Lumbar Degenerative Disease Part 1: Anatomy and Pathophysiology of Intervertebral Discogenic Pain and Radiofrequency Ablation of Basivertebral and Sinuvertebral Nerve Treatment for Chronic Discogenic Back Pain: A Prospective Case Series and Review of Literature



Abstract
:1. Introduction
2. Results
3. Discussion
3.1. Anatomy of a Normal Disc
3.2. Structure of Annulus Fibrosus
3.3. Structure of Nucleus Pulposus
3.4. Structure of Vertebral End Plates
3.5. Pathoanatomy: Structural Changes to a Disc in a Pathological State
3.6. Types of Pathology in a Disc
3.7. Pathophysiology: Etiology of Degenerative Disc Disease
3.8. Potential Trigger Events
3.9. Structural and Biomechanics of Spine and Pelvis Affecting DDD
3.10. Muscle Dynamics and General Joint Laxity Effect on Disc Pathology
3.11. Mechanical Load
3.12. Genetics and Degenerated Disc
3.13. Environmental and Psychosocial Factors Associated with DDD
3.14. Nutritional Deficiency
3.15. Exercise
3.16. Pathophysiology of Pain in Lumbar Degenerative Disc Disease
3.17. Types of Lower Back Pain
3.18. Adjacent Vertebra End Plates and Bodies Stressed Related Pain Response
3.19. Modic Changes and Pain Simulation
3.20. Genetics and Its Effect on Pain Perception in Disc Diseases
3.21. Factors Release Inducing Innervation and Neuronal Sensitization
3.21.1. Inflammatory Processes
3.21.2. Neuronal Sensitization and Pathologic Innervation of Disc
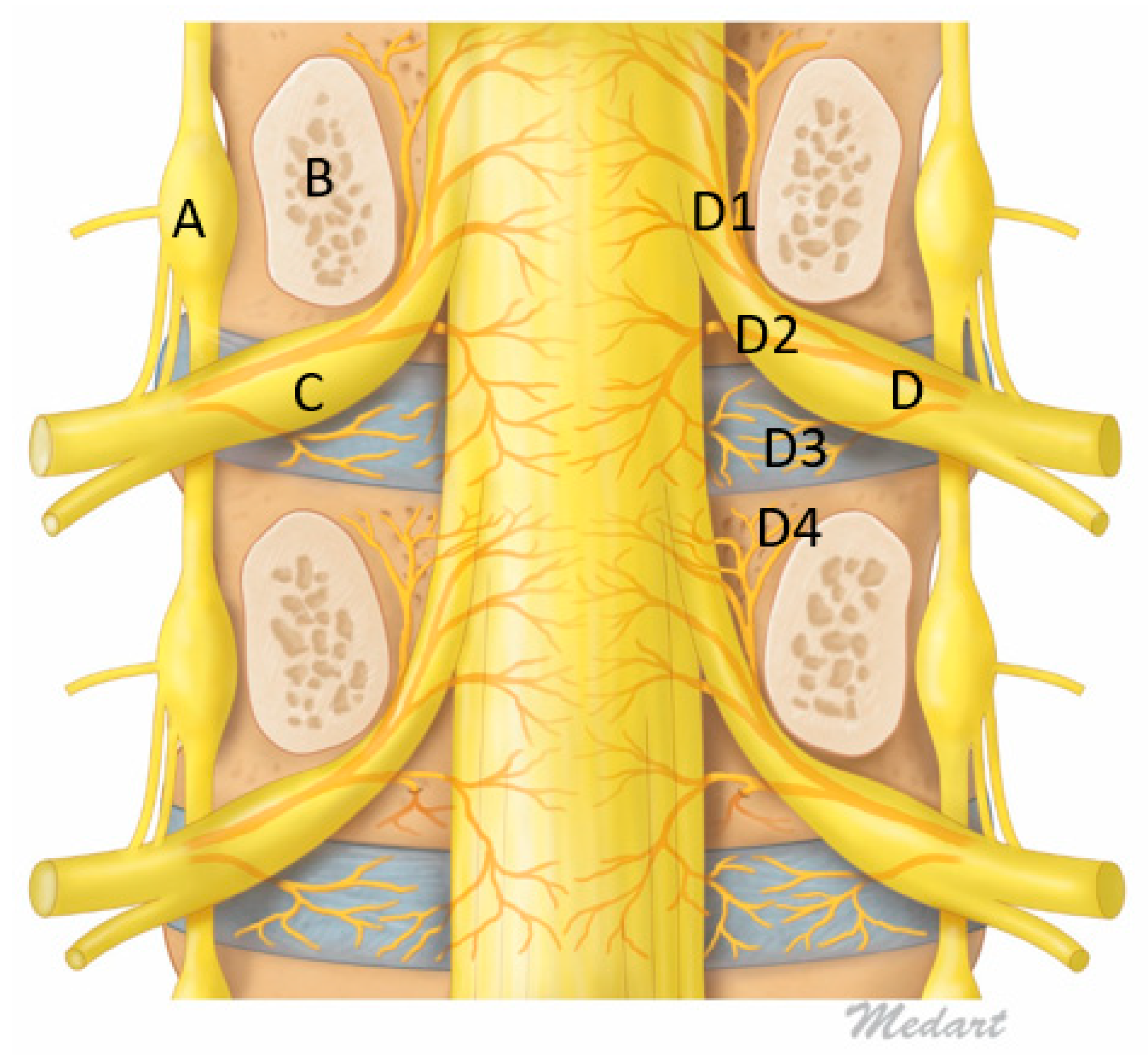
3.21.3. Sinuvertebral Nerve
3.22. Discogenic Back Pain and Sinuvertebral Nerves
3.22.1. Basivertebral Nerve
3.22.2. Diagnostic and Treatment Procedures
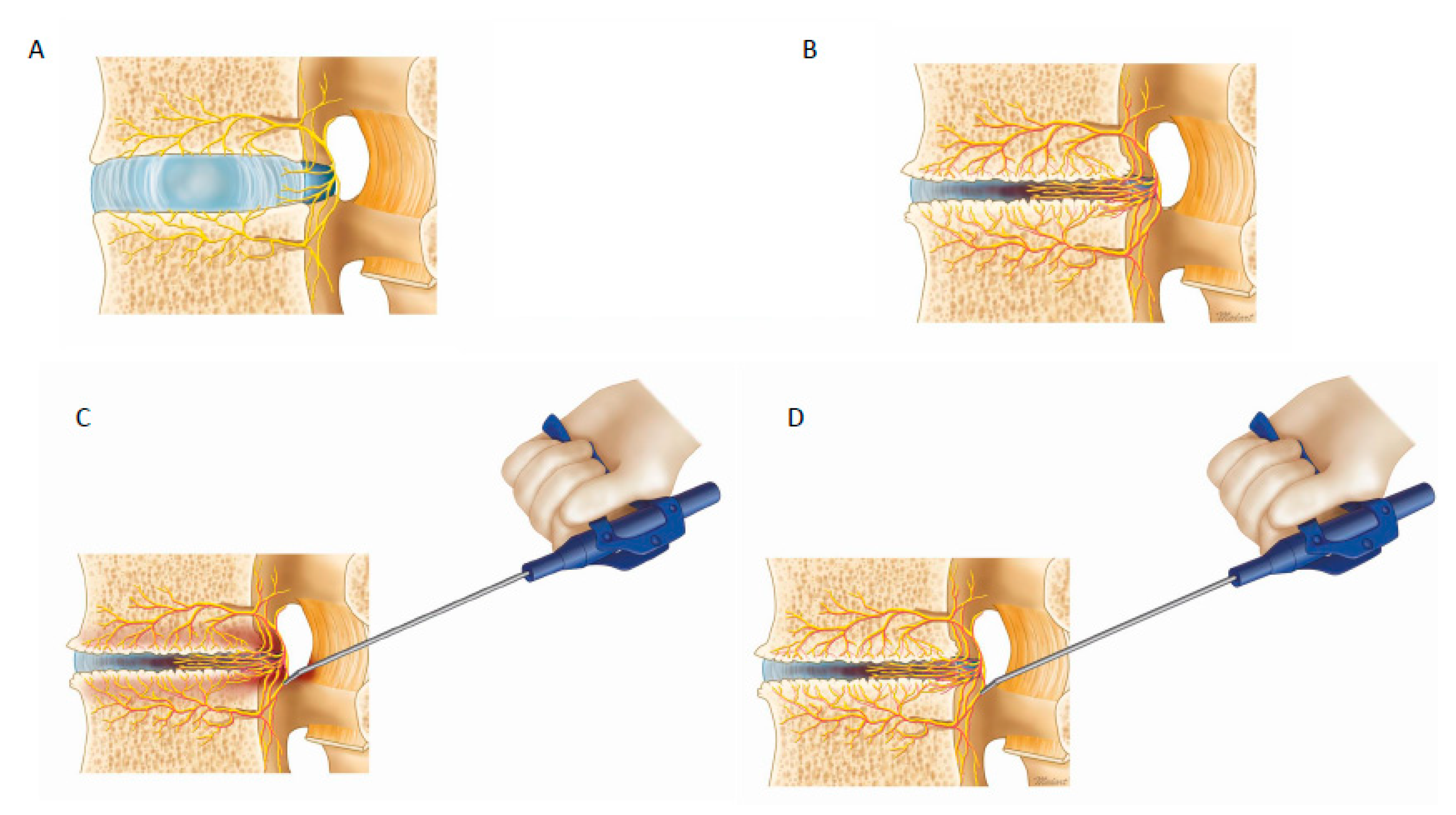
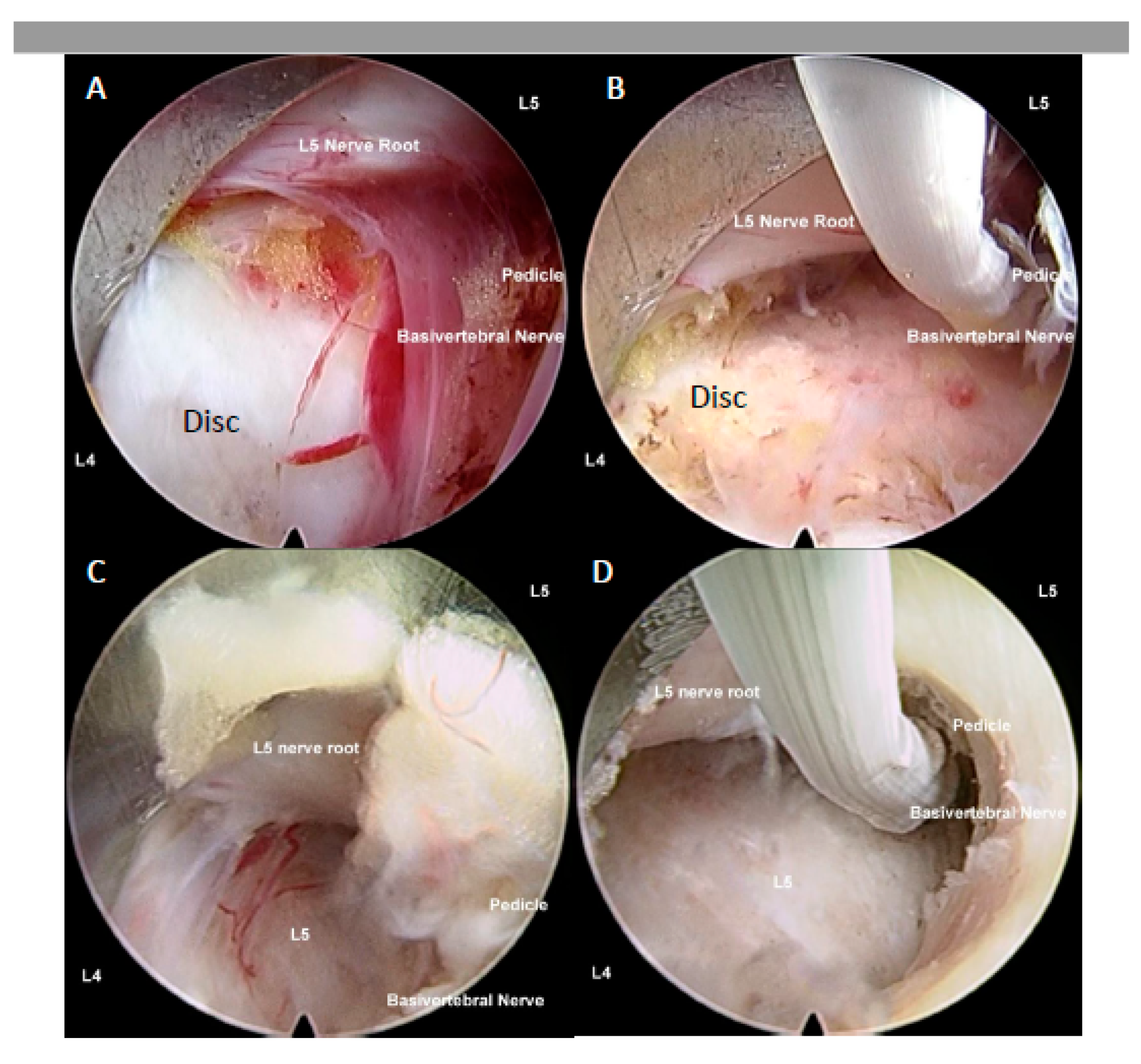
3.22.3. Radiofrequency Ablation
3.23. Limitations
3.24. Summary of Discogenic Back Pain Pathway and the Role Sinuvertebral Nerve and Basivertebral Nerve in Molecular Science
4. Materials and Methods
4.1. Surgical Technique
4.1.1. Interlaminar Endoscopic Lumbar Approach to Disc
4.1.2. Lumbar Endoscopic Unilateral Laminotomy for Bilateral Decompression with Radiofrequency Ablation
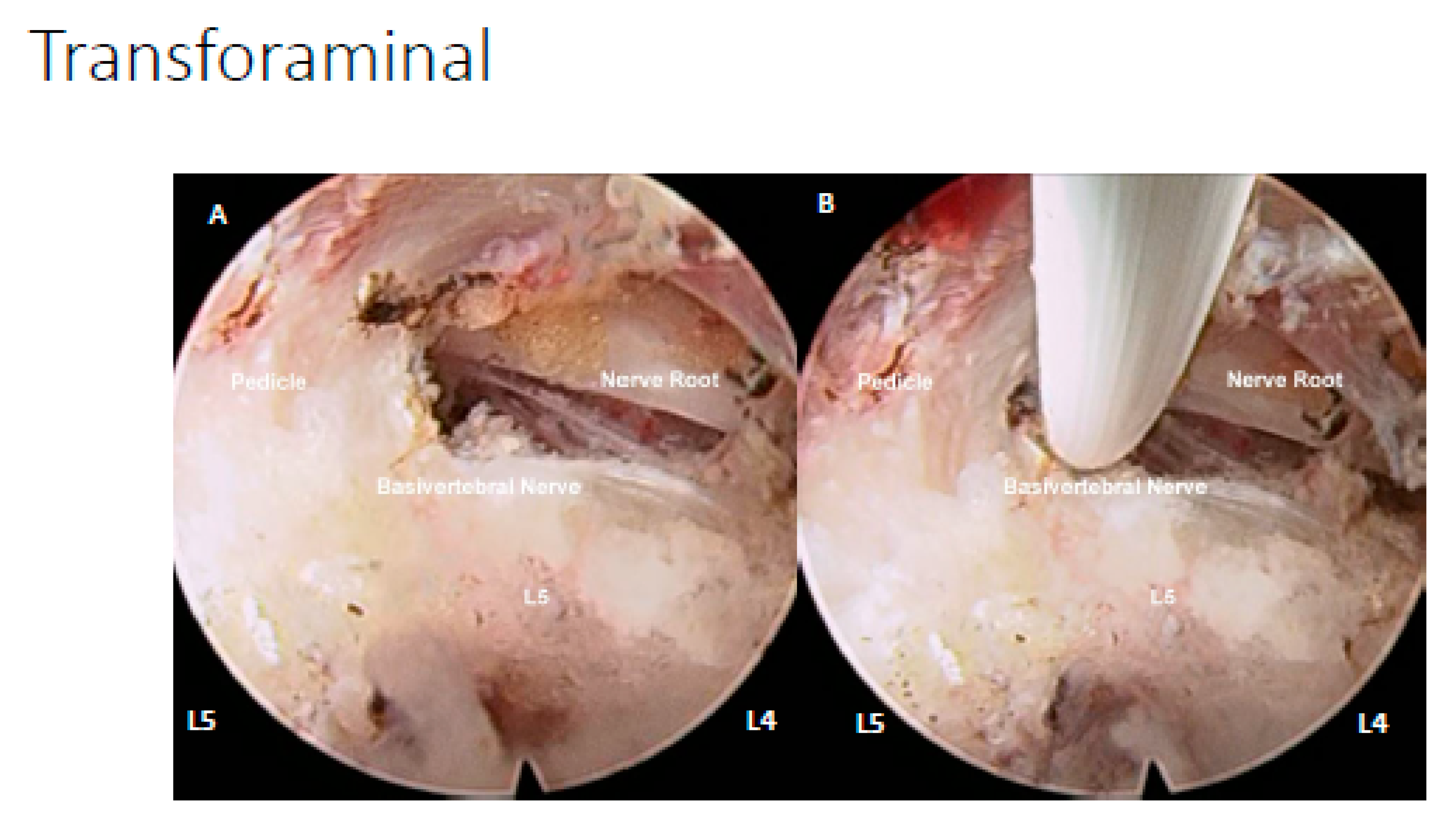
4.1.3. Transforaminal Endoscopic Lumbar Approach for Radiofrequency Ablation
4.2. Ablation of Neuropathic Basivertebral Nerve and Sinuvertebral Nerve
4.3. Data Collection
4.4. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| IVD | Intervertebral Disc |
| DDD | Degenerative Disc Disease |
| ODI | Oswestry Disability Index |
| VAS | Visual Analogue Scale |
| AF | Annulus Fibrosus |
| NP | Nucleus Pulposus |
| PLL | Posterior Longitudinal Ligament |
| SVN | Sinuvertebral Nerve |
| BVN | Basivertebral Nerve |
References
- Vos, T.P.; Flaxman, A.D.P.; Naghavi, M.P.; Lozano, R.P.; Michaud, C.M.D.; Ezzati, M.P.; Shibuya, K.P.; Salomon, J.A.P.; Abdalla, S.M.; Aboyans, V.P.; et al. Years lived with disability (YLDs) for 1160 sequelae of 289 diseases and injuries 1990–2010: A systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012, 380, 2163–2196. [Google Scholar] [CrossRef]
- Zhu, Q.; Gao, X.; Levene, H.B.; Brown, M.D.; Gu, W. Influences of Nutrition Supply and Pathways on the Degenerative Patterns in Human Intervertebral Disc. Spine (Phila Pa 1976) 2016, 41, 568–576. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zawilla, N.H.; Darweesh, H.; Mansour, N.; Helal, S.; Taha, F.M.; Awadallah, M.; El Shazly, R. Matrix metalloproteinase-3, vitamin D receptor gene polymorphisms, and occupational risk factors in lumbar disc degeneration. J. Occup. Rehabil. 2014, 24, 370–381. [Google Scholar] [CrossRef]
- Willems, P. Decision making in surgical treatment of chronic low back pain: The performance of prognostic tests to select patients for lumbar spinal fusion. Acta Orthop. 2013, 84, 1–35. [Google Scholar] [CrossRef] [PubMed]
- Wong, J.J.; Cote, P.; Sutton, D.A.; Randhawa, K.; Yu, H.; Varatharajan, S.; Goldgrub, R.; Nordin, M.; Gross, D.P.; Shearer, H.M.; et al. Clinical practice guidelines for the noninvasive management of low back pain: A systematic review by the Ontario Protocol for Traffic Injury Management (OPTIMa) Collaboration. Eur. J. Pain 2017, 21, 201–216. [Google Scholar] [CrossRef] [PubMed]
- Simon, J.; McAuliffe, M.; Shamim, F.; Vuong, N.; Tahaei, A. Discogenic low back pain. Phys. Med. Rehabil. Clin. N. Am. 2014, 25, 305–317. [Google Scholar] [CrossRef]
- Suseki, K.; Takahashi, Y.; Takahashi, K.; Chiba, T.; Yamagata, M.; Moriya, H. Sensory nerve fibres from lumbar intervertebral discs pass through rami communicantes. A possible pathway for discogenic low back pain. J. Bone Jt. Surg Br. 1998, 80, 737–742. [Google Scholar] [CrossRef]
- Shayota, B.; Wong, T.L.; Fru, D.; David, G.; Iwanaga, J.; Loukas, M.; Tubbs, R.S. A comprehensive review of the sinuvertebral nerve with clinical applications. Anat Cell Biol 2019, 52, 128–133. [Google Scholar] [CrossRef]
- Schliessbach, J.; Siegenthaler, A.; Heini, P.; Bogduk, N.; Curatolo, M. Blockade of the sinuvertebral nerve for the diagnosis of lumbar diskogenic pain: An exploratory study. Anesth. Analg. 2010, 111, 204–206. [Google Scholar] [CrossRef]
- Kim, H.S.; Paudel, B.; Chung, S.K.; Jang, J.S.; Oh, S.H.; Jang, I.T. Transforaminal Epiduroscopic Laser Ablation of Sinuvertebral Nerve in Patients with Chronic Diskogenic Back Pain: Technical Note and Preliminary Result. J. Neurol. Surg.. 2017, 78, 529–534. [Google Scholar] [CrossRef]
- Kim, H.S.; Adsul, N.; Yudoyono, F.; Paudel, B.; Kim, K.J.; Choi, S.H.; Kim, J.H.; Chung, S.K.; Choi, J.-H.; Jang, J.-S.; et al. Transforaminal Epiduroscopic Basivertebral Nerve Laser Ablation for Chronic Low Back Pain Associated with Modic Changes: A Preliminary Open-Label Study. Pain Res. Manag 2018, 2018, 6857983. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fischgrund, J.S.; Rhyne, A.; Franke, J.; Sasso, R.; Kitchel, S.; Bae, H.; Yeung, C.; Truumees, E.; Schaufele, M.; Yuan, P.; et al. Intraosseous Basivertebral Nerve Ablation for the Treatment of Chronic Low Back Pain: 2-Year Results From a Prospective Randomized Double-Blind Sham-Controlled Multicenter Study. Int. J. Spine Surg. 2019, 13, 110–119. [Google Scholar] [CrossRef] [PubMed]
- Tagliaferri, S.D.; Miller, C.T. Domains of Chronic Low Back Pain and Assessing Treatment Effectiveness: A Clinical Perspective. Pain Pract. 2019. [Google Scholar] [CrossRef] [PubMed]
- Steelman, T.; Lewandowski, L.; Helgeson, M.; Wilson, K.; Olsen, C.; Gwinn, D. Population-based Risk Factors for the Development of Degenerative Disk Disease. Clin. Spine Surg. 2018, 31, E409–E412. [Google Scholar] [CrossRef]
- Dowdell, J.; Erwin, M.; Choma, T.; Vaccaro, A.; Iatridis, J.; Cho, S.K. Intervertebral Disk Degeneration and Repair. Neurosurgery 2017, 80, S46–S54. [Google Scholar] [CrossRef]
- Humzah, M.D.; Soames, R.W. Human intervertebral disc: Structure and function. Anat. Rec. 1988, 220, 337–356. [Google Scholar] [CrossRef]
- Pooni, J.S.; Hukins, D.W.; Harris, P.F.; Hilton, R.C.; Davies, K.E. Comparison of the structure of human intervertebral discs in the cervical, thoracic and lumbar regions of the spine. Surg. Radiol. Anat. Sra 1986, 8, 175–182. [Google Scholar] [CrossRef]
- Raj, P.P. Intervertebral disc: Anatomy-physiology-pathophysiology-treatment. Pain Pract. 2008, 8, 18–44. [Google Scholar] [CrossRef]
- Balkovec, C.; Adams, M.A.; Dolan, P.; McGill, S.M. Annulus Fibrosus Can Strip Hyaline Cartilage End Plate from Subchondral Bone: A Study of the Intervertebral Disk in Tension. Glob. Spine J. 2015, 5, 360–365. [Google Scholar] [CrossRef] [Green Version]
- Guerin, H.L.; Elliott, D.M. Quantifying the contributions of structure to annulus fibrosus mechanical function using a nonlinear, anisotropic, hyperelastic model. J. Orthop. Res. 2007, 25, 508–516. [Google Scholar] [CrossRef]
- Mouw, J.K.; Ou, G.; Weaver, V.M. Extracellular matrix assembly: A multiscale deconstruction. Nat. Rev. Mol. Cell Biol. 2014, 15, 771–785. [Google Scholar] [CrossRef] [PubMed]
- Smith, L.J.; Fazzalari, N.L. The elastic fibre network of the human lumbar anulus fibrosus: Architecture, mechanical function and potential role in the progression of intervertebral disc degeneration. Eur. Spine J. 2009, 18, 439–448. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eyre, D.R.; Muir, H. Types I and II collagens in intervertebral disc. Interchanging radial distributions in annulus fibrosus. Biochem. J. 1976, 157, 267–270. [Google Scholar] [CrossRef]
- Yanagishita, M. Function of proteoglycans in the extracellular matrix. Acta Pathol. Jpn. 1993, 43, 283–293. [Google Scholar] [CrossRef] [PubMed]
- Green, T.P.; Adams, M.A.; Dolan, P. Tensile properties of the annulus fibrosus II. Ultimate tensile strength and fatigue life. Eur. Spine J. 1993, 2, 209–214. [Google Scholar] [CrossRef] [PubMed]
- Bonetti, M.I. Microfibrils: A cornerstone of extracellular matrix and a key to understand Marfan syndrome. Ital. J. Anat. Embryol. Arch. Ital. Anat. Ed. Embriol. 2009, 114, 201–224. [Google Scholar]
- Iatridis, J.C.; Setton, L.A.; Weidenbaum, M.; Mow, V.C. Alterations in the mechanical behavior of the human lumbar nucleus pulposus with degeneration and aging. J. Orthop. Res. 1997, 15, 318–322. [Google Scholar] [CrossRef]
- Muir, H. The chondrocyte, architect of cartilage. Biomechanics, structure, function and molecular biology of cartilage matrix macromolecules. Bioessays News Rev. Mol. Cell. Dev. Biol. 1995, 17, 1039–1048. [Google Scholar] [CrossRef]
- Mwale, F.; Roughley, P.; Antoniou, J. Distinction between the extracellular matrix of the nucleus pulposus and hyaline cartilage: A requisite for tissue engineering of intervertebral disc. Eur. Cells Mater. 2004, 8, 58–63, discussion 63–54. [Google Scholar] [CrossRef]
- Moore, R.J. The vertebral endplate: Disc degeneration, disc regeneration. Eur. Spine J. 2006, 15, S333–S337. [Google Scholar] [CrossRef] [Green Version]
- Lotz, J.C.; Fields, A.J.; Liebenberg, E.C. The role of the vertebral end plate in low back pain. Glob. Spine J. 2013, 3, 153–164. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grant, J.P.; Oxland, T.R.; Dvorak, M.F. Mapping the structural properties of the lumbosacral vertebral endplates. Spine (Phila Pa 1976) 2001, 26, 889–896. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nekkanty, S.; Yerramshetty, J.; Kim, D.G.; Zauel, R.; Johnson, E.; Cody, D.D.; Yeni, Y.N. Stiffness of the endplate boundary layer and endplate surface topography are associated with brittleness of human whole vertebral bodies. Bone 2010, 47, 783–789. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Akkiraju, H.; Nohe, A. Role of Chondrocytes in Cartilage Formation, Progression of Osteoarthritis and Cartilage Regeneration. J. Dev. Biol. 2015, 3, 177–192. [Google Scholar] [CrossRef] [Green Version]
- Rudert, M.; Tillmann, B. Lymph and blood supply of the human intervertebral disc. Cadaver study of correlations to discitis. Acta Orthop. Scand. 1993, 64, 37–40. [Google Scholar] [CrossRef] [Green Version]
- Nerlich, A.G.; Schaaf, R.; Walchli, B.; Boos, N. Temporo-spatial distribution of blood vessels in human lumbar intervertebral discs. Eur. Spine J. 2007, 16, 547–555. [Google Scholar] [CrossRef] [Green Version]
- Nachemson, A.; Lewin, T.; Maroudas, A.; Freeman, M.A. In vitro diffusion of dye through the end-plates and the annulus fibrosus of human lumbar inter-vertebral discs. Acta Orthop. Scand. 1970, 41, 589–607. [Google Scholar] [CrossRef] [Green Version]
- Fardon, D.F.; Williams, A.L.; Dohring, E.J.; Murtagh, F.R.; Gabriel Rothman, S.L.; Sze, G.K. Lumbar disc nomenclature: Version 2.0: Recommendations of the combined task forces of the North American Spine Society, the American Society of Spine Radiology and the American Society of Neuroradiology. Spine J. 2014, 14, 2525. [Google Scholar] [CrossRef] [Green Version]
- Modic, M.T.; Herfkens, R.J. Intervertebral disk: Normal age-related changes in MR signal intensity. Radiology 1990, 177, 332–333, discussion 333–334. [Google Scholar] [CrossRef]
- Resnick, D. Degenerative diseases of the vertebral column. Radiology 1985, 156, 3–14. [Google Scholar] [CrossRef]
- Ford, L.T.; Gilula, L.A.; Murphy, W.A.; Gado, M. Analysis of gas in vacuum lumbar disc. Ajr. Am. J. Roentgenol. 1977, 128, 1056–1057. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oh, K.J.; Lee, J.W.; Yun, B.L.; Kwon, S.T.; Park, K.W.; Yeom, J.S.; Kang, H.S. Comparison of MR imaging findings between extraligamentous and subligamentous disk herniations in the lumbar spine. Ajnr. Am. J. Neuroradiol. 2013, 34, 683–687. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Williams, A.L.; Haughton, V.M.; Daniels, D.L.; Grogan, J.P. Differential CT diagnosis of extruded nucleus pulposus. Radiology 1983, 148, 141–148. [Google Scholar] [CrossRef] [PubMed]
- Ahn, Y.; Ahn, Y.; Jeong, T.S.; Jeong, T.S.; Lim, T.; Lim, T.; Jeon, J.Y.; Jeon, J.Y. Grading system for migrated lumbar disc herniation on sagittal magnetic resonance imaging: An agreement study. Neuroradiology 2018, 60, 101–107. [Google Scholar] [CrossRef] [PubMed]
- Holm, S.; Holm, A.K.; Ekstrom, L.; Karladani, A.; Hansson, T. Experimental disc degeneration due to endplate injury. J. Spinal Disord Tech. 2004, 17, 64–71. [Google Scholar] [CrossRef] [PubMed]
- Strube, P.; Pumberger, M.; Sonnow, L.; Zippelius, T.; Nowack, D.; Zahn, R.K.; Putzier, M. Association Between Lumbar Spinal Degeneration and Anatomic Pelvic Parameters. Clin. Spine Surg. 2018, 31, 263–267. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Wang, H.; Lv, F.; Ma, X.; Xia, X.; Jiang, J. Asymmetry between the superior and inferior endplates is a risk factor for lumbar disc degeneration. J. Orthop. Res. 2018, 36, 2469–2475. [Google Scholar] [CrossRef] [Green Version]
- Fei, H.; Li, W.S.; Sun, Z.R.; Ma, Q.W.; Chen, Z.Q. Analysis of Spino-pelvic Sagittal Alignment in Young Chinese Patients with Lumbar Disc Herniation. Orthop. Surg. 2017, 9, 271–276. [Google Scholar] [CrossRef] [Green Version]
- Bao, H.; Zhu, F.; Liu, Z.; Zhu, Z.; He, S.; Ding, Y.; Qiu, Y. Coronal Curvature and Spinal Imbalance in Degenerative Lumbar Scoliosis: Disc Degeneration Is Associated. Spine 2014, 39, E1441–E1447. [Google Scholar] [CrossRef]
- Panjabi, M.M. The stabilizing system of the spine. Part II. Neutral zone and instability hypothesis. J. Spinal Disord. 1992, 5, 390–396, discussion 397. [Google Scholar] [CrossRef]
- Cooley, J.R.; Walker, B.F.; Ardakani, E.M.; Kjaer, P.; Jensen, T.S.; Hebert, J.J. Relationships between paraspinal muscle morphology and neurocompressive conditions of the lumbar spine: A systematic review with meta-analysis. BMC Musculoskelet Disord. 2018, 19, 351. [Google Scholar] [CrossRef] [PubMed]
- Lee, G.W.; Lee, S.M.; Suh, B.G. The impact of generalized joint laxity on the occurrence and disease course of primary lumbar disc herniation. Spine J. 2015, 15, 65–70. [Google Scholar] [CrossRef] [PubMed]
- Han, W.J.; Kim, H.B.; Lee, G.W.; Choi, J.H.; Jo, W.J.; Lee, S.M. Generalized Joint Laxity is Associated with Primary Occurrence and Treatment Outcome of Lumbar Disc Herniation. Korean J. Fam. Med. 2015, 36, 141–145. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pesakova, L.; Hlavkova, J.; Nakladalova, M.; Urban, P.; Gadourek, P.; Tichy, T.; Borikova, A.; Lastovkova, A.; Pelclova, D. Exposure criteria for evaluating lumbar spine load. Cent. Eur. J. Public Health 2018, 26, 98–103. [Google Scholar] [CrossRef] [PubMed]
- Yang, S.; Kim, W.; Choi, K.H.; Yi, Y.G. Influence of occupation on lumbar spine degeneration in men: The Korean National Health and Nutrition Examination Survey 2010–2013. Int. Arch. Occup. Environ. Health 2016, 89, 1321–1328. [Google Scholar] [CrossRef] [PubMed]
- Illien-Junger, S.; Gantenbein-Ritter, B.; Grad, S.; Lezuo, P.; Ferguson, S.J.; Alini, M.; Ito, K. The combined effects of limited nutrition and high-frequency loading on intervertebral discs with endplates. Spine (Phila Pa 1976) 2010, 35, 1744–1752. [Google Scholar] [CrossRef]
- Junger, S.; Gantenbein-Ritter, B.; Lezuo, P.; Alini, M.; Ferguson, S.J.; Ito, K. Effect of limited nutrition on in situ intervertebral disc cells under simulated-physiological loading. Spine (Phila Pa 1976) 2009, 34, 1264–1271. [Google Scholar] [CrossRef]
- Gullbrand, S.E.; Peterson, J.; Ahlborn, J.; Mastropolo, R.; Fricker, A.; Roberts, T.T.; Abousayed, M.; Lawrence, J.P.; Glennon, J.C.; Ledet, E.H. ISSLS Prize Winner: Dynamic Loading-Induced Convective Transport Enhances Intervertebral Disc Nutrition. Spine (Phila Pa 1976) 2015, 40, 1158–1164. [Google Scholar] [CrossRef] [Green Version]
- Livshits, G.; Popham, M.; Malkin, I.; Sambrook, P.N.; Macgregor, A.J.; Spector, T.; Williams, F.M. Lumbar disc degeneration and genetic factors are the main risk factors for low back pain in women: The UK Twin Spine Study. Ann. Rheum. Dis. 2011, 70, 1740–1745. [Google Scholar] [CrossRef]
- Dario, A.B.; Ferreira, M.L.; Refshauge, K.M.; Lima, T.S.; Ordonana, J.R.; Ferreira, P.H. The relationship between obesity, low back pain, and lumbar disc degeneration when genetics and the environment are considered: A systematic review of twin studies. Spine J. 2015, 15, 1106–1117. [Google Scholar] [CrossRef]
- Simmons, E.D., Jr.; Guntupalli, M.; Kowalski, J.M.; Braun, F.; Seidel, T. Familial predisposition for degenerative disc disease. A case-control study. Spine (Phila Pa 1976) 1996, 21, 1527–1529. [Google Scholar] [CrossRef] [PubMed]
- Jakoi, A.M.; Pannu, G.; D’Oro, A.; Buser, Z.; Pham, M.H.; Patel, N.N.; Hsieh, P.C.; Liu, J.C.; Acosta, F.L.; Hah, R.; et al. The Clinical Correlations between Diabetes, Cigarette Smoking and Obesity on Intervertebral Degenerative Disc Disease of the Lumbar Spine. Asian Spine J. 2017, 11, 337–347. [Google Scholar] [CrossRef] [PubMed]
- Ngo, K.; Pohl, P.; Wang, D.; Leme, A.S.; Lee, J.; Di, P.; Roughley, P.; Robbins, P.D.; Niedernhofer, L.J.; Sowa, G.; et al. ADAMTS5 Deficiency Protects Mice From Chronic Tobacco Smoking-induced Intervertebral Disc Degeneration. Spine (Phila Pa 1976) 2017, 42, 1521–1528. [Google Scholar] [CrossRef] [PubMed]
- Elmasry, S.; Asfour, S.; de Rivero Vaccari, J.P.; Travascio, F. Effects of Tobacco Smoking on the Degeneration of the Intervertebral Disc: A Finite Element Study. PLoS ONE 2015, 10, e0136137. [Google Scholar] [CrossRef] [Green Version]
- Akmal, M.; Kesani, A.; Anand, B.; Singh, A.; Wiseman, M.; Goodship, A. Effect of nicotine on spinal disc cells: A cellular mechanism for disc degeneration. Spine (Phila Pa 1976) 2004, 29, 568–575. [Google Scholar] [CrossRef]
- Seyithanoglu, H.; Aydin, T.; Taspinar, O.; Camli, A.; Kiziltan, H.; Eris, A.H.; Hocaoglu, I.T.; Ozder, A.; Denizli, E.; Kepekci, M.; et al. Association between nutritional status and Modic classification in degenerative disc disease. J. Phys. Ther. Sci. 2016, 28, 1250–1254. [Google Scholar] [CrossRef] [Green Version]
- Chou, R.; Atlas, S.J.; Stanos, S.P.; Rosenquist, R.W. Nonsurgical interventional therapies for low back pain: A review of the evidence for an American Pain Society clinical practice guideline. Spine (Phila Pa 1976) 2009, 34, 1078–1093. [Google Scholar] [CrossRef]
- Luan, S.; Wan, Q.; Luo, H.; Li, X.; Ke, S.; Lin, C.; Wu, Y.; Wu, S.; Ma, C. Running exercise alleviates pain and promotes cell proliferation in a rat model of intervertebral disc degeneration. Int. J. Mol. Sci. 2015, 16, 2130–2144. [Google Scholar] [CrossRef]
- Steele, J.; Bruce-Low, S.; Smith, D.; Osborne, N.; Thorkeldsen, A. Can specific loading through exercise impart healing or regeneration of the intervertebral disc? Spine J. 2015, 15, 2117–2121. [Google Scholar] [CrossRef]
- Kim, S.; Kim, H.; Chung, J. Effects of Spinal Stabilization Exercise on the Cross-sectional Areas of the Lumbar Multifidus and Psoas Major Muscles, Pain Intensity, and Lumbar Muscle Strength of Patients with Degenerative Disc Disease. J. Phys. Ther. Sci. 2014, 26, 579–582. [Google Scholar] [CrossRef] [Green Version]
- Fujii, K.; Yamazaki, M.; Kang, J.D.; Risbud, M.V.; Cho, S.K.; Qureshi, S.A.; Hecht, A.C.; Iatridis, J.C. Discogenic Back Pain: Literature Review of Definition, Diagnosis, and Treatment. JBMR Plus 2019, 3, e10180. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dudli, S.; Sing, D.C.; Hu, S.S.; Berven, S.H.; Burch, S.; Deviren, V.; Cheng, I.; Tay, B.K.B.; Alamin, T.F.; Ith, M.A.M.; et al. ISSLS PRIZE IN BASIC SCIENCE 2017: Intervertebral disc/bone marrow cross-talk with Modic changes. Eur. Spine J. 2017, 26, 1362–1373. [Google Scholar] [CrossRef] [PubMed]
- Jensen, T.S.; Karppinen, J.; Sorensen, J.S.; Niinimaki, J.; Leboeuf-Yde, C. Vertebral endplate signal changes (Modic change): A systematic literature review of prevalence and association with non-specific low back pain. Eur. Spine J. 2008, 17, 1407–1422. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dudli, S.; Fields, A.; Samartzis, D.; Karppinen, J.; Lotz, J. Pathobiology of Modic changes. Eur. Spine J. 2016, 25, 3723–3734. [Google Scholar] [CrossRef] [PubMed]
- Schistad, E.I.; Espeland, A.; Rygh, L.J.; Roe, C.; Gjerstad, J. The association between Modic changes and pain during 1-year follow-up in patients with lumbar radicular pain. Skelet. Radiol 2014, 43, 1271–1279. [Google Scholar] [CrossRef]
- Jarvinen, J.; Karppinen, J.; Niinimaki, J.; Haapea, M.; Gronblad, M.; Luoma, K.; Rinne, E. Association between changes in lumbar Modic changes and low back symptoms over a two-year period. BMC Musculoskelet Disord. 2015, 16, 98. [Google Scholar] [CrossRef]
- Jensen, T.S.; Bendix, T.; Sorensen, J.S.; Manniche, C.; Korsholm, L.; Kjaer, P. Characteristics and natural course of vertebral endplate signal (Modic) changes in the Danish general population. BMC Musculoskelet Disord. 2009, 10, 81. [Google Scholar] [CrossRef] [Green Version]
- Liu, H.; Zhao, H.; Li, Z.; Xue, H.; Lu, J.; Ma, W. A common polymorphism of COMT was associated with symptomatic lumbar disc herniation based on a large sample with Chinese Han ancestry. Sci. Rep. 2018, 8, 13000. [Google Scholar] [CrossRef]
- Omair, A.; Lie, B.A.; Reikeras, O.; Holden, M.; Brox, J.I. Genetic contribution of catechol-O-methyltransferase variants in treatment outcome of low back pain: A prospective genetic association study. BMC Musculoskelet Disord. 2012, 13, 76. [Google Scholar] [CrossRef] [Green Version]
- Dai, F.; Belfer, I.; Schwartz, C.E.; Banco, R.; Martha, J.F.; Tighioughart, H.; Tromanhauser, S.G.; Jenis, L.G.; Kim, D.H. Association of catechol-O-methyltransferase genetic variants with outcome in patients undergoing surgical treatment for lumbar degenerative disc disease. Spine J. 2010, 10, 949–957. [Google Scholar] [CrossRef]
- Olmarker, K.; Blomquist, J.; Stromberg, J.; Nannmark, U.; Thomsen, P.; Rydevik, B. Inflammatogenic properties of nucleus pulposus. Spine (Phila Pa 1976) 1995, 20, 665–669. [Google Scholar] [CrossRef] [PubMed]
- Byrod, G.; Otani, K.; Brisby, H.; Rydevik, B.; Olmarker, K. Methylprednisolone reduces the early vascular permeability increase in spinal nerve roots induced by epidural nucleus pulposus application. J. Orthop. Res. Off. Publ. Orthop. Res. Soc. 2000, 18, 983–987. [Google Scholar] [CrossRef] [PubMed]
- Peng, B.; Hao, J.; Hou, S.; Wu, W.; Jiang, D.; Fu, X.; Yang, Y. Possible pathogenesis of painful intervertebral disc degeneration. Spine (Phila Pa 1976) 2006, 31, 560–566. [Google Scholar] [CrossRef] [PubMed]
- Krock, E.; Rosenzweig, D.H.; Chabot-Doré, A.J.; Jarzem, P.; Weber, M.H.; Ouellet, J.A.; Stone, L.S.; Haglund, L. Painful, degenerating intervertebral discs up-regulate neurite sprouting and CGRP through nociceptive factors. J. Cell. Mol. Med. 2014, 18, 1213–1225. [Google Scholar] [CrossRef]
- Risbud, M.V.; Shapiro, I.M. Role of cytokines in intervertebral disc degeneration: Pain and disc content. Nat. Rev. Rheumatol. 2014, 10, 44–56. [Google Scholar] [CrossRef]
- Bjorland, S.; Moen, A.; Schistad, E.; Gjerstad, J.; Røe, C. Genes associated with persistent lumbar radicular pain; a systematic review. BMC Musculoskelet. Disord. 2016, 17, 500. [Google Scholar] [CrossRef] [Green Version]
- Li, Y.R.; Hu, X.; Yang, B.Z. Studies on structural changes of collagen in silicosis. Biomed. Environ. Sci. Bes. 1994, 7, 302–306. [Google Scholar]
- Shinohara, H. [Lumbar disc lesion, with special reference to the histological significance of nerve endings of the lumbar discs]. Nihon Seikeigeka Gakkai Zasshi 1970, 44, 553–570. [Google Scholar]
- Edgar, M.A. The nerve supply of the lumbar intervertebral disc. J. Bone Jt. Surg Br. 2007, 89, 1135–1139. [Google Scholar] [CrossRef]
- Kojima, Y.; Maeda, T.; Arai, R.; Shichikawa, K. Nerve supply to the posterior longitudinal ligament and the intervertebral disc of the rat vertebral column as studied by acetylcholinesterase histochemistry. II. Regional differences in the distribution of the nerve fibres and their origins. J. Anat. 1990, 169, 247–255. [Google Scholar]
- Nakamura, S.; Takahashi, K.; Takahashi, Y.; Morinaga, T.; Shimada, Y.; Moriya, H. Origin of nerves supplying the posterior portion of lumbar intervertebral discs in rats. Spine (Phila Pa 1976) 1996, 21, 917–924. [Google Scholar] [CrossRef] [PubMed]
- Sekiguchi, Y.; Konnai, Y.; Kikuchi, S.; Sugiura, Y. An anatomic study of neuropeptide immunoreactivities in the lumbar dura mater after lumbar sympathectomy. Spine (Phila Pa 1976) 1996, 21, 925–930. [Google Scholar] [CrossRef] [PubMed]
- Cavanaugh, J.M.; Ozaktay, A.C.; Yamashita, T.; Avramov, A.; Getchell, T.V.; King, A.I. Mechanisms of low back pain: A neurophysiologic and neuroanatomic study. Clin. Orthop. Relat. Res. 1997, 335, 166–180. [Google Scholar] [CrossRef]
- Imai, S.; Hukuda, S.; Maeda, T. Dually innervating nociceptive networks in the rat lumbar posterior longitudinal ligaments. Spine (Phila Pa 1976) 1995, 20, 2086–2092. [Google Scholar] [CrossRef]
- Coppes, M.H.; Marani, E.; Thomeer, R.T.; Groen, G.J. Innervation of “painful” lumbar discs. Spine (Phila Pa 1976) 1997, 22, 2342–2349, discussion 2349–2350. [Google Scholar] [CrossRef]
- Ahmed, M.; Bjurholm, A.; Kreicbergs, A.; Schultzberg, M. Neuropeptide Y, tyrosine hydroxylase and vasoactive intestinal polypeptide-immunoreactive nerve fibers in the vertebral bodies, discs, dura mater, and spinal ligaments of the rat lumbar spine. Spine (Phila Pa 1976) 1993, 18, 268–273. [Google Scholar] [CrossRef]
- Morinaga, T.; Takahashi, K.; Yamagata, M.; Chiba, T.; Tanaka, K.; Takahashi, Y.; Nakamura, S.; Suseki, K.; Moriya, H. Sensory innervation to the anterior portion of lumbar intervertebral disc. Spine (Phila Pa 1976) 1996, 21, 1848–1851. [Google Scholar] [CrossRef]
- Manchikanti, L.; Singh, V.; Pampati, V.; Damron, K.S.; Barnhill, R.C.; Beyer, C.; Cash, K.A. Evaluation of the relative contributions of various structures in chronic low back pain. Pain Physician 2001, 4, 308–316. [Google Scholar]
- Schwarzer, A.C.; Aprill, C.N.; Derby, R.; Fortin, J.; Kine, G.; Bogduk, N. The prevalence and clinical features of internal disc disruption in patients with chronic low back pain. Spine (Phila Pa 1976) 1995, 20, 1878–1883. [Google Scholar] [CrossRef]
- Ashton, I.K.; Walsh, D.A.; Polak, J.M.; Eisenstein, S.M. Substance P in intervertebral discs. Binding sites on vascular endothelium of the human annulus fibrosus. Acta Orthop. Scand. 1994, 65, 635–639. [Google Scholar] [CrossRef]
- McCarthy, P.W.; Carruthers, B.; Martin, D.; Petts, P. Immunohistochemical demonstration of sensory nerve fibers and endings in lumbar intervertebral discs of the rat. Spine (Phila Pa 1976) 1991, 16, 653–655. [Google Scholar] [CrossRef] [PubMed]
- Peng, B.; Wu, W.; Hou, S.; Li, P.; Zhang, C.; Yang, Y. The pathogenesis of discogenic low back pain. J. Bone Jt. Surg Br. 2005, 87, 62–67. [Google Scholar] [CrossRef]
- Purmessur, D.; Freemont, A.J.; Hoyland, J.A. Expression and regulation of neurotrophins in the nondegenerate and degenerate human intervertebral disc. Arthritis Res. Ther. 2008, 10, R99. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fagan, A.; Moore, R.; Vernon Roberts, B.; Blumbergs, P.; Fraser, R. ISSLS prize winner: The innervation of the intervertebral disc: A quantitative analysis. Spine (Phila Pa 1976) 2003, 28, 2570–2576. [Google Scholar] [CrossRef]
- Ohtori, S.; Miyagi, M.; Inoue, G. Sensory nerve ingrowth, cytokines, and instability of discogenic low back pain: A review. Spine Surg. Relat. Res. 2018, 2, 11–17. [Google Scholar] [CrossRef] [Green Version]
- Kim, H.S.; Kashlan, O.N.; Singh, R.; Adsul, N.M.; Yong, Z.; Oh, S.W.; Noh, J.H.; Jang, I.T.; Oh, S.H. Percutaneous Transforaminal Endoscopic Radiofrequency Ablation of the Sinuvertebral Nerve in an Olympian with a Left L5 Pedicle/Pars Interarticularis Fracture–Associated Left L5-S1 Disk Desiccation. World Neurosurg X 2019, 3, 100032. [Google Scholar] [CrossRef] [PubMed]
- Choi, S.H.; Adsul, N.; Kim, H.S.; Jang, J.-S.; Jang, I.-T.; Oh, S.-H. Magnetic Resonance Imaging Undetectable Epiduroscopic Hotspot in Chronic Diskogenic Back Pain—Does Sinuvertebral Neuropathy Actually Exist? World Neurosurg. 2018, 110, 354–358. [Google Scholar] [CrossRef]
- Brown, M.F.; Hukkanen, M.V.; McCarthy, I.D.; Redfern, D.R.; Batten, J.J.; Crock, H.V.; Hughes, S.P.; Polak, J.M. Sensory and sympathetic innervation of the vertebral endplate in patients with degenerative disc disease. J. Bone Jt. Surg Br. 1997, 79, 147–153. [Google Scholar] [CrossRef]
- Bailey, J.F.; Liebenberg, E.; Degmetich, S.; Lotz, J.C. Innervation patterns of PGP 9.5-positive nerve fibers within the human lumbar vertebra. J. Anat. 2011, 218, 263–270. [Google Scholar] [CrossRef]
- Anderson, J.T.; Haas, A.R.; Percy, R.; Woods, S.T.; Ahn, U.M.; Ahn, N.U. Chronic Opioid Therapy After Lumbar Fusion Surgery for Degenerative Disc Disease in a Workers’ Compensation Setting. Spine (Phila Pa 1976) 2015, 40, 1775–1784. [Google Scholar] [CrossRef]
- Fras, C.; Kravetz, P.; Mody, D.R.; Heggeness, M.H. Substance P-containing nerves within the human vertebral body. an immunohistochemical study of the basivertebral nerve. Spine J. Soc. 2003, 3, 63–67. [Google Scholar] [CrossRef]
- Yong-Hing, K.; Kirkaldy-Willis, W.H. The pathophysiology of degenerative disease of the lumbar spine. Orthop. Clin. N. Am. 1983, 14, 491–504. [Google Scholar]
- Kumar, N.; Kumar, A.; Siddharth, M.S.; Sambhav, P.S.; Tan, J. Annulo-nucleoplasty using Disc-FX in the management of lumbar disc pathology: Early results. Int. J. Spine Surg. 2014, 8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Appleby, D.; Andersson, G.; Totta, M. Meta-analysis of the efficacy and safety of intradiscal electrothermal therapy (IDET). Pain Med. (MaldenMass.) 2006, 7, 308–316. [Google Scholar] [CrossRef]
- Urrutia, J.; Besa, P.; Campos, M.; Cikutovic, P.; Cabezon, M.; Molina, M.; Cruz, J.P. The Pfirrmann classification of lumbar intervertebral disc degeneration: An independent inter- and intra-observer agreement assessment. Eur. Spine J. Res. Soc. 2016, 25, 2728–2733. [Google Scholar] [CrossRef]
- Canbulat, N.; Oktenoglu, T.; Ataker, Y.; Sasani, M.; Ercelen, O.; Cerezci, O.; Suzer, T.; Ozer, A.F. A Rehabilitation Protocol for Patients with Lumbar Degenerative Disc Disease Treated with Posterior Transpedicular Dynamic Stabilization. Turk. Neurosurg 2017, 27, 426–435. [Google Scholar] [CrossRef] [Green Version]
- Khalil, J.G.; Smuck, M.; Koreckij, T.; Keel, J.; Beall, D.; Goodman, B.; Kalapos, P.; Nguyen, D.; Garfin, S. A prospective, randomized, multicenter study of intraosseous basivertebral nerve ablation for the treatment of chronic low back pain. Spine J. 2019, 19, 1620–1632. [Google Scholar] [CrossRef] [Green Version]
- Pfirrmann, C.W.; Metzdorf, A.; Zanetti, M.; Hodler, J.; Boos, N. Magnetic resonance classification of lumbar intervertebral disc degeneration. Spine (Phila Pa 1976) 2001, 26, 1873–1878. [Google Scholar] [CrossRef]
- Modic, M.T.; Steinberg, P.M.; Ross, J.S.; Masaryk, T.J.; Carter, J.R. Degenerative disk disease: Assessment of changes in vertebral body marrow with MR imaging. Radiology 1988, 166, 193–199. [Google Scholar] [CrossRef]
- Kim, H.S.; Paudel, B.; Jang, J.S.; Lee, K.; Oh, S.H.; Jang, I.T. Percutaneous Endoscopic Lumbar Discectomy for All Types of Lumbar Disc Herniations (LDH) Including Severely Difficult and Extremely Difficult LDH Cases. Pain Physician 2018, 21, E401–E408. [Google Scholar]
- Ruetten, S.; Komp, M.; Merk, H.; Godolias, G. Surgical treatment for lumbar lateral recess stenosis with the full-endoscopic interlaminar approach versus conventional microsurgical technique: A prospective, randomized, controlled study. J. Neurosurg. Spine 2009, 10, 476–485. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, H.-S.M.D.P.; Paudel, B.M.D.M.S.; Jang, J.-S.M.D.P.; Oh, S.-H.M.D.P.; Lee, S.B.E.; Park, J.E.B.S.; Jang, I.-T.M.D.P. Percutaneous Full Endoscopic Bilateral Lumbar Decompression of Spinal Stenosis through Uniportal-Contralateral Approach: Techniques and Preliminary Results. World Neurosurg. 2017, 103, 201–209. [Google Scholar] [CrossRef] [PubMed]
- Wu, P.H.; Kim, H.S.; Jang, I.-T. How I do it? Uniportal full endoscopic contralateral approach for lumbar foraminal stenosis with double crush syndrome. Acta Neurochir. 2019. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, H.S.; Adsul, N.; Kapoor, A.; Choi, S.H.; Kim, J.H.; Kim, K.J.; Bang, J.S.; Yang, K.H.; Han, S.; Lim, J.H.; et al. A Mobile Outside-in Technique of Transforaminal Lumbar Endoscopy for Lumbar Disc Herniations. J. Vis. Exp. JOVE 2018. [Google Scholar] [CrossRef] [Green Version]
- Yeung, A.T.; Yeung, C.A. Advances in endoscopic disc and spine surgery: Foraminal approach. Surg. Technol. Int. 2003, 11, 255–263. [Google Scholar]
- Schizas, C.; Theumann, N.; Burn, A.; Tansey, R.; Wardlaw, D.; Smith, F.W.; Kulik, G. Qualitative grading of severity of lumbar spinal stenosis based on the morphology of the dural sac on magnetic resonance images. Spine 2010, 35, 1919–1924. [Google Scholar] [CrossRef] [Green Version]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Age (Mean/Range) | 48 | 18–71 | |
|---|---|---|---|
| Sex (Male/Female) | 13 | 17 | |
| Diagnosis Types | |||
| Degenerative disc disease without protrusion | 4 | ||
| Spinal Stenosis | 12 | ||
| Degenerated Disc Protrysion | 14 | ||
| Follow up duration (Mean/Range) | 27 | 4–120 | |
| Types of Operation | 23 | ||
| Interlaminar Diac Approach | 23 | ||
| Interlaminar Stenosis Approach | 12 | ||
| Transforaminal Approach | 6 | ||
| Neovascularization Grade | 0 | ||
| Grade 1 | 0 | ||
| Grade 2 | 6 | ||
| Grade 3 | 24 | ||
| Modic Type | |||
| Type 1 | 24 | ||
| Type 2 | 6 | ||
| Schiaz Grade | |||
| Grade A1 | 25 | ||
| Grade A2 | 5 | ||
| Grade A3 | 1 | ||
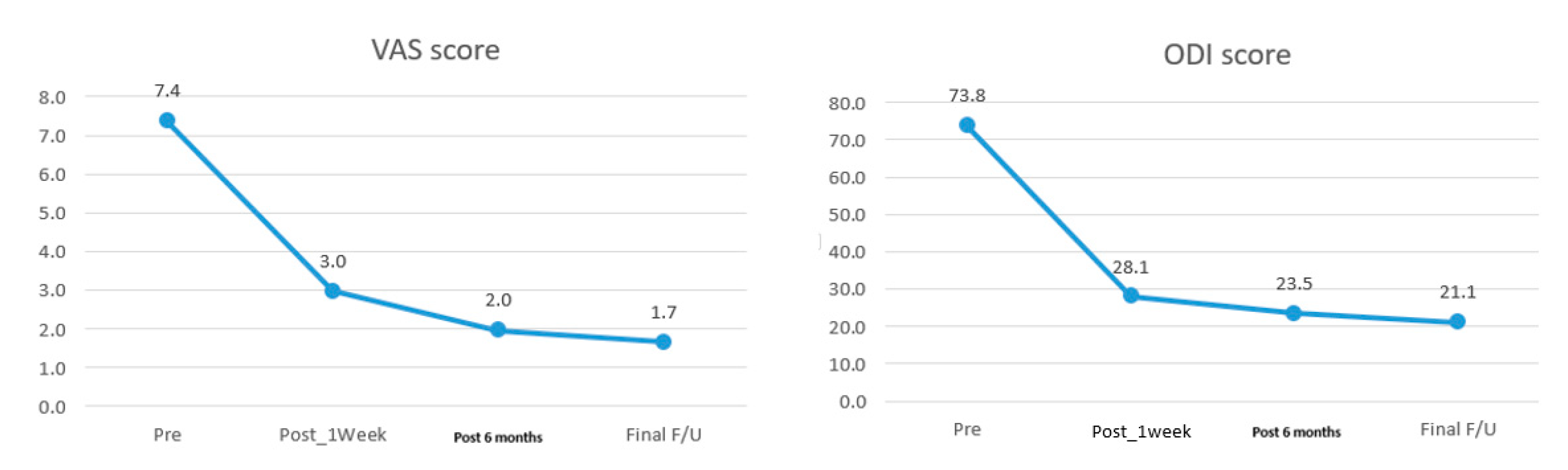
| Mean/SD VAS (Pre and Final) | 7.4 ± 0.7 | 1.7 ± 1.5 | p < 0.05 |
| Mean/SD ODI (Pre and Final) | 71.8 ± 1.88 | 20.8 ± 14.9 | p < 0.05 |
| MacNab Criteria | |||
| Fair | 2 | ||
| Good | 11 | ||
| Excellent | 17 | ||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, H.S.; Wu, P.H.; Jang, I.-T. Lumbar Degenerative Disease Part 1: Anatomy and Pathophysiology of Intervertebral Discogenic Pain and Radiofrequency Ablation of Basivertebral and Sinuvertebral Nerve Treatment for Chronic Discogenic Back Pain: A Prospective Case Series and Review of Literature. Int. J. Mol. Sci. 2020, 21, 1483. https://doi.org/10.3390/ijms21041483
Kim HS, Wu PH, Jang I-T. Lumbar Degenerative Disease Part 1: Anatomy and Pathophysiology of Intervertebral Discogenic Pain and Radiofrequency Ablation of Basivertebral and Sinuvertebral Nerve Treatment for Chronic Discogenic Back Pain: A Prospective Case Series and Review of Literature. International Journal of Molecular Sciences. 2020; 21(4):1483. https://doi.org/10.3390/ijms21041483
Chicago/Turabian StyleKim, Hyeun Sung, Pang Hung Wu, and Il-Tae Jang. 2020. "Lumbar Degenerative Disease Part 1: Anatomy and Pathophysiology of Intervertebral Discogenic Pain and Radiofrequency Ablation of Basivertebral and Sinuvertebral Nerve Treatment for Chronic Discogenic Back Pain: A Prospective Case Series and Review of Literature" International Journal of Molecular Sciences 21, no. 4: 1483. https://doi.org/10.3390/ijms21041483