Intermittently Administered Parathyroid Hormone [1–34] Promotes Tendon-Bone Healing in a Rat Model

Abstract
:1. Introduction
2. Results and Discussion
2.1. Results
2.1.1. Serum Chemistry

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Concentration | Control | PTH | p-Value |
|---|---|---|---|
| Calcium (mmol/L) | 2.026 ± 0.396 | 2.383 ± 0.074 * | 0.012 |
| AP (U/L) | 180.6 ± 44.7 | 228.5 ± 22.8 * | 0.007 |
| Osteocalcin (pg/mL) | 353.07 ± 29.62 | 425.77 ± 15.98 * | 0.000 |
| TRAP (mIU/mL) | 2.567 ± 0.892 | 2.938 ± 0.139 * | 0.000 |
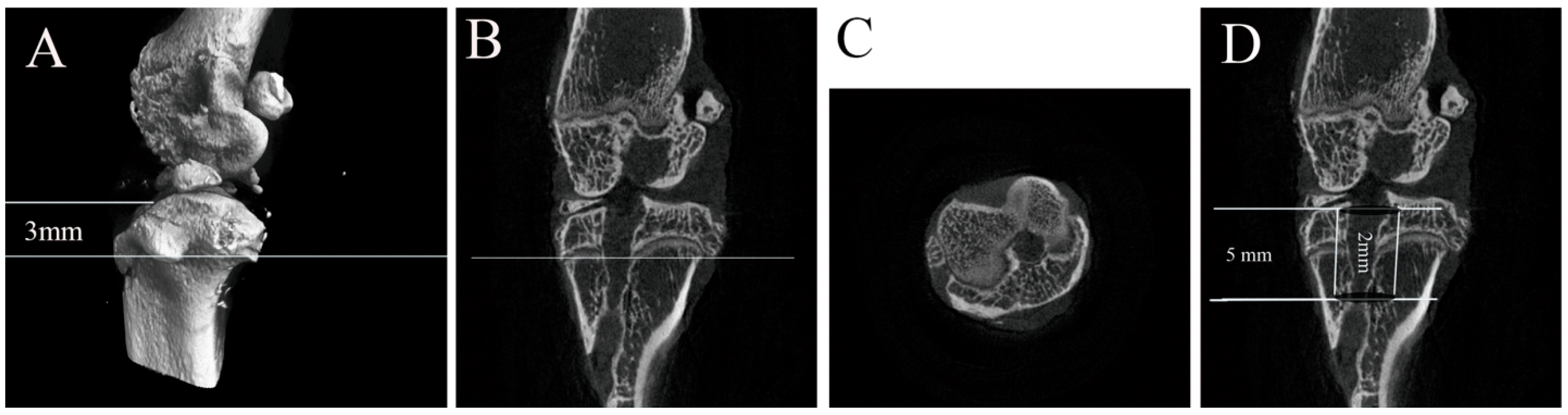
2.1.2. Micro-CT
| Items | Control | PTH | p-Value |
|---|---|---|---|
| Area (mm2) | 2.88 ± 0.32 | 2.35 ± 0.38 * | 0.043 |
| BMD (mg/mL) | 0.3426 ± 0.0059 | 0.4009 ± 0.0083 * | 0.000 |
| BV/TV (%) | 28.52 ± 1.56 | 33.43 ± 1.67 * | 0.001 |
| BS/BV (1/mm) | 11.64225 ± 1.369840 | 16.24998 ± 1.580501 * | 0.001 |
| BS/TV (1/mm) | 3.900066 ± 0.574287 | 4.625814 ± 0.652808 | 0.099 |
| Tb.Th (mm) | 0.235796 ± 0.053191 | 0.349876 ± 0.071286 * | 0.021 |
| Tb.N (1/mm) | 0.992012 ± 0.233659 | 1.243782 ± 0.260488 | 0.146 |
| Tb.Sp (mm) | 1.061898 ± 0.099597 | 0.81308 ± 0.144448 * | 0.013 |
2.1.3. Biomechanical Test
| Items | Control | PTH | p-Value |
|---|---|---|---|
| Failure load (N) | 8.17 ± 0.59 | 16.49 ± 4.90 * | 0.005 |
| Stiffness (N/mm) | 2.48 ± 0.47 | 4.32 ± 1.95 | 0.102 |
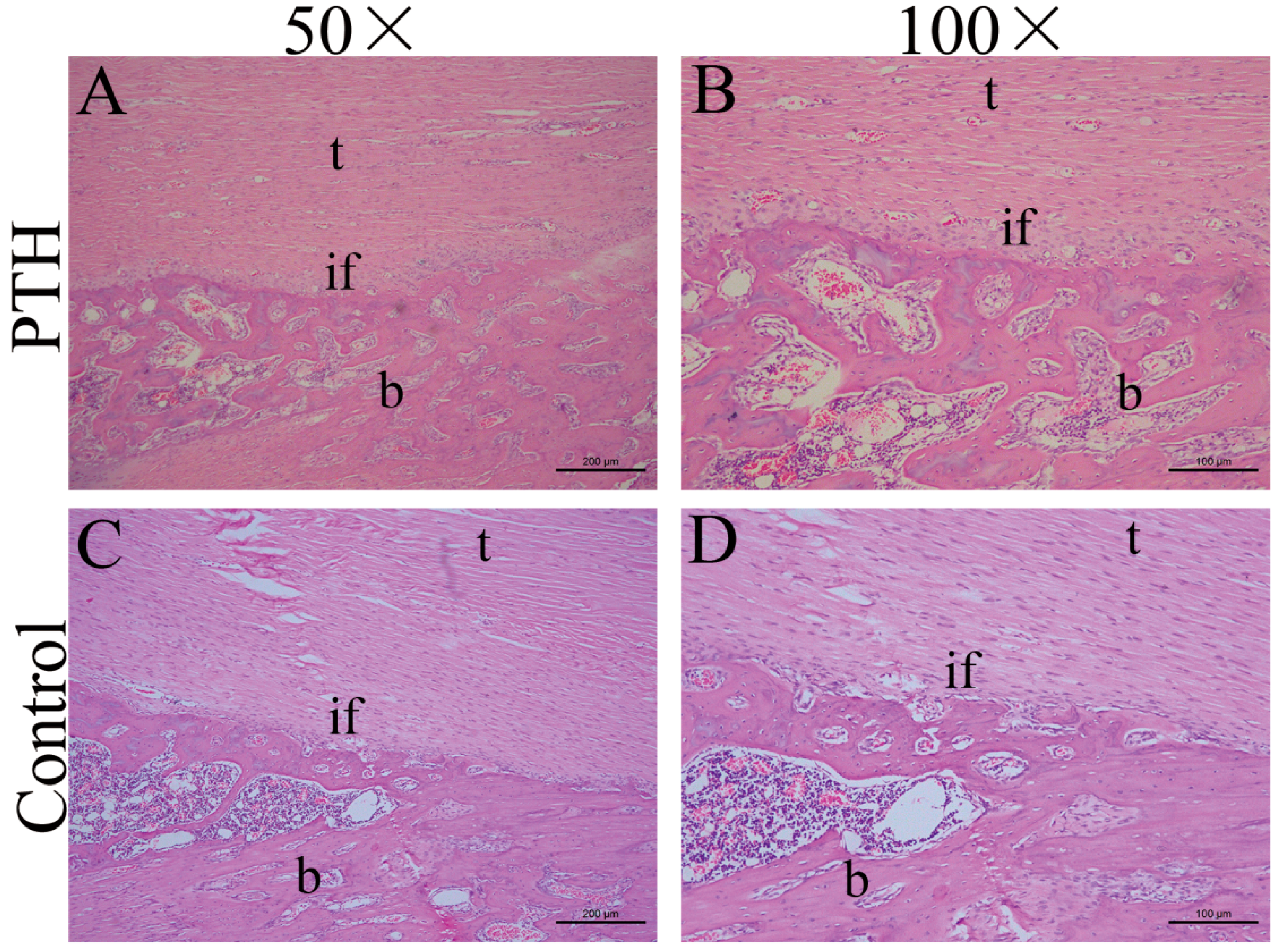
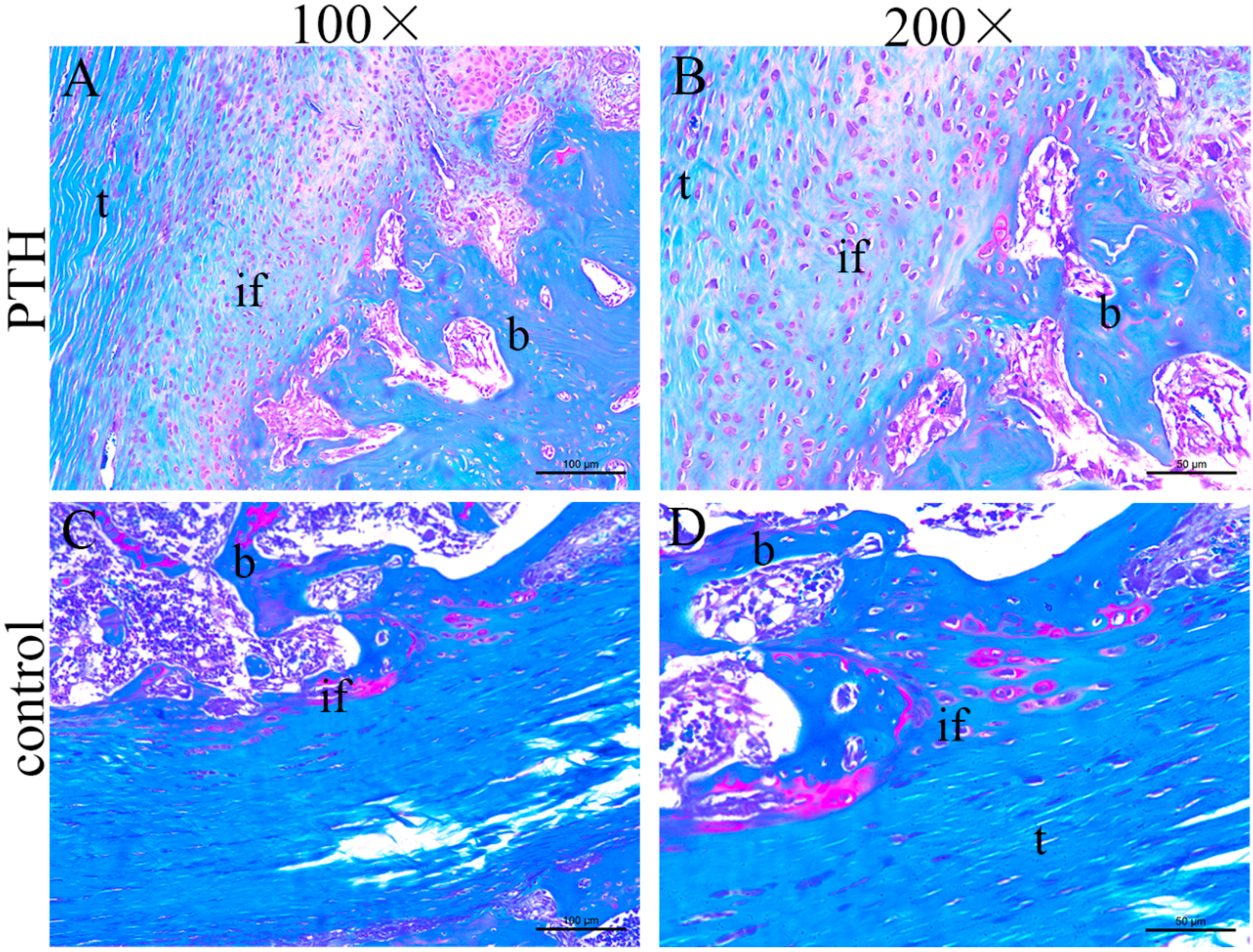
2.1.4. Histological Staining


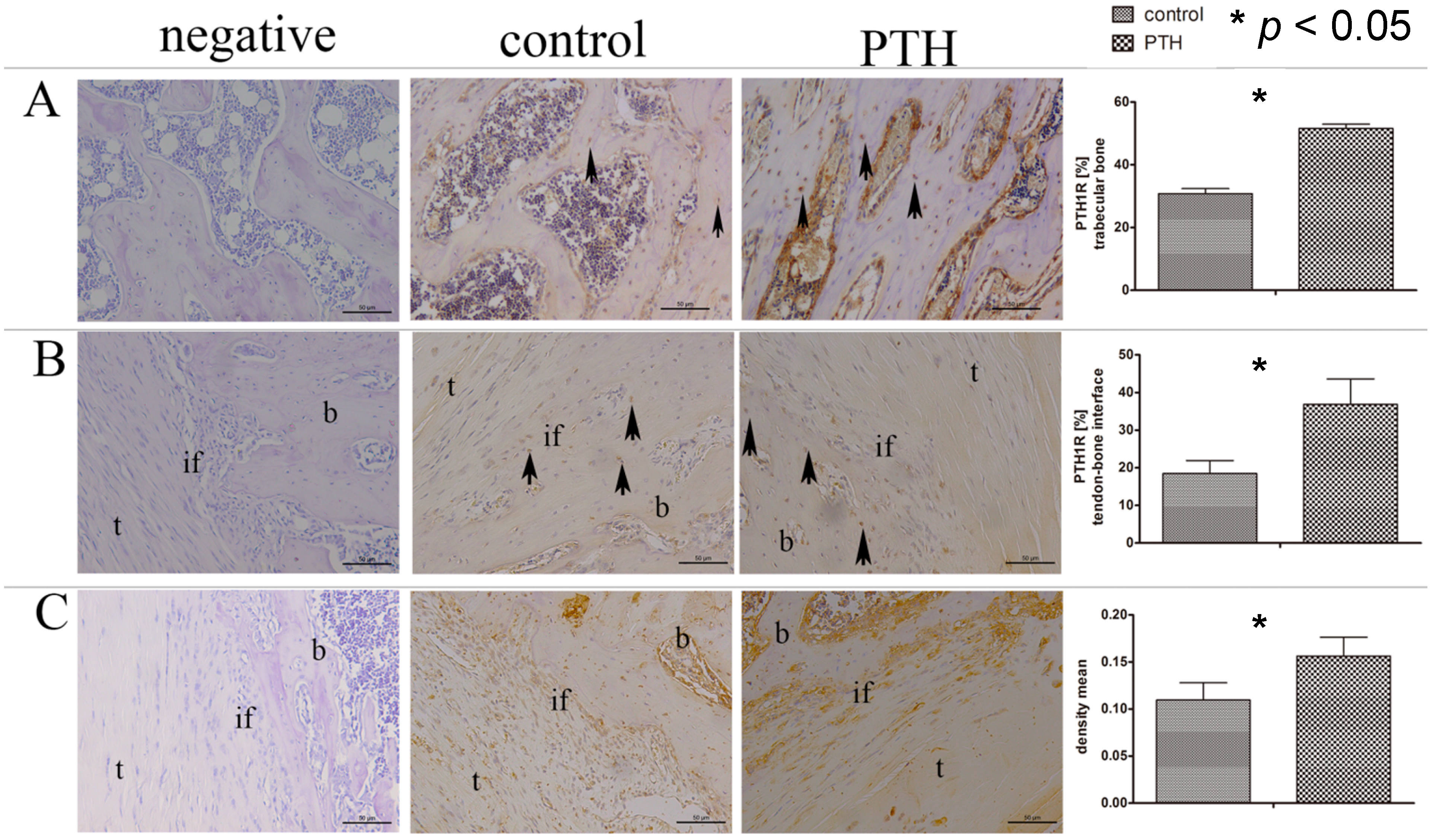
2.1.5. Immunohistochemistry Staining
2.2. Discussion

3. Experimental Section
3.1. Study Design
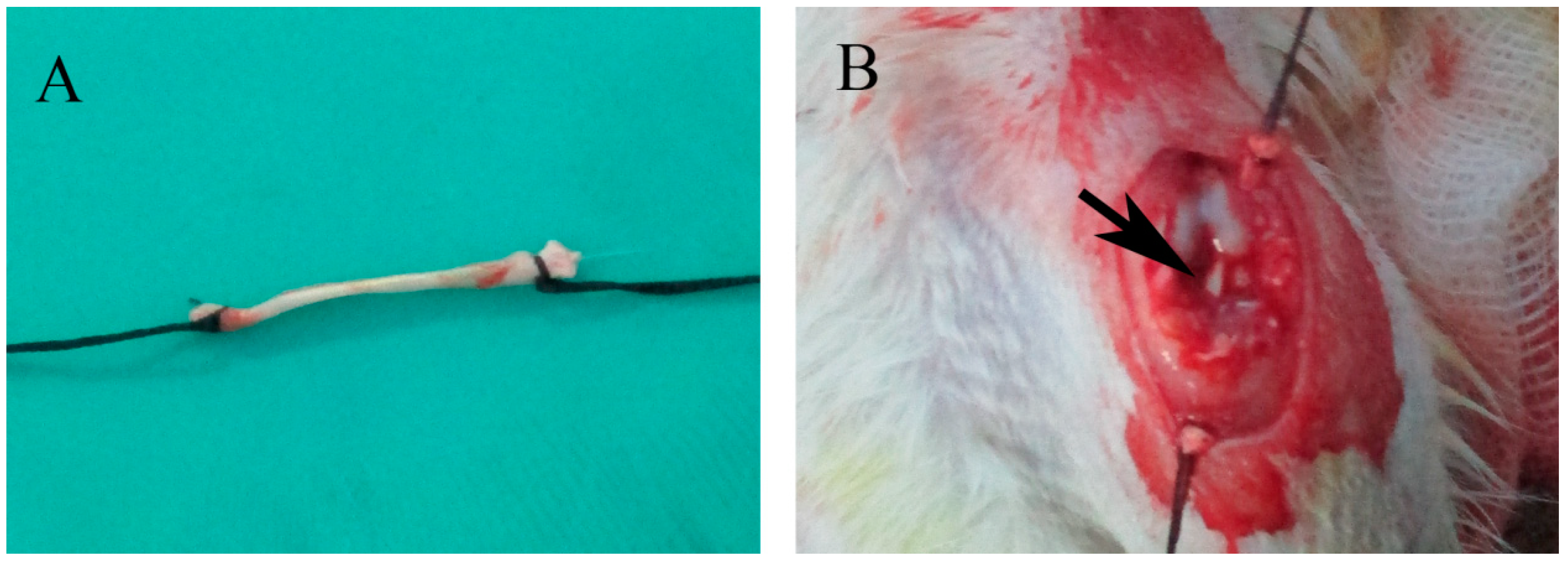
3.2. Surgical Procedure

3.3. Serum Chemistry
3.4. Micro-CT

3.5. Biomechanical Test
3.6. Histological and Immunohistochemical Analyses
3.7. Statistical Analysis
4. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Harner, C.D.; Giffin, J.R.; Dunteman, R.C.; Annunziata, C.C.; Friedman, M.J. Evaluation and treatment of recurrent instability after anterior cruciate ligament reconstruction. Instr. Course Lect. 2001, 50, 463–474. [Google Scholar]
- Fujita, N.; Kuroda, R.; Matsumoto, T.; Yamaguchi, M.; Yagi, M.; Matsumoto, A.; Kubo, S.; Matsushita, T.; Hoshino, Y.; Nishimoto, K.; et al. Comparison of the clinical outcome of double-bundle, anteromedial single-bundle, and posterolateral single-bundle anterior cruciate ligament reconstruction using hamstring tendon graft with minimum 2-year follow-up. Arthroscopy 2011, 27, 906–913. [Google Scholar]
- Giron, F.; Cuomo, P.; Edwards, A.; Bull, A.M.; Amis, A.A.; Aglietti, P. Double-bundle “anatomic” anterior cruciate ligament reconstruction: A cadaveric study of tunnel positioning with a transtibial technique. Arthroscopy 2007, 23, 7–13. [Google Scholar]
- Fu, F.H.; Shen, W.; Starman, J.S.; Okeke, N.; Irrgang, J.J. Primary anatomic double-bundle anterior cruciate ligament reconstruction: A preliminary 2-year prospective study. Am. J. Sports Med. 2008, 36, 1263–1274. [Google Scholar]
- Tomita, F.; Yasuda, K.; Mikami, S.; Sakai, T.; Yamazaki, S.; Tohyama, H. Comparisons of intraosseous graft healing between the doubled flexor tendon graft and the bone-patellar tendon-bone graft in anterior cruciate ligament reconstruction. Arthroscopy 2001, 17, 461–476. [Google Scholar]
- Park, M.J.; Lee, M.C.; Seong, S.C. A comparative study of the healing of tendon autograft and tendon-bone autograft using patellar tendon in rabbits. Int. Orthop. 2001, 25, 35–39. [Google Scholar]
- Papageorgiou, C.D.; Ma, C.B.; Abramowitch, S.D.; Clineff, T.D.; Woo, S.L. A multidisciplinary study of the healing of an intraarticular anterior cruciate ligament graft in a goat model. Am. J. Sports Med. 2001, 29, 620–626. [Google Scholar]
- Rodeo, S.A.; Suzuki, K.; Deng, X.H.; Wozney, J.; Warren, R.F. Use of recombinant human bone morphogenetic protein-2 to enhance tendon healing in a bone tunnel. Am. J. Sports Med. 1999, 27, 476–488. [Google Scholar]
- Wong, M.W.; Qin, L.; Tai, J.K.; Lee, S.K.; Leung, K.S.; Chan, K.M. Engineered allogeneic chondrocyte pellet for reconstruction of fibrocartilage zone at bone-tendon junction—A preliminary histological observation. J. Biomed. Mater. Res. B 2004, 70, 362–367. [Google Scholar]
- Rothrauff, B.B.; Tuan, R.S. Cellular therapy in bone-tendon interface regeneration. Organogenesis 2014, 10, 13–28. [Google Scholar]
- Gulotta, L.V.; Kovacevic, D.; Ying, L.; Ehteshami, J.R.; Montgomery, S.; Rodeo, S.A. Augmentation of tendon-to-bone healing with a magnesium-based bone adhesive. Am. J. Sports Med. 2008, 36, 1290–1297. [Google Scholar]
- Rhee, Y.; Allen, M.R.; Condon, K.; Lezcano, V.; Ronda, A.C.; Galli, C.; Olivos, N.; Passeri, G.; O’Brien, C.A.; Bivi, N.; et al. PTH receptor signaling in osteocytes governs periosteal bone formation and intracortical remodeling. J. Bone Miner. Res. 2011, 26, 1035–1046. [Google Scholar]
- Bukata, S.V. Systemic administration of pharmacological agents and bone repair: What can we expect. Injury 2011, 42, 605–608. [Google Scholar]
- Weisser, J.; Riemer, S.; Schmidl, M.; Suva, L.J.; Poschl, E.; Brauer, R.; von der Mark, K. Four distinct chondrocyte populations in the fetal bovine growth plate: Highest expression levels of PTH/PTHrP receptor, Indian hedgehog, and MMP-13 in hypertrophic chondrocytes and their suppression by PTH (1–34) and PTHrP (1–40). Exp. Cell Res. 2002, 279, 1–13. [Google Scholar]
- Jilka, R.L. Molecular and cellular mechanisms of the anabolic effect of intermittent PTH. Bone 2007, 40, 1434–1446. [Google Scholar]
- Chandra, A.; Lan, S.; Zhu, J.; Lin, T.; Zhang, X.; Siclari, V.A.; Altman, A.R.; Cengel, K.A.; Liu, X.S.; Qin, L. PTH prevents the adverse effects of focal radiation on bone architecture in young rats. Bone 2013, 55, 449–457. [Google Scholar]
- Qin, L.; Raggatt, L.J.; Partridge, N.C. Parathyroid hormone: A double-edged sword for bone metabolism. Trends Endocrinol. Metab. 2004, 15, 60–65. [Google Scholar]
- Recker, R.R.; Bare, S.P.; Smith, S.Y.; Varela, A.; Miller, M.A.; Morris, S.A.; Fox, J. Cancellous and cortical bone architecture and turnover at the iliac crest of postmenopausal osteoporotic women treated with parathyroid hormone 1–84. Bone 2009, 44, 113–119. [Google Scholar]
- Jiang, Y.; Zhao, J.J.; Mitlak, B.H.; Wang, O.; Genant, H.K.; Eriksen, E.F. Recombinant human parathyroid hormone (1–34) [teriparatide] improves both cortical and cancellous bone structure. J. Bone Miner. Res. 2003, 18, 1932–1941. [Google Scholar]
- Ma, C.B.; Kawamura, S.; Deng, X.H.; Ying, L.; Schneidkraut, J.; Hays, P.; Rodeo, S.A. Bone morphogenetic proteins-signaling plays a role in tendon-to-bone healing: A study of rhBMP-2 and noggin. Am. J. Sports Med. 2007, 35, 597–604. [Google Scholar]
- Manning, C.N.; Kim, H.M.; Sakiyama-Elbert, S.; Galatz, L.M.; Havlioglu, N.; Thomopoulos, S. Sustained delivery of transforming growth factor beta three enhances tendon-to-bone healing in a rat model. J. Orthop. Res. 2011, 29, 1099–1105. [Google Scholar]
- Sasaki, K.; Kuroda, R.; Ishida, K.; Kubo, S.; Matsumoto, T.; Mifune, Y.; Kinoshita, K.; Tei, K.; Akisue, T.; Tabata, Y.; et al. Enhancement of tendon-bone osteointegration of anterior cruciate ligament graft using granulocyte colony-stimulating factor. Am. J. Sports Med. 2008, 36, 1519–1527. [Google Scholar]
- Kovacevic, D.; Fox, A.J.; Bedi, A.; Ying, L.; Deng, X.H.; Warren, R.F.; Rodeo, S.A. Calcium–phosphate matrix with or without TGF-β3 improves tendon-bone healing after rotator cuff repair. Am. J. Sports Med. 2011, 39, 811–819. [Google Scholar]
- Walsh, W.R.; Stephens, P.; Vizesi, F.; Bruce, W.; Huckle, J.; Yu, Y. Effects of low-intensity pulsed ultrasound on tendon-bone healing in an intra-articular sheep knee model. Arthroscopy 2007, 23, 197–204. [Google Scholar]
- Atesok, K.; Fu, F.H.; Wolf, M.R.; Ochi, M.; Jazrawi, L.M.; Doral, M.N.; Lubowitz, J.H.; Rodeo, S.A. Augmentation of tendon-to-bone healing. J. Bone Jt. Surg. Am. 2014, 96, 513–521. [Google Scholar]
- Ellegaard, M.; Kringelbach, T.; Syberg, S.; Petersen, S.; Beck Jensen, J.E.; Bruel, A.; Jorgensen, N.R.; Schwarz, P. The effect of PTH(1–34) on fracture healing during different loading conditions. J. Bone Miner. Res. 2013, 28, 2145–2155. [Google Scholar]
- Malhotra, R.; Meena, S.; Digge, V.K. Tensile type of stress fracture neck of femur: Role of teriparatide in the process of healing in a high risk patient for impaired healing of fracture. Clin. Cases Mineral Bone Metab. 2013, 10, 210–212. [Google Scholar]
- Ellegaard, M.; Jorgensen, N.R.; Schwarz, P. Parathyroid hormone and bone healing. Calcif. Tissue Int. 2010, 87, 1–13. [Google Scholar]
- Bruel, A.; Vegger, J.B.; Raffalt, A.C.; Andersen, J.E.; Thomsen, J.S. PTH(1–34), but not strontium ranelate counteract loss of trabecular thickness and bone strength in disuse osteopenic rats. Bone 2013, 53, 51–58. [Google Scholar]
- Li, Y.F.; Li, X.D.; Bao, C.Y.; Chen, Q.M.; Zhang, H.; Hu, J. Promotion of peri-implant bone healing by systemically administered parathyroid hormone (1–34) and zoledronic acid adsorbed onto the implant surface. Osteoporos. Int. 2013, 24, 1063–1071. [Google Scholar]
- Hock, J.M.; Gera, I. Effects of continuous and intermittent administration and inhibition of resorption on the anabolic response of bone to parathyroid hormone. J. Bone Miner. Res. 1992, 7, 65–72. [Google Scholar]
- Neer, R.M.; Arnaud, C.D.; Zanchetta, J.R.; Prince, R.; Gaich, G.A.; Reginster, J.Y.; Hodsman, A.B.; Eriksen, E.F.; Ish-Shalom, S.; Genant, H.K.; et al. Effect of parathyroid hormone (1–34) on fractures and bone mineral density in postmenopausal women with osteoporosis. N. Engl. J. Med. 2001, 344, 1434–1441. [Google Scholar]
- Hirano, T.; Burr, D.B.; Turner, C.H.; Sato, M.; Cain, R.L.; Hock, J.M. Anabolic effects of human biosynthetic parathyroid hormone fragment (1–34), LY333334, on remodeling and mechanical properties of cortical bone in rabbits. J. Bone Miner. Res. 1999, 14, 536–545. [Google Scholar]
- Wu, X.; Pang, L.; Lei, W.; Lu, W.; Li, J.; Li, Z.; Frassica, F.J.; Chen, X.; Wan, M.; Cao, X. Inhibition of Sca-1-positive skeletal stem cell recruitment by alendronate blunts the anabolic effects of parathyroid hormone on bone remodeling. Cell Stem Cell 2010, 7, 571–580. [Google Scholar]
- Brouwers, J.E.; van Rietbergen, B.; Huiskes, R.; Ito, K. Effects of PTH treatment on tibial bone of ovariectomized rats assessed by in vivo micro-CT. Osteoporos. Int. 2009, 20, 1823–1835. [Google Scholar]
- Bellido, M.; Lugo, L.; Roman-Blas, J.A.; Castaneda, S.; Calvo, E.; Largo, R.; Herrero-Beaumont, G. Improving subchondral bone integrity reduces progression of cartilage damage in experimental osteoarthritis preceded by osteoporosis. Osteoarthr. Cartil. 2011, 19, 1228–1236. [Google Scholar]
- Fan, H.; Liu, H.; Wong, E.J.; Toh, S.L.; Goh, J.C. In vivo study of anterior cruciate ligament regeneration using mesenchymal stem cells and silk scaffold. Biomaterials 2008, 29, 3324–3337. [Google Scholar]
- Pinczewski, L.A.; Clingeleffer, A.J.; Otto, D.D.; Bonar, S.F.; Corry, I.S. Integration of hamstring tendon graft with bone in reconstruction of the anterior cruciate ligament. Arthroscopy 1997, 13, 641–643. [Google Scholar]
- Oka, S.; Matsumoto, T.; Kubo, S.; Matsushita, T.; Sasaki, H.; Nishizawa, Y.; Matsuzaki, T.; Saito, T.; Nishida, K.; Tabata, Y.; et al. Local administration of low-dose simvastatin-conjugated gelatin hydrogel for tendon-bone healing in anterior cruciate ligament reconstruction. Tissue Eng. A 2013, 19, 1233–1243. [Google Scholar]
- Kobayashi, M.; Watanabe, N.; Oshima, Y.; Kajikawa, Y.; Kawata, M.; Kubo, T. The fate of host and graft cells in early healing of bone tunnel after tendon graft. Am. J. Sports Med. 2005, 33, 1892–1897. [Google Scholar]
- Kawamura, S.; Ying, L.; Kim, H.; Dynybil, C.; Rodeo, S. Macrophages accumulate in the early phase of tendon-bone healing. J. Orthop. Res. 2005, 23, 1425–1432. [Google Scholar]
- Lim, J.K.; Hui, J.; Li, L.; Thambyah, A.; Goh, J.; Lee, E.H. Enhancement of tendon graft osteointegration using mesenchymal stem cells in a rabbit model of anterior cruciate ligament reconstruction. Arthroscopy 2004, 20, 899–910. [Google Scholar]
- Soon, M.Y.; Hassan, A.; Hui, J.H.; Goh, J.C.; Lee, E.H. An analysis of soft tissue allograft anterior cruciate ligament reconstruction in a rabbit model: A short-term study of the use of mesenchymal stem cells to enhance tendon osteointegration. Am. J. Sports Med. 2007, 35, 962–971. [Google Scholar]
- Mendez-Ferrer, S.; Michurina, T.V.; Ferraro, F.; Mazloom, A.R.; Macarthur, B.D.; Lira, S.A.; Scadden, D.T.; Ma’ayan, A.; Enikolopov, G.N.; Frenette, P.S. Mesenchymal and haematopoietic stem cells form a unique bone marrow niche. Nature 2010, 466, 829–834. [Google Scholar]
- Fermor, B.; Skerry, T.M. PTH/PTHrP receptor expression on osteoblasts and osteocytes but not resorbing bone surfaces in growing rats. J. Bone Miner. Res. 1995, 10, 1935–1943. [Google Scholar]
- Bellido, T.; Saini, V.; Pajevic, P.D. Effects of PTH on osteocyte function. Bone 2013, 54, 250–257. [Google Scholar]
- Chen, Y.; Bai, B.; Zhang, S.; Ye, J.; Chen, Y.; Zeng, Y. Effects of parathyroid hormone on calcium ions in rat bone marrow mesenchymal stem cells. BioMed Res. Int. 2014, 2014, 258409. [Google Scholar]
- Coleman, D.T.; Bilezikian, J.P. Parathyroid hormone stimulates formation of inositol phosphates in a membrane preparation of canine renal cortical tubular cells. J. Bone Miner. Res. 1990, 5, 299–306. [Google Scholar]
- Wang, Y.; Nishida, S.; Boudignon, B.M.; Burghardt, A.; Elalieh, H.Z.; Hamilton, M.M.; Majumdar, S.; Halloran, B.P.; Clemens, T.L.; Bikle, D.D. IGF-I receptor is required for the anabolic actions of parathyroid hormone on bone. J. Bone Miner. Res. 2007, 22, 1329–1337. [Google Scholar]
- Lovric, V.; Chen, D.; Yu, Y.; Oliver, R.A.; Genin, F.; Walsh, W.R. Effects of demineralized bone matrix on tendon-bone healing in an intra-articular rodent model. Am. J. Sports Med. 2012, 40, 2365–2374. [Google Scholar]
- Bouxsein, M.L.; Boyd, S.K.; Christiansen, B.A.; Guldberg, R.E.; Jepsen, K.J.; Muller, R. Guidelines for assessment of bone microstructure in rodents using micro-computed tomography. J. Bone Miner. Res. 2010, 25, 1468–1486. [Google Scholar]
© 2014 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bi, F.; Shi, Z.; Jiang, S.; Guo, P.; Yan, S. Intermittently Administered Parathyroid Hormone [1–34] Promotes Tendon-Bone Healing in a Rat Model. Int. J. Mol. Sci. 2014, 15, 17366-17379. https://doi.org/10.3390/ijms151017366
Bi F, Shi Z, Jiang S, Guo P, Yan S. Intermittently Administered Parathyroid Hormone [1–34] Promotes Tendon-Bone Healing in a Rat Model. International Journal of Molecular Sciences. 2014; 15(10):17366-17379. https://doi.org/10.3390/ijms151017366
Chicago/Turabian StyleBi, Fanggang, Zhongli Shi, Shuai Jiang, Peng Guo, and Shigui Yan. 2014. "Intermittently Administered Parathyroid Hormone [1–34] Promotes Tendon-Bone Healing in a Rat Model" International Journal of Molecular Sciences 15, no. 10: 17366-17379. https://doi.org/10.3390/ijms151017366