparison with Home-Based Conventional Exercise in Low Back Pain Patients. Bursa Uludag Univ. Res. Inf. Syst. 2014. [Google Scholar] [CrossRef]
- Frih, Z.B.S.; Fendri, Y.; Jellad, A.; Boudoukhane, S.; Rejeb, N. Efficacy and treatment compliance of a home-based rehabilitation programme for chronic low back pain: A randomized, controlled study. Ann. Phys. Rehabil. Med. 2009, 52, 485–496. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bertozzi, L.; Villafañe, J.H.; Capra, F.; Reci, M.; Pillastrini, P. Effect of an Exercise Programme for the Prevention of Back and Neck Pain in Poultry Slaughterhouse Workers. Occup. Ther. Int. 2014, 22, 36–42. [Google Scholar] [CrossRef] [PubMed]
- Bronfort, G.; Maiers, M.J.; Evans, R.L.; Schulz, C.; Bracha, Y.; Svendsen, K.H.; Grimm, R.H.; Owens, E.F.; Garvey, T.A.; Transfeldt, E.E. Supervised exercise, spinal manipulation, and home exercise for chronic low back pain: A randomized clinical trial. Spine J. 2011, 11, 585–598. [Google Scholar] [CrossRef] [PubMed]
- Buttagat, V.; Techakhot, P.; Wiriya, W.; Mueller, M.; Areeudomwong, P. Effectiveness of traditional Thai self-massage combined with stretching exercises for the treatment of patients with chronic non-specific low back pain: A single-blinded randomized controlled trial. J. Bodyw. Mov. Ther. 2020, 24, 19–24. [Google Scholar] [CrossRef]
- Chhabra, H.S.; Sharma, S.; Verma, S. Smartphone app in self-management of chronic low back pain: A randomized controlled trial. Eur. Spine J. 2018, 27, 2862–2874. [Google Scholar] [CrossRef]
- Chaléat-Valayer, E.; Denis, A.; Abelin-Genevois, K.; Zelmar, A.; Siani-Trebern, F.; Touzet, S.; Bergeret, A.; Colin, C.; Fassier, J.B. Long-term effectiveness of an educational and physical intervention for preventing low-back pain recurrence: A randomized controlled trial. Scand. J. Work Environ. Health 2016, 42, 510–519. [Google Scholar] [CrossRef] [Green Version]
- Descarreaux, M.; Normand, M.C.; Laurencelle, L.; Dugas, C. Evaluation of a specific home exercise program for low back pain. J. Manip. Physiol. Ther. 2002, 25, 497–503. [Google Scholar] [CrossRef]
- Ewert, T.; Limm, H.; Wessels, T.; Rackwitz, B.; Von Garnier, K.; Freumuth, R.; Stucki, G. The Comparative Effectiveness of a Multimodal Program Versus Exercise Alone for the Secondary Prevention of Chronic Low Back Pain and Disability. PM&R 2009, 1, 798–808. [Google Scholar] [CrossRef]
- Frost, H.; Lamb, S.; Moffett, K.A.J.; Fairbank, T.J.; Moser, S.J. A fitness programme for patients with chronic low back pain: 2-year follow-up of a randomised controlled trial. Pain 1998, 75, 273–279. [Google Scholar] [CrossRef]
- Garcia, A.N.; Costa, L.D.C.M.; da Silva, T.M.; Gondo, F.L.B.; Cyrillo, F.N.; Costa, R.A.; Costa, L. Effectiveness of Back School Versus McKenzie Exercises in Patients with Chronic Nonspecific Low Back Pain: A Randomized Controlled Trial. Phys. Ther. 2013, 93, 729–747. [Google Scholar] [CrossRef] [Green Version]
- Goode, A.P.; Taylor, S.S.; Hastings, S.N.; Stanwyck, C.; Coffman, C.J.; Allen, K.D. Effects of a Home-Based Telephone-Supported Physical Activity Program for Older Adult Veterans with Chronic Low Back Pain. Phys. Ther. 2018, 98, 369–380. [Google Scholar] [CrossRef]
- Groessl, E.J.; Liu, L.; Chang, D.G.; Wetherell, J.L.; Bormann, J.E.; Atkinson, J.H.; Baxi, S.; Schmalzl, L. Yoga for Military Veterans with Chronic Low Back Pain: A Randomized Clinical Trial. Am. J. Prev. Med. 2017, 53, 599–608. [Google Scholar] [CrossRef] [PubMed]
- Haufe, S.; Wiechmann, K.; Stein, L.; Kück, M.; Smith, A.; Meineke, S.; Zirkelbach, Y.; Duarte, S.R.; Drupp, M.; Tegtbur, U. Low-dose, non-supervised, health insurance initiated exercise for the treatment and prevention of chronic low back pain in employees. Results from a randomized controlled trial. PLoS ONE 2017, 12, e0178585. [Google Scholar] [CrossRef] [Green Version]
- Ibrahim, A.A.; Akindele, M.O.; Ganiyu, S.O. Motor control exercise and patient education program for low resource rural community dwelling adults with chronic low back pain: A pilot randomized clinical trial. J. Exerc. Rehabil. 2018, 14, 851–863. [Google Scholar] [CrossRef] [Green Version]
- Iversen, V.M.; Vasseljen, O.; Mork, P.J.; Berthelsen, I.R.; Børke, J.-B.B.; Berheussen, G.F.; Tveter, A.T.; Salvesen, Ø.; Fimland, M.S. Resistance training in addition to multidisciplinary rehabilitation for patients with chronic pain in the low back: Study protocol. Contemp. Clin. Trials Commun. 2017, 6, 115–121. [Google Scholar] [CrossRef]
- Kendall, K.D.; Emery, C.A.; Wiley, J.P.; Ferber, R. The effect of the addition of hip strengthening exercises to a lumbopelvic exercise programme for the treatment of non-specific low back pain: A randomized controlled trial. J. Sci. Med. Sport 2015, 18, 626–631. [Google Scholar] [CrossRef] [Green Version]
- Doğan, K.; Tur, B.S.; Kurtaiş, Y.; Atay, M.B. Comparison of three different approaches in the treatment of chronic low back pain. Clin. Rheumatol. 2008, 27, 873–881. [Google Scholar] [CrossRef] [PubMed]
- Kuukkanen, T.; Mälkiä, E.; Kautiainen, H.; Pohjolainen, T. Effectiveness of a home exercise programme in low back pain: A randomized five-year follow-up study. Physiother. Res. Int. J. Res. Clin. Phys. Ther. 2007, 12, 213–224. [Google Scholar] [CrossRef] [PubMed]
- Kuukkanen, T.M.; Mälkiä, E.A. An experimental controlled study on postural sway and therapeutic exercise in subjects with low back pain. Clin. Rehabil. 2000, 14, 192–202. [Google Scholar] [CrossRef]
- Miller, J.; Stanley, I.; Moore, K. Videotaped exercise instruction: A randomised controlled trial in musculoskeletal physiotherapy. Physiother. Theory Pract. 2004, 20, 145–154. [Google Scholar] [CrossRef]
- Neyaz, O.; Sumila, L.; Nanda, S.; Wadhwa, S. Effectiveness of Hatha Yoga Versus Conventional Therapeutic Exercises for Chronic Nonspecific Low-Back Pain. J. Altern. Complement. Med. 2019, 25, 938–945. [Google Scholar] [CrossRef]
- Shirado, O.; Doi, T.; Akai, M.; Hoshino, Y.; Fujino, K.; Hayashi, K.; Marui, E.; Iwaya, T. Multicenter Randomized Controlled Trial to Evaluate the Effect of Home-Based Exercise on Patients with Chronic Low Back Pain. Spine 2010, 35, E811–E819. [Google Scholar] [CrossRef] [PubMed]
- Schulz, C.; Evans, R.; Maiers, M.; Schulz, K.; Leininger, B.; Bronfort, G. Spinal manipulative therapy and exercise for older adults with chronic low back pain: A randomized clinical trial. Chiropr. Man Ther. 2019, 27, 1–14. [Google Scholar] [CrossRef] [Green Version]
- Sakuma, Y.; Sasaki-Otomaru, A.; Ishida, S.; Kanoya, Y.; Arakawa, C.; Mochizuki, Y.; Seiishi, Y.; Sato, C. Effect of a Home-Based Simple Yoga Program in Child-Care Workers: A Randomized Controlled Trial. J. Altern. Complement. Med. 2012, 18, 769–776. [Google Scholar] [CrossRef]
- Tottoli, C.R.; van Tulder, M.; da Silva, E.N.; Marques, Y.A.; Martins, W.R.; Carregaro, R.L. Effectiveness and cost-effectiveness of Pilates versus home-based exercises in individuals with chronic non-specific low back pain: Randomised controlled trial protocol. Eur. J. Physiother. 2019, 23, 95–101. [Google Scholar] [CrossRef]
- Wajswelner, H.; Metcalf, B.; Bennell, K. Clinical Pilates versus General Exercise for Chronic Low Back Pain. Med. Sci. Sports Exerc. 2012, 44, 1197–1205. [Google Scholar] [CrossRef]
- Winter, S. Effectiveness of targeted home-based hip exercises in individuals with non-specific chronic or recurrent low back pain with reduced hip mobility: A randomised trial. J. Back Musculoskelet. Rehabil. 2015, 28, 811–825. [Google Scholar] [CrossRef]
- Bronfort, G.; Hondras, M.A.; Schulz, C.; Evans, R.L.; Long, C.R.; Grimm, R. Spinal Manipulation and Home Exercise with Advice for Subacute and Chronic Back-Related Leg Pain. Ann. Intern. Med. 2014, 161, 381–391. [Google Scholar] [CrossRef]
- Michalsen, A.; Kunz, N.; Jeitler, M.; Brunnhuber, S.; Meier, L.; Lüdtke, R.; Büssing, A.; Kessler, C. Effectiveness of focused meditation for patients with chronic low back pain—A randomized controlled clinical trial. Complement. Ther. Med. 2016, 26, 79–84. [Google Scholar] [CrossRef]
- Zadro, J.; Shirley, D.; Simic, M.; Mousavi, S.J.; Ceprnja, D.; Maka, K.; Sung, J.; Ferreira, P. Video-Game–Based Exercises for Older People with Chronic Low Back Pain: A Randomized Controlledtable Trial (GAMEBACK). Phys. Ther. 2018, 99, 14–27. [Google Scholar] [CrossRef] [PubMed]
- Saper, R.B.; LeMaster, C.; Delitto, A.; Sherman, K.J.; Herman, P.M.; Sadikova, E.; Stevans, J.; Keosaian, J.E.; Cerrada, C.J.; Femia, A.L.; et al. Yoga, Physical Therapy, or Education for Chronic Low Back Pain. Ann. Intern. Med. 2017, 167, 85–94. [Google Scholar] [CrossRef]
- Bernardelli, G.; Vigna, L.; Nava, C.; Colonna, V.D.G.; Andersen, L.L.; Consonni, D.; Riboldi, L. Physical Activity in Healthcare Workers with Low Back Pain. J. Occup. Environ. Med. 2020, 62, e245–e249. [Google Scholar] [CrossRef]
- Anwer, S.; Alghadir, A.; Brismée, J.-M. Effect of Home Exercise Program in Patients with Knee Osteoarthritis. J. Geriatr. Phys. Ther. 2016, 39, 38–48. [Google Scholar] [CrossRef]
- Hayden, J.A.; van Tulder, M.; Tomlinson, G. Systematic Review: Strategies for Using Exercise Therapy to Improve Outcomes in Chronic Low Back Pain. Ann. Intern. Med. 2005, 142, 776–785. [Google Scholar] [CrossRef] [PubMed]
- DeBusk, R.F.; Stenestrand, U.; Sheehan, M.; Haskell, W.L. Training Effects of Long Versus Short Bouts of Exercise in Healthy Subjects. Am. J. Cardiol. 1990, 65, 1010–1013. [Google Scholar] [CrossRef]
- Kim, H.; Reece, J.; Kang, M. Effects of Accumulated Short Bouts of Exercise on Weight and Obesity Indices in Adults: A Meta-Analysis. Am. J. Health Promot. 2020, 34, 96–104. [Google Scholar] [CrossRef]
- Sukhato, K.; Lotrakul, M.; Dellow, A.; Ittasakul, P.; Thakkinstian, A.; Anothaisintawee, T. Efficacy of home-based non-pharmacological interventions for treating depression: A systematic review and network meta-analysis of randomised controlled trials. BMJ Open 2017, 7, e014499. [Google Scholar] [CrossRef]
- Flynn, A. Home-based prescribed exercise improves balance-related activities in people with Parkinson’s disease and has ben-efits similar to centre-based exercise: A systematic review. J. Physiother. 2019, 65, 189–199. [Google Scholar] [CrossRef]
- Wuytack, F.; Devane, D.; Stovold, E.; McDonnell, M.; Casey, M.; McDonnell, T.J.; Gillespie, P.; Raymakers, A.; Lacasse, Y.; McCarthy, B. Comparison of outpatient and home-based exercise training programmes for COPD: A systematic review and meta-analysis. Respirology 2017, 23, 272–283. [Google Scholar] [CrossRef] [Green Version]
- Anderson, L.; Thompson, D.; Oldridge, N.; Zwisler, A.-D.; Rees, K.; Martin, N.; Taylor, R.S. Exercise-based cardiac rehabilitation for coronary heart disease. Cochrane Database Syst. Rev. 2016, 1, CD001800. [Google Scholar] [CrossRef] [Green Version]
- Van Middelkoop, M.; Rubinstein, S.M.; Verhagen, A.P.; Ostelo, R.; Koes, B.; van Tulder, M.W. Exercise therapy for chronic nonspecific low-back pain. Best Pract. Res. Clin. Rheumatol. 2010, 24, 193–204. [Google Scholar] [CrossRef] [PubMed]
- Karlsson, M.; Bergenheim, A.; Larsson, M.E.H.; Nordeman, L.; Van Tulder, M.; Bernhardsson, S. Effects of exercise therapy in patients with acute low back pain: A systematic review of systematic reviews. Syst. Rev. 2020, 9, 1–25. [Google Scholar] [CrossRef]
- Saner, J.; Bergman, E.M.; de Bie, R.A.; Sieben, J.M. Low back pain patients’ perspectives on long-term adherence to home-based exercise programmes in physiotherapy. Musculoskelet. Sci. Pract. 2018, 38, 77–82. [Google Scholar] [CrossRef] [PubMed]
- Lacroix, A.; Hortobágyi, T.; Beurskens, R.; Granacher, U. Effects of Supervised vs. Unsupervised Training Programs on Balance and Muscle Strength in Older Adults: A Systematic Review and Meta-Analysis. Sports Med. 2017, 47, 2341–2361. [Google Scholar] [CrossRef]
- Ferreira, M.L.; Smeets, R.J.; Kamper, S.J.; Ferreira, P.H.; Machado, L.A. Can we explain heterogeneity among randomized clinical trials of exercise for chronic back pain? A meta-regression analysis of randomized controlled trials. Phys. Ther. 2010, 90, 1383–1403. [Google Scholar] [CrossRef]
- Alschuler, K.N.; Hoodin, F.; Murphy, S.L.; Rice, J.; Geisser, M.E. Factors contributing to physical activity in a chronic low back pain clinical sample: A comprehensive analysis using continuous ambulatory monitoring. Pain 2011, 152, 2521–2527. [Google Scholar] [CrossRef] [PubMed]
- Mura, G. Active exergames to improve cognitive functioning in neurological disabilities: A systematic review and meta-analysis. Eur. J. Phys. Rehabil. Med. 2018, 54, 13. [Google Scholar] [CrossRef]
- Brownson, R.C.; Baker, E.A.; Housemann, R.A.; Brennan, L.K.; Bacak, S.J. Environmental and Policy Determinants of Physical Activity in the United States. Am. J. Public Health 2001, 91, 1995–2003. [Google Scholar] [CrossRef] [PubMed]
- Medina-Mirapeix, F.; Escolar-Reina, P.; Gascón-Cánovas, J.J.; Montilla-Herrador, J.; Jimeno-Serrano, F.J.; Collins, S.M. Predictive factors of adherence to frequency and duration components in home exercise programs for neck and low back pain: An observational study. BMC Musculoskelet. Disord. 2009, 10, 155. [Google Scholar] [CrossRef] [Green Version]
- Murphy, M.H.; Lahart, I.; Carlin, A.; Murtagh, E. The Effects of Continuous Compared to Accumulated Exercise on Health: A Meta-Analytic Review. Sports Med. 2019, 49, 1585–1607. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bener, A.; El-Rufaie, O.F.; Siyam, A.; Abuzeid, M.S.O.; Toth, F.; Lovasz, G. Epidemiology of low back pain in the United Arab Emirates. APLAR J. Rheumatol. 2004, 7, 189–195. [Google Scholar] [CrossRef]
- Byberg, L. Total mortality after changes in leisure time physical activity in 50 year old men: 35 year follow-up of population based cohort. BMJ 2009. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dutheil, F.; Comptour, A.; Morlon, R.; Mermillod, M.; Pereira, B.; Baker, J.S.; Charkhabi, M.; Clinchamps, M.; Bourdel, N. Autism spectrum disorder and air pollution: A systematic review and meta-analysis. Environ. Pollut. 2021, 278, 116856. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Characteristics of Indivuals | Exercise Setting | Type of Intervention | Volume of | Exercise | Outco | Mes | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Study | Design | Country | n gp | Age (Mean ± SD) | Sex (% Men) | Home | Other | Strength | Stretching | Relaxation | Aerobic | Education | Postural | Yoga | Other | Number of weeks | n Session/Week | Duration of Session | Pain | Functionnal Disability |
| Alp 2014 | RCT | Turkey | 24 | 48 ± 27.5 | 0 | X | X | X | 6 weeks | 3 | 45–60 min | VAS | RMDQ | |||||||
| 24 | 51 ± 39.8 | 0 | X | X | X | 7 | ? | |||||||||||||
| Ben Salah Frih 2009 | RCT | Tunisia | 54 | 34.7 ± 1.14 | 24.1 | X | X | X | X | 4 weeks | 7 | 30 min | VAS | |||||||
| 53 | 36.9 ± 1.29 | 26.4 | X | X | X | Proprioception exercise | 4 weeks | 3 | 90 min | |||||||||||
| Bernadelli 2020 | RCT | Italy | 51 | 50.5 ± 9.7 | 25.5 | X | X | X | X | 7 weeks | 1 | 30 min | RMDQ | |||||||
| 50 | 51.9 ± 8.1 | 16 | X | X | X | |||||||||||||||
| Bertozzi 2015 | RCT | Italy | 20 | 42.7 ± 8.7 | - | X | X | X | X | X | 5 weeks | 2 | 60 min | VAS | RMDQ | |||||
| 20 | 47.5 ± 7.5 | - | X | X | X | X | ? | ? | ||||||||||||
| Bronfort 2014 | RCT | USA | 96 | 57.1 ± 12 | 41 | X | X | X | X | X | 12 weeks | 7 | ? | NPRS | RMDQ | |||||
| 96 | 57.7 ± 11.9 | 32 | X | X | X | X | ||||||||||||||
| Bronfort 2011 | RCT | USA | 100 | 44.5 ± 11.8 | 43 | X | X | X | 12 weeks | 2 | 60 min | |||||||||
| 100 | 45.2 ± 10.8 | 44 | Spinal manipulative therapy | 12 weeks | 2 | 60 min | NPRS | RMDQ | ||||||||||||
| 101 | 45.6 ± 10.3 | 41.6 | X | X | X | X | 12 weeks | 7 | 60 min | |||||||||||
| Buttagat 2019 | RCT | Thailand | 11 | 39.7 ± 17.4 | 27.2 | X | X | Thai self-massage | 4 weeks | 3 | ? | VAS | ODI | |||||||
| 11 | 41.3 ± 15.8 | 9 | X | X | ? | ? | ? | |||||||||||||
| Chaléat-Valayer 2016 | RCT | France | 171 | 47.1 ± 8.5 | 23 | X | X | X | X | X | X | rhythmic exercise | 2 years | 7 | 10 min | VAS | QBPDS | |||
| Descarreaux 2002 | RCT | Canada | 10 | 33.1 | 70 | X | X | 3 weeks | 14 | ? | VAS | ODI | ||||||||
| 20 | 35.0 | 35 | X | X | X | 6 weeks | 14 | ? | ||||||||||||
| Ewert 2009 | RCT | Germany | 100 | 37.9 ± 11.6 | 8.0 | X | X | X | X | X | X | X | X | cognitive– behavioral approach/stress control + warm up | 13 weeks | 2 | 60 min | WHYMPI | sf36-pcs | |
| 102 | 41.1 ± 10.8 | 5.9 | X | X | X | X | X | X | Warm up | 13 weeks | ? | ? | ||||||||
| Frost 1998 | RCT | England | 36 | 34.2 ± 9.4 | - | X | X | X | X | X | X | X | 4 weeks | 2 | ? | MODI | ||||
| 35 | 38.5 ± 9.3 | - | X | X | X | X | ? | ? | ||||||||||||
| Garcia 2013 | RCT | Brasil | 74 | 54.2 ± 1.57 | 31.0 | X | X | X | X | X | 24 weeks | 7 | 240 min | VAS | RMDQ | |||||
| 74 | 53.7 ± 1.53 | 21.6 | X | X | X | X | X | |||||||||||||
| Goode 2018 | RCT | England | 20 | 69.6 ± 3.5 | 95 | X | X | X | X | X | X | |||||||||
| 20 | 69.5 ± 4,0 | 90 | X | X | X | X | X | X | Activity pacing + Cognitive restructuring | 12 weeks | ? | ? | RMDQ | |||||||
| 20 | 71.9 ± 6.5 | 95 | X | X | ||||||||||||||||
| Groessl 2017 | RCT | USA | 76 | 53.3 ± 12.7 | 73 | X | X | X | Breathing | 12 weeks | 7 | 60 min | BPI | RMDQ | ||||||
| 76 | 53.6 ± 13.9 | 75 | none | - | - | |||||||||||||||
| Haufe 2017 | RCT | Germany | 112 | 43.5 ± 9.7 | - | X | X | X | 20 weeks | 3 | 20 min | |||||||||
| 114 | 41.9 ± 10.6 | - | 20 weeks | 3 | 20 min | VAS | ODI | |||||||||||||
| 10 | 49.9 ± 8.8 | 80 | X | X | X | X | X | X | 6 weeks | 2 | 20 min | |||||||||
| Ibrahim 2018 | RCT | Nigeria | 10 | 48.5 ± 14.9 | 70 | X | X | X | X | X | X | 6 weeks | 2 | 20 min | NPRS | ODI | ||||
| 10 | 50.3 ± 9.1 | 90 | X | X | X | X | X | 1 | ? | |||||||||||
| Iversen 2018 | RCT | Norway | 37 | 43 ± 13 | 46 | X | X | X | X | X | X | 12 weeks | 4 | ? | ||||||
| 37 | 47 ± 11 | 41 | X | X | X | X | X | X | ball games + body awareness + circle training | 12 weeks | 4.5 | ? | NPRS | ODI | ||||||
| 34 | 45 ± 15 | 55 | none | - | - | |||||||||||||||
| Kanas 2018 | RCT | Brasil | 17 | - | - | X | X | X | X | 8 weeks | 3 | ? | NPRS | RMDQ | ||||||
| 13 | - | - | X | X | X | X | X | |||||||||||||
| Kendall 2015 | RCT | Canada | 40 | 33 | 55 | X | X | X | X | RTUS | 6 weeks | ? | ? | VAS | ODI | |||||
| Australia | 40 | 41 | 40 | X | X | X | X | RTUS | ||||||||||||
| Koldaş 2008 | RCT | Turkey | 20 | 37.1 ± 6.5 | 21.1 | X | X | X | X | X | X | 10 | ? | |||||||
| 20 | 41.5 ± 8.3 | 22.2 | X | X | X | X | X | 6 weeks | 7 | ? | VAS | RMDQ | ||||||||
| 20 | 42.1 ± 9.5 | 22.2 | X | X | X | X | 7 | ? | ||||||||||||
| Kuukkanen 2000 | RCT | Finland | 29 | 39.9 ± 8.9 | - | X | X | warm-up + Balance + coordination | 12 weeks | ? | ? | |||||||||
| 29 | 39.9 ± 7.9 | - | X | X | 12 weeks | ? | ? | ODI | ||||||||||||
| 28 | 39.9 ± 7.9 | - | none | - | - | |||||||||||||||
| Kuukkanen 2007 | RCT | Finland | 28 | 40 ± 7.9 | 46.4 | X | X | X | 12 weeks | 7 | ? | Borg CR-10 scale | ODI | |||||||
| Miller 2007 | RCT | England | 98 | 44.1 ± 16.2 | - | X | 5 weeks | ? | ? | |||||||||||
| 137 | 43.7 ± 14.8 | - | X | 5 weeks | ? | ? | RMDQ | |||||||||||||
| 150 | 44.9 ± 15.4 | - | - | - | - | |||||||||||||||
| Michalsen 2016 | RCT | Germany | 32 | 55.5 ± 10.6 | - | X | X | Jyoti meditaion | 8 weeks | 7 | 25 min | VAS | RMDQ | |||||||
| Germany | 36 | 54.8 ± 10.6 | - | X | X | X | 20 min | |||||||||||||
| Neyaz 2019 | RCT | India | 35 | 33 | - | X | X | X | X | X | X | 6 weeks | 7 | 30–35 min | DVPRS | RMDQ | ||||
| 35 | 38 | - | X | X | X | X | ||||||||||||||
| Shirado 2010 | RCT | Japan | 103 | 42.0 ± 11.6 | 47.5 | X | X | X | X | 8 weeks | 14 | ? | VAS | |||||||
| 98 | 42.5 ± 12.3 | 40.8 | X | Massage | ? | |||||||||||||||
| Schulz 2019 | RCT | USA | 81 | 72.5 ± 5.6 | 43.2 | X | X | X | X | X | X | Balance exercise + massage | 2 | 45–60 min | ||||||
| 80 | 73.6 ± 5.3 | 52.5 | X | X | X | X | X | X | Balance exercise + massage | 12 weeks | 1 | 60 min | NPRS | RMDQ | ||||||
| 80 | 74.7 ± 5.6 | 50.0 | X | X | X | X | X | 1 | 15 min | |||||||||||
| Saper 2017 | RCT | USA | 127 | 46.4 ± 10.4 | - | X | X | X | X | breathing | ? | 75 min | ||||||||
| 129 | 46.4 ± 11,0 | - | X | X | X | X | 12 weeks | 7 | 60 min | NPRS | RMDQ | |||||||||
| 64 | 44.2 ± 10.8 | - | X | ? | ? | |||||||||||||||
| Sakuma 2012 | RCT | Japan | 67 | 32.6 ± 11.5 | - | X | X | X | 2 weeks | 7 | 9 min | VAS | ||||||||
| 31 | 35.8 ± 13 | none | - | - | ||||||||||||||||
| Tottoli 2019 | RCT | Brazil | 72 | - | X | X | X | X | 6 weeks | 2 | 50 min | VAS | BQBPSDQ | |||||||
| 72 | X | X | X | X | Warm up | |||||||||||||||
| Wajswelner 2012 | RCT | Australia | 44 | 49.3 ± 14.1 | X | X | X | Breathing | 24 weeks | 60 min | NPRS | |||||||||
| 43 | 48.9 ± 16.4 | X | X | X | X | Swiss ball | ||||||||||||||
| Winter 2015 | RCT | Australia | 12 | 45.9 ± 13.3 | X | X | 5 | |||||||||||||
| 13 | 48.9 ± 7.2 | X | X | 6 weeks | 5 | NPRS | MODI | |||||||||||||
| 13 | 38.3 ± 12.8 | X | X | X | 3 | |||||||||||||||
| Zadro 2019 | RCT | Australia | 30 | 68.8 ± 5.5 | 40.0 | X | X | X | X | 8 weeks | 3 | 60 min | NPRS | RMDQ | ||||||
| 30 | 67.8 ± 6 | 56.6 | none | |||||||||||||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Quentin, C.; Bagheri, R.; Ugbolue, U.C.; Coudeyre, E.; Pélissier, C.; Descatha, A.; Menini, T.; Bouillon-Minois, J.-B.; Dutheil, F. Effect of Home Exercise Training in Patients with Nonspecific Low-Back Pain: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2021, 18, 8430. https://doi.org/10.3390/ijerph18168430
Quentin C, Bagheri R, Ugbolue UC, Coudeyre E, Pélissier C, Descatha A, Menini T, Bouillon-Minois J-B, Dutheil F. Effect of Home Exercise Training in Patients with Nonspecific Low-Back Pain: A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health. 2021; 18(16):8430. https://doi.org/10.3390/ijerph18168430
Chicago/Turabian StyleQuentin, Chloé, Reza Bagheri, Ukadike C. Ugbolue, Emmanuel Coudeyre, Carole Pélissier, Alexis Descatha, Thibault Menini, Jean-Baptiste Bouillon-Minois, and Frédéric Dutheil. 2021. "Effect of Home Exercise Training in Patients with Nonspecific Low-Back Pain: A Systematic Review and Meta-Analysis" International Journal of Environmental Research and Public Health 18, no. 16: 8430. https://doi.org/10.3390/ijerph18168430