
The Role of Virtual Reality as a Psychological Intervention for Mental Health Disturbances during the COVID-19 Pandemic: A Narrative Review

 , , , and
, , , and 
Abstract
:1. Introduction
2. COVID-19 Pandemic, Stress, and Mental Health Disturbances
3. The Use of Computer-Based Technology as a Psychological Intervention: The Role of VR
4. Who Is Using VR? An Online Survey on the Characteristics of the Respondents
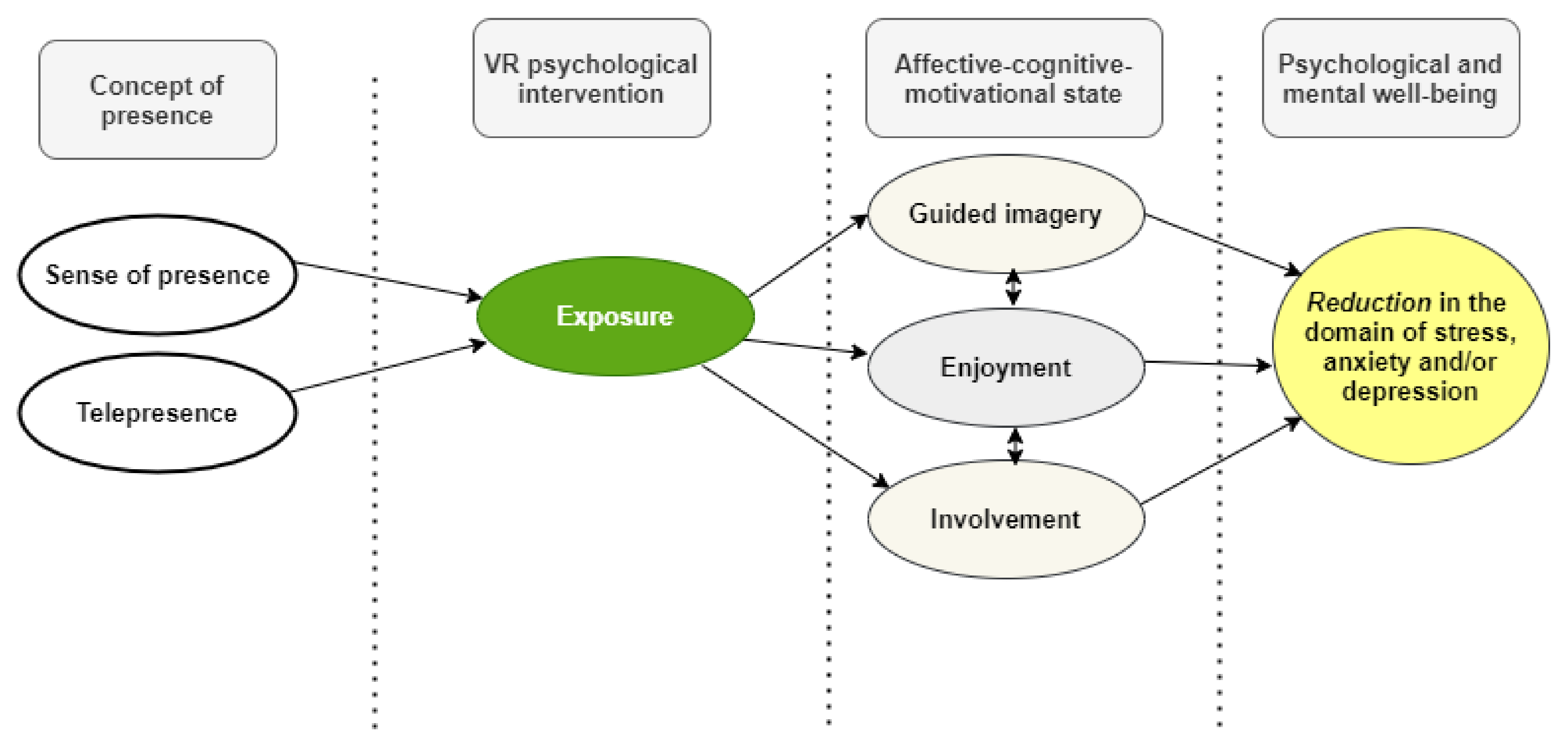
5. A Research Model for the Usefulness of VR as an Intervention: The Role of Sense of Presence Guided Imagery, Enjoyment, and Involvement
6. VR vs. 2-Dimension Intervention for Psychological Stress during the COVID-19 Pandemic
7. VR Development for Psychological Intervention: Technological Innovation, Assessment, and Troubleshooting
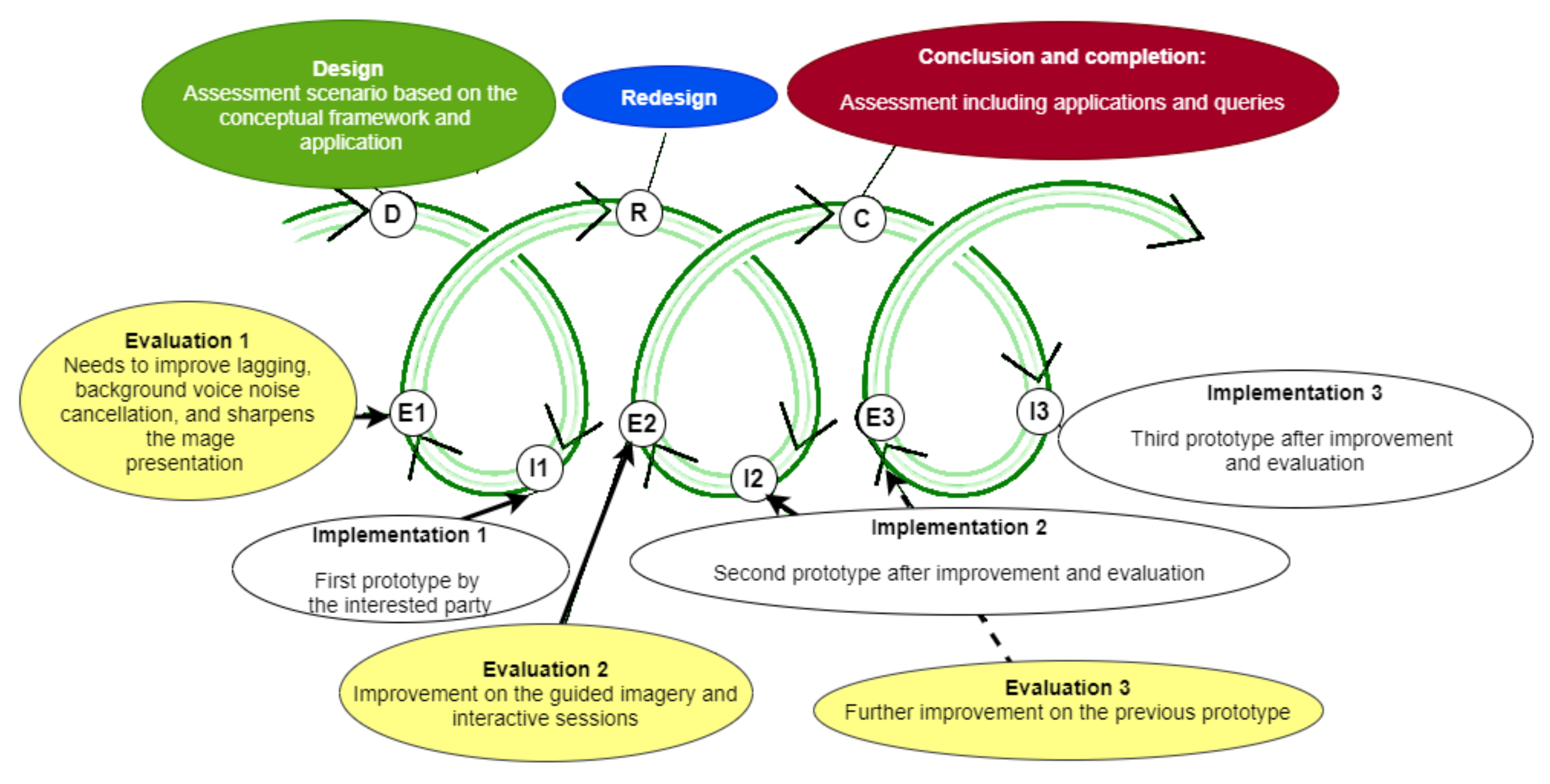
8. VR Design-Based Research (DBR) for Psychological Intervention for Mental Health: The Evolution of Software Development
9. How to Create a Scenario? The Interventional Settings
10. Implications for Expanding the Use of VR in Communities Experiencing COVID-19 Mental Health Disparities
11. Limitations
12. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Li, H.; Liu, S.-M.; Yu, X.-H.; Tang, S.-L.; Tang, C.-K. Coronavirus disease 2019 (COVID-19): Current status and future perspectives. Int. J. Antimicrob. Agents 2020, 55, 105951. [Google Scholar] [CrossRef] [PubMed]
- WHO. Coronavirus disease (COVID-19) Pandemic, World Health Organization. 2020. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019 (accessed on 16 November 2020).
- Xiao, C. A Novel Approach of Consultation on 2019 Novel Coronavirus (COVID-19)-Related Psychological and Mental Problems: Structured Letter Therapy. Psychiatry Investig. 2020, 17, 175–176. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jordan, E.J.; Moran, C.; Godwyll, J.M. Does tourism really cause stress? A natural experiment utilizing ArcGIS Survey123. Curr. Issues Tour. 2019, 24, 1–15. [Google Scholar] [CrossRef]
- Da Silva, F.C.T.; Neto, M.L.R. Psychiatric symptomatology associated with depression, anxiety, distress, and insomnia in health professionals working in patients affected by COVID-19: A systematic review with meta-analysis. Prog. Neuropsychopharmacol. Biol. Psychiatry 2021, 104, 110057. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.; Zhao, N. Generalized anxiety disorder, depressive symptoms and sleep quality during COVID-19 outbreak in China: A web-based cross-sectional survey. Psychiatry Res. 2020, 288, 112954. [Google Scholar] [CrossRef] [PubMed]
- Vindegaard, N.; Benros, M.E. COVID-19 pandemic and mental health consequences: Systematic review of the current evidence. Brain Behav. Immun. 2020, 89, 531–542. [Google Scholar] [CrossRef]
- Cao, W.; Fang, Z.; Hou, G.; Han, M.; Xu, X.; Dong, J.; Zheng, J. The psychological impact of the COVID-19 epidemic on college students in China. Psychiatry Res. 2020, 287, 112934. [Google Scholar] [CrossRef]
- Brooks, S.K.; Webster, R.K.; Smith, L.E.; Woodland, L.; Wessely, S.; Greenberg, N.; Rubin, G.J. The psychological impact of quarantine and how to reduce it: Rapid review of the evidence. Lancet 2020, 395, 912–920. [Google Scholar] [CrossRef] [Green Version]
- Kaur, S. The coronavirus pandemic in Malaysia: A commentary. Psychol. Trauma Theory Res. Prac. Policy 2020, 12, 482–484. [Google Scholar] [CrossRef]
- Kaplan, S. The restorative benefits of nature: Toward an integrative framework. J. Environ. Psychol. 1995, 15, 169–182. [Google Scholar] [CrossRef]
- Chen, C.C.; Petrick, J.F.; Shahvali, M. Tourism experiences as a stress reliever: Examining the effects of tourism recovery experiences on life satisfaction. J. Travel Res. 2016, 55, 150–160. [Google Scholar] [CrossRef]
- Hartig, T.; Mang, M.; Evans, G.W. Restorative Effects of Natural Environment Experiences. Environ. Behav. 1991, 23, 3–26. [Google Scholar] [CrossRef]
- Anderson, A.P.; Mayer, M.D.; Fellows, A.M.; Cowan, D.R.; Hegel, M.T.; Buckey, J.C. Relaxation with immersive natural scenes presented using virtual reality. Aerosp. Med. Hum. Perform. 2017, 88, 520–526. [Google Scholar] [CrossRef] [PubMed]
- McCloy, R.; Stone, R. Science, medicine, and the future. Virtual reality in surgery. BMJ 2001, 323, 912–915. [Google Scholar] [CrossRef] [PubMed]
- Tashjian, V.C.; Mosadeghi, S.; Howard, A.R.; Lopez, M.; Dupuy, T.; Reid, M.; Martinez, B.; Ahmed, S.; Dailey, F.; Robbins, K.; et al. Virtual Reality for Management of Pain in Hospitalized Patients: Results of a Controlled Trial. JMIR Ment. Health 2017, 4, e9. [Google Scholar] [CrossRef]
- Mohammad, E.B.; Ahmad, M. Virtual reality as a distraction technique for pain and anxiety among patients with breast cancer: A randomized control trial. Palliat. Support Care 2019, 17, 29–34. [Google Scholar] [CrossRef]
- Curtin, L.L. The Yerkes-Dodson law. Nurs. Manag. 1984, 15, 7–8. [Google Scholar]
- Selye, H. The general adaptation syndrome and the diseases of adaptation. J. Clin. Endocrinol. Metab. 1946, 6, 117–230. [Google Scholar] [CrossRef]
- Baum, A. Stress, intrusive imagery, and chronic distress. Health Psychol. 1990, 9, 653–675. [Google Scholar] [CrossRef]
- Dolnicar, S.; Yanamandram, V.; Cliff, K. The contribution of vacations to quality of life. Ann. Tour. Res. 2012, 39, 59–83. [Google Scholar] [CrossRef] [Green Version]
- Felton, J.S. Does vacation enable recuperation? Changes in well-being associated with time away from work. Strauss-Blasche et al. Occup Med 2000; 50: 167-172. Occup. Med. 2000, 50, 534. [Google Scholar] [CrossRef] [Green Version]
- Marwah, S. Practical Tips for 22 Mental and Behavioural Disorders; Educreation Publishing: Bilaspur, India, 2019. [Google Scholar]
- Chang, J.; Yuan, Y.; Wang, D. Mental health status and its influencing factors among college students during the epidemic of COVID-19. Nan Fang Yi Ke Da Xue Xue Bao 2020, 40, 171–176. (In Chinese) [Google Scholar] [CrossRef]
- Chi, X.; Becker, B.; Yu, Q.; Willeit, P.; Jiao, C.; Huang, L.; Hossain, M.M.; Grabovac, I.; Yeung, A.; Lin, J.; et al. Prevalence and Psychosocial Correlates of Mental Health Outcomes Among Chinese College Students During the Coronavirus Disease (COVID-19) Pandemic. Front. Psychiatry 2020, 11, 803. [Google Scholar] [CrossRef]
- Elmer, T.; Mepham, K.; Stadtfeld, C. Students under lockdown: Comparisons of students’ social networks and mental health before and during the COVID-19 crisis in Switzerland. PLoS ONE 2020, 15, e0236337. [Google Scholar] [CrossRef]
- Li, Y.; Wang, Y.; Jiang, J.; Valdimarsdóttir, U.A.; Fall, K.; Fang, F.; Song, H.; Lu, D.; Zhang, W. Psychological distress among health professional students during the COVID-19 outbreak. Psychol. Med. 2021, 11, 1952–1954. [Google Scholar] [CrossRef]
- Liang, S.-W.; Chen, R.-N.; Liu, L.-L.; Li, X.-G.; Chen, J.-B.; Tang, S.-Y.; Zhao, J.-B. The Psychological Impact of the COVID-19 Epidemic on Guangdong College Students: The Difference Between Seeking and Not Seeking Psychological Help. Front. Psychol. 2020, 11, 2231. [Google Scholar] [CrossRef]
- Son, C.; Hegde, S.; Smith, A.; Wang, X.; Sasangohar, F. Effects of COVID-19 on College Students’ Mental Health in the United States: Interview Survey Study. J. Med. Internet Res. 2020, 22, e21279. [Google Scholar] [CrossRef]
- Sundarasen, S.; Chinna, K.; Kamaludin, K.; Nurunnabi, M.; Baloch, G.M.; Khoshaim, H.B.; Hossain, S.F.A.; Sukayt, A. Psychological Impact of COVID-19 and Lockdown among University Students in Malaysia: Implications and Policy Recommendations. Int. J. Environ. Res. Public Health 2020, 17, 6206. [Google Scholar] [CrossRef]
- Chu, D.K.; Akl, E.A.; Duda, S.; Solo, K.; Yaacoub, S.; Schünemann, H.J. COVID-19 Systematic Urgent Review Group Effort (SURGE) study authors. Physical distancing, face masks, and eye protection to prevent person-to-person transmission of SARS-CoV-2 and COVID-19: A systematic review and meta-analysis. Lancet 2020, 395, 1973–1987. [Google Scholar] [CrossRef]
- Iberdrola. 2020. Available online: https://www.iberdrola.com (accessed on 16 November 2021).
- Tussyadiah, I.P.; Wang, D.; Jung, T.H.; Dieck, M.C.T. Virtual reality, presence, and attitude change: Empirical evidence from tourism. Tour. Manag. 2018, 66, 140–154. [Google Scholar] [CrossRef]
- Kimiecik, J.C.; Harris, A.T. What Is Enjoyment? A Conceptual/Definitional Analysis with Implications for Sport and Exercise Psychology. J. Sport Exerc. Psychol. 1996, 18, 247–263. [Google Scholar] [CrossRef]
- Witmer, B.G.; Singer, M.J. Measuring Presence in Virtual Environments: A Presence Questionnaire. Presence Teleoper. Virtual Environ. 1998, 7, 225–240. [Google Scholar] [CrossRef]
- Brom, C.; Děchtěrenko, F.; Frollová, N.; Stárková, T.; Bromová, E.; D’Mello, S.K. Education, enjoyment or involvement? Affective-motivational mediation during learning from a complex computerized simulation. Comput. Educ. 2017, 114, 236–254. [Google Scholar] [CrossRef]
- Hruby, F.; Sánchez, L.F.Á.; Ressl, R.; Escobar-Briones, E.G. An Empirical Study on Spatial Presence in Immersive Geo-Environments. PFG—J. Photogramm. Remote Sens. Geoinf. Sci. 2020, 88, 155–163. [Google Scholar] [CrossRef] [Green Version]
- Siani, A.; Marley, S.A. Impact of the recreational use of virtual reality on physical and mental wellbeing during the Covid-19 lockdown. Health Technol. 2021, 11, 425–435. [Google Scholar] [CrossRef] [PubMed]
- Williams, R.; Jenkins, D.A.; Ashcroft, D.M.; Brown, B.; Campbell, S.; Carr, M.J.; Cheraghi-Sohi, S.; Kapur, N.; Thomas, O.; Webb, R.T.; et al. Diagnosis of physical and mental health conditions in primary care during the COVID-19 pandemic: A retrospective cohort study. Lancet Public Health 2020, 5, e543–e550. [Google Scholar] [CrossRef]
- Lai, J.; Ma, S.; Wang, Y.; Cai, Z.; Hu, J.; Wei, N.; Wu, J.; Du, H.; Chen, T.; Li, R.; et al. Factors associated with mental health outcomes among health care workers exposed to coronavirus disease 2019. JAMA Netw. Open 2020, 3, e203976. [Google Scholar] [CrossRef]
- Rosenman, R.; Tennekoon, V.; Hill, L.G. Measuring bias in self-reported data. Int. J. Behav. Health Res. 2011, 2, 320–332. [Google Scholar] [CrossRef]
- Yang, T.; Lai, I.K.W.; Bin Fan, Z.; Mo, Q.M. The impact of a 360° virtual tour on the reduction of psychological stress caused by COVID-19. Technol. Soc. 2021, 64, 101514. [Google Scholar] [CrossRef]
- Kim, D.; Ko, Y.J. The impact of virtual reality (VR) technology on sport spectators’ flow experience and satisfaction. Comput. Hum. Behav. 2019, 93, 346–356. [Google Scholar] [CrossRef]
- Kim, M.J.; Hall, C.M. A hedonic motivation model in virtual reality tourism: Comparing visitors and non-visitors. Int. J. Inf. Manag. 2019, 46, 236–249. [Google Scholar] [CrossRef]
- Van Damme, K.; All, A.; De Marez, L.; Van Leuven, S. 360° Video Journalism: Experimental Study on the Effect of Immersion on News Experience and Distant Suffering. Journal. Stud. 2019, 20, 2053–2076. [Google Scholar] [CrossRef]
- Zarzuela, M.; Pernas, F.J.D.; Calzon, S.M.; Ortega, D.G.; Rodriguez, M.A. Educational tourism through a virtual reality platform. In Proceedings of the 2013 International Conference on Virtual and Augmented Reality in Education, Puerto de la Cruz, Spain, 7–8 November 2013; MartinGutierrez, J., Ginters, E., Eds.; Elsevier Science: Amsterdam, The Netherlands, 2013; pp. 382–388. [Google Scholar]
- Waller, M.; Mistry, D.; Jetly, R.; Frewen, P. Meditating in Virtual Reality 3: 360° Video of Perceptual Presence of Instructor. Mindfulness 2021, 12, 1424–1437. [Google Scholar] [CrossRef]
- Gross David, C.; Stanney, K.M.; Cohn, L.J. Evoking Affordances in Virtual Environments via Sensory-Stimuli Substitution. Presence Teleoper. Virtual Environ. 2005, 14, 482–491. [Google Scholar] [CrossRef]
- Bogomolova, K.; Sam, A.H.; Misky, A.T.; Gupte, C.M.; Strutton, P.H.; Hurkxkens, T.J.; Hierck, B.P. Development of a Virtual Three-Dimensional Assessment Scenario for Anatomical Education. Anat. Sci. Educ. 2021, 14, 385–393. [Google Scholar] [CrossRef]
- Wang, F.; Hannafin, M.J. Design-based research and technology-enhanced learning environments. Educ. Technol. Res. Dev. 2005, 53, 5–23. [Google Scholar] [CrossRef]
- Dolmans, D.H.J.M.; Tigelaar, D. Building bridges between theory and practice in medical education using a design-based research approach: AMEE Guide No. 60. Med. Teach. 2012, 34, 1–10. [Google Scholar] [CrossRef]
- Anderson, T.; Shattuck, J. Design-based research: A decade of progress in education research? Educ. Res. 2012, 41, 16–25. [Google Scholar] [CrossRef] [Green Version]
- Zheng, L. A systematic literature review of design-based research from 2004 to 2013. J. Comput. Educ. 2015, 2, 399–420. [Google Scholar] [CrossRef] [Green Version]
- Rasouli, B.; Aliabadi, K.; Aradkani, S.P.; Ahmady, S.; Asgari, M. Determining Components of Medical Instructional Design based on Virtual Reality by Research Synthesis. J. Med. Educ. Dev. 2020, 14, 232–244. [Google Scholar] [CrossRef]
- Zydney, J.M.; Warner, Z.; Angelone, L. Learning through experience: Using design based research to redesign protocols for blended synchronous learning environments. Comput. Educ. 2020, 143, 103678. [Google Scholar] [CrossRef]
- Birt, J.; Cowling, M. Assessing mobile mixed reality affordances as a comparative visualization pedagogy for design communication. Res. Learn. Technol. 2018, 26. [Google Scholar] [CrossRef] [Green Version]
- Riva, G.; Bernardelli, L.; Browning, M.H.E.M.; Castelnuovo, G.; Cavedoni, S.; Chirico, A.; Cipresso, P.; de Paula, D.M.B.; Di Lernia, D.; Fernández-Álvarez, J.; et al. COVID Feel Good—An Easy Self-Help Virtual Reality Protocol to Overcome the Psychological Burden of Coronavirus. Front. Psychiatry 2020, 11, 563319. [Google Scholar] [CrossRef] [PubMed]
- Alyan, E.; Combe, T.; Rambli, D.R.A.; Sulaiman, S.; Merienne, F.; Diyana, N. The Influence of Virtual Forest Walk on Physiological and Psychological Responses. Int. J. Environ. Res. Public Health 2021, 18, 11420. [Google Scholar] [CrossRef]
- Rutkowski, S.; Szczegielniak, J.; Szczepańska-Gieracha, J. Evaluation of the Efficacy of Immersive Virtual Reality Therapy as a Method Supporting Pulmonary Rehabilitation: A Randomized Controlled Trial. J. Clin. Med. 2021, 10, 352. [Google Scholar] [CrossRef]
- Reips, U.-D.; Funke, F. Interval-level measurement with visual analogue scales in Internet-based research: VAS Generator. Behav. Res. Methods 2008, 40, 699–704. [Google Scholar] [CrossRef]
- Grant, S.; Aitchison, T.; Henderson, E.; Christie, J.; Zare, S.; McMurray, J.; Dargie, H. A comparison of the reproducibility and the sensitivity to change of visual analogue scales, Borg scales, and Likert scales in normal subjects during submaximal exercise. Chest 1999, 116, 1208–1217. [Google Scholar] [CrossRef]
- Osman, A.; Wong, J.L.; Bagge, C.L.; Freedenthal, S.; Gutierrez, P.M.; Lozano, G. The Depression Anxiety Stress Scales-21 (DASS-21): Further Examination of Dimensions, Scale Reliability, and Correlates. J. Clin. Psychol. 2012, 68, 1322–1338. [Google Scholar] [CrossRef]
- Henry, J.D.; Crawford, J.R. The short-form version of the Depression Anxiety Stress Scales (DASS-21): Construct validity and normative data in a large non-clinical sample. Br. J. Clin. Psychol. 2005, 44, 227–239. [Google Scholar] [CrossRef] [Green Version]
- Kolbe, L.; Jaywant, A.; Gupta, A.; Vanderlind, W.M.; Jabbour, G. Use of virtual reality in the inpatient rehabilitation of COVID-19 patients. Gen. Hosp. Psychiatry 2021, 71, 76–81. [Google Scholar] [CrossRef]
- Berry, N.; Lobban, F.; Bucci, S. A qualitative exploration of service user views about using digital health interventions for self-management in severe mental health problems. BMC Psychiatry 2019, 19, 35. [Google Scholar] [CrossRef] [Green Version]
- Li, J.; Theng, Y.-L.; Foo, S. Game-Based Digital Interventions for Depression Therapy: A Systematic Review and Meta-Analysis. Cyberpsychol. Behav. Soc. Netw. 2014, 17, 519–527. [Google Scholar] [CrossRef] [Green Version]
- Fleming, T.M.; Bavin, L.; Stasiak, K.; Hermansson-Webb, E.; Merry, S.N.; Cheek, C.; Lucassen, M.; Lau, H.M.; Pollmuller, B.; Hetrick, S. Serious Games and Gamification for Mental Health: Current Status and Promising Directions. Front. Psychiatry 2017, 7, 215. [Google Scholar] [CrossRef] [Green Version]
- Girden, E.R. ANOVA: Repeated Measures; Sage: Thousand Oaks, CA, USA, 1992. [Google Scholar]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Study Design | Country | Setting | Inclusion Criteria | Exclusion Criteria | Intervention | Exposure Measurement Scale | Outcome Measurement | Comparator/Control | Statistics (E.G., OR/RR, p-Value, 95% CI) | VR-Based Intervention (Outcome) |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Waller 2021 [47] | RCT | Canada | Not defined | Not defined | Not controlled for, but participants evaluated for life events, childhood events, traumatic events, PTSD, and life experiences before commencing study | Non-VR group (1) traditional face-to-face (in vivo [IV] method), (2) pre-recorded 360° video viewed by standard laptop computer monitor (2D format), and (3) prerecorded 360° video viewed through an HMD (VR condition; 3D format) | A modified emotional questionnaire, Buddhist Affective States, Meditation Breath Attention Scores Meditative Experience Questionnaire | Experiences of relaxation, less distractibility from the process of breathing, and less fatigue | 3D (VR) vs. 2D format | Qualitative thematic analysis | When compared to the 2D format, VR meditations were associated with more significant |
| Riva 2020 [57] | Multicentric, pragmatic pilot randomized controlled trial | Italy | Online |
|
| The 10-min “Secret Garden” 360° VR experience | Perceived Stress Scale (PSS) Depression Anxiety Stress Scale (DASS-21) Beck Hopelessness Scale (BHS) Social Connectedness Scale (SCS) | A reduction in anxiety, depression, perceived stress, and hopelessness, as measured by DASS-21, PSS, and BHS. A reduction in state anxiety and subjective distress, as measured by SUDS. An increase in relaxation, as measured by SRSI3. | Control (waiting list) vs. Two-Group Random Assignment Pretest–Post-test Design | N/A | No intervention (at a protocol level) |
| Alyan 2021 [58] | Cross-sectional | Malaysia | Online | Healthy university students | Eye impairment | VR intervention with a forest environment, i.e., one realistic experience (RE) and the other dream-like state experience (DE) | Physiological Index, i.e., the heart rate (HR) and skin conductance level (SCL) Physiological measure, i.e., Profile of Mood States (POMS) questionnaire | Relaxation in the domain of the psychological index and low HR and better SCL | Healthy control in RE and DE | Two analytical methods were used: (1) for the HR and SCL data before and after the LDT, related paired t-tests were carried out to verify whether the LDT played a role in increasing stress levels, and (2) for the same indicators (HR and SCL), the differences b | The use of VR led to significant decreases in participants’ psychological and physiological stress |
| Rutkowski 2021 [59] | RCT | Poland | Pulmonary rehabilitation conducted in a ward setting | Patients with chronic obstructive pulmonary disease (COPD), age 45–85 years; anxiety or depressive symptom score of >8 on the Hospital Anxiety and Depression Scale (HADS) | Cognitive impairment; inability to self-complete the research questionnaires, presence of disturbances of consciousness, psychotic symptoms or other serious psychiatric disorders at the time of examination or in the medical data; initiation of psychiatric treatment during the research project; contraindications for VR therapy (epilepsy, vertigo, eyesight impairment) | A VR TierOne device (Stolgraf®, Stanowice, Poland) as the VR source. A head-mounted display with total immersion created an intensely visual, auditory, and kinesthetic stimulation | Perception of Stress Questionnaire (PSQ), Depression and Anxiety Depression Scale (DASS), Evaluation of Functional Capacity (EFC) | The changes in stress levels and depressive and anxiety symptoms was the primary outcome. As a secondary outcome, we evaluated functional capacity. | Immersive VR therapy and the control group performed 10 sessions of Schultz autogenic training | Effect size between control and experimental group using Shapiro–Wilk test, the Mann–Whitney U test and repeated-measures analysis of variance (ANOVA) [68] | ↑ |
| Berry 2019 [65] | Qualitative study (interviews) | United Kingdom | People with severe mental health problems focus on two domains: (1) views about Digital Health Interventions (DHIs) for severe mental health problems, and (2) ideas for future DHI content and design features. |
| Recruitment stopped when data sufficiency was reached; that is, based on analysis of transcripts and discussion amongst the research team, it was agreed that no additional themes were generated from the data | Digital health interventions (DHIs) | Thematic analysisbased on the role of VR intervention |
| Nil | Data were analyzed thematically | ↑ |
| Kolbe 2021 [64] | Cross-sectional | USA | CRU (COCID-19 Rehabilitation Unit) |
| N/A | VR with maximum use time by AppliedVR is 30 min | Simple 1–10 yes/no rating scale (10 indicates the highest satisfaction and highest recommendation) | Satisfaction (“Feeling of enjoyment and get connected with what they see”) Perceived enhancement (“excellent escape and immersive experience”) | Patients and staff | 13/13 patients answered “yes” to recommending the therapy to others, and 12/13 answered “yes” to the perceived enhancement of their treatment. 11/11 staff answered “yes” to recommend the therapy to others, and 11/11 answered “yes” to perceived enhancement of their well-being | ↑ |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hatta, M.H.; Sidi, H.; Sharip, S.; Das, S.; Saini, S.M. The Role of Virtual Reality as a Psychological Intervention for Mental Health Disturbances during the COVID-19 Pandemic: A Narrative Review. Int. J. Environ. Res. Public Health 2022, 19, 2390. https://doi.org/10.3390/ijerph19042390
Hatta MH, Sidi H, Sharip S, Das S, Saini SM. The Role of Virtual Reality as a Psychological Intervention for Mental Health Disturbances during the COVID-19 Pandemic: A Narrative Review. International Journal of Environmental Research and Public Health. 2022; 19(4):2390. https://doi.org/10.3390/ijerph19042390
Chicago/Turabian StyleHatta, Muhammad Hizri, Hatta Sidi, Shalisah Sharip, Srijit Das, and Suriati Mohamed Saini. 2022. "The Role of Virtual Reality as a Psychological Intervention for Mental Health Disturbances during the COVID-19 Pandemic: A Narrative Review" International Journal of Environmental Research and Public Health 19, no. 4: 2390. https://doi.org/10.3390/ijerph19042390