1. Introduction
Modic changes (MCs) are MRI signal intensity features within vertebrae adjacent to degenerated intervertebral discs [
1,
2,
3]. There are three interconvertible types that are defined according to their appearance on T1-weighted and T2-weighted MR images [
2]. In a systematic review, the prevalence of MC in patients with chronic low back pain (cLBP) was 43% (in contrast to 6% in the non-clinical population) [
4] but varied greatly with geographic location. Generally, prevalence is lower in Asia (China and India: 10.9–22.4%) [
5,
6,
7] and Africa (Nigeria: 22.8%) [
8]. Prevalence increases with age and is most frequent at lower lumbar levels, i.e., L4/L5 and L5/S1 [
2,
9]. Endplate defects predict MC and suggest biomechanical aspects as important etiological parameters of MC [
3,
10].
MC have a high specificity for discography-concordant cLBP [
11]. In contrast to disc herniation, where nerve compression causes back and leg pain, MC pain is believed to arise from pathologic innervation in the endplate and vertebra [
11,
12,
13]. From a clinical population-based study, including 412 Danes, Kjaer et al. concluded that “MC in combination with disc degeneration is an entity on its own, which is different from disc degeneration without MC” [
14]. LBP patients with MC report a greater frequency and duration of LBP episodes, seek care more often and have a higher risk for a poor outcome [
4,
15,
16,
17,
18]. The larger the MC lesions, the lower the chance for resolution, and the higher the positive predictive value for pain in discography [
9,
19]. Therefore, early detection of MC may be important for informing clinical decisions and treatment monitoring [
20,
21,
22]. However, MC may be underdiagnosed in primary care because clinical guidelines recommend against routine spine MRI for “unspecific” cLBP. Serum biomarkers are a fast and inexpensive way to detect pathological conditions. A robust MC biomarker should reflect the pathophysiological processes (face validity).
MC have been described as inflammatory changes with fibrosis, increased vascular supply, and high bone turnover [
2,
10,
23,
24]. Discs adjacent to MCs degenerate at an increased rate and secrete higher levels of pro-inflammatory cytokines and aggrecanases [
10,
24,
25,
26,
27,
28]. No biomarkers for MC have yet been identified. Yet, a small French study reported elevated high-sensitivity C-reactive protein (hsCRP) in patients with Modic type 1 changes (MC1) [
29]. HsCRP is a non-specific marker for inflammation and hence not a robust biomarker. A recent study on 80 subjects investigated the concentrations of 46 serum cytokines between MC patients and healthy volunteers [
30]. Interestingly, 16 cytokines related to inflammation, bone turnover, angiogenesis, and vascular injury were downregulated in MC. In a case-control study, with 13 MC1 patients and 21 control cLBP patients without MC, Boisson et al. found no difference in serum markers of inflammation (interleukin (IL)-1β, IL-6, IL-8, tumor necrosis factor alpha (TNF-α)) [
31]. This stands in contrast to the current ideas about MC pathophysiology. Therefore, blood serum cytokines may have little face validity for MC. Blood biomarkers for oxidative stress (total thiols, advanced oxidation protein products, and carbonyl groups) in MC1 patients are inconclusive [
31,
32] and degradation markers for type II collagen (Coll2-1, Coll2-1NO
2), important disc collagen, were not elevated in MC1 patients [
31]. Taken together, these studies do not yet validate the concept of ‘active discopathy’, defined as an accelerated disc degeneration with low grade local and systemic inflammation [
33]. However, no study has yet investigated biomarkers related to bone marrow fibrosis, which is a histological hallmark of MC.
We aimed to detect biomarkers reflecting connective tissue and basement membrane turnover for MC that have high face validity. These biomarkers may relate to the rapid resorption of the adjacent disc and the fibrotic changes of the bone marrow. The disc matrix consists mainly of type I and II collagen, as well as aggrecan. Type III collagen is present only in traces in the pericellular environment of disc cells and type IV collagen is absent [
34,
35]. Therefore, resorption of the disc generates neo-epitopes of type I and II collagen and aggrecan. In myelofibrosis (a fibrotic condition of the bone marrow different from MC), type I and III collagen are the major deposited matrix constituents [
36]. Neovascularization of fibrotic bone marrow increases the spatial abundance of type IV collagen because type IV collagen is the main constituent of the basement membrane of vascular sinusoids [
37,
38]. Serum procollagen type III and IV are known to be increased in myelofibrosis [
39]. Therefore, biomarkers for type III and IV collagen, but not type I and II collagen and aggrecan, may relate to bone marrow fibrosis. In this current study, we quantified the association of nine matrix biomarkers related to disc resorption and bone marrow fibrosis (neo-epitopes of type I to IV pro-collagen (PRO-C1, PRO-C2, PRO-C3, PRO-C4), type I to IV collagen degradation neo-eiptopes (C1M, C2M, C3M, C4M, aggrecan degradation neo-epitope (huARGS)) to lumbar MC. Since a previous study reported no increase in type II collagen degradation markers [
31], we hypothesized that biomarkers related to bone marrow fibrosis are increased in MC.
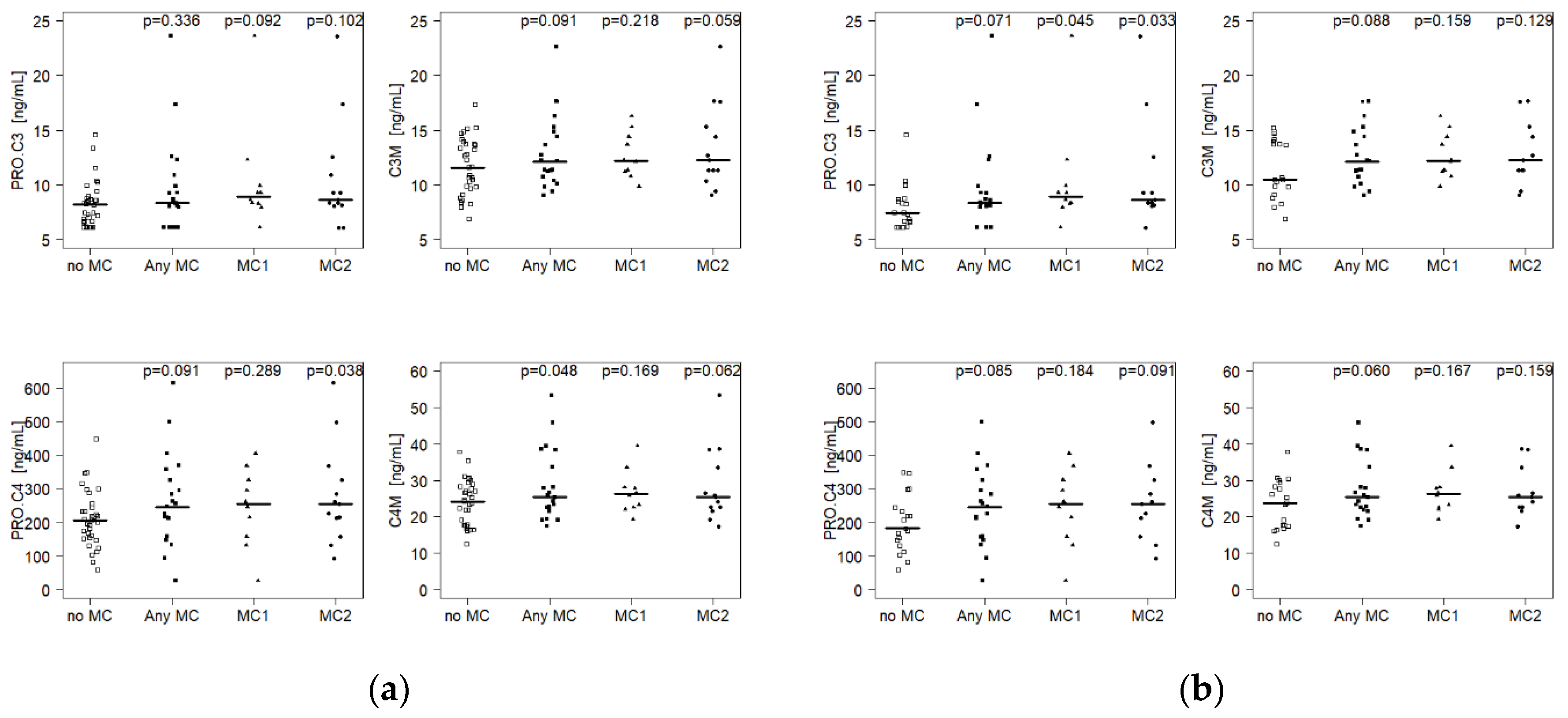
We observed that serum biomarkers related to the formation and degradation of type III (PRO-C3, C3M) and type IV collagen (PRO-C4, C4M), correlated with MC presence. This underscores that bone marrow fibrosis is an important pathophysiological process in MC, and suggests that it should be a focus in larger biomarker and treatment studies.
3. Discussion
We measured serum biomarkers of extracellular matrix turnover related to disc and bone marrow in subjects with and without MC and tested these biomarkers’ ability to predict MC. We found that biomarkers related to type III and IV collagen degradation (C3M and C4M, respectively) and formation (PRO-C3 and PRO-C4, respectively) correlated with the presence of MC in patients with cLBP (p = 0.060–0.088). PRO-C3 in combination with C4M had a moderate diagnostic value for MC in cLBP patients (AUC = 0.73, specificity = 78.9%, sensitivity = 73.7%).
These results agree with the pathomolecular mechanism of MC, in particular MC1, where bone marrow fibrosis has been described [
2,
10]. Type III and IV collagen are key bone marrow matrix constituents and known to be increased in bone marrow fibrosis [
36]. From biomarker studies of other fibrotic diseases, including myelofibrosis, it is likely that an increase of PRO-C3 correlates with an increased type III collagen deposition. An increased C4M (and in some analysis PRO-C4) indicates a remodeling of tissue vascularization as type IV collagen is an important basement membrane constituent. This is in agreement with previous reports of decreased pro-angiogenic serum cytokines in MC patients, i.e., vascular endothelial growth factor (VEGF)-C, VEGF-D, tyrosine-protein kinase receptor 2 (Tie-2), VEGF receptor 1 (Flt-1), intercellular adhesion molecule 1 (ICAM-1), vascular cell adhesion molecule 1 (VCAM-1) [
30]. Biomarkers related to disc degradation were not increased (C1M, C2M, huARGS), indicating that disc resorption is not a specific mechanistic target for MC, as previously reported [
31].
Bone marrow fibrosis and accelerated disc degeneration are hallmarks of MC [
2,
3,
10,
11,
33]. Extracellular matrix biomarkers related to these processes could be valuable in detecting MC at an early stage of the typically long treatment history of cLBP patients. In this study, we found that circulating biomarkers related to bone marrow fibrosis (PRO-C3, C3M, PRO-C4, C4M) but not to disc degeneration (C1M, C2M, huARGS) were increased in cLBP patients with MC. Our statistical models with the highest diagnostic accuracy for MC were combinations of PRO-C3 with PRO-C4, C3M or C4M, depending on the type of MC. Correlation analysis between the different biomarkers showed that PRO-C4, C3M, and C4M correlate significantly with each other, and hence, combining C3M, and C4M did not enhance diagnostic value. PRO-C3 did not correlate with PRO-C4, C3M, and C4M, and, therefore, the combination of PRO-C3 with any of the other three biomarkers increases the diagnostic value. The best model in this study for AnyMC in cLBP patients was PROC3 + C4M and reached a moderate diagnostic value with an AUC = 0.73. While this is not satisfactory for clinical usage, the correlation of fibrosis-related serum biomarkers with MC indicates that bone marrow fibrosis is an active process in MC. Marrow fibrosis in MC has been mainly associated with MC1 but not MC2 [
2,
10]. Interestingly, we found significantly increased serum concentrations of PRO-C4 and PRO-C3 in subjects with MC2. The model PRO-C3 + PRO-C4 had a classification accuracy for MC2 with an AUC = 0.75 and a sensitivity of 100%. This suggests that bone marrow fibrosis is also a relevant pathomechanism in MC2. Histopathological studies of MC2 bone marrow will have to corroborate the fibrotic mechanisms in MC2.
The biomarkers PRO-C3, PRO-C4, C3M, and C4M that correlate with MC have been identified as markers for other fibrotic conditions. In myelofibrosis, a myeloproliferative and fibrotic disease of the bone marrow, serum PRO-C3 and PRO-C4 have already been described as potential biomarkers that correlate with increased type III and IV collagen in the bone marrow [
36,
37,
38,
39,
40]. PRO-C4 has been identified as a serum marker to predict the progression of systemic sclerosis [
41]. PRO-C3 has been suggested as a biomarker for several pathologies related to tissue fibrosis such as lung injury, viral and non-viral hepatitis, systemic sclerosis, vascular remodeling, and kidney diseases [
42]. The epitope recognized by the PRO-C3 assay is generated by cleaving intact procollagen type III. The cleaved
N-terminal fragment is liberated into the systemic level and measured in the blood serum. Hence, PRO-C3 correlates stoichiometrically with type III collagen formation.
The type IV collagen neoepitope C4M is increased in idiopathic pulmonary fibrosis, chronic obstructive pulmonary disease, and liver fibrosis [
43]. The epitope recognized by the C4M assay is exposed when matrix metalloproteinase-2 and -9 (MMP-2, MMP-9) cleave intact type IV collagen, a major component of the basement membranes, including basement membranes from vascular sinusoids in the bone marrow. The activity of the gelatinases MMP-2 and -9 is locally increased in fibrotic tissue and disrupts the basement membrane, and allows the infiltration of fibroblasts and macrophage. Similarly, the type III collagen neoepitope C3M is exposed when MMP-9 cleaves intact type III collagen. C3M is a biomarker for liver fibrosis [
44]. The specificity of these biomarkers for local fibrotic pathomechanisms grants them a high test and content validity for fibrotic disorders. Our data suggest that turnover of type III and IV collagen is increased in patients with MC and that increased serum concentrations could relate to MC because these patients were not known to have other fibrotic disorders.
Serum cytokines related to inflammation, bone turnover, angiogenesis, and vascular injury have recently been investigated as MC biomarkers [
21,
30,
31]. However, no correlations were found with local pathophysiological processes. Therefore, these cytokines only have limited test validity. Cytokines have an average half-life in the range of minutes to hours [
45], which allows the human body to react with a fast and dynamic cytokine response. Consequently, serum cytokine levels are very dynamic. In contrast, collagens are by the nature of their function thermodynamically very stable. For example, collagens of human intervertebral discs have an average half-life of 95–215 years [
46]. Although collagen fragments may have a reduced half-life compared to intact collagen, they are more stable biomarkers than cytokines and are less affected by the diurnal cycle, food intake, and other acute events. In MC, inflammation is indicated by the edema seen on fat-saturated T2-weighted and on T1-weighted MR images. Yet, there is no direct evidence of inflammation in MC bone marrow [
10]. Discs adjacent to MC were reported to secrete higher levels of inflammatory cytokines [
10,
24,
26,
27]. However, degenerated discs contain very few cells (<1 Mio) [
47], and a small increase of inflammatory cytokine secretion is not detected on a systemic level, with no positive correlations with presence and size of MC [
21].
The clinical relevance of MC is controversial [
48,
49]. Variability in the identification, classification, and reporting of MC contribute to discrepancies between study findings [
50]. Besides known methodological factors related to imaging, time-varying changes in MC pathophysiology may contribute to the inconsistent findings. For example, fibrosis and bone resorption/high bone turnover are both hallmarks of MC [
2,
10,
23]. These processes may occur in distinct phases. Therefore, serum biomarkers for bone marrow fibrosis, i.e., for PRO-C3, PRO-C4, and C4M, may not only help to detect MC but also help to stratify patients into a “fibrotic phase” and an “inflammatory bone resorption phase”. This could potentially inform treatment decisions and monitoring.
This study had several limitations. It was a single-site study with 54 participants with only 10 cLBP patients with MC1 and 11 cLBP patients with MC2. Variation in all biomarker concentration was high (Cohen’s d < 0.61 for AnyMC vs. no MC). Therefore, posthoc power analysis resulted in low power (power < 0.47). Despite the low power, differences in type III and IV collagen turnover suggest bone marrow fibrosis as a relevant MC pathomechanism. However, these findings need to be validated in independent cohorts. Given the limited number, it is important to note that there was no difference in gender, age, and BMI between patients and the control group and between subjects with and without MC. Nevertheless, results should be interpreted carefully and not over-generalized. The small participant number also limited the construction of more powerful statistical models. For example, including available patient data (sex, age, BMI) in biomarker models may improve the diagnostic accuracy. In order to avoid overfitting, we limited construct complexity to two biomarkers. Patient data were not included because they did not correlate with the presence of lumbar MC in our sample. Despite the limited data, fibrosis-related biomarkers were consistently upregulated and allowed for careful interpretation.
The causal relationship of serum type III and IV collagen with the pathological mechanism of MC remains unknown. Low local inflammation, as well as altered biomechanical loads, may both be factors contributing to bone marrow fibrosis. Clarification of these relationships requires cross-sectional histological studies as well as longitudinal studies that investigate the correlation of these biomarkers with MC progression and clinical parameters.
Bone marrow lesions (BML) in osteoarthritic joints share many characteristics with MC1, including pain association, natural history, local inflammation, and degradation of the adjacent cartilage [
47]. Therefore, assessing biomarkers for type III and IV collagen in patients with osteoarthritic BML will gauge their specificity for MC and indicate pathomechanistic similarities between MC and BML in osteoarthritic joints.
MC size, type, and number may also affect serum biomarker concentration. In this current study, a correlation analysis of the number of MC lesions with serum biomarker concentrations revealed no significance.
Six patients had both MC1 and MC2, and some MC were of mixed type. Subgroup analysis for MC1 and MC2 showed similar biomarker trends. Nevertheless, MC1 and MC2 present different stages of the pathomechanism and have different histological features [
2,
10,
11]. Therefore, larger, longitudinal studies are required in order to define accurate biomarkers for MC1 and MC2.

 ,
, 
{kind=link}
