Metabolomic Approach in STEMI-Patients Undergoing Left Ventricular Remodeling

 , ,
, ,
Abstract
:1. Introduction
2. Results
2.1. Baseline Characteristics
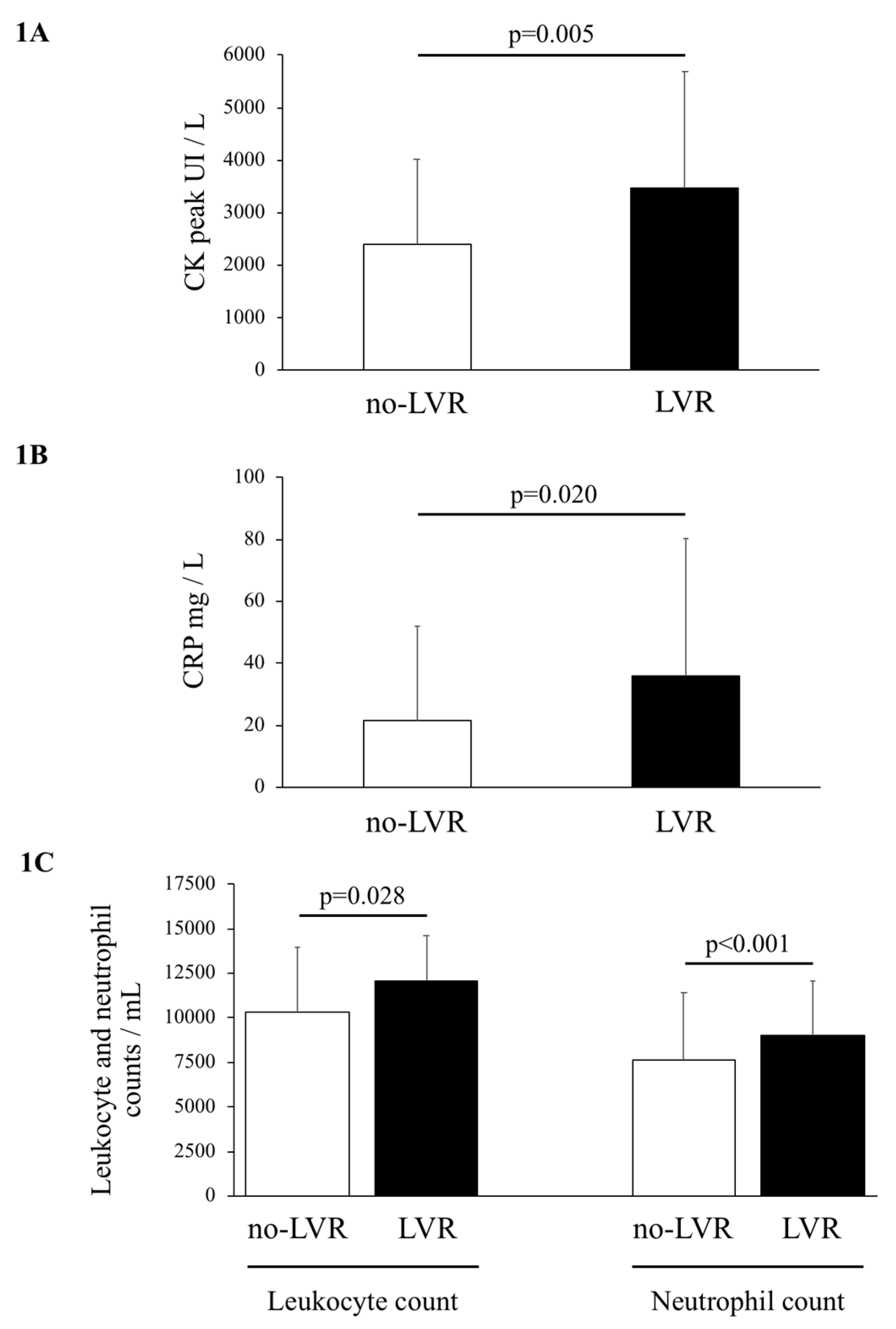
2.2. Creatine Kinase Peak and Inflammatory Biomarkers
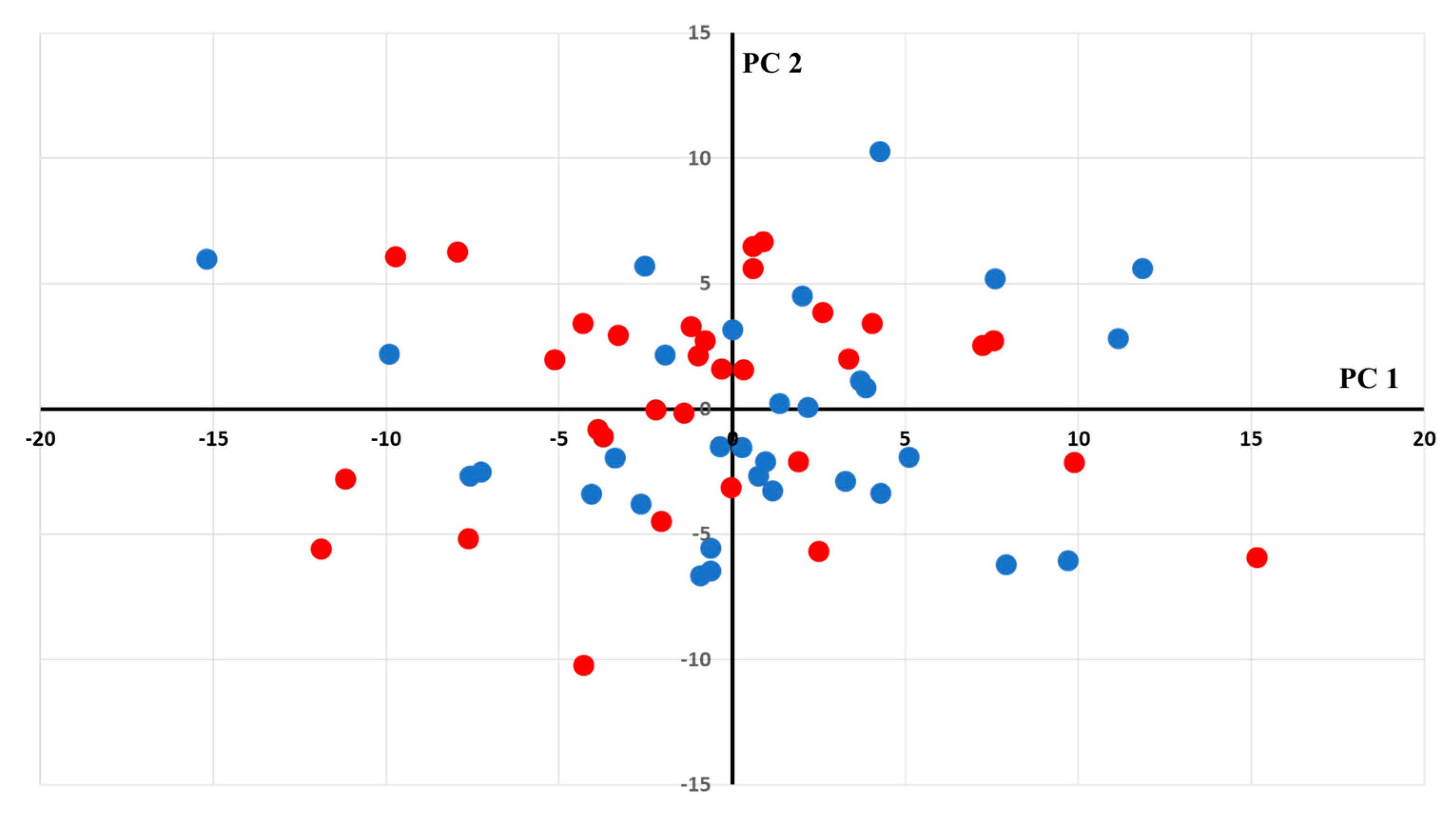
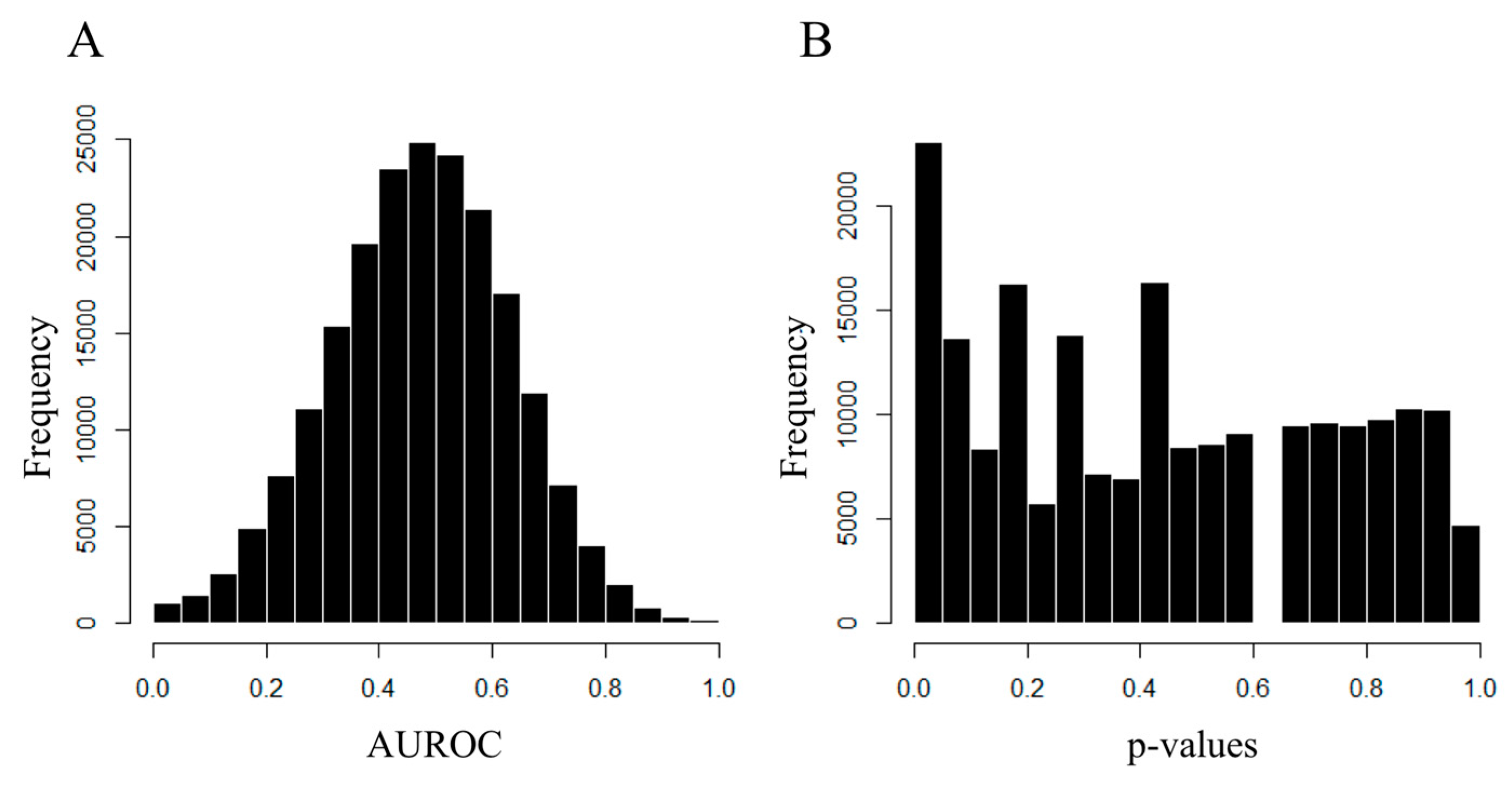
2.3. Metabolomic Analysis
3. Discussion
4. Material and Methods
4.1. Study Population
4.2. CMR Data
4.2.1. CMR Protocol
4.2.2. Image Analysis
4.3. Biomarkers
4.3.1. Metabolomics
4.3.2. Other Biomarkers
4.4. Statistical Analysis
4.4.1. Biomarker Analysis
4.4.2. Metabolomic Analysis
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Galli, A.; Lombardi, F. Postinfarct Left Ventricular Remodelling: A Prevailing Cause of Heart Failure. Cardiol. Res. Pract. 2016, 2016, 2579832. [Google Scholar] [CrossRef] [PubMed]
- Fertin, M.; Dubois, E.; Belliard, A.; Amouyel, P.; Pinet, F.; Bauters, C. Usefulness of circulating biomarkers for the prediction of left ventricular remodeling after myocardial infarction. Am. J. Cardiol. 2012, 110, 277–283. [Google Scholar] [CrossRef] [PubMed]
- Dunn, W.B.; Bailey, N.J.C.; Johnson, H.E. Measuring the metabolome: Current analytical technologies. Analyst 2005, 130, 606–625. [Google Scholar] [CrossRef] [PubMed]
- Barallobre-Barreiro, J.; Chung, Y.-L.; Mayr, M. Proteomics and metabolomics for mechanistic insights and biomarker discovery in cardiovascular disease. Rev. Esp. Cardiol. Engl. Ed. 2013, 66, 657–661. [Google Scholar] [CrossRef] [PubMed]
- Cheng, M.-L.; Wang, C.-H.; Shiao, M.-S.; Liu, M.-H.; Huang, Y.-Y.; Huang, C.-Y.; Mao, C.T.; Lin, J.F.; Ho, H.Y.; Yang, N.I. Metabolic disturbances identified in plasma are associated with outcomes in patients with heart failure: Diagnostic and prognostic value of metabolomics. J. Am. Coll. Cardiol. 2015, 65, 1509–1520. [Google Scholar] [CrossRef] [PubMed]
- Reinstadler, S.J.; Feistritzer, H.-J.; Reindl, M.; Klug, G.; Mayr, A.; Mair, J.; Jaschke, W.; Metzler, B. Combined biomarker testing for the prediction of left ventricular remodelling in ST-elevation myocardial infarction. Open Heart 2016, 3, e000485. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Farah, E.; Cogni, A.L.; Minicucci, M.F.; Azevedo, P.S.; Okoshi, K.; Matsubara, B.B.; Zanati, S.G.; Haggeman, R.; Paiva, S.A.; Zornoff, L.A. Prevalence and predictors of ventricular remodeling after anterior myocardial infarction in the era of modern medical therapy. Med. Sci. Monit. Int. Med. J. Exp. Clin. Res. 2012, 18, CR276–CR281. [Google Scholar] [CrossRef] [Green Version]
- Choi, H.; Yoo, B.-S.; Doh, J.-H.; Yooh, H.-J.; Ahn, M.-S.; Kim, J.-Y.; Lee, S.H.; Yoon, J. The optimal time of B-type natriuretic peptide sampling associated with post-myocardial infarction remodelling after primary percutaneous coronary intervention. Cardiovasc. J. Afr. 2013, 24, 165–170. [Google Scholar] [CrossRef]
- Siva Sankara, C.; Rajasekhar, D.; Vanajakshamma, V.; Praveen Kumar, B.S.; Vamsidhar, A. Prognostic significance of NT-proBNP, 3D LA volume and LV dyssynchrony in patients with acute STEMI undergoing primary percutaneous intervention. Indian Heart J. 2015, 67, 318–327. [Google Scholar] [CrossRef] [Green Version]
- Swiatkiewicz, I.; Kozinski, M.; Magielski, P.; Fabiszak, T.; Sukiennik, A.; Navarese, E.P.; Odrowaz-Sypniewska, G.; Kubica, J. Value of C-reactive protein in predicting left ventricular remodelling in patients with a first ST-segment elevation myocardial infarction. Mediat. Inflamm. 2012, 2012, 250867. [Google Scholar] [CrossRef]
- Bauters, A.; Ennezat, P.V.; Tricot, O.; Lallemant, R.; Aumégeat, V.; Segrestin, B.; Quandalle, P.; Lamblin, N.; Bauters, C.; REVE Investigators. Relation of admission white blood cell count to left ventricular remodeling after anterior wall acute myocardial infarction. Am. J. Cardiol. 2007, 100, 182–184. [Google Scholar] [CrossRef] [PubMed]
- Djordjevic-Radojkovic, D.; Koracevic, G.; Stanojevic, D.; Damjanovic, M.; Apostolovic, S.; Pavlovic, M. Stress hyperglycemia in acute ST-segment elevation myocardial infarction is a marker of left ventricular remodeling. Acute Card. Care 2013, 15, 38–43. [Google Scholar] [CrossRef] [PubMed]
- PubMed Entry. Available online: http://www.ncbi.nlm.nih.gov/pubmed/26337652 (accessed on 5 June 2018).
- Buono, F.; Spinelli, L.; Giallauria, F.; Assante di Panzillo, E.; Di Marino, S.; Ferrara, F.; Vigorito, C.; Trimarco, B.; Morisco, C. Usefulness of satisfactory control of low-density lipoprotein cholesterol to predict left ventricular remodeling after a first ST-elevation myocardial infarction successfully reperfused. Am. J. Cardiol. 2011, 107, 1772–1778. [Google Scholar] [CrossRef] [PubMed]
- Fertin, M.; Beseme, O.; Duban, S.; Amouyel, P.; Bauters, C.; Pinet, F. Deep plasma proteomic analysis of patients with left ventricular remodeling after a first myocardial infarction. Proteom. Clin. Appl. 2010, 4, 654–673. [Google Scholar] [CrossRef]
- Zhu, W.; Gregory, J.C.; Org, E.; Buffa, J.A.; Gupta, N.; Wang, Z.; Li, L.; Fu, X.; Wu, Y.; Mehrabian, M.; et al. Gut Microbial Metabolite TMAO Enhances Platelet Hyperreactivity and Thrombosis Risk. Cell 2016, 165, 111–124. [Google Scholar] [CrossRef] [PubMed]
- Lewis, G.D.; Wei, R.; Liu, E.; Yang, E.; Shi, X.; Martinovic, M.; Farrell, L.; Asnani, A.; Cyrille, M.; Ramanathan, A.; et al. Metabolite profiling of blood from individuals undergoing planned myocardial infarction reveals early markers of myocardial injury. J. Clin. Investig. 2008, 118, 3503–3512. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, L.; Song, J.; Hu, S. Metabolic remodeling of substrate utilization during heart failure progression. Heart Fail. Rev. 2018, 24, 143–154. [Google Scholar] [CrossRef] [PubMed]
- Anzai, T. Post-infarction inflammation and left ventricular remodeling: A double-edged sword. Circ. J. 2013, 77, 580–587. [Google Scholar] [CrossRef] [PubMed]
- Organ, C.L.; Otsuka, H.; Bhushan, S.; Wang, Z.; Bradley, J.; Trivedi, R.; Polhemus, D.J.; Tang, W.W.; Wu, Y.; Hazen, S.L.; et al. Choline Diet and Its Gut Microbe-Derived Metabolite, Trimethylamine N-Oxide, Exacerbate Pressure Overload-Induced Heart Failure. Circ. Heart Fail. 2016, 9, e002314. [Google Scholar] [CrossRef]
- Lorin, J.; Guilland, J.-C.; Stamboul, K.; Guenancia, C.; Cottin, Y.; Rochette, L.; Vergely, C.; Zeller, M. Increased Symmetric Dimethylarginine Level Is Associated with Worse Hospital Outcomes through Altered Left Ventricular Ejection Fraction in Patients with Acute Myocardial Infarction. PLoS ONE 2017, 12, e0169979. [Google Scholar] [CrossRef]
- Kiechl, S.; Lee, T.; Santer, P.; Thompson, G.; Tsimikas, S.; Egger, G.; Holt, D.W.; Willeit, J.; Xu, Q.; Mayr, M. Asymmetric and symmetric dimethylarginines are of similar predictive value for cardiovascular risk in the general population. Atherosclerosis 2009, 205, 261–265. [Google Scholar] [CrossRef] [PubMed]
- Potočnjak, I.; Radulović, B.; Degoricija, V.; Trbušić, M.; Pregartner, G.; Berghold, A.; Meinitzer, A.; Frank, S. Serum concentrations of asymmetric and symmetric dimethylarginine are associated with mortality in acute heart failure patients. Int. J. Cardiol. 2018, 261, 109–113. [Google Scholar] [CrossRef] [PubMed]
- Bière, L.; Donal, E.; Terrien, G.; Kervio, G.; Willoteaux, S.; Furber, A.; Prunier, F. Longitudinal strain is a marker of microvascular obstruction and infarct size in patients with acute ST-segment elevation myocardial infarction. PLoS ONE 2014, 9, e86959. [Google Scholar] [CrossRef] [PubMed]
- Bière, L.; Donal, E.; Jacquier, A.; Croisille, P.; Genée, O.; Christiaens, L.; Prunier, F.; Gueret, P.; Boyer, L.; Furber, A. A new look at left ventricular remodeling definition by cardiac imaging. Int. J. Cardiol. 2016, 209, 17–19. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Baseline Characteristics | Total n = 64 | No-LVR n = 32 | LVR n = 32 | p Value |
|---|---|---|---|---|
| Anthropometry | ||||
| Male sex | 52 (81%) | 26 (81%) | 26 (81%) | 1.00 |
| Age, years | 58 ± 9 | 59 ± 8 | 58 ± 9 | 0.56 |
| Body mass index, kg/m² | 27 ± 4 | 27 ± 4 | 28 ± 3 | 0.17 |
| Cardiovascular Risk Factors | ||||
| Hypertension | 26 (41%) | 8 (25%) | 18 (56%) | 0.010 |
| Diabetes mellitus | 9 (14%) | 3 (9%) | 6 (19%) | 0.29 |
| Hypercholesterolemia | 34 (53%) | 16 (50%) | 18 (56%) | 0.62 |
| Current smoker | 29 (45%) | 12 (38%) | 17 (53%) | 0.22 |
| STEMI Characteristics | ||||
| Anterior infarction | 34 (53%) | 17 (53%) | 17 (53%) | 1.00 |
| Thrombectomy | 31 (48%) | 12 (38%) | 19 (59%) | 0.082 |
| Complete revascularization | 38 (59%) | 19 (59%) | 19 (59%) | 1.00 |
| Time to reperfusion (min) | 293 ± 130 | 280 ± 117 | 307 ± 140 | 0.39 |
| In-hospital heart failure | 10 (16%) | 2 (6%) | 8 (25%) | 0.041 |
| Thrombolysis | 14 (22%) | 5 (16%) | 9 (28%) | 0.36 |
| GPIIb/IIIa inhibitors | 15 (23%) | 8 (25%) | 7 (22%) | 0.77 |
| Pharmaceutical Treatment at Discharge | ||||
| β-blockers | 61 (95%) | 31 (97%) | 30 (94%) | 0.56 |
| ACE inhibitors | 62 (97%) | 32 (100%) | 30 (94%) | 0.16 |
| Anti-aldosterone | 25 (39%) | 11 (34%) | 14 (44%) | 0.45 |
| CMR Data | Total n = 64 | No-LVR n = 32 | LVR n = 32 | p Value |
|---|---|---|---|---|
| Baseline CMR | ||||
| LVEDV index, mL/m2 | 93.0 ± 18.9 | 94.7 ± 14.8 | 91.3 ± 22.4 | 0.48 |
| LVESV index, mL/m2 | 48.2 ± 15.0 | 49.6 ± 12.2 | 46.8 ± 17.5 | 0.46 |
| LVEF, % | 48.2 ± 9.5 | 47.7 ± 9.0 | 48.6 ± 10.1 | 0.73 |
| LV mass index, g/m2 | 59.2 ± 11.7 | 57.7 ± 8.5 | 60.7 ± 14.2 | 0.31 |
| Infarct size, % LV | 18.0 ± 12.5 | 15.8 ± 10.0 | 20.0 ± 14.4 | 0.19 |
| 3 Months CMR | ||||
| LVEDV index, mL/m2 | 94.1 ± 21.7 | 88.8 ± 16.2 | 99.3 ± 25.2 | 0.054 |
| LVESV index, mL/m2 | 47.6 ± 19.0 | 42.1 ± 13.5 | 53.1 ± 22.1 | 0.019 |
| LVEF, % | 50.9 ± 9.8 | 53.1 ± 8.6 | 48.6 ± 10.4 | 0.064 |
| LV mass index, g/m2 | 54.4 ± 10.5 | 53.2 ± 8.5 | 54.6 ± 12.2 | 0.60 |
| Infarct size, % LV | 16.4 ± 11.2 | 14.2 ± 9.4 | 17.3 ± 12 | 0.25 |
| 1 Year CMR | ||||
| LVEDV index, mL/m2 | 96.4 ± 25.1 | 86.6 ± 17.9 | 106.2 ± 27.6 | 0.001 |
| LVESV index, mL/m2 | 49.0 ± 21.8 | 40.9 ± 14.5 | 57.2 ± 25.0 | 0.002 |
| LVEF, % | 50.4 ± 9.8 | 53.5 ± 8.9 | 47.3 ± 9.9 | 0.011 |
| LV mass index, g/m2 | 52.3 ± 11.5 | 50.0 ± 8.9 | 54.6 ± 13.4 | 0.11 |
| Infarct size, % LV | 14.8 ± 8.9 | 13.0 ± 7.7 | 15.6 ± 10.2 | 0.25 |
| Biomarkers | Total n = 64 | No-LVR n = 32 | LVR n = 32 | p Value |
|---|---|---|---|---|
| NT-proBNP, ng/L | 1610 ± 1762 | 1375 ± 1630 | 1844 ± 1882 | 0.23 |
| High-sensitive cardiac troponin I, ng/L | 59,669 ± 80,127 | 43,557 ± 46,803 | 75,782 ± 101,594 | 0.26 |
| Creatine kinase, UI/L | 708 ± 791 | 566 ± 596 | 850 ± 935 | 0.27 |
| Creatine kinase peak, UI/L | 2930 ± 1995 | 2394 ± 1615 | 3466 ± 2211 | 0.005 |
| CRP, mg/L | 28.8 ± 38.3 | 21.7 ± 30.4 | 35.9 ± 44.3 | 0.020 |
| Leukocyte count, /mL | 11,187 ± 3240 | 10,346 ± 3626 | 12,028 ± 2593 | 0.028 |
| Neutrophil count, /mL | 8341 ± 3482 | 7596 ± 3822 | 9035 ± 3036 | <0.001 |
| Creatinine, µmol/L | 73.5 ± 14.8 | 72.2 ± 15.3 | 74.8 ± 14.3 | 0.41 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Garcia, G.; Chao de la Barca, J.M.; Mirebeau-Prunier, D.; Reynier, P.; Furber, A.; Prunier, F.; Bière, L. Metabolomic Approach in STEMI-Patients Undergoing Left Ventricular Remodeling. Int. J. Mol. Sci. 2019, 20, 289. https://doi.org/10.3390/ijms20020289
Garcia G, Chao de la Barca JM, Mirebeau-Prunier D, Reynier P, Furber A, Prunier F, Bière L. Metabolomic Approach in STEMI-Patients Undergoing Left Ventricular Remodeling. International Journal of Molecular Sciences. 2019; 20(2):289. https://doi.org/10.3390/ijms20020289
Chicago/Turabian StyleGarcia, Gabriel, Juan Manuel Chao de la Barca, Delphine Mirebeau-Prunier, Pascal Reynier, Alain Furber, Fabrice Prunier, and Loïc Bière. 2019. "Metabolomic Approach in STEMI-Patients Undergoing Left Ventricular Remodeling" International Journal of Molecular Sciences 20, no. 2: 289. https://doi.org/10.3390/ijms20020289