
Hereditary Diffuse Gastric Cancer: Molecular Genetics, Biological Mechanisms and Current Therapeutic Approaches

Abstract
:1. Introduction
2. Molecular Genetics and Histopathological Alterations in HDGC
2.1. Driving Mutations and Cancer-Predisposing Genes for HDGC
2.2. Spectrum of CDH1 Germline Variants
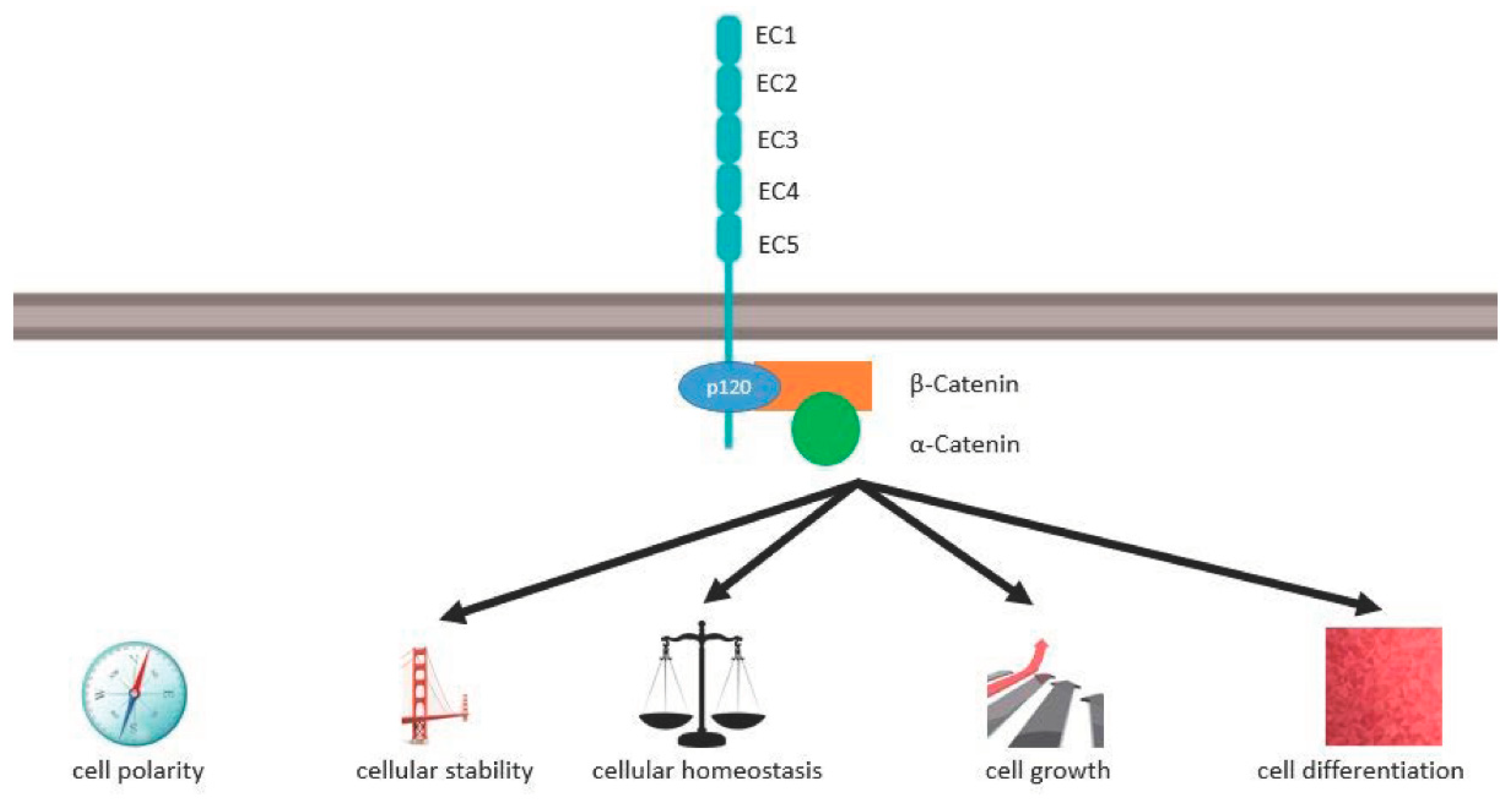
2.3. E-Cadherin Structure, Molecular Function, and Signal Pathways in Cancer

{kind=link}
| Genes | Corresponding Proteins | Cancers in Which the Related Genes Express | Encoded Functions | Reference |
|---|---|---|---|---|
| CDH1 | E-cadherin | Gastric cancer (diffuse type including HDGC), lobular breast cancer, colorectal cancer, hepatocellular carcinoma, squamous cell carcinomas of the skin, neck, and head, esophageal carcinoma, pancreatic ductal adenocarcinoma | Tumor suppressor and adhesion, adhesion in cell-cell contact | [4,10,11,13,14,15,18,24,25,26,27,28,29,30,31,32,33,34,35,38,39,40,41,42,43,44,45,46,47,48] |
| CTNNA1 | Alpha E-cadherin | HDGC (HDGC without CDH1-mutation, as well), diffuse type GC and colorectal cancer | Tumor suppressor and adhesion, adhesion in cell-cell contact | [16,19,20] |
| MAP3K6 | A serine/threonine protein kinase | HDGC, diffuse and intestinal type GC | Tumor suppressor | [24,25] |
| BRCA1, PALB2, RAD51C | Corresponding Proteins on their own | HDGC, breast cancer, pancreatic cancer, pancreatic ductal adenocarcinoma | Regulate homologous DNA recombination | [16,17,18] |
| DOT1L | Histone Methyltransferase | DGC | Effect on DNA Repair | [17,24] |
| MSH2 | Codes for a DNA mismatch repair (MMR) protein | Hereditary nonpolyposis colorectal cancer (HNPCC) HDGC diffuse and intestinal type gastric cancer | Component of the post-replicative DNA mismatch repair system (MMR) | [16,17,18] |
| MET | A protein with an extracellular, transmembrane and a tyrosine kinase domain | Gastric cancer (intestinal and diffuse type, including HDGC, breast-, prostate-, ovarian- cancer, hereditary papillary renal carcinoma | Functions in cellular survival, embryogenesis, cellular migration, and invasion | [26] |
| CD44 | A cell-surface glycoprotein | Hyperplastic polyps, intestinal metaplasia, gastric cancer (intestinal and diffuse type, including HDGC) | Cell surface glycoprotein | [27] |
| INSR | Receptor tyrosine kinase | HDGC | Effect on tumor cell invasion | [17] |
| FBXO24 | F-box protein | DGC | Tumor driver | [17] |
2.4. Other Contributing Risk Factors for HDGC
2.5. Histological Alterations in CDH1 Gene Mutation
3. Implications of CDH1 Gene Alterations in the Diagnosis and Management of HDGC
3.1. IGCLC Diagnostic Criteria for HDGC Syndrome
3.2. Genetic Counseling and Genetic Testing for HDGC Syndrome
3.3. Management of CDH1 Mutation Gene Carriers
3.4. Therapy Strategies for HDGC
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| ACMG | American College of Medical Genetics and Genomics |
| AMP | Association for Molecular Pathology |
| APC | adenomatous polyposis coli |
| ATM | ataxia telangiectasia mutated gene |
| BRCA2 | breast cancer gene 2 |
| CDH1 | cadherin-1 or E-cadherin |
| CMA | chromosomal microarray analysis |
| CTNNA1 | catenin alpha-1 |
| DNA | deoxyribonucleic acid |
| DGC | diffuse gastric cancer |
| HDGC | hereditary diffuse gastric cancer |
| HNPCC | hereditary nonpolyposis colorectal cancer |
| IGCLC | international gastric cancer linkage consortium |
| LBC | lobular breast cancer |
| MGPT | multiplex genetic panel testing |
| MPLA | multiplex ligation-dependent probe amplification |
| OR | odds ratio |
| PALB2 | partner and localizer of BRCA2 |
| PCR | polymerase chain reaction |
| PTG | prophylactic total gastrectomy |
| RNA | ribonucleic acid |
| SRC | signet-ring cells |
| StoP | stomach cancer pooling project |
| TP53 | tumor protein 53 |
References
- Guilford, P.; Hopkins, J.; Harraway, J.; McLeod, M.; McLeod, N.; Harawira, P.; Taite, H.; Scoular, R.; Miller, A.; Reeve, A.E. E-Cadherin Germline Mutations in Familial Gastric Cancer. Nature 1998, 392, 402–405. [Google Scholar] [CrossRef] [PubMed]
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: Globocan Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA A Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Fitzgerald, R.C.; Hardwick, R.; Huntsman, D.; Carneiro, F.; Guilford, P.; Blair, V.; Chung, D.C.; Norton, J.; Ragunath, K.; Van Krieken, J.H.; et al. Hereditary Diffuse Gastric Cancer: Updated Consensus Guidelines for Clinical Management and Directions for Future Research. J. Med. Genet. 2010, 47, 436–444. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hansford, S.; Kaurah, P.; Li-Chang, H.; Woo, M.; Senz, J.; Pinheiro, H.; Schrader, K.A.; Schaeffer, D.F.; Shumansky, K.; Zogopoulos, G.; et al. Hereditary Diffuse Gastric Cancer Syndrome: CDH1 Mutations and Beyond. JAMA Oncol. 2015, 1, 23–32. [Google Scholar] [CrossRef] [Green Version]
- Wang, Z.; Graham, D.Y.; Khan, A.; Balakrishnan, M.; Abrams, H.R.; El-Serag, H.B.; Thrift, A.P. Incidence of Gastric Cancer in the USA during 1999 to 2013: A 50-State Analysis. Int. J. Epidemiol. 2018, 47, 966–975. [Google Scholar] [CrossRef]
- Rona, K.A.; Schwameis, K.; Zehetner, J.; Samakar, K.; Green, K.; Samaan, J.; Sandhu, K.; Bildzukewicz, N.; Katkhouda, N.; Lipham, J.C. Gastric Cancer in the Young: An Advanced Disease with Poor Prognostic Features. J. Surg. Oncol. 2017, 115, 371–375. [Google Scholar] [CrossRef]
- Lecuit, T.; Yap, A.S. E-Cadherin Junctions as Active Mechanical Integrators in Tissue Dynamics. Nat. Cell Biol. 2015, 17, 533–539. [Google Scholar] [CrossRef]
- Blair, V.R.; McLeod, M.; Carneiro, F.; Coit, D.G.; D’Addario, J.L.; van Dieren, J.M.; Harris, K.L.; Hoogerbrugge, N.; Oliveira, C.; van der Post, R.S.; et al. Hereditary Diffuse Gastric Cancer: Updated Clinical Practice Guidelines. Lancet Oncol. 2020, 21, e386–e397. [Google Scholar] [CrossRef]
- Kaurah, P.; MacMillan, A.; Boyd, N.; Senz, J.; De Luca, A.; Chun, N.; Suriano, G.; Zaor, S.; Van Manen, L.; Gilpin, C.; et al. Founder and Recurrent CDH1 Mutations in Families with Hereditary Diffuse Gastric Cancer. JAMA 2007, 297, 2360–2372. [Google Scholar] [CrossRef] [Green Version]
- van der Post, R.S.; Vogelaar, I.P.; Carneiro, F.; Guilford, P.; Huntsman, D.; Hoogerbrugge, N.; Caldas, C.; Schreiber, K.E.C.; Hardwick, R.H.; Ausems, M.G.E.M.; et al. Hereditary Diffuse Gastric Cancer: Updated Clinical Guidelines with an Emphasis on Germline CDH1 Mutation Carriers. J. Med. Genet. 2015, 52, 361–374. [Google Scholar] [CrossRef] [Green Version]
- van der Post, R.S.; Gullo, I.; Oliveira, C.; Tang, L.H.; Grabsch, H.I.; O’Donovan, M.; Fitzgerald, R.C.; van Krieken, H.; Carneiro, F. Histopathological, Molecular, and Genetic Profile of Hereditary Diffuse Gastric Cancer: Current Knowledge and Challenges for the Future. Adv. Exp. Med. Biol. 2016, 908, 371–391. [Google Scholar] [CrossRef] [PubMed]
- Hallowell, N.; Badger, S.; Richardson, S.; Caldas, C.; Hardwick, R.H.; Fitzgerald, R.C.; Lawton, J. High-Risk Individuals’ Perceptions of Reproductive Genetic Testing for CDH1 Mutations. Fam. Cancer 2017, 16, 531–535. [Google Scholar] [CrossRef] [PubMed]
- Luo, W.; Fedda, F.; Lynch, P.; Tan, D. CDH1 Gene and Hereditary Diffuse Gastric Cancer Syndrome: Molecular and Histological Alterations and Implications for Diagnosis And Treatment. Front. Pharmacol. 2018, 9, 1421. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Benusiglio, P.R.; Malka, D.; Rouleau, E.; De Pauw, A.; Buecher, B.; Noguès, C.; Fourme, E.; Colas, C.; Coulet, F.; Warcoin, M.; et al. CDH1 Germline Mutations and the Hereditary Diffuse Gastric and Lobular Breast Cancer Syndrome: A Multicentre Study. J. Med. Genet. 2013, 50, 486–489. [Google Scholar] [CrossRef]
- Majewski, I.J.; Kluijt, I.; Cats, A.; Scerri, T.S.; de Jong, D.; Kluin, R.J.C.; Hansford, S.; Hogervorst, F.B.L.; Bosma, A.J.; Hofland, I.; et al. An α-E-Catenin (CTNNA1) Mutation in Hereditary Diffuse Gastric Cancer. J. Pathol. 2013, 229, 621–629. [Google Scholar] [CrossRef]
- Donner, I.; Kiviluoto, T.; Ristimäki, A.; Aaltonen, L.A.; Vahteristo, P. Exome Sequencing Reveals Three Novel Candidate Predisposition Genes for Diffuse Gastric Cancer. Fam. Cancer 2015, 14, 241–246. [Google Scholar] [CrossRef]
- Fewings, E.; Larionov, A.; Redman, J.; Goldgraben, M.A.; Scarth, J.; Richardson, S.; Brewer, C.; Davidson, R.; Ellis, I.; Evans, D.G.; et al. Germline Pathogenic Variants in PALB2 and Other Cancer-Predisposing Genes in Families with Hereditary Diffuse Gastric Cancer without CDH1 Mutation: A Whole-Exome Sequencing Study. Lancet Gastroenterol. Hepatol. 2018, 3, 489–498. [Google Scholar] [CrossRef] [Green Version]
- Benusiglio, P.R.; Colas, C.; Guillerm, E.; Canard, A.; Delhomelle, H.; Warcoin, M.; Bellanger, J.; Eyries, M.; Zizi, M.; Netter, J.; et al. Clinical Implications of CTNNA1 Germline Mutations in Asymptomatic Carriers. Gastric Cancer 2019, 22, 899–903. [Google Scholar] [CrossRef] [Green Version]
- Clark, D.F.; Michalski, S.T.; Tondon, R.; Nehoray, B.; Ebrahimzadeh, J.; Hughes, S.K.; Soper, E.R.; Domchek, S.M.; Rustgi, A.K.; Pineda-Alvarez, D.; et al. Loss-of-Function Variants in CTNNA1 Detected on Multigene Panel Testing in Individuals with Gastric or Breast Cancer. Genet. Med. 2020, 22, 840–846. [Google Scholar] [CrossRef] [Green Version]
- Sahasrabudhe, R.; Lott, P.; Bohorquez, M.; Toal, T.; Estrada, A.P.; Suarez, J.J.; Brea-Fernández, A.; Cameselle-Teijeiro, J.; Pinto, C.; Ramos, I.; et al. Germline Mutations in PALB2, BRCA1, and RAD51C, Which Regulate DNA Recombination Repair, in Patients With Gastric Cancer. Gastroenterology 2017, 152, 983–986. [Google Scholar] [CrossRef] [Green Version]
- Carvajal-Carmona, L.G. PALB2 as a Familial Gastric Cancer Gene: Is the Wait Over? Lancet Gastroenterol. Hepatol. 2018, 3, 451–452. [Google Scholar] [CrossRef] [Green Version]
- Alexandrov, L.B.; Nik-Zainal, S.; Siu, H.C.; Leung, S.Y.; Stratton, M.R. A Mutational Signature in Gastric Cancer Suggests Therapeutic Strategies. Nat. Commun. 2015, 6, 8683. [Google Scholar] [CrossRef] [Green Version]
- Berx, G.; Becker, K.F.; Höfler, H.; van Roy, F. Mutations of the Human E-Cadherin (CDH1) Gene. Hum. Mutat. 1998, 12, 226–237. [Google Scholar] [CrossRef]
- Melo, S.; Figueiredo, J.; Fernandes, M.S.; Gonçalves, M.; Morais-de-Sá, E.; Sanches, J.M.; Seruca, R. Predicting the Functional Impact of CDH1 Missense Mutations in Hereditary Diffuse Gastric Cancer. Int. J. Mol. Sci. 2017, 18, 2687. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, D.; Lo, W.; Rudloff, U. Merging Perspectives: Genotype-Directed Molecular Therapy for Hereditary Diffuse Gastric Cancer (HDGC) and E-Cadherin-EGFR Crosstalk. Clin. Transl. Med. 2018, 7, 7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oliveira, C.; Pinheiro, H.; Figueiredo, J.; Seruca, R.; Carneiro, F. E-Cadherin Alterations in Hereditary Disorders with Emphasis on Hereditary Diffuse Gastric Cancer. Prog. Mol. Biol. Transl. Sci. 2013, 116, 337–359. [Google Scholar] [CrossRef] [PubMed]
- Figueiredo, J.; Söderberg, O.; Simões-Correia, J.; Grannas, K.; Suriano, G.; Seruca, R. The Importance of E-Cadherin Binding Partners to Evaluate the Pathogenicity of E-Cadherin Missense Mutations Associated to HDGC. Eur. J. Hum. Genet. 2013, 21, 301–309. [Google Scholar] [CrossRef] [Green Version]
- Oliveira, C.; Sousa, S.; Pinheiro, H.; Karam, R.; Bordeira-Carriço, R.; Senz, J.; Kaurah, P.; Carvalho, J.; Pereira, R.; Gusmão, L.; et al. Quantification of Epigenetic and Genetic 2nd Hits in CDH1 during Hereditary Diffuse Gastric Cancer Syndrome Progression. Gastroenterology 2009, 136, 2137–2148. [Google Scholar] [CrossRef] [PubMed]
- Grady, W.M.; Willis, J.; Guilford, P.J.; Dunbier, A.K.; Toro, T.T.; Lynch, H.; Wiesner, G.; Ferguson, K.; Eng, C.; Park, J.G.; et al. Methylation of the CDH1 Promoter as the Second Genetic Hit in Hereditary Diffuse Gastric Cancer. Nat. Genet. 2000, 26, 16–17. [Google Scholar] [CrossRef]
- Oliveira, C.; de Bruin, J.; Nabais, S.; Ligtenberg, M.; Moutinho, C.; Nagengast, F.M.; Seruca, R.; van Krieken, H.; Carneiro, F. Intragenic Deletion of CDH1 as the Inactivating Mechanism of the Wild-Type Allele in an HDGC Tumour. Oncogene 2004, 23, 2236–2240. [Google Scholar] [CrossRef] [Green Version]
- Figueiredo, J.; Melo, S.; Carneiro, P.; Moreira, A.M.; Fernandes, M.S.; Ribeiro, A.S.; Guilford, P.; Paredes, J.; Seruca, R. Clinical Spectrum and Pleiotropic Nature of CDH1 Germline Mutations. J. Med. Genet. 2019, 56, 199–208. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oliveira, C.; Senz, J.; Kaurah, P.; Pinheiro, H.; Sanges, R.; Haegert, A.; Corso, G.; Schouten, J.; Fitzgerald, R.; Vogelsang, H.; et al. Germline CDH1 Deletions in Hereditary Diffuse Gastric Cancer Families. Hum. Mol. Genet. 2009, 18, 1545–1555. [Google Scholar] [CrossRef] [PubMed]
- Kluijt, I.; Siemerink, E.J.M.; Ausems, M.G.E.M.; van Os, T.A.M.; de Jong, D.; Simões-Correia, J.; van Krieken, J.H.; Ligtenberg, M.J.; Figueiredo, J.; van Riel, E.; et al. CDH1-Related Hereditary Diffuse Gastric Cancer Syndrome: Clinical Variations and Implications for Counseling. Int. J. Cancer 2012, 131, 367–376. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lo, W.; Zhu, B.; Sabesan, A.; Wu, H.-H.; Powers, A.; Sorber, R.A.; Ravichandran, S.; Chen, I.; McDuffie, L.A.; Quadri, H.S.; et al. Associations of CDH1 Germline Variant Location and Cancer Phenotype in Families with Hereditary Diffuse Gastric Cancer (HDGC). J. Med. Genet. 2019, 56, 370–379. [Google Scholar] [CrossRef]
- Yu, W.; Yang, L.; Li, T.; Zhang, Y. Cadherin Signaling in Cancer: Its Functions and Role as a Therapeutic Target. Front. Oncol. 2019, 9, 989. [Google Scholar] [CrossRef] [PubMed]
- Biswas, K.H. Molecular Mobility-Mediated Regulation of E-Cadherin Adhesion. Trends Biochem. Sci. 2020, 45, 163–173. [Google Scholar] [CrossRef] [PubMed]
- Rasool, S.; Geethakumari, A.M.; Biswas, K.H. Role of Actin Cytoskeleton in E-Cadherin-Based Cell–Cell Adhesion Assembly and Maintenance. J. Indian Inst. Sci. 2021, 101, 51–62. [Google Scholar] [CrossRef]
- Gloushankova, N.A.; Rubtsova, S.N.; Zhitnyak, I.Y. Cadherin-Mediated Cell-Cell Interactions in Normal and Cancer Cells. Tissue Barriers 2017, 5, e1356900. [Google Scholar] [CrossRef] [Green Version]
- Lobo, S.; Benusiglio, P.R.; Coulet, F.; Boussemart, L.; Golmard, L.; Spier, I.; Hüneburg, R.; Aretz, S.; Colas, C.; Oliveira, C. Cancer Predisposition and Germline CTNNA1 Variants. Eur. J. Med. Genet. 2021, 64, 104316. [Google Scholar] [CrossRef]
- Bernegger, S.; Jarzab, M.; Wessler, S.; Posselt, G. Proteolytic Landscapes in Gastric Pathology and Cancerogenesis. Int. J. Mol. Sci. 2022, 23, 2419. [Google Scholar] [CrossRef]
- Kourtidis, A.; Lu, R.; Pence, L.J.; Anastasiadis, P.Z. A Central Role for Cadherin Signaling in Cancer. Exp. Cell Res. 2017, 358, 78–85. [Google Scholar] [CrossRef] [PubMed]
- Kaszak, I.; Witkowska-Piłaszewicz, O.; Niewiadomska, Z.; Dworecka-Kaszak, B.; Ngosa Toka, F.; Jurka, P. Role of Cadherins in Cancer—A Review. Int. J. Mol. Sci. 2020, 21, 7624. [Google Scholar] [CrossRef] [PubMed]
- Mendonsa, A.M.; Na, T.-Y.; Gumbiner, B.M. E-Cadherin in Contact Inhibition and Cancer. Oncogene 2018, 37, 4769–4780. [Google Scholar] [CrossRef] [PubMed]
- Cureus | Significance of E-Cadherin Gene Mutations in Patients With Hereditary Diffuse Gastric Cancer Syndrome: A Systematic Review. Available online: https://www.cureus.com/articles/39243-significance-of-e-cadherin-gene-mutations-in-patients-with-hereditary-diffuse-gastric-cancer-syndrome-a-systematic-review (accessed on 23 August 2021).
- Pelucchi, C.; Lunet, N.; Boccia, S.; Zhang, Z.-F.; Praud, D.; Boffetta, P.; Levi, F.; Matsuo, K.; Ito, H.; Hu, J.; et al. The Stomach Cancer Pooling (StoP) Project: Study Design and Presentation. Eur. J. Cancer Prev. 2015, 24, 16–23. [Google Scholar] [CrossRef]
- Ferro, A.; Rosato, V.; Rota, M.; Costa, A.R.; Morais, S.; Pelucchi, C.; Johnson, K.C.; Hu, J.; Palli, D.; Ferraroni, M.; et al. Meat Intake and Risk of Gastric Cancer in the Stomach Cancer Pooling (StoP) Project. Int. J. Cancer 2020, 147, 45–55. [Google Scholar] [CrossRef]
- Corso, G.; Montagna, G.; Figueiredo, J.; La Vecchia, C.; Fumagalli Romario, U.; Fernandes, M.S.; Seixas, S.; Roviello, F.; Trovato, C.; Guerini-Rocco, E.; et al. Hereditary Gastric and Breast Cancer Syndromes Related to CDH1 Germline Mutation: A Multidisciplinary Clinical Review. Cancers 2020, 12, 1598. [Google Scholar] [CrossRef]
- Rocha, J.P.; Gullo, I.; Wen, X.; Devezas, V.; Baptista, M.; Oliveira, C.; Carneiro, F. Pathological Features of Total Gastrectomy Specimens from Asymptomatic Hereditary Diffuse Gastric Cancer Patients and Implications for Clinical Management. Histopathology 2018, 73, 878–886. [Google Scholar] [CrossRef]
- Spoto, C.P.E.; Gullo, I.; Carneiro, F.; Montgomery, E.A.; Brosens, L.A.A. Hereditary Gastrointestinal Carcinomas and Their Precursors: An Algorithm for Genetic Testing. Semin. Diagn. Pathol. 2018, 35, 170–183. [Google Scholar] [CrossRef]
- Carreño, M.; Pena-Couso, L.; Mercadillo, F.; Perea, J.; Urioste, M. Investigation on the Role of PALB2 Gene in CDH1-Negative Patients With Hereditary Diffuse Gastric Cancer. Clin. Transl. Gastroenterol. 2020, 11, e00280. [Google Scholar] [CrossRef]
- Pharoah, P.D.; Guilford, P.; Caldas, C. Incidence of Gastric Cancer and Breast Cancer in CDH1 (E-Cadherin) Mutation Carriers from Hereditary Diffuse Gastric Cancer Families. Gastroenterology 2001, 121, 1348–1353. [Google Scholar] [CrossRef]
- Xicola, R.M.; Li, S.; Rodriguez, N.; Reinecke, P.; Karam, R.; Speare, V.; Black, M.H.; LaDuca, H.; Llor, X. Clinical Features and Cancer Risk in Families with Pathogenic CDH1 Variants Irrespective of Clinical Criteria. J. Med. Genet. 2019, 56, 838–843. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huynh, J.M.; Laukaitis, C.M. Panel Testing Reveals Nonsense and Missense CDH1 Mutations in Families without Hereditary Diffuse Gastric Cancer. Mol. Genet. Genomic. Med. 2016, 4, 232–236. [Google Scholar] [CrossRef] [PubMed]
- Moslim, M.A.; Heald, B.; Tu, C.; Burke, C.A.; Walsh, R.M. Early Genetic Counseling and Detection of CDH1 Mutation in Asymptomatic Carriers Improves Survival in Hereditary Diffuse Gastric Cancer. Surgery 2018, 164, 754–759. [Google Scholar] [CrossRef] [PubMed]
- Choi, H.-J.; Ki, C.-S.; Suh, S.-P.; Kim, J.-W. Presymptomatic Identification of CDH1 Germline Mutation in a Healthy Korean Individual with Family History of Gastric Cancer. Ann. Lab. Med. 2014, 34, 386–389. [Google Scholar] [CrossRef] [Green Version]
- Katona, B.W.; Clark, D.F.; Domchek, S.M. CDH1 on Multigene Panel Testing: Look Before You Leap. JNCI J. Natl. Cancer Inst. 2020, 112, 330–334. [Google Scholar] [CrossRef]
- López, M.; Cervera-Acedo, C.; Santibáñez, P.; Salazar, R.; Sola, J.-J.; Domínguez-Garrido, E. A Novel Mutation in the CDH1 Gene in a Spanish Family with Hereditary Diffuse Gastric Cancer. Springerplus 2016, 5, 1181. [Google Scholar] [CrossRef] [Green Version]
- Suriano, G.; Yew, S.; Ferreira, P.; Senz, J.; Kaurah, P.; Ford, J.M.; Longacre, T.A.; Norton, J.A.; Chun, N.; Young, S.; et al. Characterization of a Recurrent Germ Line Mutation of the E-Cadherin Gene: Implications for Genetic Testing and Clinical Management. Clin. Cancer Res. 2005, 11, 5401–5409. [Google Scholar] [CrossRef] [Green Version]
- Hakkaart, C.; Ellison-Loschmann, L.; Day, R.; Sporle, A.; Koea, J.; Harawira, P.; Cheng, S.; Gray, M.; Whaanga, T.; Pearce, N.; et al. Germline CDH1 Mutations Are a Significant Contributor to the High Frequency of Early-Onset Diffuse Gastric Cancer Cases in New Zealand Māori. Fam. Cancer 2019, 18, 83–90. [Google Scholar] [CrossRef] [Green Version]
- Zhang, H.; Feng, M.; Feng, Y.; Bu, Z.; Li, Z.; Jia, S.; Ji, J. Germline Mutations in Hereditary Diffuse Gastric Cancer. Chin. J. Cancer Res. 2018, 30, 122–130. [Google Scholar] [CrossRef]
- Molinaro, V.; Pensotti, V.; Marabelli, M.; Feroce, I.; Barile, M.; Pozzi, S.; Laghi, L.; Serrano, D.; Bernard, L.; Bonanni, B.; et al. Complementary Molecular Approaches Reveal Heterogeneous CDH1 Germline Defects in Italian Patients with Hereditary Diffuse Gastric Cancer (HDGC) Syndrome. Genes Chromosomes Cancer 2014, 53, 432–445. [Google Scholar] [CrossRef]
- Lajus, T.B.P.; Sales, R.M.D. CDH1 Germ-Line Missense Mutation Identified by Multigene Sequencing in a Family with No History of Diffuse Gastric Cancer. Gene 2015, 568, 215–219. [Google Scholar] [CrossRef] [PubMed]
- Sanches, J.M.; Figueiredo, J.; Fonseca, M.; Durães, C.; Melo, S.; Esménio, S.; Seruca, R. Quantification of Mutant E-Cadherin Using Bioimaging Analysis of in Situ Fluorescence Microscopy. A New Approach to CDH1 Missense Variants. Eur. J. Hum. Genet. 2015, 23, 1072–1079. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, K.; Krempely, K.; Roberts, M.E.; Anderson, M.J.; Carneiro, F.; Chao, E.; Dixon, K.; Figueiredo, J.; Ghosh, R.; Huntsman, D.; et al. Specifications of the ACMG/AMP Variant Curation Guidelines for the Analysis of Germline CDH1 Sequence Variants. Hum. Mutat. 2018, 39, 1553–1568. [Google Scholar] [CrossRef]
- Gjyshi, O.; Vashi, P.; Seewald, L.; Kohan, M.; Abboud, E.; Fowler, E.; Suppiah, R.; Halabi, H. Therapeutic and Prophylactic Gastrectomy in a Family with Hereditary Diffuse Gastric Cancer Secondary to a CDH1 Mutation: A Case Series. World J. Surg. Oncol. 2018, 16, 143. [Google Scholar] [CrossRef] [PubMed]
- Lynch, H.T.; Nustas, R.; Kassim, T.; Snyder, C.; Shaw, T.; Diab, O. The Benefits of a Model of Interval Comprehensive Assessments (MICA) in Hereditary Cancer Syndromes: Hereditary Diffuse Gastric Cancer (HDGC) as an Example. Cancer Genet. 2019, 233–234, 43–47. [Google Scholar] [CrossRef] [PubMed]
- Hallowell, N.; Lawton, J.; Badger, S.; Richardson, S.; Hardwick, R.H.; Caldas, C.; Fitzgerald, R.C. The Psychosocial Impact of Undergoing Prophylactic Total Gastrectomy (PTG) to Manage the Risk of Hereditary Diffuse Gastric Cancer (HDGC). J. Genet. Couns. 2017, 26, 752–762. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hallowell, N.; Badger, S.; Richardson, S.; Caldas, C.; Hardwick, R.H.; Fitzgerald, R.C.; Lawton, J. An Investigation of the Factors Effecting High-Risk Individuals’ Decision-Making about Prophylactic Total Gastrectomy and Surveillance for Hereditary Diffuse Gastric Cancer (HDGC). Fam. Cancer 2016, 15, 665–676. [Google Scholar] [CrossRef]
- van der Post, R.S.; Vogelaar, I.P.; Manders, P.; van der Kolk, L.E.; Cats, A.; van Hest, L.P.; Sijmons, R.; Aalfs, C.M.; Ausems, M.G.E.M.; Gómez García, E.B.; et al. Accuracy of Hereditary Diffuse Gastric Cancer Testing Criteria and Outcomes in Patients With a Germline Mutation in CDH1. Gastroenterology 2015, 149, 897–906. [Google Scholar] [CrossRef]
- Stjepanovic, N.; Moreira, L.; Carneiro, F.; Balaguer, F.; Cervantes, A.; Balmaña, J.; Martinelli, E. Hereditary Gastrointestinal Cancers: ESMO Clinical Practice Guidelines for Diagnosis, Treatment and Follow-Up. Ann. Oncol. 2019, 30, 1558–1571. [Google Scholar] [CrossRef] [Green Version]
- Vreemann, S.; van Zelst, J.C.M.; Schlooz-Vries, M.; Bult, P.; Hoogerbrugge, N.; Karssemeijer, N.; Gubern-Mérida, A.; Mann, R.M. The Added Value of Mammography in Different Age-Groups of Women with and without BRCA Mutation Screened with Breast MRI. Breast Cancer Res. 2018, 20, 84. [Google Scholar] [CrossRef]
- King, T.A.; Pilewskie, M.; Muhsen, S.; Patil, S.; Mautner, S.K.; Park, A.; Oskar, S.; Guerini-Rocco, E.; Boafo, C.; Gooch, J.C.; et al. Lobular Carcinoma in Situ: A 29-Year Longitudinal Experience Evaluating Clinicopathologic Features and Breast Cancer Risk. J. Clin. Oncol. 2015, 33, 3945–3952. [Google Scholar] [CrossRef] [PubMed]
- Aitchison, A.; Hakkaart, C.; Whitehead, M.; Khan, S.; Siddique, S.; Ahmed, R.; Frizelle, F.A.; Keenan, J.I. CDH1 Gene Mutation in Early-Onset, Colorectal Signet-Ring Cell Carcinoma. Pathol. Res. Pract. 2020, 216, 152912. [Google Scholar] [CrossRef] [PubMed]
- Hamilton, L.E.; Jones, K.; Church, N.; Medlicott, S. Synchronous Appendiceal and Intramucosal Gastric Signet Ring Cell Carcinomas in an Individual with CDH1-Associated Hereditary Diffuse Gastric Carcinoma: A Case Report of a Novel Association and Review of the Literature. BMC Gastroenterol. 2013, 13, 114. [Google Scholar] [CrossRef] [Green Version]
- Richards, F.M.; McKee, S.A.; Rajpar, M.H.; Cole, T.R.P.; Evans, D.G.R.; Jankowski, J.A.; McKeown, C.; Sanders, D.S.A.; Maher, E.R. Germline E-Cadherin Gene (CDH1) Mutations Predispose to Familial Gastric Cancer and Colorectal Cancer. Hum. Mol. Genet. 1999, 8, 607–610. [Google Scholar] [CrossRef] [PubMed]
- Salahshor, S.; Hou, H.; Diep, C.B.; Loukola, A.; Zhang, H.; Liu, T.; Chen, J.; Iselius, L.; Rubio, C.; Lothe, R.A.; et al. A Germline E-Cadherin Mutation in a Family with Gastric and Colon Cancer. Int. J. Mol. Med. 2001, 8, 439–443. [Google Scholar] [CrossRef]
- Castro, R.; Lobo, J.; Pita, I.; Videira, F.; Pedro-Afonso, L.; Dinis-Ribeiro, M.; Brandão, C. Random Biopsies in Patients Harboring a CDH1 Mutation: Time to Change the Approach? Rev. Esp. Enfermadades Dig. 2020, 112, 367–372. [Google Scholar] [CrossRef]
- van Dieren, J.M.; Kodach, L.L.; den Hartog, P.; van der Kolk, L.E.; Sikorska, K.; van Velthuysen, M.-L.F.; van Sandick, J.W.; Koemans, W.J.; Snaebjornsson, P.; Cats, A. Gastroscopic Surveillance with Targeted Biopsies Compared with Random Biopsies in CDH1 Mutation Carriers. Endoscopy 2020, 52, 839–846. [Google Scholar] [CrossRef]
- Mi, E.Z.; Mi, E.Z.; di Pietro, M.; O’Donovan, M.; Hardwick, R.H.; Richardson, S.; Ziauddeen, H.; Fletcher, P.C.; Caldas, C.; Tischkowitz, M.; et al. Comparative Study of Endoscopic Surveillance in Hereditary Diffuse Gastric Cancer According to CDH1 Mutation Status. Gastrointest. Endosc. 2018, 87, 408–418. [Google Scholar] [CrossRef] [Green Version]
- Yasuda, T.; Yagi, N.; Omatsu, T.; Hayashi, S.; Nakahata, Y.; Yasuda, Y.; Obora, A.; Kojima, T.; Naito, Y.; Itoh, Y. Benefits of Linked Color Imaging for Recognition of Early Differentiated-Type Gastric Cancer: In Comparison with Indigo Carmine Contrast Method and Blue Laser Imaging. Surg. Endosc. 2021, 35, 2750–2758. [Google Scholar] [CrossRef]
- Smyth, E.C.; Verheij, M.; Allum, W.; Cunningham, D.; Cervantes, A.; Arnold, D. Gastric Cancer: ESMO Clinical Practice Guidelines for Diagnosis, Treatment and Follow-Up. Ann. Oncol. 2016, 27, v38–v49. [Google Scholar] [CrossRef]
- El Rami, F.E.; Barsoumian, H.B.; Khneizer, G.W. Hereditary Diffuse Gastric Cancer Therapeutic Roadmap: Current and Novel Approaches in a Nutshell. Ther. Adv. Med. Oncol. 2020, 12, 1758835920967238. [Google Scholar] [CrossRef] [PubMed]

| Family Criteria (1st or 2nd Degree Blood Relatives of Each Other) 1 | Individual Criteria |
|---|---|
| ≥2 cases of gastric cancer in family regardless of age, with at least one DGC ≥1 case of DGC at any age and ≥1 case of LBC < 70 years in different family members ≥2 cases of LBC in family members < 50 years | DGC < 50 years DGC at any age in individuals of Māori ethnicity DGC at any age in individuals with a personal or family history (1st degree) of cleft lip/cleft palate |
| History of DGC and LBC, both diagnosed < 70 years Bilateral LBC, diagnosed < 70 years Gastric in situ signet ring cells and/or pagetoid spread of signet ring cells in individuals < 50 years |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cosma, L.-S.; Schlosser, S.; Tews, H.C.; Müller, M.; Kandulski, A. Hereditary Diffuse Gastric Cancer: Molecular Genetics, Biological Mechanisms and Current Therapeutic Approaches. Int. J. Mol. Sci. 2022, 23, 7821. https://doi.org/10.3390/ijms23147821
Cosma L-S, Schlosser S, Tews HC, Müller M, Kandulski A. Hereditary Diffuse Gastric Cancer: Molecular Genetics, Biological Mechanisms and Current Therapeutic Approaches. International Journal of Molecular Sciences. 2022; 23(14):7821. https://doi.org/10.3390/ijms23147821
Chicago/Turabian StyleCosma, Lidia-Sabina, Sophie Schlosser, Hauke C. Tews, Martina Müller, and Arne Kandulski. 2022. "Hereditary Diffuse Gastric Cancer: Molecular Genetics, Biological Mechanisms and Current Therapeutic Approaches" International Journal of Molecular Sciences 23, no. 14: 7821. https://doi.org/10.3390/ijms23147821