The Prognostic Impact of the Aryl Hydrocarbon Receptor (AhR) in Primary Breast Cancer Depends on the Lymph Node Status

 ,
,
Abstract
:1. Introduction
2. Results
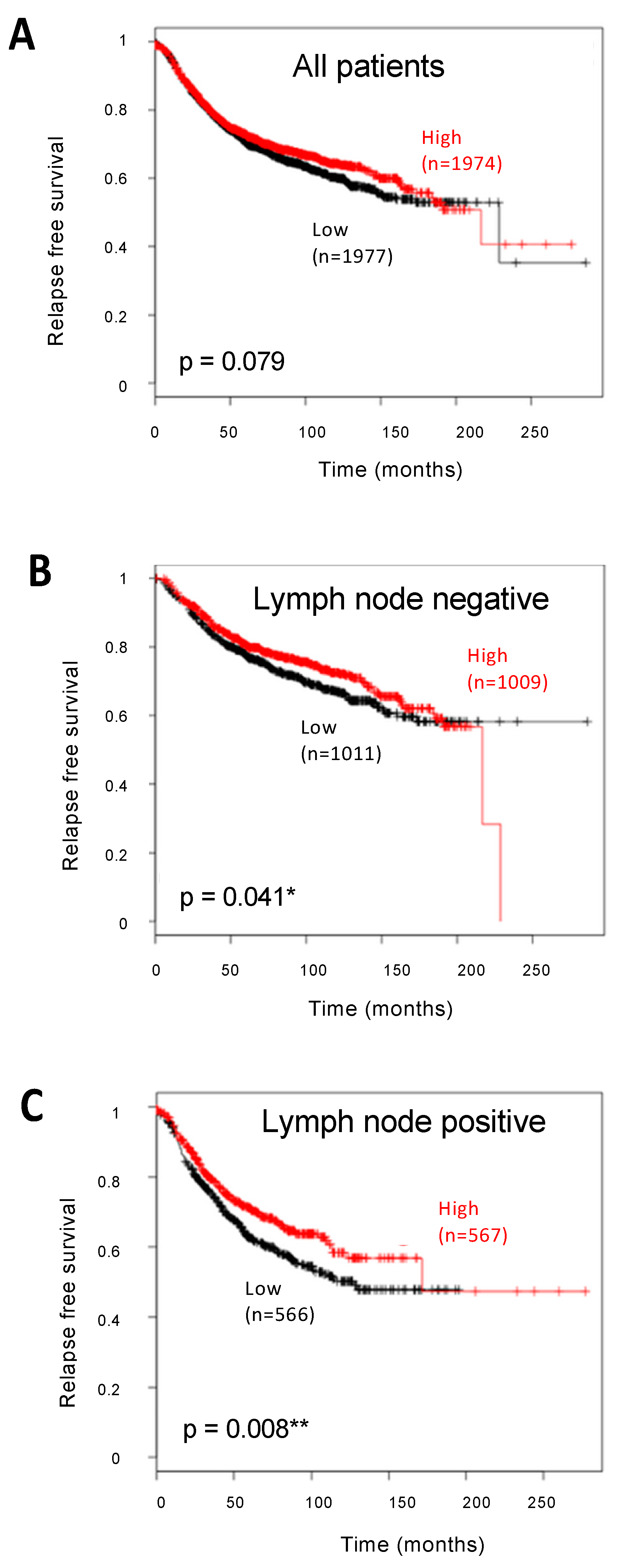
2.1. Analysis of AhR Expression in BC at the mRNA Level
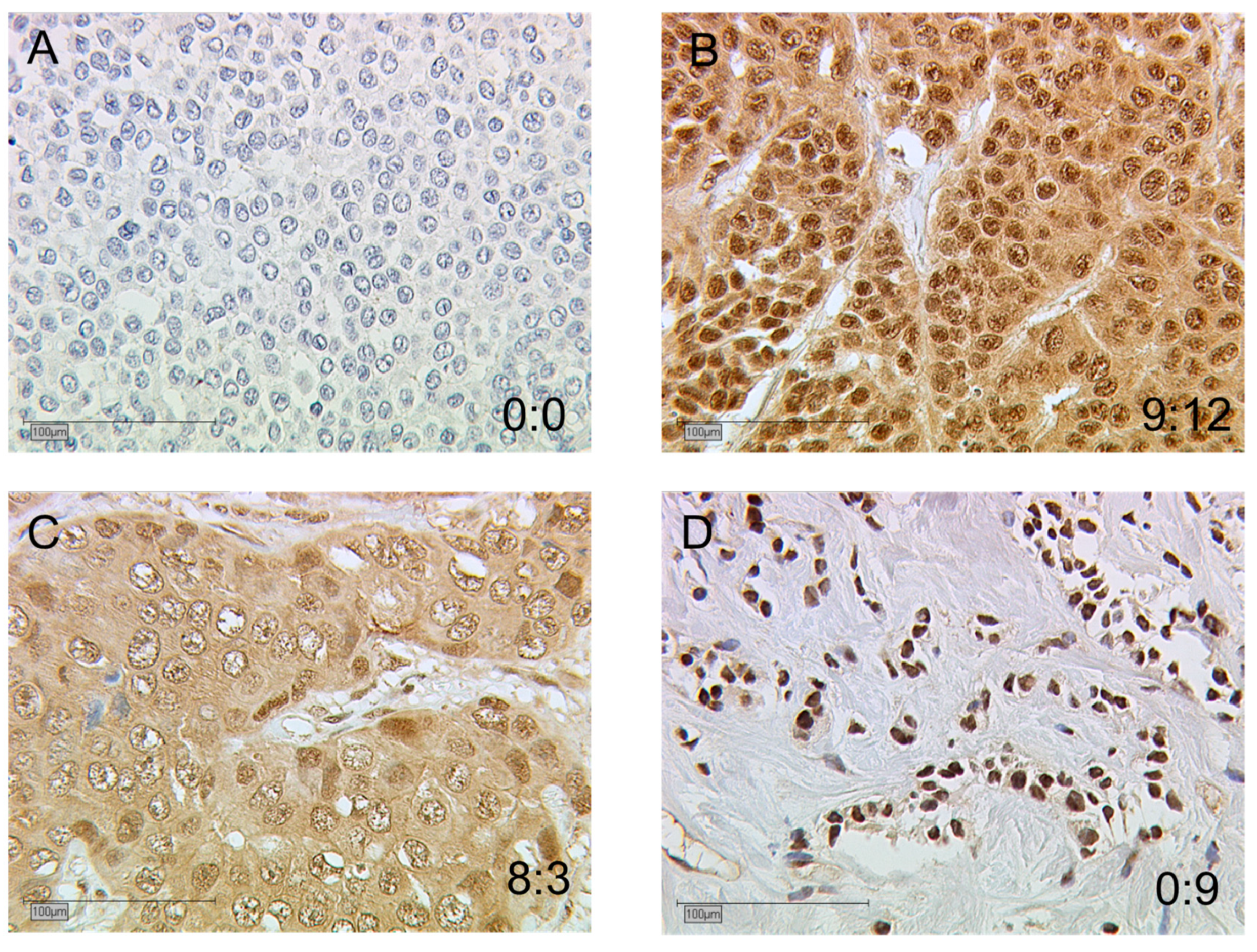
2.2. Immunodetection of AhR in BC
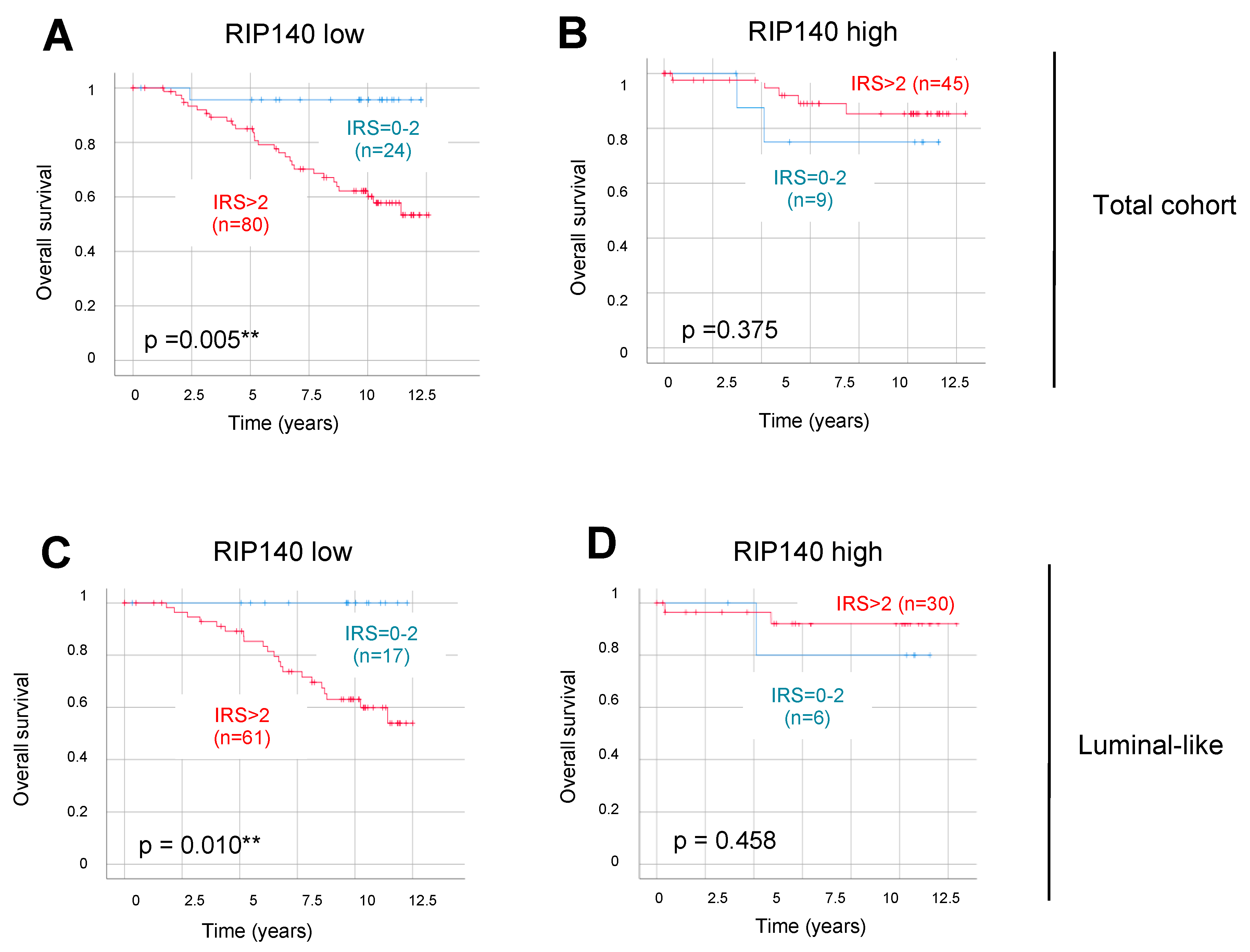
2.3. Analysis of the Correlation between AhR Expression and Clinicopathological Characteristics and RIP140 Expression
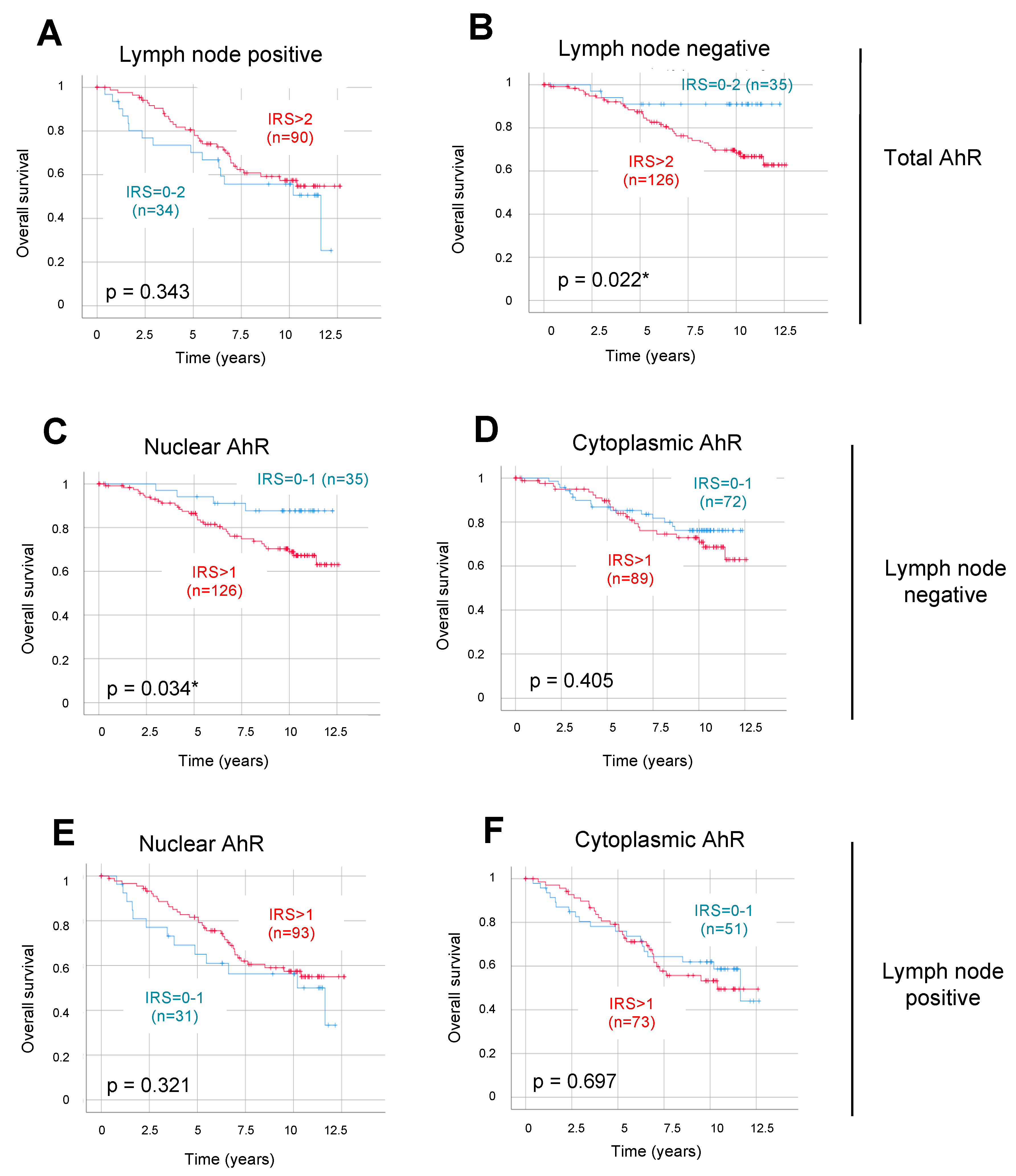
2.4. AhR Expression as an Independent Prognostic Parameter in LN-Negative Tumors
3. Discussion
4. Materials and Methods
4.1. Correlation of Gene Expression with Patient Survival
4.2. Collective
4.3. Immunohistochemistry
4.4. Data Analysis
4.5. Statistical and Survival Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| AhR | Aryl hydrocarbon receptor |
| ARNT | AhR nuclear transporter |
| BC | breast cancer |
| DFS | disease free survival |
| EMT | epithelial mesenchymal transition |
| ER | estrogen receptor |
| FISH | fluorescence in situ hybridization |
| HER2 | human epidermal growth factor receptor 2 |
| IRS | immunoreactive score |
| LCoR | ligand dependent corepressor |
| LMU | Ludwig Maximilians University |
| LN | lymph node |
| NCAD | N-Cadherin |
| NST | non-special type |
| OS | overall survival |
| PBS | phosphate buffered saline |
| pN | primary tumor node |
| PR | progesterone receptor |
| pT | primary tumor size |
| RAR | retinoic acid receptor |
| ROC curve | receiver operating characteristic curve |
| RIP140 | receptor interacting protein of 140 kDa |
| RXR | retinoid X receptor |
| THR | thyroid hormone receptor |
| TNM status | tumor node metastasis status |
| TNBC | triple-negative breast cancer |
| VDR | vitamin D receptor |
References
- Global Burden of Disease Cancer, Collaboration; Fitzmaurice, C.; Allen, C.; Barber, R.M.; Barregard, L.; Bhutta, Z.A.; Brenner, H.; Dicker, D.J.; Chimed-Orchir, O.; Dandona, R.; et al. Global, Regional, and National Cancer Incidence, Mortality, Years of Life Lost, Years Lived with Disability, and Disability-Adjusted Life-Years for 32 Cancer Groups, 1990 to 2015: A Systematic Analysis for the Global Burden of Disease Study. JAMA Oncol. 2017, 3, 524–548. [Google Scholar] [PubMed]
- Duffy, M.J.; Harbeck, N.; Nap, M.; Molina, R.; Nicolini, A.; Senkus, E.; Cardoso, F. Clinical Use of Biomarkers in Breast Cancer: Updated Guidelines from the European Group on Tumor Markers (Egtm). Eur. J. Cancer 2017, 75, 284–298. [Google Scholar] [CrossRef] [PubMed]
- Murray, I.A.; Patterson, A.D.; Perdew, G.H. Aryl Hydrocarbon Receptor Ligands in Cancer: Friend and Foe. Nat. Rev. Cancer 2014, 14, 801–814. [Google Scholar] [CrossRef] [PubMed]
- Bersten, D.C.; Sullivan, A.E.; Peet, D.J.; Whitelaw, M.L. Bhlh-Pas Proteins in Cancer. Nat. Rev. Cancer 2013, 13, 827–841. [Google Scholar] [CrossRef] [PubMed]
- Dietrich, C. Antioxidant Functions of the Aryl Hydrocarbon Receptor. Stem Cells Int. 2016, 2016, 7943495. [Google Scholar] [CrossRef] [PubMed]
- Kumar, M.B.; Tarpey, R.W.; Perdew, G.H. Differential Recruitment of Coactivator Rip140 by Ah and Estrogen Receptors. Absence of a Role for Lxxll Motifs. J. Biol. Chem. 1999, 274, 22155–22164. [Google Scholar] [CrossRef] [PubMed]
- Augereau, P.; Badia, E.; Fuentes, M.; Rabenoelina, F.; Corniou, M.; Derocq, D.; Balaguer, P.; Cavailles, V. Transcriptional Regulation of the Human Nrip1/Rip140 Gene by Estrogen Is Modulated by Dioxin Signalling. Mol. Pharmacol. 2006, 69, 1338–1346. [Google Scholar] [CrossRef] [PubMed]
- Kolluri, S.K.; Jin, U.H.; Safe, S. Role of the Aryl Hydrocarbon Receptor in Carcinogenesis and Potential as an Anti-Cancer Drug Target. Arch. Toxicol. 2017, 91, 2497–2513. [Google Scholar] [CrossRef] [PubMed]
- Barhoover, M.A.; Hall, J.M.; Greenlee, W.F.; Thomas, R.S. Aryl Hydrocarbon Receptor Regulates Cell Cycle Progression in Human Breast Cancer Cells Via a Functional Interaction with Cyclin-Dependent Kinase 4. Mol. Pharmacol. 2010, 77, 195–201. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.D.; Wang, K.; Yang, X.W.; Zhuang, Z.G.; Wang, J.J.; Tong, X.W. Expression of Aryl Hydrocarbon Receptor in Relation to P53 Status and Clinicopathological Parameters in Breast Cancer. Int. J. Clin. Exp. Pathol. 2014, 7, 7931–7937. [Google Scholar] [PubMed]
- Vacher, S.; Castagnet, P.; Chemlali, W.; Lallemand, F.; Meseure, D.; Pocard, M.; Bieche, I.; Perrot-Applanat, M. High Ahr Expression in Breast Tumors Correlates with Expression of Genes from Several Signaling Pathways Namely Inflammation and Endogenous Tryptophan Metabolism. PLoS ONE 2018, 13, e0190619. [Google Scholar]
- O’Donnell, E.F.; Koch, D.C.; Bisson, W.H.; Jang, H.S.; Kolluri, S.K. The Aryl Hydrocarbon Receptor Mediates Raloxifene-Induced Apoptosis in Estrogen Receptor-Negative Hepatoma and Breast Cancer Cells. Cell Death Dis. 2014, 5, e1038. [Google Scholar] [CrossRef] [PubMed]
- Powell, J.B.; Goode, G.D.; Eltom, S.E. The Aryl Hydrocarbon Receptor: A Target for Breast Cancer Therapy. J. Cancer Ther. 2013, 4, 1177–1186. [Google Scholar] [CrossRef] [PubMed]
- Bock, C.; Kuhn, C.; Ditsch, N.; Krebold, R.; Heublein, S.; Mayr, D.; Doisneau-Sixou, S.; Jeschke, U. Strong Correlation between N-Cadherin and Cd133 in Breast Cancer: Role of Both Markers in Metastatic Events. J. Cancer Res. Clin. Oncol. 2014, 140, 1873–1881. [Google Scholar] [CrossRef] [PubMed]
- Ditsch, N.; Mayr, D.; Lenhard, M.; Strauss, C.; Vodermaier, A.; Gallwas, J.; Stoeckl, D.; Graeser, M.; Weissenbacher, T.; Friese, K.; et al. Correlation of Thyroid Hormone, Retinoid X, Peroxisome Proliferator-Activated, Vitamin D and Oestrogen/Progesterone Receptors in Breast Carcinoma. Oncol. Lett. 2012, 4, 665–671. [Google Scholar] [CrossRef] [PubMed]
- Ditsch, N.; Toth, B.; Himsl, I.; Lenhard, M.; Ochsenkuhn, R.; Friese, K.; Mayr, D.; Jeschke, U. Thyroid Hormone Receptor (Tr)Alpha and Trbeta Expression in Breast Cancer. Histol. Histopathol. 2013, 28, 227–237. [Google Scholar] [PubMed]
- Sixou, S.; Muller, K.; Jalaguier, S.; Kuhn, C.; Harbeck, N.; Mayr, D.; Engel, J.; Jeschke, U.; Ditsch, N.; Cavailles, V. Importance of Rip140 and Lcor Sub-Cellular Localization for Their Association with Breast Cancer Aggressiveness and Patient Survival. Transl. Oncol. 2018, 11, 1090–1096. [Google Scholar] [CrossRef] [PubMed]
- Remmele, W.; Stegner, H.E. Recommendation for Uniform Definition of an Immunoreactive Score (Irs) for Immunohistochemical Estrogen Receptor Detection (Er-Ica) in Breast Cancer Tissue. Pathologe 1987, 8, 138–140. [Google Scholar] [PubMed]
- Saito, R.; Miki, Y.; Hata, S.; Takagi, K.; Iida, S.; Oba, Y.; Ono, K.; Ishida, T.; Suzuki, T.; Ohuchi, N.; et al. Aryl Hydrocarbon Receptor in Breast Cancer-a Newly Defined Prognostic Marker. Horm. Cancer 2014, 5, 11–21. [Google Scholar] [CrossRef] [PubMed]
- Trombino, A.F.; Near, R.I.; Matulka, R.A.; Yang, S.; Hafer, L.J.; Toselli, P.A.; Kim, D.W.; Rogers, A.E.; Sonenshein, G.E.; Sherr, D.H. Expression of the Aryl Hydrocarbon Receptor/Transcription Factor (Ahr) and Ahr-Regulated Cyp1 Gene Transcripts in a Rat Model of Mammary Tumorigenesis. Breast Cancer Res. Treat. 2000, 63, 117–131. [Google Scholar] [CrossRef] [PubMed]
- Ikuta, T.; Eguchi, H.; Tachibana, T.; Yoneda, Y.; Kawajiri, K. Nuclear Localization and Export Signals of the Human Aryl Hydrocarbon Receptor. J. Biol. Chem. 1998, 273, 2895–2904. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ikuta, T.; Tachibana, T.; Watanabe, J.; Yoshida, M.; Yoneda, Y.; Kawajiri, K. Nucleocytoplasmic Shuttling of the Aryl Hydrocarbon Receptor. J. Biochem. 2000, 127, 503–509. [Google Scholar] [CrossRef] [PubMed]
- Ikuta, T.; Watanabe, J.; Kawajiri, K. Characterization of the Lxxll Motif in the Aryl Hydrocarbon Receptor: Effects on Subcellular Localization and Transcriptional Activity. J. Biochem. 2002, 131, 79–85. [Google Scholar] [CrossRef] [PubMed]
- Mandl, M.; Lieberum, M.; Dunst, J.; Depping, R. The Expression Level of the Transcription Factor Aryl Hydrocarbon Receptor Nuclear Translocator (Arnt) Determines Cellular Survival after Radiation Treatment. Radiat. Oncol. 2015, 10, 229. [Google Scholar] [CrossRef] [PubMed]
- Luecke-Johansson, S.; Gralla, M.; Rundqvist, H.; Ho, J.C.; Johnson, R.S.; Gradin, K.; Poellinger, L. A Molecular Mechanism to Switch the Aryl Hydrocarbon Receptor from a Transcription Factor to an E3 Ubiquitin Ligase. Mol. Cell Biol. 2017, 37, e00630-16. [Google Scholar] [CrossRef] [PubMed]
- Li, C.H.; Liu, C.W.; Tsai, C.H.; Peng, Y.J.; Yang, Y.H.; Liao, P.L.; Lee, C.C.; Cheng, Y.W.; Kang, J.J. Cytoplasmic Aryl Hydrocarbon Receptor Regulates Glycogen Synthase Kinase 3 Beta, Accelerates Vimentin Degradation, and Suppresses Epithelial-Mesenchymal Transition in Non-Small Cell Lung Cancer Cells. Arch. Toxicol. 2017, 91, 2165–2178. [Google Scholar] [CrossRef] [PubMed]
- Harbeck, N.; Alt, U.; Berger, U.; Kruger, A.; Thomssen, C.; Janicke, F.; Hofler, H.; Kates, R.E.; Schmitt, M. Prognostic Impact of Proteolytic Factors (Urokinase-Type Plasminogen Activator, Plasminogen Activator Inhibitor 1, and Cathepsins B, D, and L) in Primary Breast Cancer Reflects Effects of Adjuvant Systemic Therapy. Clin. Cancer Res. 2001, 7, 2757–2764. [Google Scholar] [PubMed]
- Madak-Erdogan, Z.; Katzenellenbogen, B.S. Aryl Hydrocarbon Receptor Modulation of Estrogen Receptor Alpha-Mediated Gene Regulation by a Multimeric Chromatin Complex Involving the Two Receptors and the Coregulator Rip140. Toxicol. Sci. 2012, 125, 401–411. [Google Scholar] [CrossRef] [PubMed]
- Henry, N.L.; Bedard, P.L.; DeMichele, A. Standard and Genomic Tools for Decision Support in Breast Cancer Treatment. Am. Soc. Clin. Oncol. Educ. Book 2017, 37, 106–115. [Google Scholar] [CrossRef] [PubMed]
- Schlezinger, J.J.; Liu, D.; Farago, M.; Seldin, D.C.; Belguise, K.; Sonenshein, G.E.; Sherr, D.H. A Role for the Aryl Hydrocarbon Receptor in Mammary Gland Tumorigenesis. Biol. Chem. 2006, 387, 1175–1187. [Google Scholar] [CrossRef] [PubMed]
- Gyorffy, B.; Lanczky, A.; Eklund, A.C.; Denkert, C.; Budczies, J.; Li, Q.; Szallasi, Z. An Online Survival Analysis Tool to Rapidly Assess the Effect of 22,277 Genes on Breast Cancer Prognosis Using Microarray Data of 1,809 Patients. Breast Cancer Res. Treat. 2010, 123, 725–731. [Google Scholar] [CrossRef] [PubMed]
- Madden, S.F.; Clarke, C.; Gaule, P.; Aherne, S.T.; O’Donovan, N.; Clynes, M.; Crown, J.; Gallagher, W.M. Breastmark: An Integrated Approach to Mining Publicly Available Transcriptomic Datasets Relating to Breast Cancer Outcome. Breast Cancer Res. 2013, 15, R52. [Google Scholar] [CrossRef] [PubMed]
- Elston, E.W.; Ellis, I.O. Method for Grading Breast Cancer. J. Clin. Pathol. 1993, 46, 189–190. [Google Scholar] [CrossRef] [PubMed]
- Weissenbacher, T.; Hirte, E.; Kuhn, C.; Janni, W.; Mayr, D.; Karsten, U.; Rack, B.; Friese, K.; Jeschke, U.; Heublein, S.; et al. Multicentric and Multifocal Versus Unifocal Breast Cancer: Differences in the Expression of E-Cadherin Suggest Differences in Tumor Biology. BMC Cancer 2013, 13, 361. [Google Scholar] [CrossRef] [PubMed]
- Mylonas, I.; Makovitzky, J.; Jeschke, U.; Briese, V.; Friese, K.; Gerber, B. Expression of Her2/Neu, Steroid Receptors (Er and Pr), Ki67 and P53 in Invasive Mammary Ductal Carcinoma Associated with Ductal Carcinoma in Situ (Dcis) Versus Invasive Breast Cancer Alone. Anticancer Res. 2005, 25, 1719–1723. [Google Scholar] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Clinical and Pathological Characteristics a | n = 302 b | % |
|---|---|---|
| ER status | ||
| Negative | 58 | 19.2 |
| Positive | 244 | 80.8 |
| PR status | ||
| Negative | 126 | 41.7 |
| Positive | 176 | 58.3 |
| HER2 status | ||
| Negative | 265 | 87.7 |
| Positive | 35 | 11.6 |
| Unknown | 2 | 0.7 |
| Triple negative | ||
| No | 264 | 87.4 |
| Yes | 36 | 11.9 |
| Unknown | 2 | 0.7 |
| Histologic type c | ||
| Invasive lobular | 40 | 13.2 |
| Invasive medullar | 11 | 3.6 |
| Invasive mucinous | 4 | 1.3 |
| No Special Type (NST) | 163 | 54 |
| DCIS (only or with NST) | 82 | 27.2 |
| Unknown | 2 | 0.7 |
| Tumor size | ||
| pT1 | 199 | 65.8 |
| pT2 | 87 | 28.8 |
| pT3 | 4 | 1.3 |
| pT4 | 11 | 3.6 |
| Unknown | 1 | 0.3 |
| Grade | ||
| I | 15 | 5 |
| II | 106 | 35.1 |
| III | 46 | 15.2 |
| Unknown | 135 | 44.7 |
| Lymph node status | ||
| Negative | 162 | 53.6 |
| Positive | 124 | 41.1 |
| Unknown | 16 | 5.3 |
| Local recurrence d | ||
| No | 251 | 83.1 |
| Yes | 40 | 13.2 |
| Unknown | 11 | 3.6 |
| Distant metastases d | ||
| No | 232 | 76.8 |
| Yes | 59 | 19.5 |
| Unknown | 11 | 3.6 |
| Whole Cohort (n = 302) | Lymph Node-Negative (n = 162) | Lymph Node-Positive (n = 124) | |
|---|---|---|---|
| Total AhR expression | |||
| Mean IRS +/− SE | 6.66 +/− 4.85 | 6 +/− 4.56 | 6.85 +/− 4.30 |
| Low expressing tumors n (%) | 27 (8.9%) | 12 (7.4%) | 15 (12.1%) |
| High expressing tumors n (%) | 275 (91.1%) | 150 (92.6%) | 109 (87.9%) |
| Nuclear AhR expression | |||
| Mean IRS +/− SE | 4.15 * +/− 2.92 | 4.10 * +/− 2.69 | 4.21 * +/− 2.52 |
| Low expressing tumors n (%) | 27 * (8.9%) | 12 * (7.4%) | 15 * (12.1%) |
| High expressing tumors n (%) | 275 * (91.1%) | 150 * (92.6%) | 109* (87.9%) |
| Cytoplasmic AhR expression | |||
| Mean IRS +/− SE | 2.51 * +/− 2.67 | 2.41 * +/− 2.64 | 2.65 *+/− 2.28 |
| Low expressing tumors n (%) | 125 * (41.4%) | 69 * (42.6%) | 57 *(46%) |
| High expressing tumors n (%) | 177 * (58.6%) | 93 * (57.4%) | 67 *(54%) |
| Correlation between nuclear and cytoplasmic AhR | |||
| Correlation coefficient | 0.539 *** | 0.476 *** | 0.618 *** |
| p values | 5.66 10−23 | 1.57 10−10 | 2.09 10−14 |
| Whole Cohort (n = 167–302) | Lymph Node-Negative (n = 91–162) | Lymph Node-Positive (n = 71–124) | |
|---|---|---|---|
| Age (diagnosis) | 0.027 | 0.091 | 0.006 |
| Histologic type | −0.061 | −0.122 | 0.043 |
| Tumor size | −0.055 | −0.045 | −0.059 |
| Grade | 0.055 | 0.029 | 0.052 |
| Local recurrence | −0.020 | −0.009 | −0.028 |
| Metastasis | −0.064 | −0.086 | −0.073 |
| Triple negative | −0.045 | −0.103 | 0.038 |
| ER | 0.024 | 0.047 | −0.010 |
| PR | 0.071 | 0.078 | 0.061 |
| HER2 | 0.010 | 0.079 | −0.016 |
| RIP140 | 0.284 *** | 0.256 ** | 0.309 *** |
| p Value | Hazard Ratio | |||||
|---|---|---|---|---|---|---|
| Whole Cohort | Lymph Node-Negative | Lymph Node-Positive | Whole Cohort | Lymph Node-Negative | Lymph Node-Positive | |
| Age | 0.000154 *** | 0.004 ** | 0.002 ** | 1.033 | 1.041 | 1.039 |
| Tumor size | 0.000001 *** | 0.061 | 0.005 ** | 1.479 | 1.345 | 1.348 |
| ER | 0.032 * | 0.064 | 0.043 * | 0.586 | 0.501 | 0.489 |
| HER2 | 0.026 * | 0.776 | 0.001 ** | 1.917 | 0.855 | 3.441 |
| Total AhR | 0.571 | 0.046* | 0.454 | 1.164 | 3.369 | 0.788 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jeschke, U.; Zhang, X.; Kuhn, C.; Jalaguier, S.; Colinge, J.; Pfender, K.; Mayr, D.; Ditsch, N.; Harbeck, N.; Mahner, S.; et al. The Prognostic Impact of the Aryl Hydrocarbon Receptor (AhR) in Primary Breast Cancer Depends on the Lymph Node Status. Int. J. Mol. Sci. 2019, 20, 1016. https://doi.org/10.3390/ijms20051016
Jeschke U, Zhang X, Kuhn C, Jalaguier S, Colinge J, Pfender K, Mayr D, Ditsch N, Harbeck N, Mahner S, et al. The Prognostic Impact of the Aryl Hydrocarbon Receptor (AhR) in Primary Breast Cancer Depends on the Lymph Node Status. International Journal of Molecular Sciences. 2019; 20(5):1016. https://doi.org/10.3390/ijms20051016
Chicago/Turabian StyleJeschke, Udo, Xi Zhang, Christina Kuhn, Stéphan Jalaguier, Jacques Colinge, Kristina Pfender, Doris Mayr, Nina Ditsch, Nadia Harbeck, Sven Mahner, and et al. 2019. "The Prognostic Impact of the Aryl Hydrocarbon Receptor (AhR) in Primary Breast Cancer Depends on the Lymph Node Status" International Journal of Molecular Sciences 20, no. 5: 1016. https://doi.org/10.3390/ijms20051016