Exploring the In Vivo Anti-Inflammatory Actions of Simvastatin-Loaded Porous Microspheres on Inflamed Tenocytes in a Collagenase-Induced Animal Model of Achilles Tendinitis

 and
and
Abstract
:
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
1. Introduction
2. Results
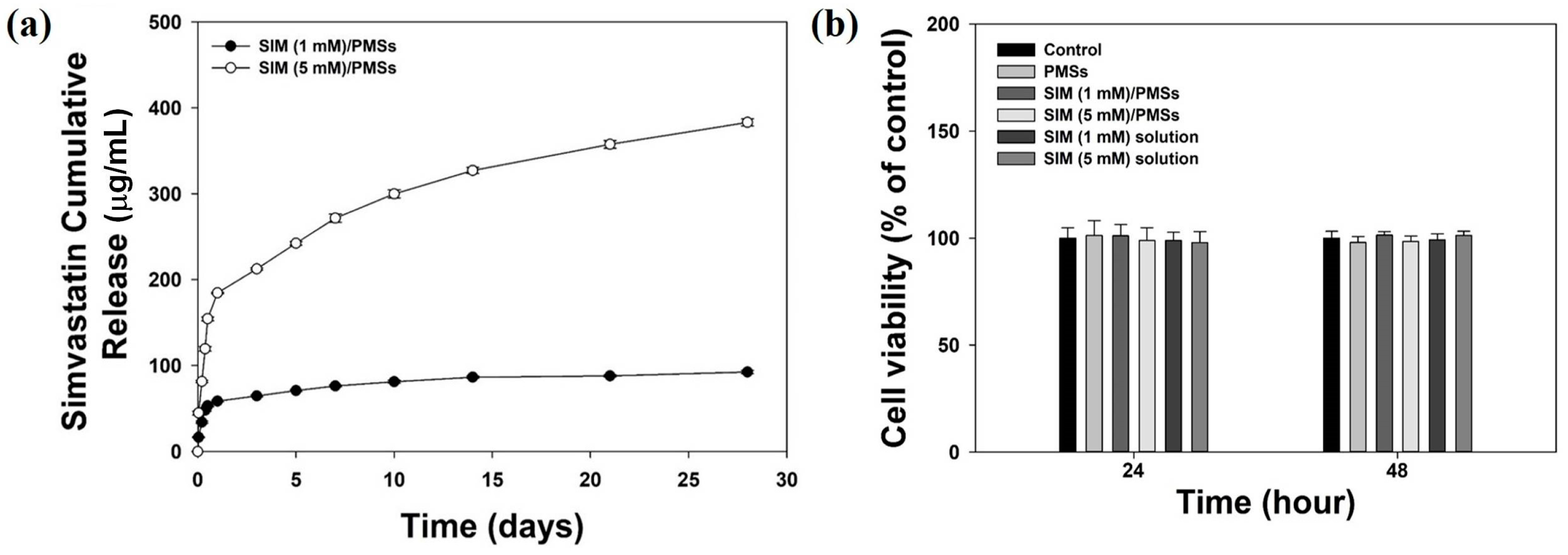
2.1. Characterizing PMSs and SIM/PMSs in an In Vitro Drug Release Study
2.2. In Vitro Cytotoxicity
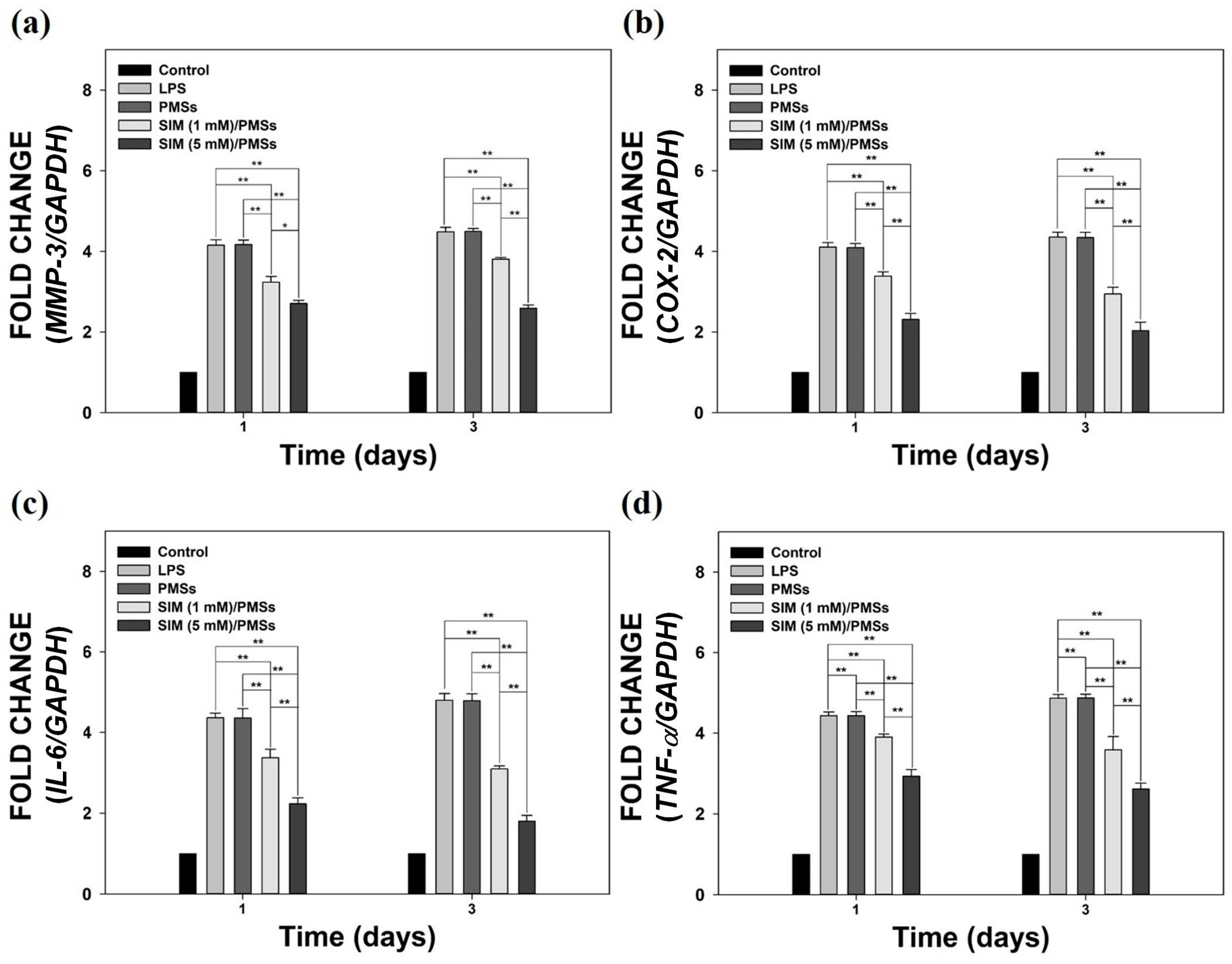
2.3. Anti-Inflammatory Properties of SIM/PMSs in Inflamed Tenocytes
2.4. Histopathological Evaluations
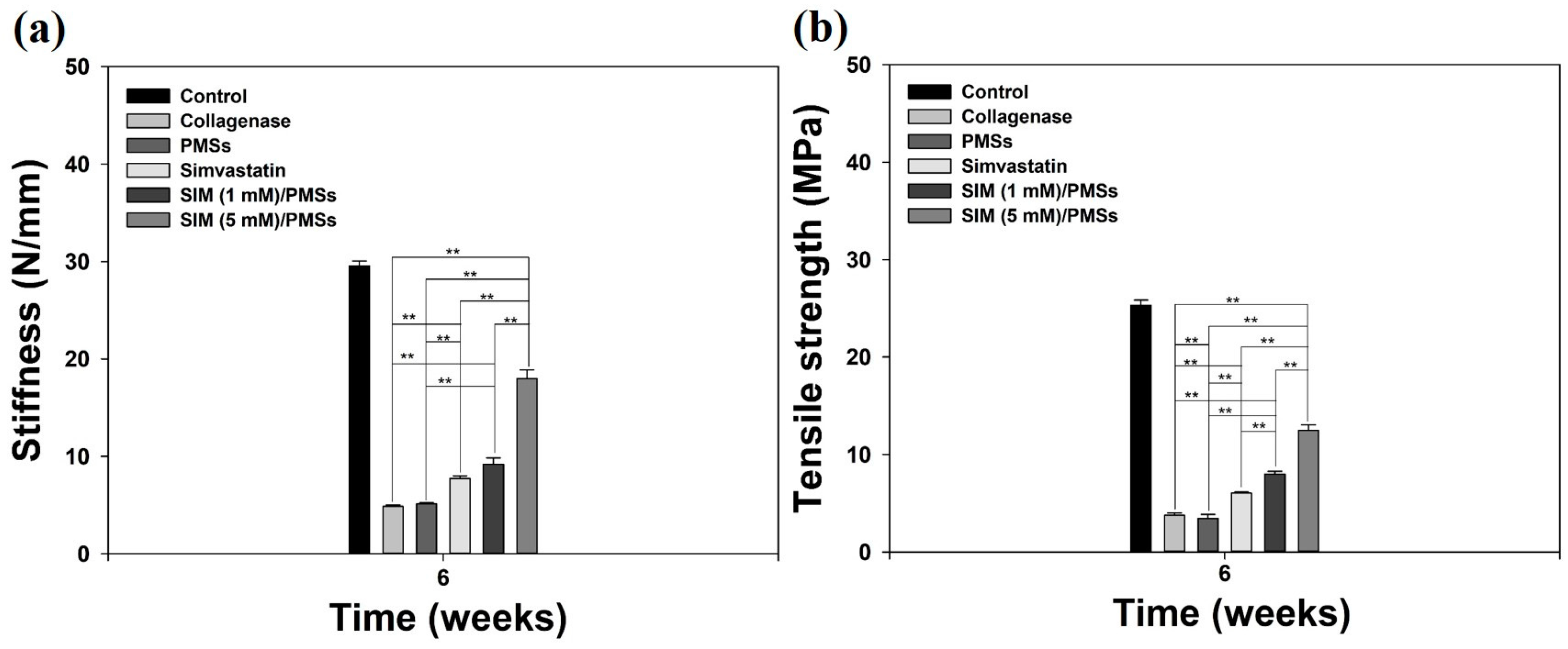
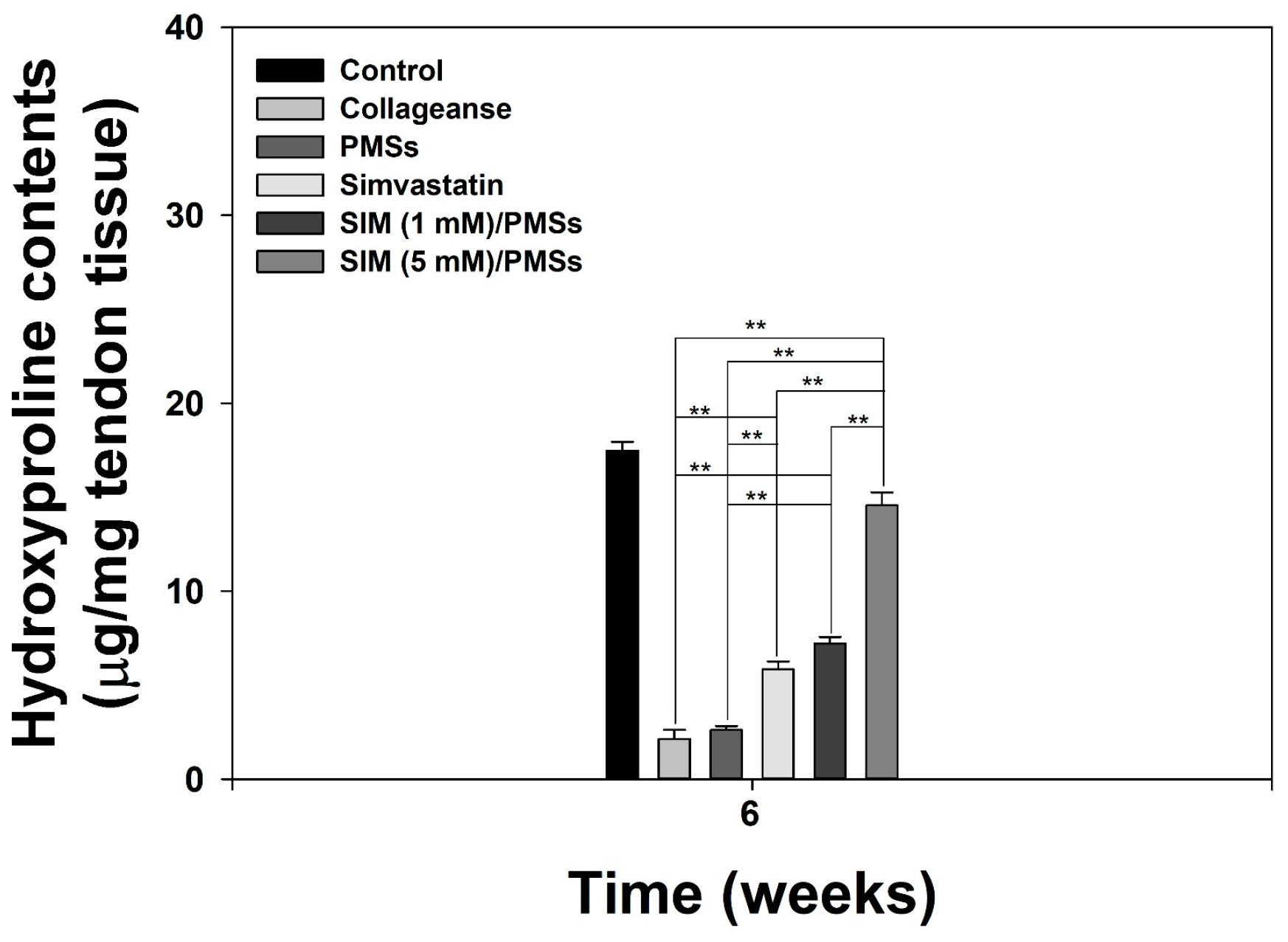
2.5. In Vivo Tendon Restorative Effects of SIM/PMSs and Biomechanical Study
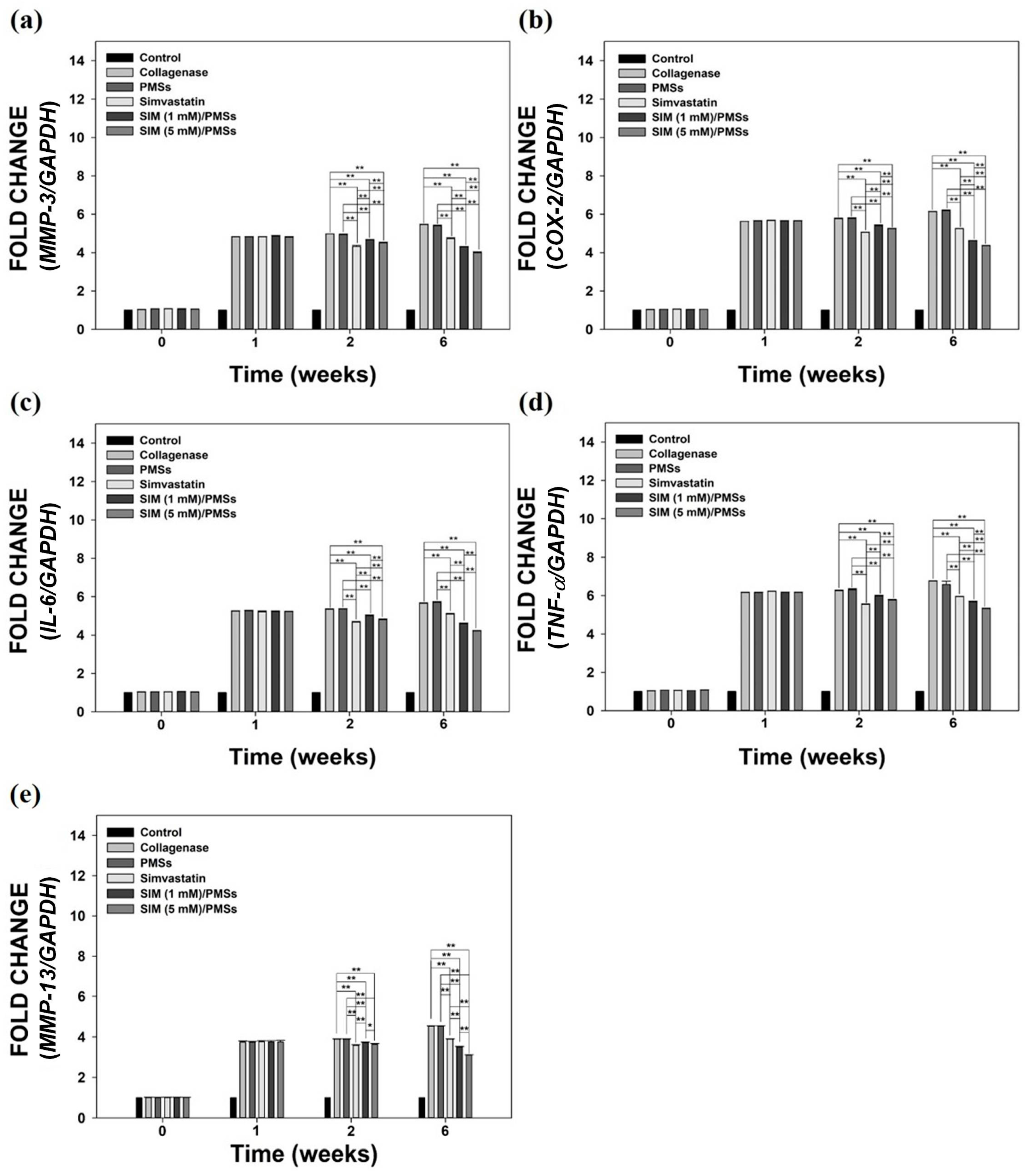
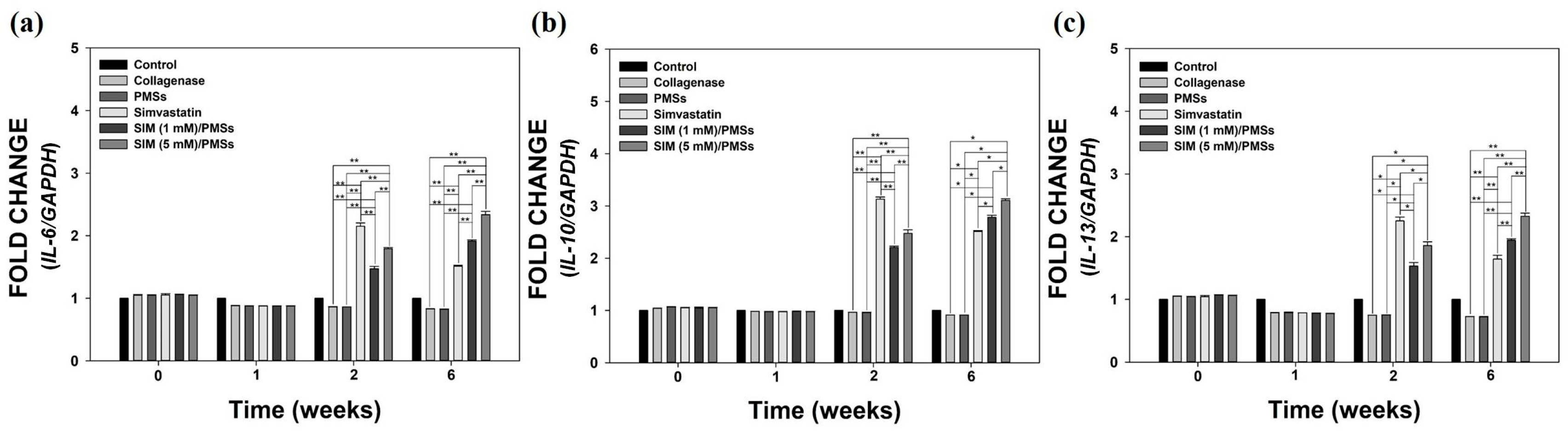
2.6. In Vivo Anti-Inflammatory Effects of SIM/PMSs
3. Discussion
4. Materials and Methods
4.1. Materials
4.2. Fabrication of SIM-Loaded Porous Microspheres (SIM/PMSs)
4.3. Characterization of PMSs and SIM/PMSs
4.4. In Vitro Drug Release Study
4.5. In Vitro Cytotoxicity
4.6. In Vitro Anti-Inflammatory Effects of SIM/PMSs on Inflamed Tenocytes
4.7. Animal Models of Collagenase-Induced Achilles Tendinitis
4.8. Histopathological Evaluations
4.9. Biomechanical Test
4.10. Hydroxyproline Assay
4.11. In Vivo Anti-Inflammatory Effects of SIM/PMSs on Collagenase-Induced Achilles Tendinitis
4.12. Statistical Analysis
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Lopez, R.G.; Jung, H.G. Achilles tendinosis: Treatment options. Clin. Orthop. Surg. 2015, 7, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Maffulli, N.; Khan, K.M.; Puddu, G. Overuse tendon conditions: Time to change a confusing terminology. Arthroscopy 1998, 14, 840–843. [Google Scholar] [CrossRef]
- Sharma, P.; Maffulli, N. Tendon injury and tendinopathy: Healing and repair. J. Bone Jt. Surg. Am. 2005, 87, 187–202. [Google Scholar]
- Nagase, H.; Visse, R.; Murphy, G. Structure and function of matrix metalloproteinases and timps. Cardiovasc. Res. 2006, 69, 562–573. [Google Scholar] [CrossRef] [PubMed]
- Langberg, H.; Boushel, R.; Skovgaard, D.; Risum, N.; Kjaer, M. Cyclo-oxygenase-2 mediated prostaglandin release regulates blood flow in connective tissue during mechanical loading in humans. J. Physiol. 2003, 551, 683–689. [Google Scholar] [CrossRef] [PubMed]
- Schulze-Tanzil, G.; Al-Sadi, O.; Wiegand, E.; Ertel, W.; Busch, C.; Kohl, B.; Pufe, T. The role of pro-inflammatory and immunoregulatory cytokines in tendon healing and rupture: New insights. Scand. J. Med. Sci. Sports 2011, 21, 337–351. [Google Scholar] [CrossRef] [PubMed]
- Moore, R.A.; Tramer, M.R.; Carroll, D.; Wiffen, P.J.; McQuay, H.J. Quantitative systematic review of topically applied non-steroidal anti-inflammatory drugs. BMJ 1998, 316, 333–338. [Google Scholar] [CrossRef] [PubMed]
- Fredberg, U.; Stengaard-Pedersen, K. Chronic tendinopathy tissue pathology, pain mechanisms, and etiology with a special focus on inflammation. Scand. J. Med. Sci. Sports 2008, 18, 3–15. [Google Scholar] [CrossRef] [PubMed]
- Smidt, N.; van der Windt, D.A.; Assendelft, W.J.; Deville, W.L.; Korthals-de Bos, I.B.; Bouter, L.M. Corticosteroid injections, physiotherapy, or a wait-and-see policy for lateral epicondylitis: A randomised controlled trial. Lancet 2002, 359, 657–662. [Google Scholar] [CrossRef]
- Tsai, W.C.; Yu, T.Y.; Lin, L.P.; Cheng, M.L.; Chen, C.L.; Pang, J.H. Prevention of simvastatin-induced inhibition of tendon cell proliferation and cell cycle progression by geranylgeranyl pyrophosphate. Toxicol. Sci. 2016, 149, 326–334. [Google Scholar] [CrossRef] [PubMed]
- McFarland, A.J.; Davey, A.K.; Anoopkumar-Dukie, S. Statins reduce lipopolysaccharide-induced cytokine and inflammatory mediator release in an in vitro model of microglial-like cells. Med. Inflamm. 2017, 2017, 2582745. [Google Scholar] [CrossRef] [PubMed]
- Rosenson, R.S.; Tangney, C.C.; Casey, L.C. Inhibition of proinflammatory cytokine production by pravastatin. Lancet 1999, 353, 983–984. [Google Scholar] [CrossRef]
- Loppnow, H.; Zhang, L.; Buerke, M.; Lautenschlager, M.; Chen, L.; Frister, A.; Schlitt, A.; Luther, T.; Song, N.; Hofmann, B.; et al. Statins potently reduce the cytokine-mediated IL-6 release in SMC/MNC cocultures. J. Cell. Mol. Med. 2011, 15, 994–1004. [Google Scholar] [CrossRef] [PubMed]
- Marschner, I.C.; Colquhoun, D.; Simes, R.J.; Glasziou, P.; Harris, P.; Singh, B.B.; Friedlander, D.; White, H.; Thompson, P.; Tonkin, A.; et al. Long-term risk stratification for survivors of acute coronary syndromes. Results from the long-term intervention with pravastatin in ischemic disease (lipid) study. Lipid study investigators. J. Am. Coll. Cardiol. 2001, 38, 56–63. [Google Scholar] [CrossRef]
- Hayem, G. Statins and muscles: What price glory? Jt. Bone Spine 2002, 69, 249–251. [Google Scholar] [CrossRef]
- Kashani, A.; Sallam, T.; Bheemreddy, S.; Mann, D.L.; Wang, Y.; Foody, J.M. Review of side-effect profile of combination ezetimibe and statin therapy in randomized clinical trials. Am. J. Cardiol. 2008, 101, 1606–1613. [Google Scholar] [CrossRef] [PubMed]
- Eliasson, P.; Svensson, R.B.; Giannopoulos, A.; Eismark, C.; Kjaer, M.; Schjerling, P.; Heinemeier, K.M. Simvastatin and atorvastatin reduce the mechanical properties of tendon constructs in vitro and introduce catabolic changes in the gene expression pattern. PLoS ONE 2017, 12, e0172797. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.E.; Yun, Y.P.; Shim, K.S.; Park, K.; Choi, S.W.; Shin, D.H.; Suh, D.H. Fabrication of a BMP-2-immobilized porous microsphere modified by heparin for bone tissue engineering. Coll. Surf. B Biointerfaces 2015, 134, 453–460. [Google Scholar] [CrossRef] [PubMed]
- Park, J.W.; Yun, Y.P.; Park, K.; Lee, J.Y.; Kim, H.J.; Kim, S.E.; Song, H.R. Ibuprofen-loaded porous microspheres suppressed the progression of monosodium iodoacetate-induced osteoarthritis in a rat model. Coll. Surf. B Biointerfaces 2016, 147, 265–273. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.Y.; Kim, S.E.; Yun, Y.P.; Choi, S.W.; Jeon, D.I.; Kim, H.J.; Park, K.; Song, H.R. Osteogenesis and new bone formation of alendronate-immobilized porous plga microspheres in a rat calvarial defect model. J. Ind. Eng. Chem. 2017, 52, 277–286. [Google Scholar] [CrossRef]
- Kim, S.E.; Yun, Y.P.; Shim, K.S.; Jeon, D.I.; Park, K.; Kim, H.J. In vitro and in vivo anti-inflammatory and tendon-healing effects in achilles tendinopathy of long-term curcumin delivery using porous microspheres. J. Ind. Eng. Chem. 2018, 58, 123–130. [Google Scholar] [CrossRef]
- Hollinger, J.O.; Battistone, G.C. Biodegradable bone repair materials. Synthetic polymers and ceramics. Clin. Orthop. Relat. Res. 1986, 290–305. [Google Scholar]
- Maffulli, N.; Wong, J.; Almekinders, L.C. Types and epidemiology of tendinopathy. Clin. Sports Med. 2003, 22, 675–692. [Google Scholar] [CrossRef]
- Weber, C.; Erl, W.; Weber, K.S.; Weber, P.C. HMG-CoA reductase inhibitors decrease CD11b expression and CD11b-dependent adhesion of monocytes to endothelium and reduce increased adhesiveness of monocytes isolated from patients with hypercholesterolemia. J. Am. Coll. Cardiol. 1997, 30, 1212–1217. [Google Scholar] [CrossRef]
- Buchwald, H.; Campos, C.T.; Boen, J.R.; Nguyen, P.A.; Williams, S.E. Disease-free intervals after partial ileal bypass in patients with coronary heart disease and hypercholesterolemia: Report from the program on the surgical control of the hyperlipidemias (posch). J. Am. Coll. Cardiol. 1995, 26, 351–357. [Google Scholar] [CrossRef]
- Contractor, T.; Beri, A.; Gardiner, J.C.; Tang, X.; Dwamena, F.C. Is statin use associated with tendon rupture? A population-based retrospective cohort analysis. Am. J. Ther. 2015, 22, 377–381. [Google Scholar] [CrossRef] [PubMed]
- Beri, A.; Dwamena, F.C.; Dwamena, B.A. Association between statin therapy and tendon rupture: A case-control study. J. Cardiovasc. Pharmacol. 2009, 53, 401–404. [Google Scholar] [CrossRef] [PubMed]
- Lin, T.T.; Lin, C.H.; Chang, C.L.; Chi, C.H.; Chang, S.T.; Sheu, W.H. The effect of diabetes, hyperlipidemia, and statins on the development of rotator cuff disease: A nationwide, 11-year, longitudinal, population-based follow-up study. Am. J. Sports Med. 2015, 43, 2126–2132. [Google Scholar] [CrossRef] [PubMed]
- Dolkart, O.; Liron, T.; Chechik, O.; Somjen, D.; Brosh, T.; Maman, E.; Gabet, Y. Statins enhance rotator cuff healing by stimulating the COX2/PGE2/EP4 pathway: An in vivo and in vitro study. Am. J. Sports Med. 2014, 42, 2869–2876. [Google Scholar] [CrossRef] [PubMed]
- Hoffman, K.B.; Kraus, C.; Dimbil, M.; Golomb, B.A. A survey of the FDA’s AERS database regarding muscle and tendon adverse events linked to the statin drug class. PLoS ONE 2012, 7, e42866. [Google Scholar] [CrossRef] [PubMed]
- De Oliveira, L.P.; Vieira, C.P.; Guerra, F.D.; Almeida, M.S.; Pimentel, E.R. Structural and biomechanical changes in the achilles tendon after chronic treatment with statins. Food Chem. Toxicol. 2015, 77, 50–57. [Google Scholar] [CrossRef] [PubMed]
- Marie, I.; Delafenetre, H.; Massy, N.; Thuillez, C.; Noblet, C. Network of the French Pharmacovigilance Centers. Tendinous disorders attributed to statins: A study on ninety-six spontaneous reports in the period 1990–2005 and review of the literature. Arthritis Rheum. 2008, 59, 367–372. [Google Scholar] [CrossRef] [PubMed]
- Tsuzaki, M.; Guyton, G.; Garrett, W.; Archambault, J.M.; Herzog, W.; Almekinders, L.; Bynum, D.; Yang, X.; Banes, A.J. IL-1 beta induces COX2, MMP-1, -3 and -13, ADAMTS-4, IL-1 beta and IL-6 in human tendon cells. J. Orthop. Res. 2003, 21, 256–264. [Google Scholar] [CrossRef]
- John, T.; Lodka, D.; Kohl, B.; Ertel, W.; Jammrath, J.; Conrad, C.; Stoll, C.; Busch, C.; Schulze-Tanzil, G. Effect of pro-inflammatory and immunoregulatory cytokines on human tenocytes. J. Orthop. Res. 2010, 28, 1071–1077. [Google Scholar] [CrossRef] [PubMed]
- Niwa, S.; Totsuka, T.; Hayashi, S. Inhibitory effect of fluvastatin, an hmg-coa reductase inhibitor, on the expression of adhesion molecules on human monocyte cell line. Int. J. Immunopharmacol. 1996, 18, 669–675. [Google Scholar] [CrossRef]
- Kothe, H.; Dalhoff, K.; Rupp, J.; Muller, A.; Kreuzer, J.; Maass, M.; Katus, H.A. Hydroxymethylglutaryl coenzyme a reductase inhibitors modify the inflammatory response of human macrophages and endothelial cells infected with chlamydia pneumoniae. Circulation 2000, 101, 1760–1763. [Google Scholar] [CrossRef] [PubMed]
- Luan, Z.; Chase, A.J.; Newby, A.C. Statins inhibit secretion of metalloproteinases-1, -2, -3, and -9 from vascular smooth muscle cells and macrophages. Arterioscler. Thromb. Vasc. Biol. 2003, 23, 769–775. [Google Scholar] [CrossRef] [PubMed]
- Hast, M.W.; Zuskov, A.; Soslowsky, L.J. The role of animal models in tendon research. Bone Jt. Res. 2014, 3, 193–202. [Google Scholar] [CrossRef] [PubMed]
- Patterson-Kane, J.C.; Firth, E.C.; Parry, D.A.; Wilson, A.M.; Goodship, A.E. Effects of training on collagen fibril populations in the suspensory ligament and deep digital flexor tendon of young thoroughbreds. Am. J. Vet. Res. 1998, 59, 64–68. [Google Scholar] [PubMed]
- Rosso, F.; Bonasia, D.E.; Marmotti, A.; Cottino, U.; Rossi, R. Mechanical stimulation (pulsed electromagnetic fields “pemf” and extracorporeal shock wave therapy “eswt”) and tendon regeneration: A possible alternative. Front. Aging Neurosci. 2015, 7, 211. [Google Scholar] [CrossRef] [PubMed]
- Aspenberg, P. Stimulation of tendon repair: Mechanical loading, gdfs and platelets. A mini-review. Int. Orthop. 2007, 31, 783–789. [Google Scholar] [CrossRef] [PubMed]
- Ricchetti, E.T.; Reddy, S.C.; Ansorge, H.L.; Zgonis, M.H.; Van Kleunen, J.P.; Liechty, K.W.; Soslowsky, L.J.; Beredjiklian, P.K. Effect of interleukin-10 overexpression on the properties of healing tendon in a murine patellar tendon model. J. Hand Surg. Am. 2008, 33, 1843–1852. [Google Scholar] [CrossRef] [PubMed]
- Lichtnekert, J.; Kawakami, T.; Parks, W.C.; Duffield, J.S. Changes in macrophage phenotype as the immune response evolves. Curr. Opin. Pharmacol. 2013, 13, 555–564. [Google Scholar] [CrossRef] [PubMed]
- Jeong, Y.J.; Kim, I.; Cho, J.H.; Park, D.W.; Kwon, J.E.; Jung, M.W.; Meng, X.; Jo, S.M.; Song, H.S.; Cho, Y.M.; et al. Anti-osteoarthritic effects of the litsea japonica fruit in a rat model of osteoarthritis induced by monosodium iodoacetate. PLoS ONE 2015, 10, e0134856. [Google Scholar] [CrossRef] [PubMed]
- Xu, Y.; Liu, Q.; Liu, Z.L.; Lim, L.; Chen, W.H.; Lin, N. Treatment with simiaofang, an anti-arthritis chinese herbal formula, inhibits cartilage matrix degradation in osteoarthritis rat model. Rejuvenation Res. 2013, 16, 364–376. [Google Scholar] [CrossRef] [PubMed]








© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jeong, C.; Kim, S.E.; Shim, K.-S.; Kim, H.-J.; Song, M.H.; Park, K.; Song, H.-R. Exploring the In Vivo Anti-Inflammatory Actions of Simvastatin-Loaded Porous Microspheres on Inflamed Tenocytes in a Collagenase-Induced Animal Model of Achilles Tendinitis. Int. J. Mol. Sci. 2018, 19, 820. https://doi.org/10.3390/ijms19030820
Jeong C, Kim SE, Shim K-S, Kim H-J, Song MH, Park K, Song H-R. Exploring the In Vivo Anti-Inflammatory Actions of Simvastatin-Loaded Porous Microspheres on Inflamed Tenocytes in a Collagenase-Induced Animal Model of Achilles Tendinitis. International Journal of Molecular Sciences. 2018; 19(3):820. https://doi.org/10.3390/ijms19030820
Chicago/Turabian StyleJeong, Chandong, Sung Eun Kim, Kyu-Sik Shim, Hak-Jun Kim, Mi Hyun Song, Kyeongsoon Park, and Hae-Ryong Song. 2018. "Exploring the In Vivo Anti-Inflammatory Actions of Simvastatin-Loaded Porous Microspheres on Inflamed Tenocytes in a Collagenase-Induced Animal Model of Achilles Tendinitis" International Journal of Molecular Sciences 19, no. 3: 820. https://doi.org/10.3390/ijms19030820