Over-Expression of CHD4 Is an Independent Biomarker of Poor Prognosis in Patients with Rectal Cancers Receiving Concurrent Chemoradiotherapy

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Results
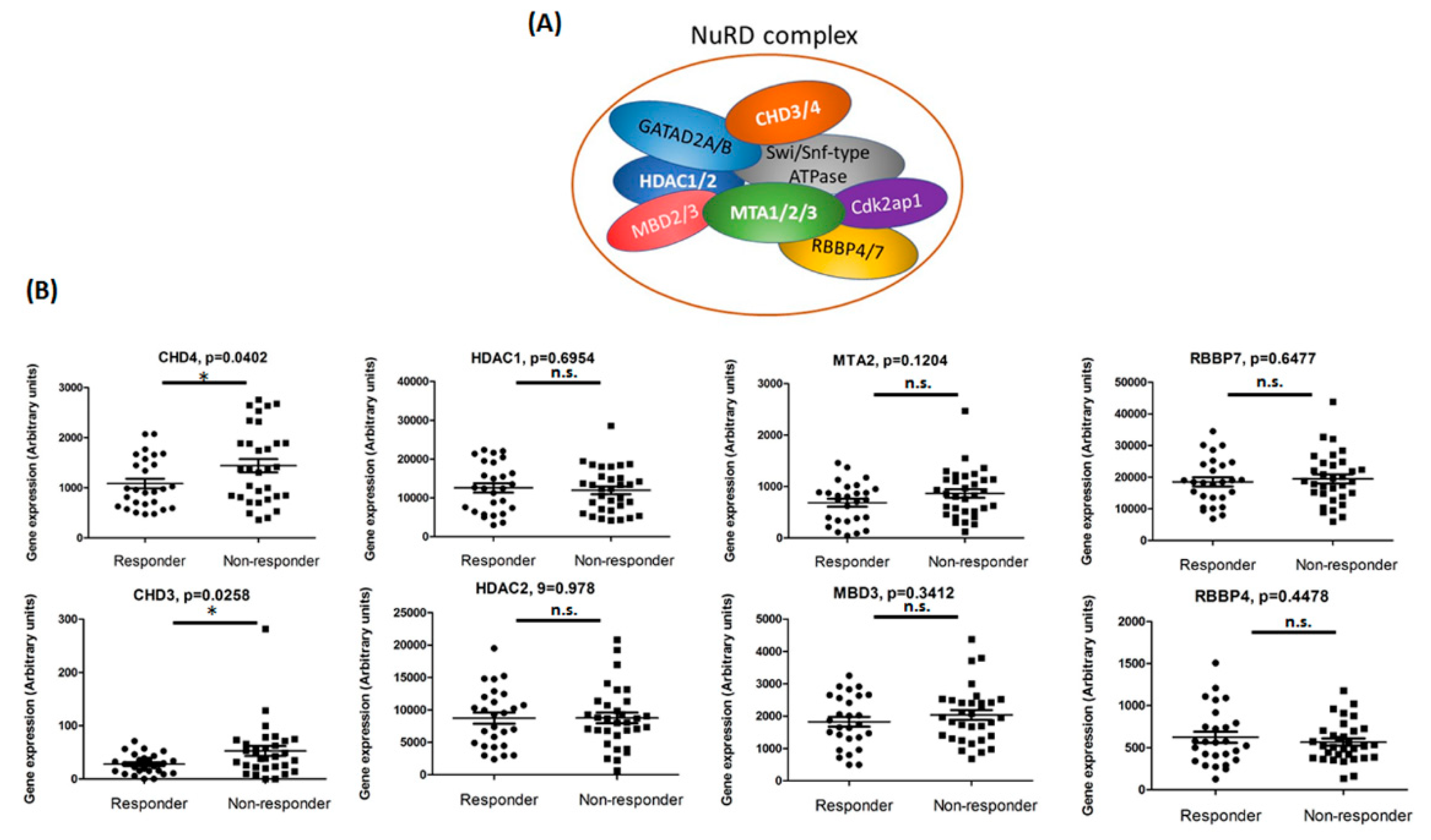
2.1. Identification of CHD4 as a Potential Biomarker Associated with Non-Responders to Pre-Operative CCRT of Rectal Cancer
2.2. Relationship between CHD4 Expression and Clinico-Pathological Features
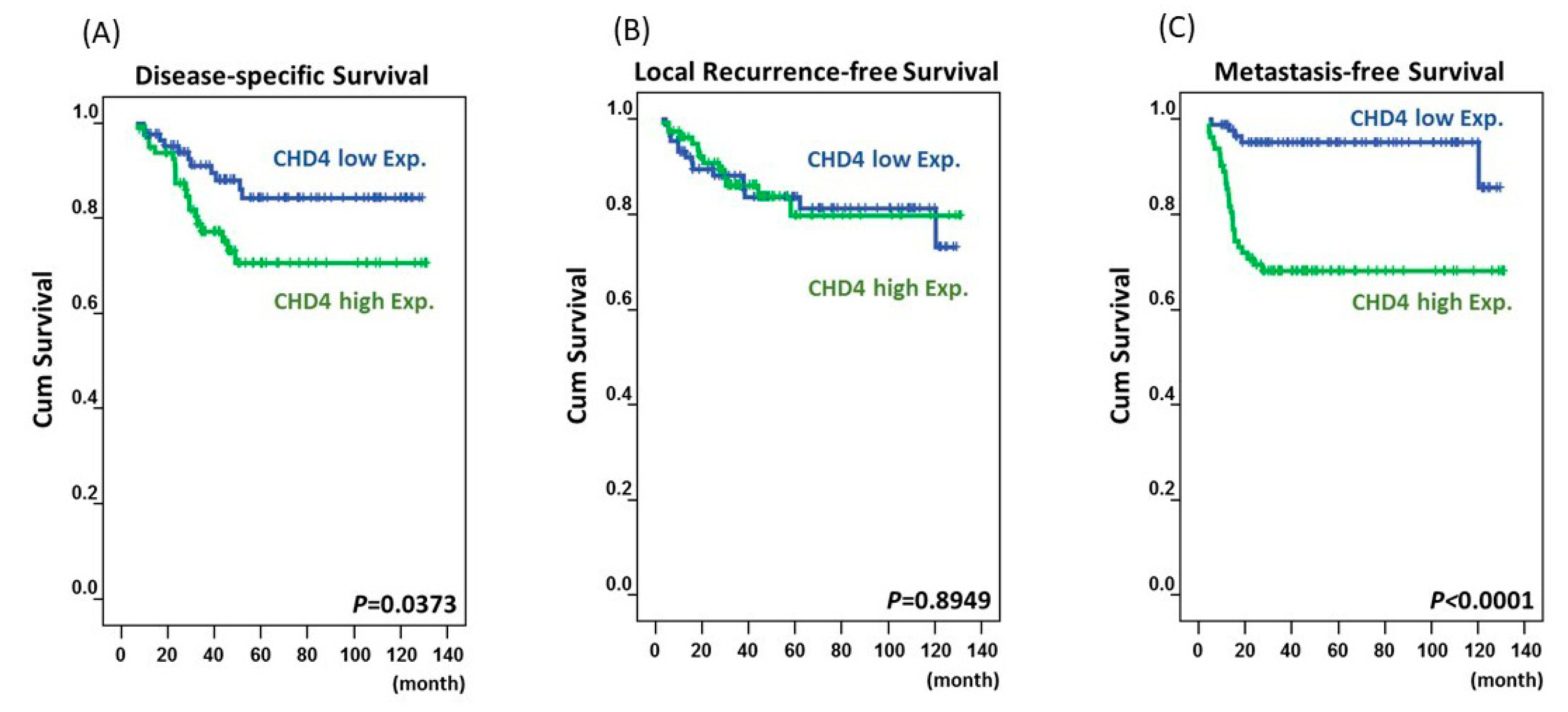
2.3. High Expression of CHD4 Is Associated with Poor Prognosis in Rectal Cancers Patients
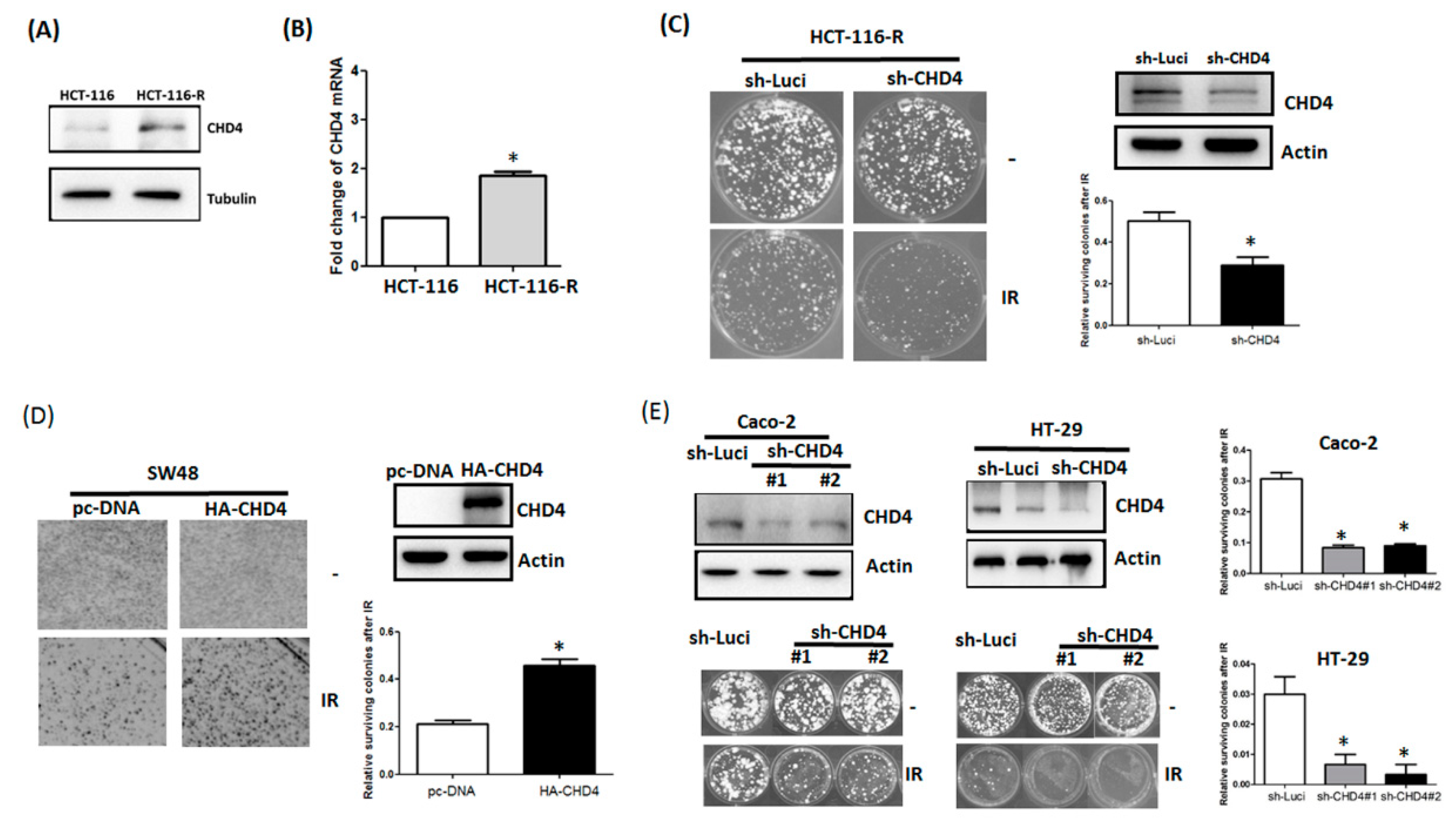
2.4. CHD4 Regulates Resistance to Radiation in CRC Cells of Varying MSI Status
3. Discussion
4. Materials and Methods
4.1. Microarray Data Analysis
4.2. Patients and Tissue Samples of Rectal Cancers
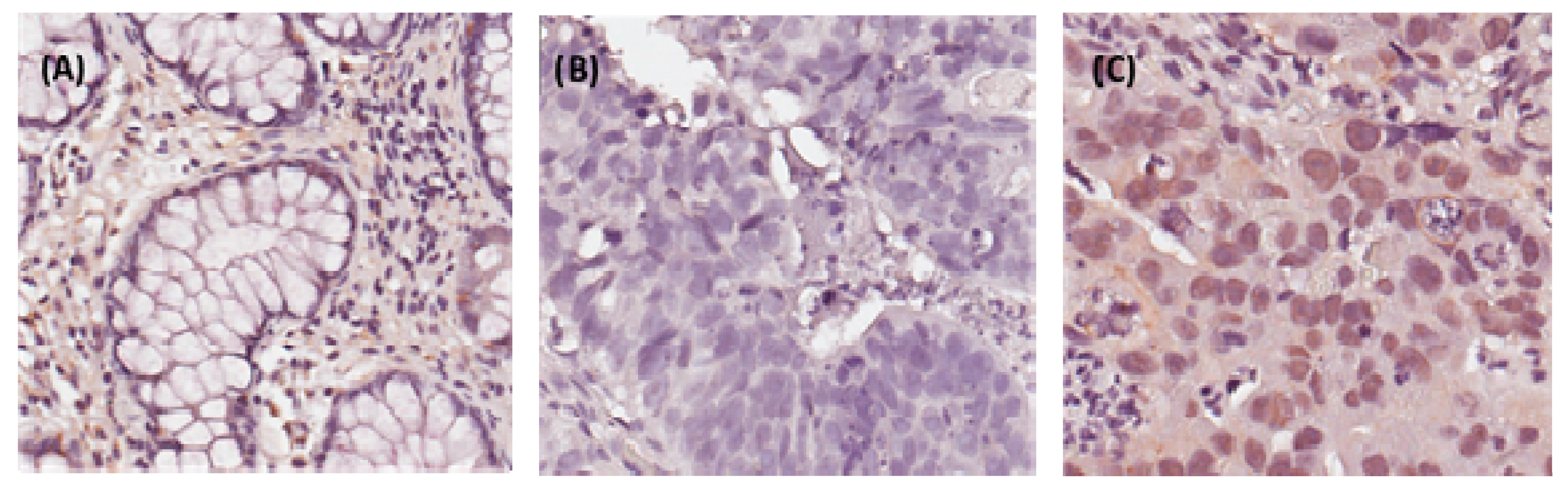
4.3. Histopathological and Immunohistochemical Assessments
4.4. Statistical Analysis
4.5. Cell Lines, Reagents and Plasmids
4.6. Quantitative Reverse-Transcription PCR (RT-qPCR)
4.7. Immunoblotting and Immunohistochemistry
4.8. Colony Formation Assays
Author Contributions
Funding
Conflicts of Interest
References
- Siegel, R.; Naishadham, D.; Jemal, A. Cancer statistics, 2013. CA Cancer J. Clin. 2013, 63, 11–30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Valentini, V.; Coco, C.; Picciocchi, A.; Morganti, A.G.; Trodella, L.; Ciabattoni, A.; Cellini, F.; Barbaro, B.; Cogliandolo, S.; Nuzzo, G. Does downstaging predict improved outcome after preoperative chemoradiation for extraperitoneal locally advanced rectal cancer? A long-term analysis of 165 patients. Int. J. Radiat. Oncol. Biol. Phys. 2002, 53, 664–674. [Google Scholar] [CrossRef]
- Rodel, C.; Martus, P.; Papadoupolos, T.; Füzesi, L.; Klimpfinger, M.; Fietkau, R.; Liersch, T.; Hohenberger, W.; Raab, R.; Sauer, R. Prognostic significance of tumor regression after preoperative chemoradiotherapy for rectal cancer. J. Clin. Oncol. 2005, 23, 8688–8696. [Google Scholar] [CrossRef] [PubMed]
- An, X.; Lin, X.; Wang, F.-H.; Goodman, K.; Cai, P.-Q.; Kong, L.-H.; Fang, Y.-J.; Gao, Y.-H.; Lin, J.-Z.; Wan, D.-S. Short term results of neoadjuvant chemoradiotherapy with fluoropyrimidine alone or in combination with oxaliplatin in locally advanced rectal cancer: A meta analysis. Eur. J. Cancer 2013, 49, 843–851. [Google Scholar] [CrossRef] [PubMed]
- Benson, A.B.; Venook, A.P.; Bekaii-Saab, T.; Chan, E.; Chen, Y.-J.; Cooper, H.S.; Engstrom, P.F.; Enzinger, P.C.; Fenton, M.J.; Fuchs, C.S. Rectal cancer, version 2.2015. J. Natl. Compr. Cancer Netw. 2015, 13, 719–728. [Google Scholar] [CrossRef]
- Van den Brink, M.; Stiggelbout, A.M.; van den Hout, W.B.; Kievit, J.; Kranenbarg, E.K.; Marijnen, C.A.; Nagtegaal, I.D.; Rutten, H.J.; Wiggers, T.; van de Velde, C.J. Clinical nature and prognosis of locally recurrent rectal cancer after total mesorectal excision with or without preoperative radiotherapy. J. Clin. Oncol. 2004, 22, 3958–3964. [Google Scholar] [CrossRef] [PubMed]
- Guillem, J.G.; Chessin, D.B.; Cohen, A.M.; Shia, J.; Mazumdar, M.; Enker, W.; Paty, P.B.; Weiser, M.R.; Klimstra, D.; Saltz, L. Long-term oncologic outcome following preoperative combined modality therapy and total mesorectal excision of locally advanced rectal cancer. Ann. Surg. 2005, 241, 829. [Google Scholar] [CrossRef] [PubMed]
- Longley, D.B.; Harkin, D.P.; Johnston, P.G. 5-fluorouracil: Mechanisms of action and clinical strategies. Nat. Rev. Cancer 2003, 3, 330. [Google Scholar] [CrossRef] [PubMed]
- Ozdian, T.; Holub, D.; Maceckova, Z.; Varanasi, L.; Rylova, G.; Rehulka, J.; Vaclavkova, J.; Slavik, H.; Moudry, P.; Znojek, P. Proteomic profiling reveals DNA damage, nucleolar and ribosomal stress are the main responses to oxaliplatin treatment in cancer cells. J. Proteom. 2017, 162, 73–85. [Google Scholar] [CrossRef] [PubMed]
- Goldstein, M.; Kastan, M.B. The DNA damage response: Implications for tumor responses to radiation and chemotherapy. Annu. Rev. Med. 2015, 66, 129–143. [Google Scholar] [CrossRef]
- Grivennikov, S.I.; Greten, F.R.; Karin, M. Immunity, inflammation, and cancer. Cell 2010, 140, 883–899. [Google Scholar] [CrossRef] [PubMed]
- Scott, T.L.; Rangaswamy, S.; Wicker, C.A.; Izumi, T. Repair of oxidative DNA damage and cancer: Recent progress in DNA base excision repair. Antioxid. Redox Signal. 2014, 20, 708–726. [Google Scholar] [CrossRef] [PubMed]
- AlDubayan, S.H.; Giannakis, M.; Moore, N.D.; Han, G.C.; Reardon, B.; Hamada, T.; Mu, X.J.; Nishihara, R.; Qian, Z.; Liu, L. Inherited DNA-repair defects in colorectal cancer. Am. J. Hum. Genet. 2018, 102, 401–414. [Google Scholar] [CrossRef] [PubMed]
- Li, S.K.; Martin, A. Mismatch repair and colon cancer: Mechanisms and therapies explored. Trends Mol. Med. 2016, 22, 274–289. [Google Scholar] [CrossRef] [PubMed]
- Allen, H.F.; Wade, P.A.; Kutateladze, T.G. The NuRD architecture. Cell. Mol. Life Sci. 2013, 70, 3513–3524. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kloet, S.L.; Baymaz, H.; Makowski, M.; Groenewold, V.; Jansen, P.W.; Berendsen, M.; Niazi, H.; Kops, G.J.; Vermeulen, M. Towards elucidating the stability, dynamics and architecture of the nucleosome remodeling and deacetylase complex by using quantitative interaction proteomics. Febs J. 2015, 282, 1774–1785. [Google Scholar] [CrossRef] [PubMed]
- Smeenk, G.; Wiegant, W.W.; Vrolijk, H.; Solari, A.P.; Pastink, A.; van Attikum, H. The NuRD chromatin–remodeling complex regulates signaling and repair of DNA damage. J. Cell Biol. 2010, 190, 741–749. [Google Scholar] [CrossRef]
- Lai, A.Y.; Wade, P.A. Cancer biology and NuRD: A multifaceted chromatin remodelling complex. Nat. Rev. Cancer 2011, 11, 588. [Google Scholar] [CrossRef]
- Ng, P.M.-L.; Lufkin, T. Embryonic stem cells: Protein interaction networks. Biomol. Concepts 2011, 2, 13–25. [Google Scholar]
- Sims, J.K.; Wade, P.A. Mi-2/NuRD complex function is required for normal S phase progression and assembly of pericentric heterochromatin. Mol. Biol. Cell 2011, 22, 3094–3102. [Google Scholar] [CrossRef]
- Silva, A.P.; Ryan, D.P.; Galanty, Y.; Low, J.K.; Vandevenne, M.; Jackson, S.P.; Mackay, J.P. The N-terminal region of chromodomain helicase DNA-binding protein 4 (CHD4) is essential for activity and contains a high mobility group (HMG) box-like-domain that can bind poly (ADP-ribose). J. Biol. Chem. 2016, 291, 924–938. [Google Scholar] [CrossRef] [PubMed]
- Larsen, D.H.; Poinsignon, C.; Gudjonsson, T.; Dinant, C.; Payne, M.R.; Hari, F.J.; Danielsen, J.M.R.; Menard, P.; Sand, J.C.; Stucki, M.; et al. The chromatin-remodeling factor CHD4 coordinates signaling and repair after DNA damage. J. Cell Biol. 2010, 190, 731–740. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pan, M.R.; Hsieh, H.J.; Dai, H.; Hung, W.C.; Li, K.; Peng, G.; Lin, S.Y. Chromodomain helicase DNA-binding protein 4 (CHD4) regulates homologous recombination DNA repair, and its deficiency sensitizes cells to poly(ADP-ribose) polymerase (PARP) inhibitor treatment. J. Biol. Chem. 2012, 287, 6764–6772. [Google Scholar] [CrossRef] [PubMed]
- Cai, Y.; Geutjes, E.-J.; De Lint, K.; Roepman, P.; Bruurs, L.; Yu, L.; Wang, W.; Van Blijswijk, J.; Mohammad, H.; De Rink, I. The NuRD complex cooperates with DNMTs to maintain silencing of key colorectal tumor suppressor genes. Oncogene 2014, 33, 2157. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.-Y.; Li, C.-F.; Lin, C.-Y.; Lee, S.-W.; Sheu, M.-J.; Lin, L.-C.; Chen, T.-J.; Wu, T.-F.; Hsing, C.-H. Overexpression of CPS1 is an independent negative prognosticator in rectal cancers receiving concurrent chemoradiotherapy. Tumor Biol. 2014, 35, 11097–11105. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.-Y.; Lin, C.-Y.; Chang, I.-W.; Sheu, M.-J.; Li, C.-F.; Lee, S.-W.; Lin, L.-C.; Lee, Y.-E.; He, H.-L. Low thrombospondin 2 expression is predictive of low tumor regression after neoadjuvant chemoradiotherapy in rectal cancer. Am. J. Transl. Res. 2015, 7, 2423. [Google Scholar] [PubMed]
- Xu, N.; Liu, F.; Zhou, J.; Bai, C. CHD4 is associated with poor prognosis of non-small cell lung cancer patients through promoting tumor cell proliferation. Eur. Respir. Soc. 2016, 48, PA2862. [Google Scholar]
- Nio, K.; Yamashita, T.; Okada, H.; Kondo, M.; Hayashi, T.; Hara, Y.; Nomura, Y.; Zeng, S.S.; Yoshida, M.; Hayashi, T. Defeating EpCAM+ liver cancer stem cells by targeting chromatin remodeling enzyme CHD4 in human hepatocellular carcinoma. J. Hepatol. 2015, 63, 1164–1172. [Google Scholar] [CrossRef] [Green Version]
- Xia, L.; Huang, W.; Bellani, M.; Seidman, M.M.; Wu, K.; Fan, D.; Nie, Y.; Cai, Y.; Zhang, Y.W.; Yu, L.-R. CHD4 has oncogenic functions in initiating and maintaining epigenetic suppression of multiple tumor suppressor genes. Cancer Cell 2017, 31, 653–668. [Google Scholar] [CrossRef]
- Guillemette, S.; Serra, R.W.; Peng, M.; Hayes, J.A.; Konstantinopoulos, P.A.; Green, M.R.; Cantor, S.B. Resistance to therapy in BRCA2 mutant cells due to loss of the nucleosome remodeling factor CHD4. Genes Dev. 2015, 29, 489–494. [Google Scholar] [CrossRef]
- D’Alesio, C.; Bellese, G.; Gagliani, M.C.; Lechiara, A.; Dameri, M.; Grasselli, E.; Lanfrancone, L.; Cortese, K.; Castagnola, P. The chromodomain helicase CHD4 regulates ERBB2 signaling pathway and autophagy in ERBB2+ breast cancer cells. Biol. Open 2019, 8, bio038323. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sperlazza, J.; Rahmani, M.; Beckta, J.; Aust, M.; Hawkins, E.; Wang, S.Z.; Zu Zhu, S.; Podder, S.; Dumur, C.; Archer, K. Depletion of the chromatin remodeler CHD4 sensitizes AML blasts to genotoxic agents and reduces tumor formation. Blood 2015, 126, 1462–1472. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Schutter, H.; Kimpe, M.; Isebaert, S.; Nuyts, S. A systematic assessment of radiation dose enhancement by 5-Aza-2′-deoxycytidine and histone deacetylase inhibitors in head-and-neck squamous cell carcinoma. Int. J. Radiat. Oncol. Biol. Phys. 2009, 73, 904–912. [Google Scholar] [CrossRef] [PubMed]
- Kwon, H.-M.; Kang, E.-J.; Kang, K.; Kim, S.-D.; Yang, K.; Yi, J.M. Combinatorial effects of an epigenetic inhibitor and ionizing radiation contribute to targeted elimination of pancreatic cancer stem cell. Oncotarget 2017, 8, 89005. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.S.; Chung, N.G.; Kang, M.R.; Yoo, N.J.; Lee, S.H. Genetic and expressional alterations of CHD genes in gastric and colorectal cancers. Histopathol. 2011, 58, 660–668. [Google Scholar] [CrossRef]
- Hou, M.-F.; Luo, C.-W.; Chang, T.-M.; Hung, W.-C.; Chen, T.-Y.; Tsai, Y.-L.; Chai, C.-Y.; Pan, M.-R. The NuRD complex-mediated p21 suppression facilitates chemoresistance in BRCA-proficient breast cancer. Exp. Cell Res. 2017, 359, 458–465. [Google Scholar] [CrossRef] [PubMed]
- Li, C.-F.; He, H.-L.; Wang, J.-Y.; Huang, H.-Y.; Wu, T.-F.; Hsing, C.-H.; Lee, S.-W.; Lee, H.-H.; Fang, J.-L.; Huang, W.-T. Fibroblast growth factor receptor 2 overexpression is predictive of poor prognosis in rectal cancer patients receiving neoadjuvant chemoradiotherapy. J. Clin. Pathol. 2014, 67, 1056–1061. [Google Scholar] [CrossRef] [Green Version]
- Sobin, L.H.; Gospodarowicz, M.K.; Wittekind, C. TNM Classification of Malignant Tumours; John Wiley & Sons: Hoboken NJ, USA, 2011. [Google Scholar]
- Dworak, O.; Keilholz, L.; Hoffmann, A. Pathological features of rectal cancer after preoperative radiochemotherapy. Int. J. Colorectal Dis. 1997, 12, 19–23. [Google Scholar] [CrossRef]
- Chang, I.-W.; Lin, V.C.-H.; Wu, W.-J.; Liang, P.-I.; Li, W.-M.; Yeh, B.-W.; He, H.-L.; Liao, A.C.-H.; Chan, T.-C.; Li, C.-F. Complement component 1, s subcomponent overexpression is an independent poor prognostic indicator in patients with urothelial carcinomas of the upper urinary tract and urinary bladder. J. Cancer 2016, 7, 1396. [Google Scholar] [CrossRef]
- Ma, L.-J.; Wu, W.-J.; Wang, Y.-H.; Wu, T.-F.; Liang, P.-I.; Chang, I.-W.; He, H.-L.; Li, C.-F. SPOCK1 overexpression confers a poor prognosis in urothelial carcinoma. J. Cancer 2016, 7, 467. [Google Scholar] [CrossRef]
- Chang, I.-W.; Li, C.-F.; Lin, V.C.-H.; He, H.-L.; Liang, P.-I.; Wu, W.-J.; Li, C.-C.; Huang, C.-N. Prognostic impact of thrombospodin-2 (THBS2) overexpression on patients with urothelial carcinomas of upper urinary tracts and bladders. J. Cancer 2016, 7, 1541. [Google Scholar] [CrossRef] [PubMed]
- Luo, C.-W.; Wu, C.-C.; Chang, S.-J.; Chang, T.-M.; Chen, T.-Y.; Chai, C.-Y.; Chang, C.-L.; Hou, M.-F.; Pan, M.-R. CHD4-mediated loss of E-cadherin determines metastatic ability in triple-negative breast cancer cells. Exp. Cell Res. 2018, 363, 65–72. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.-Y.; Lee, Y.-E.; Tian, Y.-F.; Sun, D.-P.; Sheu, M.-J.; Lin, C.-Y.; Li, C.-F.; Lee, S.-W.; Lin, L.-C.; Chang, I.-W. High expression of EphA4 predicted lesser degree of tumor regression after neoadjuvant chemoradiotherapy in rectal cancer. J. Cancer 2017, 8, 1089. [Google Scholar] [CrossRef] [PubMed]
- Tian, Y.-F.; Wang, H.-C.; Luo, C.-W.; Hung, W.-C.; Lin, Y.-H.; Chen, T.-Y.; Li, C.-F.; Lin, C.-Y.; Pan, M.-R. Preprogramming therapeutic response of PI3K/mTOR dual inhibitor via the regulation of EHMT2 and p27 in pancreatic cancer. Am. J. Cancer Res. 2018, 8, 1812. [Google Scholar] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | No. | CHD4 Expression | p-Value | ||
|---|---|---|---|---|---|
| Low Exp. | High Exp. | ||||
| Gender | Male | 108 | 60 | 48 | 0.194 |
| Female | 64 | 29 | 35 | ||
| Age | <70 | 106 | 61 | 45 | 0.054 |
| ≥70 | 66 | 28 | 38 | ||
| Pre-Tx tumor status (Pre-T) | T1–T2 | 81 | 55 | 26 | <0.001 * |
| T3–T4 | 91 | 34 | 57 | ||
| Pre-Tx nodal status (Pre-N) | N0 | 125 | 77 | 48 | <0.001 * |
| N1–N2 | 47 | 12 | 35 | ||
| Post-Tx tumor status (Post-T) | T1–T2 | 86 | 57 | 29 | <0.001 * |
| T3–T4 | 86 | 32 | 54 | ||
| Post-Tx nodal status (Post-N) | N0 | 123 | 76 | 47 | <0.001 * |
| N1–N2 | 49 | 13 | 36 | ||
| Vascular invasion | Absent | 157 | 85 | 72 | 0.042 * |
| Present | 15 | 4 | 11 | ||
| Perineural invasion | Absent | 167 | 88 | 79 | 0.149 |
| Present | 5 | 1 | 4 | ||
| Tumor regression grade | Grade 0–1 | 37 | 11 | 26 | 0.001 * |
| Grade 2–3 | 118 | 64 | 54 | ||
| Grade 4 | 17 | 14 | 3 | ||
| Parameter | No. of Case | DSS | LRFS | MeFS | ||||
|---|---|---|---|---|---|---|---|---|
| No. of Event | p-Value | No. of Event | p-Value | No. of Event | p-Value | |||
| Gender | Male | 108 | 20 | 0.6027 | 5 | 0.3096 | 14 | 0.1047 |
| Female | 64 | 11 | 17 | 15 | ||||
| Age | <70 | 106 | 19 | 0.7158 | 14 | 0.9630 | 18 | 0.9520 |
| ≥70 | 66 | 12 | 8 | 11 | ||||
| Pre-Tx tumor status (Pre-T) | T1–T2 | 81 | 10 | 0.0484 * | 7 | 0.0836 | 10 | 0.1288 |
| T3–T4 | 91 | 21 | 15 | 19 | ||||
| Pre-Tx nodal status (Pre-N) | N0 | 125 | 19 | 0.0059 * | 12 | 0.0025 * | 18 | 0.0866 |
| N1–N2 | 47 | 21 | 10 | 11 | ||||
| Post-Tx tumor status (Post-T) | T1–T2 | 86 | 7 | 0.0014 * | 5 | 0.0056 * | 8 | 0.0123 * |
| T3–T4 | 86 | 24 | 17 | 21 | ||||
| Post-Tx nodal status (Post-N) | N0 | 123 | 21 | 0.4654 | 15 | 0.6267 | 20 | 0.8403 |
| N1–N2 | 49 | 10 | 7 | 9 | ||||
| Vascular invasion | Absent | 157 | 25 | 0.0123 * | 17 | 0.0023 * | 26 | 0.7236 |
| Present | 15 | 6 | 5 | 3 | ||||
| Perineural invasion | Absent | 167 | 29 | 0.0994 | 20 | 0.0083 * | 28 | 0.8157 |
| Present | 5 | 2 | 2 | 1 | ||||
| Tumor regression grade | Grade 0–1 | 37 | 13 | 0.0037 * | 10 | 0.0021 * | 14 | 0.0008 * |
| Grade 2–3 | 118 | 17 | 12 | 14 | ||||
| Grade 4 | 17 | 1 | 0 | 1 | ||||
| Down stage after CCRT | Non-Significant | 150 | 29 | 0.2348 | 20 | 0.5234 | 28 | 0.1291 |
| Significant (≥2) | 22 | 2 | 2 | 1 | ||||
| CHD4 expression | Low Exp. | 89 | 11 | 0.0373 * | 15 | 0.8949 | 5 | <0.0001 * |
| High Exp. | 83 | 20 | 12 | 26 | ||||
| Parameter | DSS | LRFS | MeFS | ||||||
|---|---|---|---|---|---|---|---|---|---|
| H.R | 95% CI | p-Value | H.R | 95% CI | p-Value | H.R | 95% CI | p-Value | |
| Tumor regression grade | 2.262 | 1.1198–4.566 | 0.023 * | 2.198 | 1.002–4.831 | 0.015 * | 2.32 | 1.063–4.292 | 0.033 * |
| CHD4 expression | 1.181 | 0.519–2.686 | 0.692 | - | - | - | 4.575 | 1.717–12.192 | 0.002* |
| Vascular invasion | 2.082 | 0.771–5.622 | 0.148 | 2.510 | 0.902–6.985 | 0.078 | - | - | - |
| Post-Tx tumor status (Post-T) | 2.447 | 0.992–6.034 | 0.052 | 2.041 | 0.825–5.051 | 0.123 | 1.736 | 0.751–4.012 | 0.197 |
| Pre-Tx nodal status (Pre-N) | 1.286 | 0.538–3.070 | 0.571 | 1.993 | 0.833–4.770 | 0.121 | - | - | - |
| Pre-Tx tumor status (Pre-T) | 1.283 | 0.532–3.096 | 0.579 | - | - | - | - | - | - |
| Perineural invasion | - | - | - | 1.122 | 0.231–5.447 | 0.887 | - | - | - |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, H.-C.; Chou, C.-L.; Yang, C.-C.; Huang, W.-L.; Hsu, Y.-C.; Luo, C.-W.; Chen, T.-J.; Li, C.-F.; Pan, M.-R. Over-Expression of CHD4 Is an Independent Biomarker of Poor Prognosis in Patients with Rectal Cancers Receiving Concurrent Chemoradiotherapy. Int. J. Mol. Sci. 2019, 20, 4087. https://doi.org/10.3390/ijms20174087
Wang H-C, Chou C-L, Yang C-C, Huang W-L, Hsu Y-C, Luo C-W, Chen T-J, Li C-F, Pan M-R. Over-Expression of CHD4 Is an Independent Biomarker of Poor Prognosis in Patients with Rectal Cancers Receiving Concurrent Chemoradiotherapy. International Journal of Molecular Sciences. 2019; 20(17):4087. https://doi.org/10.3390/ijms20174087
Chicago/Turabian StyleWang, Hui-Ching, Chia-Lin Chou, Ching-Chieh Yang, Wei-Lun Huang, Yin-Chou Hsu, Chi-Wen Luo, Tzu-Ju Chen, Chien-Feng Li, and Mei-Ren Pan. 2019. "Over-Expression of CHD4 Is an Independent Biomarker of Poor Prognosis in Patients with Rectal Cancers Receiving Concurrent Chemoradiotherapy" International Journal of Molecular Sciences 20, no. 17: 4087. https://doi.org/10.3390/ijms20174087