
The Effects of Mind–Body Exercises on Chronic Spinal Pain Outcomes: A Synthesis Based on 72 Meta-Analyses

Abstract
:1. Introduction
2. Materials and Methods
2.1. Deviations from the Protocol
2.2. Data Sources and Search Strategy
2.3. Eligibility Criteria
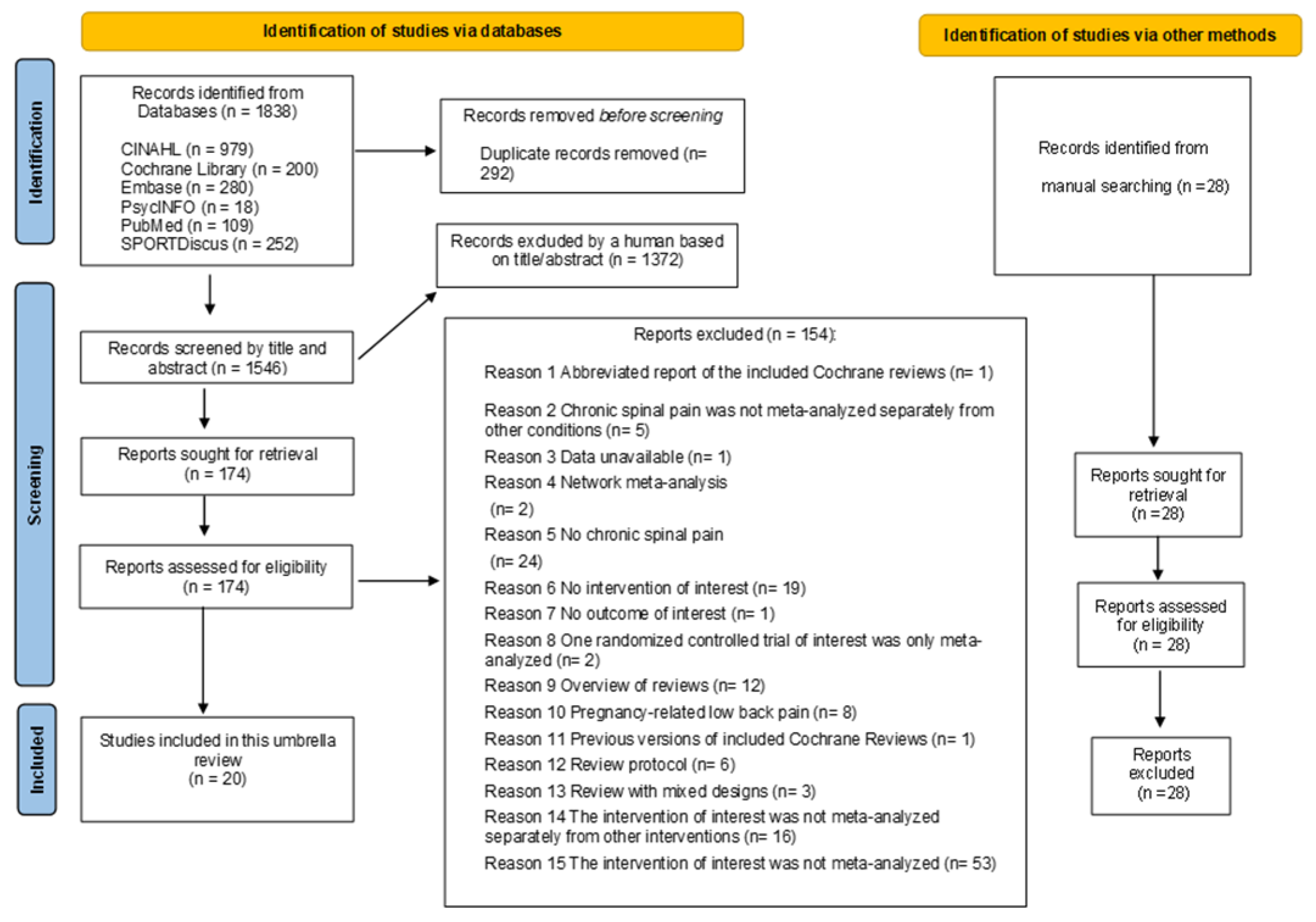
2.4. Study Selection
2.5. Methodological Quality
2.6. Data Extraction and Synthesis
2.7. Overlapping between Reviews
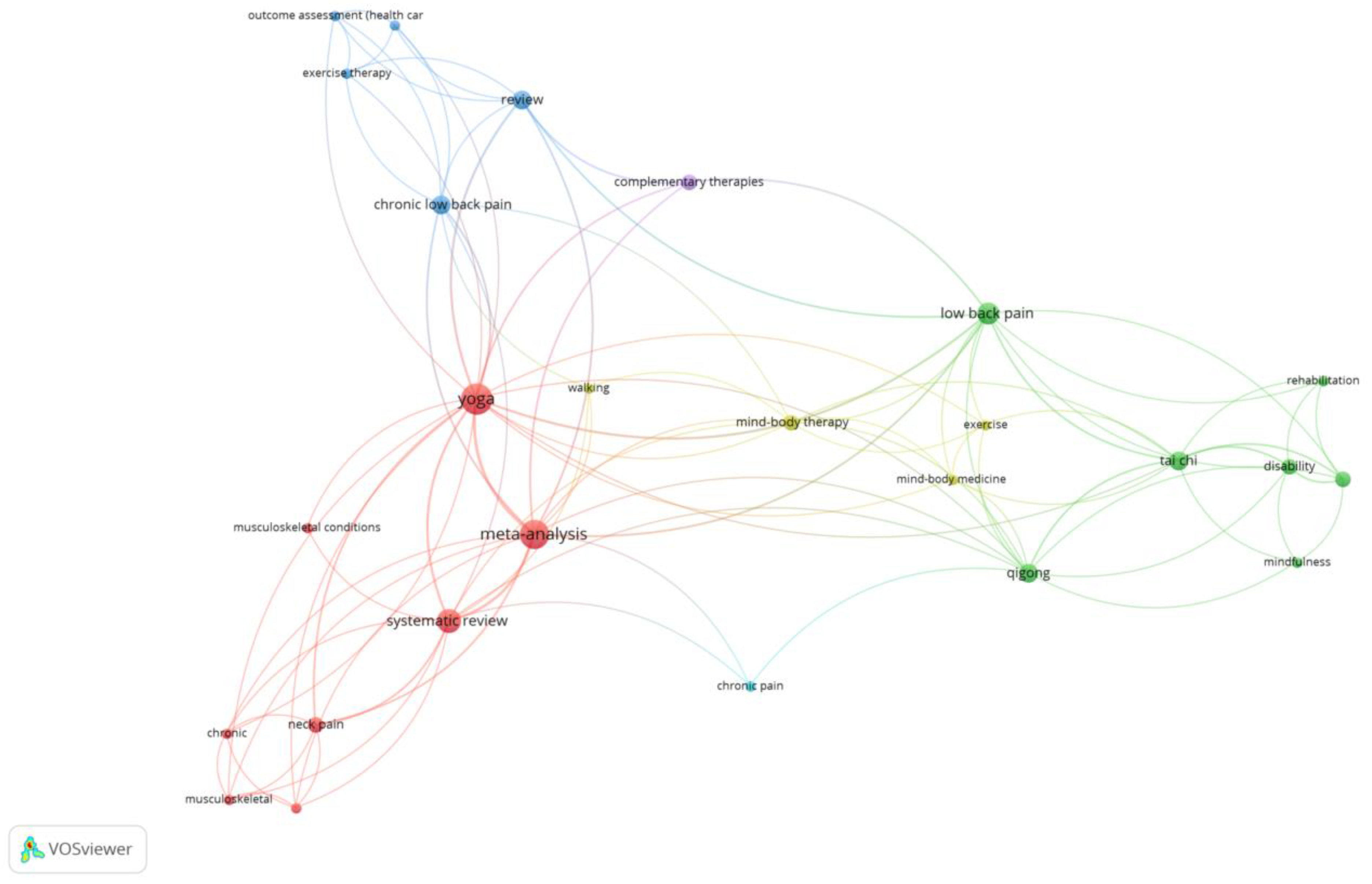
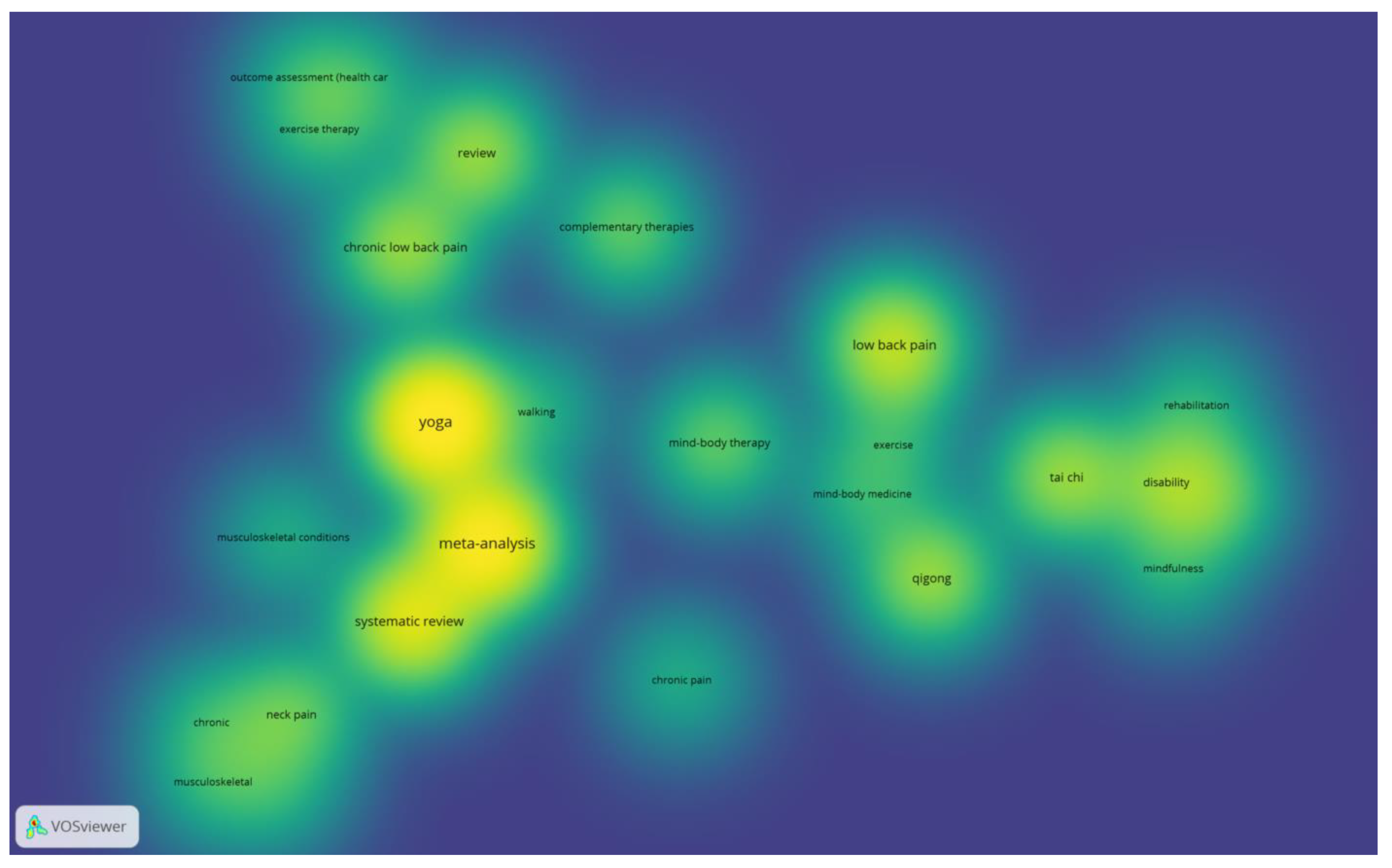
2.8. Co-Occurrence Analysis
3. Results
3.1. Co-Occurrence Analysis
3.2. Overlapping
3.3. AMSTAR 2 Rating
3.4. Qigong for Chronic Spinal Pain
3.4.1. Qigong and Chronic Low Back Pain
3.4.2. Qigong and Chronic Neck Pain
3.5. Tai Chi for Chronic Spinal Pain
Tai Chi and Chronic Low Back Pain
3.6. Yoga for Chronic Spinal Pain
3.6.1. Yoga and Chronic Low Back Pain
3.6.2. Yoga and Chronic Neck Pain
4. Discussion
4.1. Clinical Implications
4.2. Methodological Considerations
4.3. Future Agenda
4.4. Limitations
5. Conclusions
- The effect of qigong on chronic back and neck pain was often inconsistent.
- Qigong seemed to be effective in improving the physical component of quality of life only 12 weeks after the intervention.
- Tai chi could be an interesting approach to reduce chronic low back pain.
- No meta-analyses satisfied our criteria regarding tai chi and outcomes of interest in chronic neck pain.
- Yoga could improve chronic low back pain.
- A lack of relevant effects was found for yoga in reducing depression and improving overall quality of life in chronic low back pain.
- The effects of yoga on both components of quality of life (mental and physical) were inconsistent in chronic low back pain.
- Yoga could be an effective approach to decreasing anxiety, depression, and overall mood states and improving overall quality of life in chronic neck pain.
- Inconsistencies were found that were associated with the effects of yoga on chronic neck pain.
- More well-designed research is required on our covered topic to solve the clinical and methodological concerns that were discussed in this umbrella review.
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Herman, P.M.; Broten, N.; Lavelle, T.A.; Sorbero, M.E.; Coulter, I.D. Health Care Costs and Opioid Use Associated With High-impact Chronic Spinal Pain in the United States. Spine 2019, 44, 1154–1161. [Google Scholar] [CrossRef]
- Gureje, O.; Akinpelu, A.O.; Uwakwe, R.; Udofia, O.; Wakil, A.; Wakil, M. Comorbidity and Impact of Chronic Spinal Pain in Nigeria. Spine 2007, 32, E495–E500. [Google Scholar] [CrossRef]
- Von Korff, M.; Crane, P.; Lane, M.; Miglioretti, D.L.; Simon, G.; Saunders, K.; Stang, P.; Brandenburg, N.; Kessler, R. Chronic spinal pain and physical–mental comorbidity in the United States: Results from the national comorbidity survey replication. Pain 2005, 113, 331–339. [Google Scholar] [CrossRef]
- Depintor, J.D.P.; Bracher, E.S.B.; Cabral, D.M.C.; Eluf-Neto, J. Prevalence of chronic spinal pain and identification of associated factors in a sample of the population of São Paulo, Brazil: Cross-sectional study. Sao Paulo Med. J. 2016, 134, 375–384. [Google Scholar] [CrossRef]
- Vos, T.; Flaxman, A.D.; Naghavi, M.; Lozano, R.; Michaud, C.; Ezzati, M.; Shibuya, K.; Salomon, J.A.; Abdalla, S.; Aboyans, V.; et al. Years lived with disability (YLDs) for 1160 sequelae of 289 diseases and injuries 1990–2010: A systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012, 380, 2163–2196. [Google Scholar] [CrossRef]
- Johnson, C.D.; Haldeman, S.; Chou, R.; Nordin, M.; Green, B.N.; Côté, P.; Hurwitz, E.L.; Kopansky-Giles, D.; Acaroğlu, E.; Cedraschi, C.; et al. The Global Spine Care Initiative: Model of care and implementation. Eur. Spine J. 2018, 27, 925–945. [Google Scholar] [CrossRef]
- Lall, M.P.; Restrepo, E. The Biopsychosocial Model of Low Back Pain and Patient-Centered Outcomes Following Lumbar Fusion. Orthop. Nurs. 2017, 36, 213–221. [Google Scholar] [CrossRef]
- Jull, G.; Sterling, M. Bring back the biopsychosocial model for neck pain disorders. Man. Ther. 2009, 14, 117–118. [Google Scholar] [CrossRef]
- Martinez-Calderon, J.; Matias-Soto, M.J.; Luque-Suarez, A. “My Pain Is Unbearable…I Cannot Recognize Myself!” Emotions, Cognitions, and Behaviors of People Living With Musculoskeletal Disorders: An Umbrella Review. J. Orthop. Sports Phys. Ther. 2022, 52, 233–302. [Google Scholar] [CrossRef]
- Boutevillain, L.; Dupeyron, A.; Rouch, C.; Richard, E.; Coudeyre, E. Facilitators and barriers to physical activity in people with chronic low back pain: A qualitative study. PLoS ONE 2017, 12, e0179826. [Google Scholar] [CrossRef] [Green Version]
- Geneen, L.J.; Moore, R.A.; Clarke, C.; Martin, D.; Colvin, L.A.; Smith, B.H. Physical activity and exercise for chronic pain in adults: An overview of Cochrane Reviews. Cochrane Database Syst. Rev. 2017, 4, CD011279. [Google Scholar] [CrossRef]
- Sivaramakrishnan, D.; Fitzsimons, C.; Kelly, P.; Ludwig, K.; Mutrie, N.; Saunders, D.H.; Baker, G. The effects of yoga compared to active and inactive controls on physical function and health related quality of life in older adults-systematic review and meta-analysis of randomised controlled trials. Int. J. Behav. Nutr. Phys. Act. 2019, 16, 33. [Google Scholar] [CrossRef]
- Zou, L.; Zhang, Y.; Yang, L.; Loprinzi, P.D.; Yeung, A.S.; Kong, J.; Chen, K.W.; Song, W.; Xiao, T.; Li, H. Are Mindful Exercises Safe and Beneficial for Treating Chronic Lower Back Pain? A Systematic Review and Meta-Analysis of Randomized Controlled Trials. J. Clin. Med. 2019, 8, 628. [Google Scholar] [CrossRef]
- So, W.W.Y.; Lu, E.Y.; Cheung, W.M.; Tsang, H.W.H. Comparing Mindful and Non-Mindful Exercises on Alleviating Anxiety Symptoms: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2020, 17, 8692. [Google Scholar] [CrossRef]
- Li, J.; Shen, J.; Wu, G.; Tan, Y.; Sun, Y.; Keller, E.; Jiang, Y.; Wu, J. Mindful Exercise versus Non-Mindful Exercise for Schizo-phrenia: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Complement. Ther. Clin. Pract. 2018, 32, 17–24. [Google Scholar] [CrossRef]
- Sullivan, M.B.; Erb, M.; Schmalzl, L.; Moonaz, S.; Taylor, J.N.; Porges, S.W. Yoga Therapy and Polyvagal Theory: The Convergence of Traditional Wisdom and Contemporary Neuroscience for Self-Regulation and Resilience. Front. Hum. Neurosci. 2018, 12, 67. [Google Scholar] [CrossRef]
- Csala, B.; Springinsfeld, C.M.; Köteles, F. The Relationship Between Yoga and Spirituality: A Systematic Review of Empiri-cal Research. Front. Psychol. 2021, 12, 3052. [Google Scholar] [CrossRef]
- Chang, P.-S.; Lu, Y.; Nguyen, C.M.; Suh, Y.; Luciani, M.; Ofner, S.; Powell, S. Effects of Qigong Exercise on Physical and Psychological Health among African Americans. West. J. Nurs. Res. 2021, 43, 551–562. [Google Scholar] [CrossRef]
- Robins, J.L.; Elswick, R.K.J.; Sturgill, J.; McCain, N.L. The Effects of Tai Chi on Cardiovascular Risk in Women. Am. J. Health Promot. 2016, 30, 613–622. [Google Scholar] [CrossRef]
- Zhang, M.; Xv, G.; Luo, C.; Meng, D.; Ji, Y. Qigong Yi Jinjing Promotes Pulmonary Function, Physical Activity, Quality of Life and Emotion Regulation Self-Efficacy in Patients with Chronic Obstructive Pulmonary Disease: A Pilot Study. J. Altern. Complement. Med. 2016, 22, 810–817. [Google Scholar] [CrossRef]
- Murley, B.; Haas, B.; Hermanns, M.; Wang, Y.T.; Stocks, E. Influence of Tai Chi on Self-Efficacy, Quality of Life, and Fatigue Among Patients With Cancer Receiving Chemotherapy: A Pilot Study Brief. J. Holist. Nurs. 2019, 37, 354–363. [Google Scholar] [CrossRef]
- Easwaran, K.; Gopalasingam, Y.; Green, D.D.; Lach, V.; Melnyk, J.A.; Wan, C.; Bartlett, D.J. Effectiveness of Tai Chi for health promotion for adults with health conditions: A scoping review of Meta-analyses. Disabil. Rehabil. 2021, 43, 2978–2989. [Google Scholar] [CrossRef]
- Ernst, E.; Lee, M.S. How effective is yoga? A concise overview of systematic reviews. Focus Altern. Complement. Ther. 2010, 15, 274–279. [Google Scholar] [CrossRef]
- Goode, A.P.; Coeytaux, R.R.; McDuffie, J.; Duan-Porter, W.; Sharma, P.; Mennella, H.; Nagi, A.; Williams, J.W., Jr. An evidence map of yoga for low back pain. Complement. Ther. Med. 2016, 25, 170–177. [Google Scholar] [CrossRef]
- Kelley, G.A.; Kelley, K.S. Meditative Movement Therapies and Health-Related Quality-of-Life in Adults: A Systematic Review of Meta-Analyses. PLoS ONE 2015, 10, e0129181. [Google Scholar] [CrossRef]
- Wieland, L.S.; Cramer, H.; Lauche, R.; Verstappen, A.; Parker, E.A.; Pilkington, K. Evidence on yoga for health: A bibliometric analysis of systematic reviews. Complement. Ther. Med. 2021, 60, 102746. [Google Scholar] [CrossRef]
- Lorenc, A.; Feder, G.; MacPherson, H.; Little, P.; Mercer, S.; Sharp, D. Scoping review of systematic reviews of complementary medicine for musculoskeletal and mental health conditions. BMJ Open 2018, 8, e020222. [Google Scholar] [CrossRef]
- Skelly, A.C.; Chou, R.; Dettori, J.R.; Turner, J.A.; Friedly, J.L.; Rundell, S.D.; Fu, R.; Brodt, E.D.; Wasson, N.; Kantner, S.; et al. Noninvasive Nonpharmacological Treatment for Chronic Pain: A Systematic Review Update; Report No.: 20-EHC009; Agency for Healthcare Research and Quality: Rockville, MD, USA, 2020.
- Bai, Z.; Guan, Z.; Fan, Y.; Liu, C.; Yang, K.; Ma, B.; Wu, B. The Effects of Qigong for Adults with Chronic Pain: Systematic Review and Meta-Analysis. Am. J. Chin. Med. 2015, 43, 1525–1539. [Google Scholar] [CrossRef]
- Gross, A.R.; Kay, T.M.; Paquin, J.-P.; Blanchette, S.; LaLonde, P.; Christie, T.; Dupont, G.; Graham, N.; Burnie, S.J.; Gelley, G.; et al. Exercises for mechanical neck disorders. Cochrane Database Syst. Rev. 2015, 1, CD004250. [Google Scholar] [CrossRef]
- Nduwimana, I.; Nindorera, F.; Thonnard, J.L.; Kossi, O. Effectiveness of walking versus mind-body therapies in chronic low back pain: A Systematic Review and Meta-Analysis of Recent Randomized Controlled Trials. Medicine 2020, 99, e21969. [Google Scholar] [CrossRef]
- Zhang, Y.; Loprinzi, P.D.; Yang, L.; Liu, J.; Liu, S.; Zou, L. The Beneficial Effects of Traditional Chinese Exercises for Adults with Low Back Pain: A Meta-Analysis of Randomized Controlled Trials. Medicina 2019, 55, 118. [Google Scholar] [CrossRef]
- Qin, J.; Zhang, Y.; Wu, L.; He, Z.; Huang, J.; Tao, J.; Chen, L. Effect of Tai Chi alone or as additional therapy on low back pain: Systematic Review and Meta-Analysis of Randomized Controlled Trials. Medicine 2019, 98, e17099. [Google Scholar] [CrossRef]
- Anheyer, D.; Haller, H.; Lauche, R.; Dobos, G.; Cramer, H. Yoga for treating low back pain: A systematic review and meta-analysis. Pain 2021, 163, e504–e517. [Google Scholar] [CrossRef]
- Kim, S.-D. Twelve Weeks of Yoga for Chronic Nonspecific Lower Back Pain: A Meta-Analysis. Pain Manag. Nurs. 2020, 21, 536–542. [Google Scholar] [CrossRef]
- Slade, S.C.; Keating, J.L. Unloaded Movement Facilitation Exercise Compared to No Exercise or Alternative Therapy on Outcomes for People with Nonspecific Chronic Low Back Pain: A Systematic Review. J. Manip. Physiol. Ther. 2007, 30, 301–311. [Google Scholar] [CrossRef]
- Zhu, F.; Zhang, M.; Wang, D.; Hong, Q.; Zeng, C.; Chen, W. Yoga compared to non-exercise or physical therapy exercise on pain, disability, and quality of life for patients with chronic low back pain: A systematic review and meta-analysis of randomized controlled trials. PLoS ONE 2020, 15, e0238544. [Google Scholar] [CrossRef]
- Bougioukas, K.I.; Liakos, A.; Tsapas, A.; Ntzani, E.; Haidich, A.-B. Preferred reporting items for overviews of systematic reviews including harms checklist: A pilot tool to be used for balanced reporting of benefits and harms. J. Clin. Epidemiol. 2018, 93, 9–24. [Google Scholar] [CrossRef]
- Andrews, J.; Guyatt, G.; Oxman, A.D.; Alderson, P.; Dahm, P.; Falck-Ytter, Y.; Nasser, M.; Meerpohl, J.; Post, P.N.; Kunz, R.; et al. GRADE guidelines: 14. Going from evidence to recommendations: The significance and presentation of recommendations. J. Clin. Epidemiol. 2013, 66, 719–725. [Google Scholar] [CrossRef]
- Richardson, W.S.; Wilson, M.C.; Nishikawa, J.; Hayward, R.S. The well-built clinical question: A key to evidence-based decisions. ACP J. Club 1995, 123, A12–A13. [Google Scholar] [CrossRef]
- Kwon, Y.; Lemieux, M.; McTavish, J.; Wathen, N. Identifying and removing duplicate records from systematic review searches. J. Med. Libr. Assoc. 2015, 103, 184–188. [Google Scholar] [CrossRef] [Green Version]
- Shea, B.J.; Reeves, B.C.; Wells, G.; Thuku, M.; Hamel, C.; Moran, J.; Moher, D.; Tugwell, P.; Welch, V.; Kristjansson, E.; et al. AMSTAR 2: A critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ 2017, 358, j4008. [Google Scholar] [CrossRef]
- Pieper, D.; Antoine, S.-L.; Mathes, T.; Neugebauer, E.A.; Eikermann, M. Systematic review finds overlapping reviews were not mentioned in every other overview. J. Clin. Epidemiol. 2014, 67, 368–375. [Google Scholar] [CrossRef]
- Kong, L.; Lauche, R.; Klose, P.; Bu, J.H.; Yang, X.C.; Guo, C.Q.; Dobos, G.; Cheng, Y.W. Tai Chi for Chronic Pain Conditions: A Systematic Review and Meta-analysis of Randomized Controlled Trials. Sci. Rep. 2016, 6, 25325. [Google Scholar] [CrossRef]
- Holtzman, S.; Beggs, R.T. Yoga for Chronic Low Back Pain: A Meta-Analysis of Randomized Controlled Trials. Pain Res. Manag. 2013, 18, 267–272. [Google Scholar] [CrossRef]
- Li, Y.; Li, S.; Jiang, J.; Yuan, S. Effects of yoga on patients with chronic nonspecific neck pain: A PRISMA Sys-tematic Review and Meta-Analysis. Medicine 2019, 98, e14649. [Google Scholar] [CrossRef]
- Ward, L.; Stebbings, S.; Cherkin, D.; Baxter, D. Yoga for Functional Ability, Pain and Psychosocial Outcomes in Musculoskeletal Conditions: A Systematic Review and Meta-Analysis. Musculoskelet. Care 2013, 11, 203–217. [Google Scholar] [CrossRef]
- Wieland, L.S.; Skoetz, N.; Pilkington, K.; Vempati, R.; D’Adamo, C.R.; Berman, B.M. Yoga treatment for chronic non-specific low back pain. Cochrane Database Syst. Rev. 2017, 1, CD010671. [Google Scholar] [CrossRef]
- Yuan, Q.-L.; Guo, T.-M.; Liu, L.; Sun, F.; Zhang, Y.-G. Traditional Chinese Medicine for Neck Pain and Low Back Pain: A Systematic Review and Meta-Analysis. PLoS ONE 2015, 10, e0117146. [Google Scholar] [CrossRef]
- Hall, A.; Copsey, B.; Richmond, H.; Thompson, J.; Ferreira, M.; Latimer, J.; Maher, C. Effectiveness of Tai Chi for Chronic Musculoskeletal Pain Conditions: Updated Systematic Review and Meta-Analysis. Phys. Ther. 2016, 97, 227–238. [Google Scholar] [CrossRef]
- Cramer, H.; Lauche, R.; Haller, H.; Dobos, G. A Systematic Review and Meta-analysis of Yoga for Low Back Pain. Clin. J. Pain 2013, 29, 450–460. [Google Scholar] [CrossRef]
- Cramer, H.; Klose, P.; Brinkhaus, B.; Michalsen, A.; Dobos, G. Effects of yoga on chronic neck pain: A systematic review and meta-analysis. Clin. Rehabil. 2017, 31, 1457–1465. [Google Scholar] [CrossRef]
- Maher, C.G.; Sherrington, C.; Herbert, R.D.; Moseley, A.M.; Elkins, M. Reliability of the PEDro Scale for Rating Quality of Randomized Controlled Trials. Phys. Ther. 2003, 83, 713–721. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Altman, D.G.; Gotzsche, P.; Jüni, P.; Moher, D.; Oxman, A.D.; Savović, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.; et al. The Cochrane Collaboration’s Tool for Assessing Risk of Bias in Randomsed Trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef]
- Tao, J.; Chen, X.; Liu, J.; Egorova, N.; Xue, X.; Liu, W.; Zheng, G.; Li, M.; Wu, J.; Hu, K.; et al. Tai Chi Chuan and Baduanjin Mind-Body Training Changes Resting-State Low-Frequency Fluctuations in the Frontal Lobe of Older Adults: A Resting-State fMRI Study. Front. Hum. Neurosci. 2017, 11, 514. [Google Scholar] [CrossRef]
- Xia, R.; Qiu, P.; Lin, H.; Ye, B.; Wan, M.; Li, M.; Tao, J.; Chen, L.; Zheng, G. The Effect of Traditional Chinese Mind-Body Exercise (Baduanjin) and Brisk Walking on the Dorsal Attention Network in Older Adults With Mild Cognitive Impairment. Front. Psychol. 2019, 10, 2075. [Google Scholar] [CrossRef]
- Xiong, X.; Wang, P.; Li, S.; Zhang, Y.; Li, X. Effect of Baduanjin exercise for hypertension: A systematic review and meta-analysis of randomized controlled trials. Maturitas 2015, 80, 370–378. [Google Scholar] [CrossRef]
- Zou, L.; Sasaki, J.; Wang, H.; Xiao, Z.; Fang, Q.; Zhang, M. A Systematic Review and Meta-Analysis of Baduanjin Qigong for Health Benefits: Randomized Controlled Trials. Evidence-Based Complement. Altern. Med. 2017, 2017, 4548706. [Google Scholar] [CrossRef]
- George, S.Z.; Fritz, J.M.; Silfies, S.P.; Schneider, M.J.; Beneciuk, J.M.; Lentz, T.A.; Gilliam, J.R.; Hendren, S.; Norman, K.S. Interventions for the Management of Acute and Chronic Low Back Pain: Revision 2021. J. Orthop. Sports Phys. Ther. 2021, 51, CPG1–CPG60. [Google Scholar] [CrossRef]
- Corp, N.; Mansell, G.; Stynes, S.; Wynne-Jones, G.; Morsø, L.; Hill, J.C.; van der Windt, D.A. Evidence-based treatment recommendations for neck and low back pain across Europe: A systematic review of guidelines. Eur. J. Pain 2020, 25, 275–295. [Google Scholar] [CrossRef]
- Cramer, H.; Lauche, R.; Anheyer, D.; Pilkington, K.; de Manincor, M.; Dobos, G.; Ward, L. Yoga for anxiety: A systematic review and meta-analysis of randomized controlled trials. Depress. Anxiety 2018, 35, 830–843. [Google Scholar] [CrossRef]
- Cramer, H.; Lauche, R.; Langhorst, J.; Dobos, G. Yoga for Depression: A Systematic Review and Meta-analysis. Depress. Anxiety 2013, 30, 1068–1083. [Google Scholar] [CrossRef]
- Cramer, H.; Lauche, R.; Azizi, H.; Dobos, G.; Langhorst, J. Yoga for Multiple Sclerosis: A Systematic Review and Meta-Analysis. PLoS ONE 2014, 9, e112414. [Google Scholar] [CrossRef]
- Lauche, R.; Hunter, D.J.; Adams, J.; Cramer, H. Yoga for Osteoarthritis: A Systematic Review and Meta-analysis. Curr. Rheumatol. Rep. 2019, 21, 47. [Google Scholar] [CrossRef]
- O’Neill, M.; Samaroo, D.; Lopez, C.; Tomlinson, G.; Mina, D.S.; Sabiston, C.; Culos-Reed, N.; Alibhai, S.M.H. The Effect of Yoga Interventions on Cancer-Related Fatigue and Quality of Life for Women with Breast Cancer: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Integr. Cancer Ther. 2020, 19, 1–10. [Google Scholar] [CrossRef]
- Cramer, H.; Lauche, R.; Langhorst, J.; Dobos, G. Is one yoga style better than another? A systematic review of associations of yoga style and conclusions in randomized yoga trials. Complement. Ther. Med. 2016, 25, 178–187. [Google Scholar] [CrossRef]
- Cramer, H.; Lauche, R.; Dobos, G. Characteristics of randomized controlled trials of yoga: A bibliometric analysis. BMC Complement. Altern. Med. 2014, 14, 328. [Google Scholar] [CrossRef]
- Bonura, K.B.; Tenenbaum, G. Effects of Yoga on Psychological Health in Older Adults. J. Phys. Act. Health 2014, 11, 1334–1341. [Google Scholar] [CrossRef]
- Uluğ, N.; Yılmaz, Ö.T.; Kara, M.; Özçakar, L. Effects of Pilates and yoga in patients with chronic neck pain: A sonographic study. J. Rehabil. Med. 2018, 50, 80–85. [Google Scholar] [CrossRef]
- Yogitha, B.; Nagarathna, R.; John, E.; Nagendra, H. Complimentary effect of yogic sound resonance relaxation technique in patients with common neck pain. Int. J. Yoga 2010, 3, 18–25. [Google Scholar] [CrossRef]
- Phattharasupharerk, S.; Purepong, N.; Eksakulkla, S.; Siriphorn, A. Effects of Qigong practice in office workers with chronic non-specific low back pain: A randomized control trial. J. Bodyw. Mov. Ther. 2019, 23, 375–381. [Google Scholar] [CrossRef]
- Kuvačić, G.; Fratini, P.; Padulo, J.; Antonio, D.I.; De Giorgio, A. Effectiveness of yoga and educational intervention on disability, anxiety, depression, and pain in people with CLBP: A randomized controlled trial. Complement. Ther. Clin. Pract. 2018, 31, 262–267. [Google Scholar] [CrossRef]
- Cox, H.; Tilbrook, H.; Aplin, J.; Semlyen, A.; Torgerson, D.; Trewhela, A.; Watt, I. A randomised controlled trial of yoga for the treatment of chronic low back pain: Results of a pilot study. Complement. Ther. Clin. Pract. 2010, 16, 187–193. [Google Scholar] [CrossRef]
- Hoffmann, T.C.; Glasziou, P.P.; Boutron, I.; Milne, R.; Perera, R.; Moher, D.; Altman, D.G.; Barbour, V.; Macdonald, H.; Johnston, M.; et al. Better reporting of interventions: Template for intervention description and replication (TIDieR) checklist and guide. BMJ 2014, 348, g1687. [Google Scholar] [CrossRef]
- Dipietro, L.; Campbell, W.W.; Buchner, D.M.; Erickson, K.I.; Powell, K.E.; Bloodgood, B.; Hughes, T.; Day, K.R.; Piercy, K.L.; Vaux-Bjerke, A.; et al. Physical Activity, Injurious Falls, and Physical Function in Aging: An Umbrella Review. Med. Sci. Sports Exerc. 2019, 51, 1303–1313. [Google Scholar] [CrossRef]
- Cuenca-Martínez, F.; Calatayud, J.; Suso-Martí, L.; Varangot-Reille, C.; Herranz-Gómez, A.; Blanco-Díaz, M.; Casaña, J. Behavior Modification Techniques on Patients with Chronic Pain in the Context of COVID-19 Telerehabilitation: An Umbrella Review. Int. J. Environ. Res. Public Health 2022, 19, 5260. [Google Scholar] [CrossRef]
- Torres, A.; Tennant, B.; Ribeiro-Lucas, I.; Vaux-Bjerke, A.; Piercy, K.; Bloodgood, B. Umbrella and Systematic Review Methodology to Support the 2018 Physical Activity Guidelines Advisory Committee. J. Phys. Act. Health 2018, 15, 805–810. [Google Scholar] [CrossRef]
- Cuenca-Martínez, F.; La Touche, R.; Varangot-Reille, C.; Sardinoux, M.; Bahier, J.; Suso-Martí, L.; Fernández-Carnero, J. Effects of Neural Mobilization on Pain Intensity, Disability, and Mechanosensitivity: An Umbrella Review With Meta–Meta-Analysis. Phys. Ther. 2022, 102, 1–8. [Google Scholar] [CrossRef]
- Martinez-Calderon, J.; Flores-Cortes, M.; Morales-Asencio, J.M.; Luque-Suarez, A. Pain-Related Fear, Pain Intensity and Function in Individuals With Chronic Musculoskeletal Pain: A Systematic Review and Meta-Analysis. J. Pain 2019, 20, 1394–1415. [Google Scholar] [CrossRef]
- Martinez-Calderon, J.; Jensen, M.P.; Morales-Asencio, J.M.; Luque-Suarez, A. Pain Catastrophizing and Function In Individuals With Chronic Musculoskeletal Pain: A Systematic Review and Meta-Analysis. Clin. J. Pain 2019, 35, 279–293. [Google Scholar] [CrossRef]
- Whiting, P.; Savović, J.; Higgins, J.P.T.; Caldwell, D.M.; Reeves, B.C.; Shea, B.; Davies, P.; Kleijnen, J.; Churchill, R.; ROBIS Group. ROBIS: A new tool to assess risk of bias in systematic reviews was developed. J. Clin. Epidemiol. 2016, 69, 225–234. [Google Scholar] [CrossRef] [Green Version]
- Swierz, M.J.; Storman, D.; Zajac, J.; Koperny, M.; Weglarz, P.; Staskiewicz, W.; Gorecka, M.; Skuza, A.; Wach, A.; Kaluzinska, K.; et al. Similarities, reliability and gaps in assessing the quality of conduct of systematic reviews using AMSTAR-2 and ROBIS: Systematic survey of nutrition reviews. BMC Med. Res. Methodol. 2021, 21, 261. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Author(s) | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 | 16 | Overall Score |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Anheyer et al., 2021 [34] | CLQR | ||||||||||||||||
| Bai et al., 2015 [29] | CLQR | ||||||||||||||||
| Cramer et al., 2013 [51] | CLQR | ||||||||||||||||
| Cramer et al., 2017 [52] | CLQR | ||||||||||||||||
| Gross et al., 2015 [30] | LQR | ||||||||||||||||
| Hall et al., 2017 [50] | CLOR | ||||||||||||||||
| Holtzman et al., 2013 [45] | CLQR | ||||||||||||||||
| Kim 2020 [35] | CLQR | ||||||||||||||||
| Kong et al., 2016 [44] | LQR | ||||||||||||||||
| Li et al., 2019 [46] | CLQR | ||||||||||||||||
| Nduwimana et al., 2020 [31] | CLQR | ||||||||||||||||
| Qin et al., 2019 [33] | LQR | ||||||||||||||||
| Skelly et al., 2020 [28] | LQR | ||||||||||||||||
| Slade et al., 2007 [36] | CLQR | ||||||||||||||||
| Ward et al., 2013 [47] | CLQR | ||||||||||||||||
| Wieland et al., 2017 [48] | LQR | ||||||||||||||||
| Yuan et al., 2015 [49] | CLQR | ||||||||||||||||
| Zhang et al., 2019 [32] | CLQR | ||||||||||||||||
| Zhu et al., 2020 [37] | LQR | ||||||||||||||||
| Zou et al., 2019 [13] | CLQR |
| Study and Year | Quality Assessment | RCTs Included in This Umbrella | Participants | Interventions | Outcome Measurements | Effect Sizes |
|---|---|---|---|---|---|---|
| CHRONIC LOW BACK PAIN | ||||||
| Nduwimana et al., 2020 [31] | GRADE Unavailable Tool for quality assessment The PEDro scale | 3 | 375 with chronic low back pain | EXPERIMENTAL Qigong CONTROL Exercise, or no intervention, or waitlist | Short-term (ST) effects: 0–3 months after the intervention Intermediate-term (IT) effects: 3–6 months postintervention | SMD (95% CI): subgroup analysis according to the type of intervention and the outcome measurement time points 1. Pain—qigong vs. exercise, no intervention, and waitlist: a. ST effect: −1.34 (−3.19 to 0.51), p = 0.16; I2 = 98% b. IT effect: 0.12 (−2.67 to 2.91), p = 0.93; I2 = 99% |
| Zhang et al., 2019 [32] | GRADE Unavailable Tool for quality assessment The PEDro scale | 3 | 375 with chronic low back pain | EXPERIMENTAL Qigong CONTROL Exercise or waitlist | Unspecified | Hedge’s g (95% CI): subgroup analysis for the type of experimental group 1. Pain—qigong vs. exercise and waitlist: −0.54 (−0.86 to −0.23), p < 0.001; I2 = 75.9% |
| Zou et al., 2019 [13] | GRADE Unavailable Tool for quality assessment The PEDro scale | 2 | 303 with chronic low back pain | EXPERIMENTAL Qigong CONTROL Exercise or waitlist | Authors declared that none of included studies used follow-up assessments | SMD (95% CI): subgroup analysis according to the type of experimental group 1. Pain—qigong vs. exercise and waitlist: −0.21 (−0.48 to 0.06), p = 0.12; I2 = 10.0% |
| CHRONIC NECK PAIN | ||||||
| Bai et al., 2015 [29] | GRADE Unavailable Tool for quality assessment The Cochrane risk of bias tool | 2 | 240 with chronic neck pain | EXPERIMENTAL Internal qigong CONTROL Waitlist | 3-month follow-up 6-month follow-up | SMD (95% CI): subgroup analysis according to clinical condition and the outcome measurement time points 1. Pain—internal qigong vs. waitlist: a. At 3 months: −1.17 (−2.44 to 0.10), p = 0.07; I2 = 93% b. At 6 months: −1.00 (−1.94 to −0.06), p = 0.04; I2 = 87% |
| Gross et al., 2015 [30] | GRADE Available Tool for quality assessment The Cochrane risk of bias tool | 2 | 240 with chronic neck pain | EXPERIMENTAL Internal qigong CONTROL Waitlist | 12 weeks of treatment 24 weeks of treatment | MD (95% CI): subgroup analysis according to the type of intervention and the outcome measurement time points 1. Pain—internal qigong vs. waitlist: a. 12 weeks of treatment: −13.28 (−20.98 to −5.58), p = 0.00073; I2 = 0% b. 24 weeks of treatment: −7.82 (−14.57 to −1.07), p = 0.023; I2 = 0% 2. Quality of life (physical component)—internal qigong vs. waitlist: a. 12 weeks of treatment: −2.72 (−5.42 to −0.01), p = 0.049; I2 = 0% b. 24 weeks of treatment: −1.88 (−5.80 to 2.04), p = 0.35; I2 = 45% |
| Yuan et al., 2015 [49] | GRADE Available Tool for quality assessment The Cochrane risk of bias tool | 2 | 240 with chronic neck pain | EXPERIMENTAL Internal qigong CONTROL Exercise or waitlist | ST: <3 months IT: ~3–12 months | WMD (95% CI): subgroup analysis according to the type of control group and the outcome measurement time points: 1. Pain—internal qigong vs. waitlist; p-value vas not reported: a. ST effect: −15.27 (−22.49 to −8.05); I2 = 47.5% b. IT effect: −10.18 (−16.63 to −3.73); I2 = 0% 2. Pain—internal qigong vs. exercise: a. ST effect: 1.88 (−5.77 to 9.54), p = 0.63; I2 = 0% b. IT effect: 1.00 (−6.21 to 8.21), p = 0.79; I2 = 0% |
| Study and Year | Quality Assessment | RCTs Included in This Umbrella | Participants | Interventions | Outcome Measurements | Effect Sizes |
|---|---|---|---|---|---|---|
| CHRONIC LOW BACK PAIN | ||||||
| Hall et al., 2017 [50] | GRADE Available Tool for quality assessment The Cochrane risk of bias tool | 2 | 349 with chronic low back pain | EXPERIMENTAL Tai chi CONTROL Attention control, no, usual care, or waitlist | Unspecified | SMD (95%): subgroup analysis according to clinical condition 1. Pain—tai chi vs. attention control, usual care, or waitlist: −0.84 (−1.27 to −0.42), p < 0.0001; I2 = 69% |
| Kong et al., 2016 [44] | GRADE Unavailable Tool for quality assessment The PEDro scale | 3 | 385 with chronic low back pain | EXPERIMENTAL Tai chi CONTROL Physical therapy or waitlist plus health care | Immediately after the treatments—up to 1 day | SMD (95%): subgroup analysis according to clinical condition 1. Pain—tai chi vs. physical therapy or waitlist plus health care: −0.81 (−1.11 to −0.52), p < 0.00001; I2 = 46% |
| Nduwimana et al., 2020 [31] | GRADE Unavailable Tool for quality assessment The PEDro scale | 2 | 480 with chronic low back pain | EXPERIMENTAL Tai chi CONTROL Exercise (swimming, jogging), no exercise, usual care, or waitlist | Short-term (ST) effects: 0–3 months after the intervention | SMD (95%CI): subgroup analysis according to the type of experimental group and outcome measurement time points: 1. ST pain—tai chi vs. exercise, no exercise, usual care, and waitlist: −1.19 (−2.97 to 0.58), p = 0.19; I2 = 99% |
| Qin et al., 2019 [33] | GRADE Unavailable Tool for quality assessment The PEDro scale | 3 | 252 with chronic low back pain | EXPERIMENTAL Tai chi CONTROL No intervention or waitlist | Unspecified | MD (95%): subgroup analysis according to the type of control group 1. Pain—tai chi vs. no intervention, usual care, or waitlist −1.71 (−2.31 to −1.11), p < 0.00001; I2 = 82% |
| Zou et al., 2019 [13] | GRADE Unavailable Tool for quality assessment The PEDro scale | 2 | 203 with chronic low back pain | EXPERIMENTAL Tai chi CONTROL Exercise, no intervention, or waitlist | Authors declared that none of included studies used follow-up assessments | SMD (95%): subgroup analysis according to the type of experimental group 1. Pain—tai chi vs. exercise, no intervention, or waitlist: −0.75 (−1.05 to −0.46), p < 0.001; I2 = 0% |
| Study and Year | Quality Assessment | RCTs Included in This Umbrella | Participants | Interventions | Outcome Measurements | Effect Sizes |
|---|---|---|---|---|---|---|
| CHRONIC LOW BACK PAIN | ||||||
| Anheyer et al., 2021 [34] | GRADE Unavailable Tool for quality assessment The Cochrane risk of bias tool | 19 | 2250 with chronic low back pain | EXPERIMENTAL Yoga (Kundalini, Iyengar, Hatha, Vinyasa, therapeutic approach, or integrated approach) with or without usual care CONTROL Exercise, lifestyle advice, multicomponent intervention, usual care, or waitlist | Short-term (ST) effects: postintervention and closest to 12 weeks after randomization Long-term (LT) effects: closest to 6 months after randomization | SMD (95% CI): subgroup analysis according to outcome measurement time points—p value was not reported. 1. Pain—yoga vs. passive control (usual care and/or waitlist) a. LT (6 months and longer): −0.29 (−0.47 to −0.11); I2 = 33% 2. Pain—yoga vs. active control: a. LT (6 months and longer): −0.31 (−1.55 to 0.93); I2 = 91% 3. Quality of life (physical component)—yoga vs. passive control (usual care and/or waitlist): a. ST (2 to 4 months): 0.28 (0.10 to 0.47); I2 = 24% b. LT (6 months and longer): 0.22 (0.03 to 0.41); I2 = 0% 4. Quality of life (physical component)—yoga vs. active control: a. ST (2 to 4 months): 0.51 (−0.03 to 1.05); I2 = 88% b. LT (6 months and longer): 0.31 (−1.95 to 2.56); I2 = 93% 5. Quality of life (mental component)—yoga vs. passive control (usual care and/or waitlist): a. ST (2 to 4 months): 0.17 (0.02 to 0.32); I2 = 0% b. LT (6 months and longer): 0.13 (−0.23 to 0.48); I2 = 39% 6. Quality of life (mental component)—yoga vs. active control: a. ST (2 to 4 months): 0.57 (−0.25 to 1.40); I2 = 92% b. LT (6 months and longer): 0.64 (−7.81 to 9.10); I2 = 93% |
| Cramer et al., 2013 [51] | GRADE Unavailable Tool for quality assessment The Cochrane risk of bias tool | 8 | 832 with chronic low back pain | EXPERIMENTAL Yoga (Iyengar, Hatha, Viniyoga), with or without education, usual care, or vegetarian diet CONTROL Education, exercise, multicomponent intervention, usual care, or waitlist | ST: after the end of the intervention and closest to 12 weeks after randomization LT: closest to 12 months after randomization | SMD (95% CI): subgroup analysis according to outcome measurement time points 1. Pain—yoga vs. active and passive controls: a. ST: −0.48 (−0.65 to −0.31), p < 0.00001; I2 = 0% b. LT: −0.33 (−0.59 to −0.07), p = 0.01; I2 = 48% 2. General quality of life—yoga vs. active and passive controls: a. ST: 0.41 (−0.11 to 0.93), p = 0.12; I2 = 72% b. LT: 0.18 (−0.05 to 0.41), p = 0.13; I2 = 0% |
| Holtzman et al., 2013 [45] | GRADE Unavailable Tool for quality assessment CLEAR NPT | 6 | 522 with chronic low back pain | EXPERIMENTAL Yoga (Hatha, Viniyoga, Iyengar) CONTROL Exercise, education, or waitlist | Post-treatment analysis: the earliest assessment of the outcome variables after treatment Follow-up analysis: the assessment closest to three months postintervention | Cohen’s d (95%): subgroup analysis according to outcome measurement time points —p value was not reported 1. Pain—yoga vs. exercise, education, or waitlist: a. Post-treatment analysis: 0.623 (0.377 to 0.868); I2 = 22.4% b. Follow-up analysis: 0.397 (0.053 to 0.848); I2 = 74.8% |
| Kim 2020 [35] | GRADE Unavailable Tool for quality assessment The Cochrane risk of bias tool | 6 | 523 with chronic low back pain | EXPERIMENTAL Yoga (Iyengar, Hatha, Viniyoga) CONTROL Education, usual care, or waitlist | After 12 weeks of treatment | SMD (95%): overall effect 1. Pain—yoga vs. education, usual care, or waitlist: −0.41 (−0.58 to −0.23), p < 0.0001; I2 = 0% |
| Nduwimana et al., 2020 [31] | GRADE Unavailable Tool for quality assessment The PEDro scale | 4 | 241 with chronic low back pain | EXPERIMENTAL Yoga CONTROL Unspecified | Intermediate-term (IT) effects: 3–6 months postintervention | SMD (95%CI): subgroup analysis according to the type of experimental group and outcome measurement time points: 1. Pain—yoga vs. control group: a. IT: −1.70 (−3.52 to 0.12), p = 0.07; I2 = 97% |
| Skelly et al., 2020 [28] | GRADE Available Tool for quality assessment The Cochrane risk of bias tool | 9 | 1221 with chronic low back pain | EXPERIMENTAL Yoga (Hatha, Kundalini, Iyengar, Viniyoga) CONTROL Attention control, exercise, usual care, or waitlist | ST: 1 to <6 months following treatment completion IT: >6 to <12 months | MD (95%): subgroup analysis according to the type of control group and outcome measurement time points: 1. Pain—yoga vs. attention control or waitlist: a. ST: −0.87 (−1.49 vs. −0.24) p = 0.014; I2 = 64.1% b. IT: −1.16 (−2.16 to −0.27), p = 0.029; I2 = 0% 2. Pain—yoga vs. exercise: a. ST: −0.63 (−1.68 to 0.45), p = 0.196; I2 = 87.5% |
| Slade et al., 2007 [36] | GRADE Unavailable Tool for quality assessment The PEDro scale | 2 | 145 with chronic low back pain | EXPERIMENTAL Yoga (Viniyoga, Iyengar) CONTROL No exercises plus education | IT: 26 to 32 weeks | SMD (95%): subgroup analysis outcome measurement time points—p value and heterogeneity (I2) were not reported 1. Pain—yoga vs. education or no exercise: a. IT: 0.92 (0.47 to 1.37) |
| Ward et al., 2013 [47] | GRADE Unavailable Tool for quality assessment The Cochrane risk of bias tool and The PEDro scale | 4 | 449 with chronic low back pain | EXPERIMENTAL Yoga (Hatha, Viniyoga, Iyengar) CONTROL Exercise, usual care, or waitlist | Unspecified | SMD (95%): overall effect: 1. Pain—yoga vs. exercise, usual care, or waitlist: −0.61 (−0.97 to −0.26), p = 0.0007; I2 = 63% |
| Wieland et al., 2017 [48] | GRADE Available Tool for quality assessment The Cochrane risk of bias tool and | 6 | 565 with chronic low back pain | EXPERIMENTAL Yoga (Iyengar, Hatha) CONTROL Education or usual care | ST: 4 to 6 weeks SIT: 3 to 4 months IT: 6 months LT: 12 months | MD (95%CI): subgroup analysis according to outcome measurement time points: 1. Pain—Yoga vs. education or usual care: a. ST: −10.83 (−20.85 to −0.81), p = 0.034: I2 = 0% b. SIT (3 to 4 months): −4.55 (−7.04 to −2.06), p = 0.00035; I2 = 0% c. IT: −7.81 (−13.37 to −2.25), p = 0.0059; I2 = 64% d. LT: −5.40 (−14.50 to 3.70), p = 0.24; I2 = 79% SMD (95%CI): subgroup analysis according to outcome measurement time points: 2. Quality of life (physical component)—yoga vs. education or usual care: a. SIT: 0.22 (0.00 to 0.44), p = 0.051; I2 = 0% 3. Quality of life (mental component)—yoga vs. education or usual care: a. SIT: 0.20 (−0.02 to 0.41), p = 0.081; I2 = 0% 4. Depression—yoga vs. education or usual care: a. SIT (3 months): −0.15 (−0.49 to 0.19), p = 0.39; I2 = 0% |
| Zhu et al., 2020 [37] | GRADE Available Tool for quality assessment The Cochrane risk of bias tool and | 17 | 1921 with chronic low back pain | EXPERIMENTAL Yoga (Hatha, Iyengar, Viniyoga) CONTROL Education, exercise, no treatment, physical therapy, or usual care | ST, IT, and LT differed in different subgroup analyses | MD (95%CI): subgroup analysis according to the type of control group and outcome measurement time points: 1. Pain—yoga vs. non-exercise: a. ST (4 to 8 weeks): −0.83 (−1.19 to −0.48), p < 0.00001; I2 = 0% b. SIT (3 months): −0.43 (−0.64 to −0.23), p < 0.0001; I2 = 0% c. IT (6 to 7 months): −0.56 (−1.02 to −0.11), p = 0.02; I2 = 50% d. LT (12 months): −0.52 (−1.64 to 0.59), p = 0.36; I2 = 87% 2. Pain—yoga vs. physical therapy exercise: a. ST (7 days of intensive intervention): −2.36 (−3.15 to −1.56), p < 0.00001; I2 = 0% b. ST (4 to 10 weeks): −0.37 (−1.16 to 0.42), p = 0.36; I2 = 81% c. SIT (3 months): 0.19 (−0.63 to 1.01), p = 0.65; I2 = 64% d. IT (6 months): −0.73 (−2.13 to 0.67), p = 0.31; I2 = 85% 3. Quality of life (physical component)—yoga vs. physical therapy exercise: a. SIT (3 months): 0.18 (−1.97 to 2.32), p = 0.87; I2 = 0% 4. Quality of life (mental component)—yoga vs. physical therapy exercise: a. SIT (3 months): 0.07 (−2.74 to 2.89), p = 0.96; I2 = 0% Results were from a subgroup analysis according to the type of control group and outcome measurement time points: SMD (95%CI) 5. Quality of life (physical component)—yoga vs. non-exercise: a. SIT (3 months): 0.06 (−0.10 to 0.22), p = 0.48; I2 = 0% b. IT (6 months): 0.08 (−0.13 to 0.28), p = 0.45; I2 = 0% 6. Quality of life (mental component)—yoga vs. non-exercise: a. SIT (3 months): 0.15 (−0.01 to 0.31), p = 0.06; I2 = 0% b. IT (6 months): 0.18 (−0.03 to 0.39), p = 0.09; I2 = 0% |
| Zou et al., 2019 [13] | GRADE Unavailable Tool for quality assessment The PEDro scale | 8 | 1237 with chronic low back pain | EXPERIMENTAL Yoga (group and home practice) CONTROL Education, exercise, self-care, or waitlist | Authors declared that none of studies used follow-up assessments | SMD (95%): subgroup analysis according to the type of experimental group: 1. Pain—yoga vs. education, exercise, self-care, or waitlist: −0.33 (−0.47 to −0.19), p = 0.001; I2 = 33.7% |
| CHRONIC NECK PAIN | ||||||
| Cramer et al., 2017 [52] | GRADE Unavailable Tool for quality assessment The Cochrane risk of bias tool | 188 with chronic neck pain | EXPERIMENTAL Yoga (Iyengar) with physiotherapy CONTROL Usual care | ST was not defined | SMD (95%): overall effects 1. Pain—yoga vs. usual care: −1.28 (−1.81 to −0.75), p < 0.00001; I2 = 62% 2. General quality of life—yoga vs. usual care: 0.57 (0.17 to 0.97), p = 0.006; I2 = 20% 3. Mood—yoga vs. usual care: −1.02 (−1.38 to −0.65), p < 0.00001; I2 = 0% | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martinez-Calderon, J.; de-la-Casa-Almeida, M.; Matias-Soto, J. The Effects of Mind–Body Exercises on Chronic Spinal Pain Outcomes: A Synthesis Based on 72 Meta-Analyses. Int. J. Environ. Res. Public Health 2022, 19, 12062. https://doi.org/10.3390/ijerph191912062
Martinez-Calderon J, de-la-Casa-Almeida M, Matias-Soto J. The Effects of Mind–Body Exercises on Chronic Spinal Pain Outcomes: A Synthesis Based on 72 Meta-Analyses. International Journal of Environmental Research and Public Health. 2022; 19(19):12062. https://doi.org/10.3390/ijerph191912062
Chicago/Turabian StyleMartinez-Calderon, Javier, Maria de-la-Casa-Almeida, and Javier Matias-Soto. 2022. "The Effects of Mind–Body Exercises on Chronic Spinal Pain Outcomes: A Synthesis Based on 72 Meta-Analyses" International Journal of Environmental Research and Public Health 19, no. 19: 12062. https://doi.org/10.3390/ijerph191912062