
Proteinuria Is Associated with the Development of Crohn’s Disease: A Nationwide Population-Based Study

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Material and Methods
2.1. Data Source and Study Population
2.2. Dipstick Urinalysis and Study Endpoints
2.3. Covariates
2.4. Statistical Analysis
3. Results
3.1. Baseline Characteristics of the Study Population
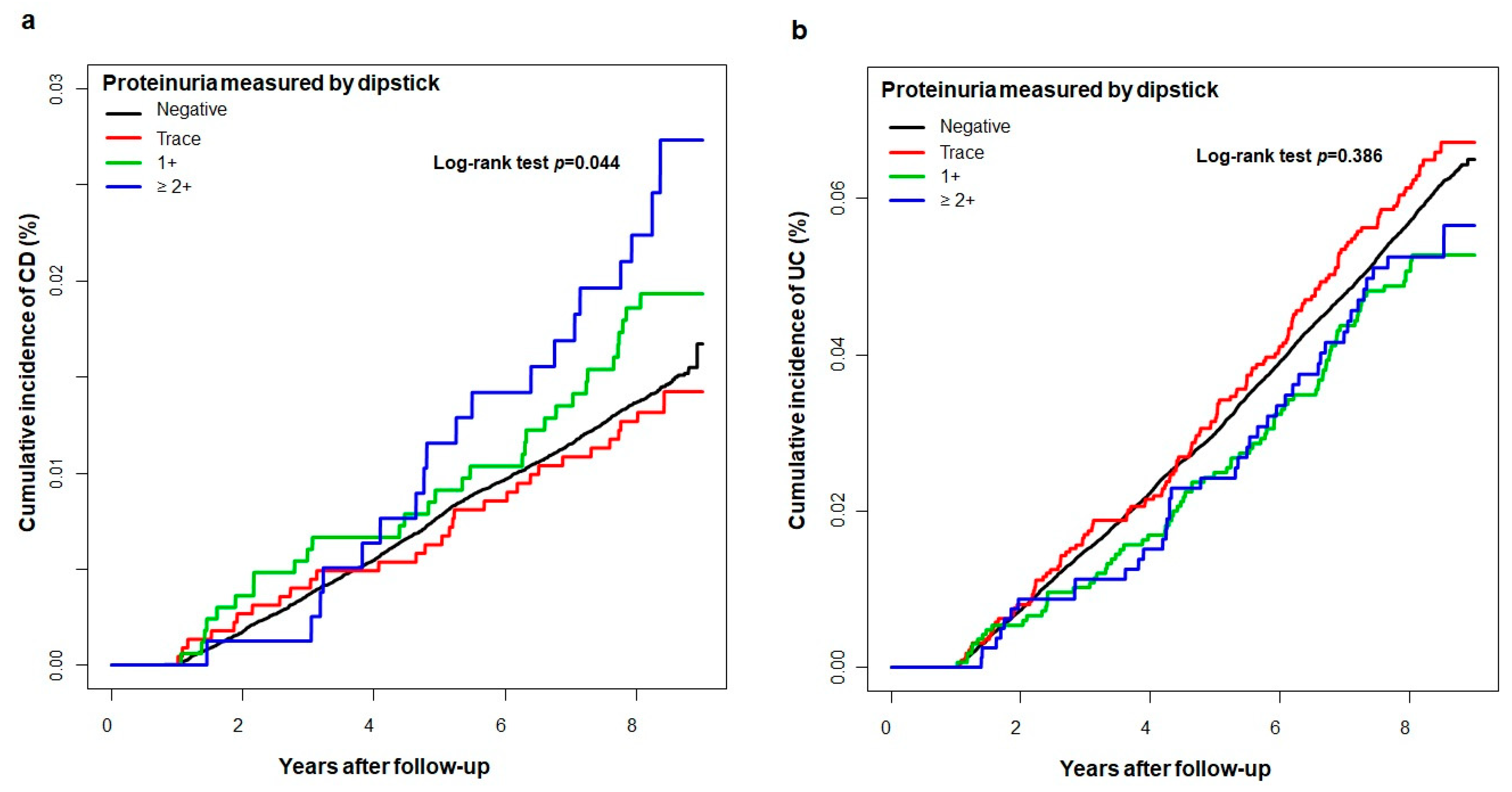
3.2. Incidence and Risk of IBD According to Proteinuria Degree on Dipstick
3.3. Subgroup Analysis of the IBD Risk in Dipstick-Positive Proteinuria
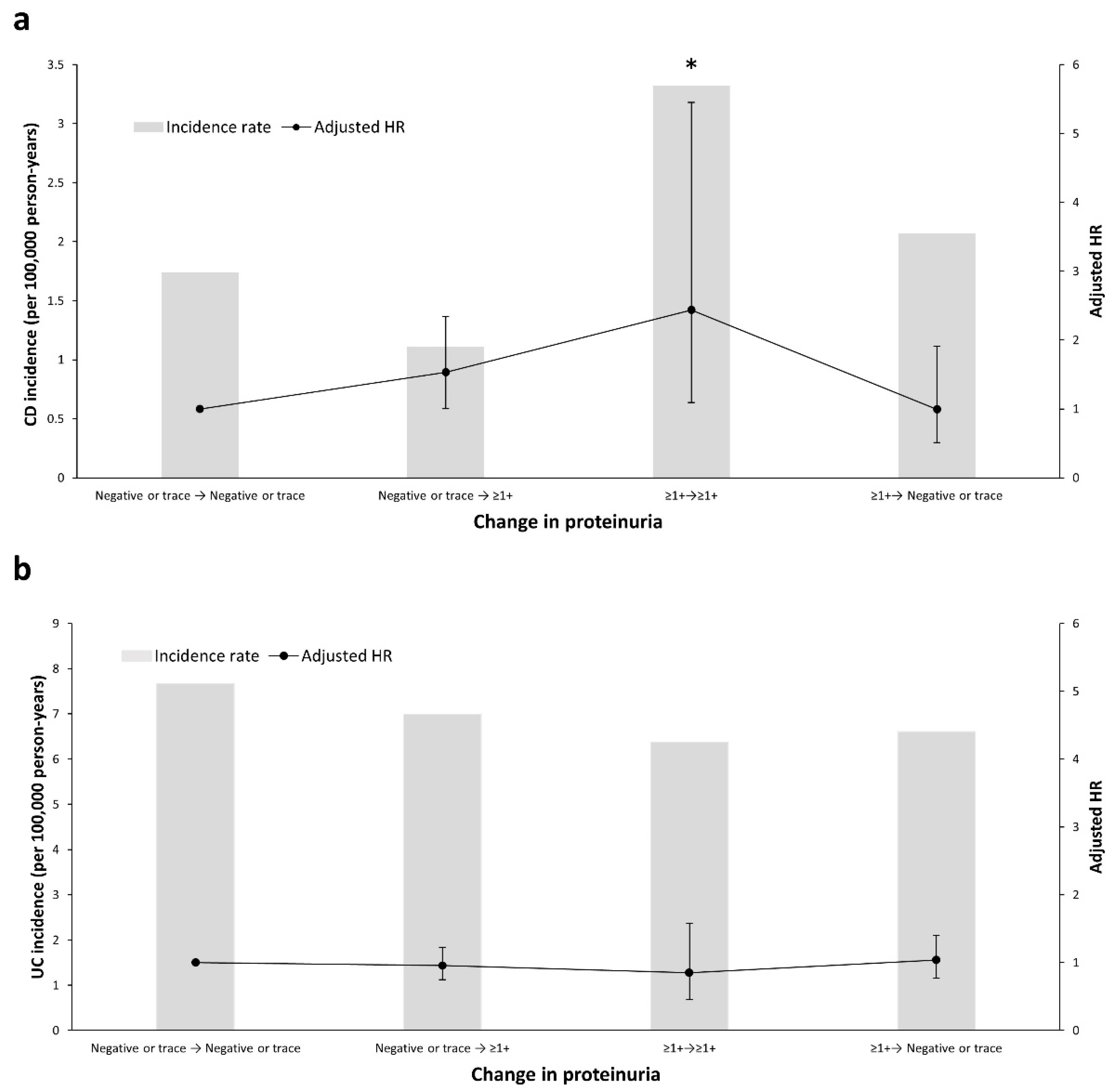
3.4. Change in Proteinuria on the Dipstick Test and Risk of IBD
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
Abbreviations
References
- Ananthakrishnan, A.N. Epidemiology and risk factors for IBD. Nat. Rev. Gastroenterol. Hepatol. 2015, 12, 205–217. [Google Scholar] [CrossRef] [PubMed]
- Molodecky, N.A.; Soon, I.S.; Rabi, D.M.; Ghali, W.A.; Ferris, M.; Chernoff, G.; Benchimol, E.I.; Panaccione, R.; Ghosh, S.; Barkema, H.W.; et al. Increasing incidence and prevalence of the inflammatory bowel diseases with time, based on systematic review. Gastroenterology 2012, 142, 46–54. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ng, W.K.; Wong, S.H.; Ng, S.C. Changing epidemiological trends of inflammatory bowel disease in Asia. Intestig. Res. 2016, 14, 111–119. [Google Scholar] [CrossRef] [Green Version]
- Kaplan, G.G. The global burden of IBD: From 2015 to 2025. Nat. Rev. Gastroenterol. Hepatol. 2015, 12, 720–727. [Google Scholar] [CrossRef]
- Turin, T.C.; James, M.; Ravani, P.; Tonelli, M.; Manns, B.J.; Quinn, R.; Jun, M.; Klarenbach, S.; Hemmelgarn, B.R. Proteinuria and Rate of Change in Kidney Function in a Community-Based Population. J. Am. Soc. Nephrol. 2013, 24, 1661–1667. [Google Scholar] [CrossRef] [Green Version]
- Hemmelgarn, B.R.; Manns, B.J.; Lloyd, A.; James, M.T.; Klarenbach, S.; Quinn, R.R.; Wiebe, N.; Tonelli, M.; Network, F.T.A.K.D. Relation Between Kidney Function, Proteinuria, and Adverse Outcomes. JAMA 2010, 303, 423–429. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paisley, K.E.; Beaman, M.; Tooke, J.E.; Mohamed-Ali, V.; Lowe, G.D.; Shore, A.C. Endothelial dysfunction and inflammation in asymptomatic proteinuria. Kidney Int. 2003, 63, 624–633. [Google Scholar] [CrossRef] [Green Version]
- Nam, G.E.; Kim, N.H.; Han, K.; Choi, K.M.; Chung, H.S.; Kim, J.W.; Han, B.; Cho, S.J.; Jung, S.J.; Yu, J.H.; et al. Chronic renal dysfunction, proteinuria, and risk of Parkinson’s disease in the elderly. Mov. Disord. 2019, 34, 1184–1191. [Google Scholar] [CrossRef] [PubMed]
- Sun, K.; Lin, D.; Li, F.; Qi, Y.; Feng, W.; Yan, L.; Chen, C.; Ren, M.; Liu, D. Fatty liver index, albuminuria and the association with chronic kidney disease: A population-based study in China. BMJ Open 2018, 8, e019097. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, A.; Liu, X.; Su, Z.; Chen, S.; Zhang, N.; Wu, S.; Wang, Y.; Wang, Y. Two-Year Changes in Proteinuria and the Risk of Stroke in the Chinese Population: A Prospective Cohort Study. J. Am. Hear. Assoc. 2017, 6, 6. [Google Scholar] [CrossRef] [PubMed]
- Hara, M.; Ando, M.; Maeda, Y.; Tsuchiya, K.; Nitta, K. Proteinuria is a simple sign of systemic inflammation that leads to a poor prognosis in individuals affected with non-Hodgkin lymphoma. Clin. Nephrol. 2014, 82, 51–57. [Google Scholar] [CrossRef]
- Okada, R.; Yasuda, Y.; Tsushita, K.; Wakai, K.; Hamajima, N.; Matsuo, S. Trace proteinuria by dipstick screening is associated with metabolic syndrome, hypertension, and diabetes. Clin. Exp. Nephrol. 2018, 22, 1387–1394. [Google Scholar] [CrossRef] [PubMed]
- Wei, X.-B.; Liu, Y.-H.; He, P.-C.; Yu, D.-Q.; Zhou, Y.-L.; Tan, N.; Chen, J.-Y. The relationship between albuminuria and poor clinical outcomes in patients with infective endocarditis. Clin. Chim. Acta 2016, 462, 28–32. [Google Scholar] [CrossRef]
- Song, S.O.; Jung, C.H.; Song, Y.D.; Park, C.-Y.; Kwon, H.-S.; Cha, B.S.; Park, J.-Y.; Lee, K.-U.; Ko, K.S.; Lee, B.-W. Background and Data Configuration Process of a Nationwide Population-Based Study Using the Korean National Health Insurance System. Diabetes Metab. J. 2014, 38, 395–403. [Google Scholar] [CrossRef]
- Kim, H.J.; Hann, H.J.; Hong, S.N.; Kim, K.H.; Ahn, I.M.; Song, J.Y.; Lee, S.H.; Ahn, H.S. Incidence and Natural Course of Inflammatory Bowel Disease in Korea, 2006–2012. Inflamm. Bowel Dis. 2015, 21, 623–630. [Google Scholar] [CrossRef] [PubMed]
- Choi, K.; Chun, J.; Han, K.; Park, S.; Soh, H.; Kim, J.; Lee, J.; Lee, H.J.; Im, J.P.; Kim, J.S. Risk of Anxiety and Depression in Patients with Inflammatory Bowel Disease: A Nationwide, Population-Based Study. J. Clin. Med. 2019, 8, 654. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kang, E.A.; Han, K.; Chun, J.; Soh, H.; Park, S.; Im, J.P.; Kim, J.S. Increased Risk of Diabetes in Inflammatory Bowel Disease Patients: A Nationwide Population-based Study in Korea. J. Clin. Med. 2019, 8, 343. [Google Scholar] [CrossRef] [Green Version]
- Park, S.; Chun, J.; Han, K.-D.; Soh, H.; Choi, K.; Kim, J.H.; Lee, J.; Lee, C.; Im, J.P.; Kim, J.S. Increased end-stage renal disease risk in patients with inflammatory bowel disease: A nationwide population-based study. World J. Gastroenterol. 2018, 24, 4798–4808. [Google Scholar] [CrossRef] [PubMed]
- Soh, H.; Chun, J.; Han, K.; Park, S.; Choi, G.; Kim, J.H.; Lee, J.; Im, J.P.; Kim, J.S. Increased Risk of Herpes Zoster in Young and Metabolically Healthy Patients with Inflammatory Bowel Disease: A Nationwide Population-Based Study. Gut Liver 2019, 13, 333–341. [Google Scholar] [CrossRef] [Green Version]
- Park, S.; Chun, J.; Han, K.-D.; Soh, H.; Kang, E.A.; Lee, H.J.; Im, J.P.; Kim, J.S. Dose-response relationship between cigarette smoking and risk of ulcerative colitis: A nationwide population-based study. J. Gastroenterol. 2019, 54, 881–890. [Google Scholar] [CrossRef]
- Levey, A.S.; Bosch, J.P.; Lewis, J.B.; Greene, T.; Rogers, N.; Roth, D.R. A more accurate method to estimate glomerular filtration rate from serum creatinine: A new prediction equation. Ann. Intern. Med. 1999, 130, 461–470. [Google Scholar] [CrossRef]
- White, S.L.; Yu, R.; Craig, J.C.; Polkinghorne, K.R.; Atkins, R.C.; Chadban, S.J. Diagnostic Accuracy of Urine Dipsticks for Detection of Albuminuria in the General Community. Am. J. Kidney Dis. 2011, 58, 19–28. [Google Scholar] [CrossRef]
- Bailie, G.R.; Uhlig, K.; Levey, A.S. Clinical Practice Guidelines in Nephrology: Evaluation, Classification, and Stratification of Chronic Kidney Disease. Pharmacother. J. Hum. Pharmacol. Drug Ther. 2005, 25, 491–502. [Google Scholar] [CrossRef] [PubMed]
- Lim, D.; Lee, D.-Y.; Cho, S.H.; Kim, O.Z.; Cho, S.W.; An, S.K.; Kim, H.W.; Moon, K.H.; Lee, M.H.; Kim, B. Diagnostic accuracy of urine dipstick for proteinuria in older outpatients. Kidney Res. Clin. Pr. 2014, 33, 199–203. [Google Scholar] [CrossRef] [Green Version]
- Bello, A.K.; Hemmelgarn, B.; Lloyd, A.; James, M.T.; Manns, B.J.; Klarenbach, S.; Tonelli, M.; Network, F.T.A.K.D. Associations among Estimated Glomerular Filtration Rate, Proteinuria, and Adverse Cardiovascular Outcomes. Clin. J. Am. Soc. Nephrol. 2011, 6, 1418–1426. [Google Scholar] [CrossRef] [PubMed]
- Jensen, J.S.; Borch-Johnsen, K.; Jensen, G.; Feldt-Rasmussen, B. Microalbuminuria Reflects a Generalized Transvascular Albumin Leakiness in Clinically Healthy Subjects. Clin. Sci. 1995, 88, 629–633. [Google Scholar] [CrossRef]
- Salmon, A.H.J.; Satchell, S.C. Endothelial glycocalyx dysfunction in disease: Albuminuria and increased microvascular permeability. J. Pathol. 2012, 226, 562–574. [Google Scholar] [CrossRef] [PubMed]
- Festa, A.; Dagostino, R.B.; Howard, G.S.; Mykkänen, L.; Tracy, R.P.; Haffner, S.M. Inflammation and microalbuminuria in nondiabetic and type 2 diabetic subjects: The Insulin Resistance Atherosclerosis Study. Kidney Int. 2000, 58, 1703–1710. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stenvinkel, P. Endothelial dysfunction and inflammation-is there a link? Nephrol. Dial. Transplant. 2001, 16, 1968–1971. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cibor, D.; Domagala-Rodacka, R.; Rodacki, T.; Jurczyszyn, A.; Mach, T.; Owczarek, D. Endothelial dysfunction in inflammatory bowel diseases: Pathogenesis, assessment and implications. World J. Gastroenterol. 2016, 22, 1067–1077. [Google Scholar] [CrossRef]
- Roifman, I.; Sun, Y.C.; Fedwick, J.P.; Panaccione, R.; Buret, A.G.; Liu, H.; Rostom, A.; Anderson, T.J.; Beck, P.L. Evidence of endothelial dysfunction in patients with inflammatory bowel disease. Clin. Gastroenterol. Hepatol. 2009, 7, 175–182. [Google Scholar] [CrossRef] [PubMed]
- Deban, L.; Correale, C.; Vetrano, S.; Malesci, A.; Danese, S. Multiple pathogenic roles of microvasculature in inflammatory bowel disease: A jack of all trades. Am. J. Pathol. 2008, 172, 1457–1466. [Google Scholar] [CrossRef] [Green Version]
- Gravina, A.G.; Dallio, M.; Masarone, M.; Rosato, V.; Aglitti, A.; Persico, M.; Loguercio, C.; Federico, A. Vascular Endothelial Dysfunction in Inflammatory Bowel Diseases: Pharmacological and Nonpharmacological Targets. Oxidative Med. Cell. Longev. 2018, 2018, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Steyers, C.M., III; Miller, F.J., Jr. Endothelial dysfunction in chronic inflammatory diseases. Int. J. Mol. Sci. 2014, 15, 11324–11349. [Google Scholar] [CrossRef] [Green Version]
- Danese, S. Role of the vascular and lymphatic endothelium in the pathogenesis of inflammatory bowel disease: Brothers in arms. Gut 2011, 60, 998–1008. [Google Scholar] [CrossRef]
- Liu, Y.-H.; Ding, Y.; Gao, C.-C.; Li, L.-S.; Wang, Y.-X.; Xu, J.-D. Functional macrophages and gastrointestinal disorders. World J. Gastroenterol. 2018, 24, 1181–1195. [Google Scholar] [CrossRef] [Green Version]
- Danese, S.; Scaldaferri, F.; Vetrano, S.; Stefanelli, T.; Graziani, C.; Repici, A.; Ricci, R.; Straface, G.; Sgambato, A.; Malesci, A.; et al. Critical role of the CD40 CD40-ligand pathway in regulating mucosal inflammation-driven angiogenesis in inflammatory bowel disease. Gut 2007, 56, 1248–1256. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Levine, A.; Boneh, R.S.; Wine, E. Evolving role of diet in the pathogenesis and treatment of inflammatory bowel diseases. Gut 2018, 67, 1726–1738. [Google Scholar] [CrossRef]
- Jantchou, P.; Morois, S.; Clavel-Chapelon, F.; Boutron-Ruault, M.-C.; Carbonnel, F. Animal Protein Intake and Risk of Inflammatory Bowel Disease: The E3N Prospective Study. Am. J. Gastroenterol. 2010, 105, 2195–2201. [Google Scholar] [CrossRef] [PubMed]
- Fagan, E.A.; Dyck, R.F.; Maton, P.N.; Hodgson, H.J.; Chadwick, V.S.; Petrie, A.; Pepys, M.B. Serum levels of C-reactive protein in Crohn’s disease and ulcerative colitis. Eur. J. Clin. Investig. 1982, 12, 351–359. [Google Scholar] [CrossRef]
- Henriksen, M.; Jahnsen, J.; Lygren, I.; Stray, N.; Sauar, J.; Vatn, M.H.; Moum, B.; the IBSEN Study Group C-Reactive Protein. A predictive factor and marker of inflammation in inflammatory bowel disease. Results from a prospective population-based study. Gut 2008, 57, 1518–1523. [Google Scholar] [CrossRef]
- Saverymuttu, S.H.; Hodgson, H.J.; Chadwick, V.S.; Pepys, M.B. Differing acute phase responses in Crohn’s disease and ulcerative colitis. Gut 1986, 27, 809–813. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gross, V.; Andus, T.; Caesar, I.; Roth, M.; Scholmerich, J. Evidence for continuous stimulation of interleukin-6 production in Crohn’s disease. Gastroenterology 1992, 102, 514–519. [Google Scholar] [CrossRef]
- Komatsu, M.; Kobayashi, D.; Saito, K.; Furuya, D.; Yagihashi, A.; Araake, H.; Tsuji, N.; Sakamaki, S.; Niitsu, Y.; Watanabe, N. Tumor Necrosis Factor-α in Serum of Patients with Inflammatory Bowel Disease as Measured by a Highly Sensitive Immuno-PCR. Clin. Chem. 2001, 47, 1297–1301. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Murch, S.H.; Braegger, C.P.; A Walker-Smith, J.; Macdonald, T.T. Location of tumour necrosis factor alpha by immunohistochemistry in chronic inflammatory bowel disease. Gut 1993, 34, 1705–1709. [Google Scholar] [CrossRef] [Green Version]
- Dionne, S.; Hiscott, J.; D’Agata, I.; Duhaime, A.; Seidman, E.G. Quantitative PCR analysis of TNF-alpha and IL-1 beta mRNA levels in pediatric IBD mucosal biopsies. Dig. Dis. Sci. 1997, 42, 1557–1566. [Google Scholar] [CrossRef]
- Bousvaros, A.; Leichtner, A.; Zurakowski, D.; Kwon, J.; Law, T.; Keough, K.; Fishman, S. Elevated serum vascular endothelial growth factor in children and young adults with Crohn’s disease. Dig. Dis. Sci. 1999, 44, 424–430. [Google Scholar] [CrossRef]
- Choi, Y.J.; Lee, D.H.; Shin, D.W.; Han, K.-D.; Yoon, H.; Shin, C.M.; Park, Y.S.; Kim, N. Patients with inflammatory bowel disease have an increased risk of myocardial infarction: A nationwide study. Aliment. Pharmacol. Ther. 2019, 50, 769–779. [Google Scholar] [CrossRef] [PubMed]
- Park, S.H.; Kim, Y.-J.; Rhee, K.H.; Kim, Y.K.; Hong, S.N.; Seo, S.I.; Cha, J.M.; Park, S.Y.; Jeong, S.K.; Lee, J.H.; et al. A 30-year Trend Analysis in the Epidemiology of Inflammatory Bowel Disease in the Songpa-Kangdong District of Seoul, Korea in 1986–2015. J. Crohn’s Colitis 2019, 13, 1410–1417. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristics | Proteinuria Measured by Dipstick | p-Value | |||
|---|---|---|---|---|---|
| Negative | Trace (±) | 1+ | ≥ 2+ | ||
| No. (%) | 9,444,344 (95.2) | 224,793 (2.3) | 167,324 (1.7) | 80,939 (0.8) | |
| Age, years † | 46.9 ± 14.0 | 48.9 ± 14.2 | 51.1 ± 14.5 | 53.2 ± 14.3 | <0.001 |
| 20–64 | 8,243,115 (87.3) | 189,309 (84.2) | 133,790 (80.0) | 61,528 (76.0) | <0.001 |
| 65–110 | 1,201,229 (12.7) | 35,484 (15.8) | 33,534 (20.0) | 19,411 (24.0) | |
| Male | 5,177,903 (54.8) | 121,349 (54.0) | 90,214 (53.9) | 45,386 (56.1) | <0.001 |
| Urban residence | 4,340,165 (46.0) | 109,178 (48.6) | 80,618 (48.2) | 37,299 (46.1) | <0.001 |
| Smoking status | <0.001 | ||||
| Nonsmokers | 5,614,771 (59.5) | 134,436 (59.8) | 100,081 (59.8) | 47,878 (59.2) | |
| Former smokers | 1,351,140 (14.3) | 33,116 (14.7) | 25,809 (15.4) | 13,498 (16.7) | |
| Current smokers | 2,478,433 (26.2) | 57,241 (25.5) | 41,434 (24.8) | 19,563 (24.2) | |
| Heavy drinker ‡ | 643,540 (6.8) | 16,784 (7.5) | 13,153 (7.9) | 6518 (8.1) | <0.001 |
| Regular exercise § | 4,870,116 (51.6) | 114,758 (51.1) | 81,648 (48.8) | 37,829 (46.7) | <0.001 |
| BMI, kg/m2 † | 23.7 ± 3.2 | 24.0 ± 3.4 | 24.3 ± 3.5 | 24.6 ± 3.7 | <0.001 |
| Height, cm † | 163.9 ± 9.2 | 163.6 ± 9.1 | 163.0 ± 9.1 | 162.6 ± 9.1 | <0.001 |
| Weight, kg † | 63.9 ± 11.6 | 64.4 ± 11.9 | 64.7 ± 12.1 | 65.3 ± 12.5 | <0.001 |
| Systolic blood pressure, mmHg † | 122.2 ± 14.8 | 124.1 ± 16.1 | 126.5 ± 17.0 | 129.8 ± 18.1 | <0.001 |
| Diastolic blood pressure, mmHg† | 76.2 ± 9.9 | 77.2 ± 10.6 | 78.43 ± 11.0 | 79.9 ± 11.4 | <0.001 |
| Fasting glucose, mg/dL † | 96.70 ± 21.9 | 101.7 ± 29.5 | 107.7 ± 37.0 | 115.2 ± 44.8 | <0.001 |
| Total cholesterol, mg/dL † | 194.8 ± 36.4 | 197.6 ± 38.3 | 199.6 ± 40.2 | 202.4 ± 43.4 | <0.001 |
| Creatinine, mg/dL † | 1.0 ± 0.9 | 1.1 ± 1.1 | 1.1 ± 1.0 | 1.2 ± 1.0 | <0.001 |
| eGFR, mL/min/1.73 m2 † | 88.6 ± 44.5 | 85.0 ± 31.5 | 82.8 ± 33.9 | 77.4 ± 35.4 | <0.001 |
| Comorbidity | |||||
| Diabetes mellitus | 2,353,771 (24.9) | 75,690 (33.7) | 72,603 (43.4) | 45,808 (56.6) | <0.001 |
| Hypertension | 767,049 (8.1) | 32,227 (14.3) | 36,117 (21.6) | 25,807 (31.9) | <0.001 |
| Dyslipidemia | 1,683,466 (17.8) | 51,939 (23.1) | 47,233 (28.2) | 29,879 (36.9) | <0.001 |
| IBD | Proteinuria Measured by Dipstick | p for Trend | |||
|---|---|---|---|---|---|
| Negative | Trace(±) | 1+ | ≥ 2+ | ||
| Crohn’s disease | |||||
| CD cases (n) | 1343 | 30 | 31 | 19 | |
| Person-years | 78,055,660 | 1,846,270 | 1,360,989 | 645,798 | |
| CD incidence (per 100,000 person-years) | 1.7 | 1.6 | 2.3 | 2.9 | |
| Crude HR (95% CI) | 1 (reference) | 0.946 (0.659–1.358) | 1.328 (0.93–1.895) | 1.72 (1.094–2.706) | 0.095 |
| p-value | 0.593 | 0.288 | 0.034 | ||
| Model 1 † HR (95% CI) | 1 (reference) | 0.99 (0.689–1.421) | 1.454 (1.018–2.077) | 1.949 (1.238–3.066) | 0.016 |
| p-value | 0.778 | 0.049 | 0.021 | ||
| Model 2 ‡ HR (95% CI) | 1 (reference) | 1.01 (0.704–1.451) | 1.515 (1.061–2.164) | 2.056 (1.306–3.235) | 0.006 |
| p-value | 0.879 | 0.039 | 0.011 | ||
| Model 3 § HR (95% CI) | 1 (reference) | 1.01 (0.703–1.451) | 1.515 (1.058–2.162) | 2.053 (1.301–3.24) | 0.007 |
| p-value | 0.871 | 0.035 | 0.013 | ||
| Ulcerative colitis | |||||
| UC cases (n) | 5634 | 143 | 85 | 41 | |
| Person-years | 78,040,796 | 1,845,890 | 1,360,805 | 645,715 | |
| UC incidence (per 100,000 person-years) | 7.2 | 7.7 | 6.2 | 6.3 | |
| Crude HR (95% CI) | 1 (reference) | 1.074 (0.91–1.268) | 0.868 (0.701–1.075) | 0.886 (0.652–1.204) | 0.16 |
| p-value | 0.367 | 0.115 | 0.277 | ||
| Model 1 † HR (95% CI) | 1 (reference) | 1.085 (0.919–1.281) | 0.882 (0.712–1.093) | 0.897 (0.66–1.22) | 0.172 |
| p-value | 0.339 | 0.128 | 0.268 | ||
| Model 2 ‡ HR (95% CI) | 1 (reference) | 1.1 (0.932–1.299) | 0.911 (0.735–1.128) | 0.938 (0.689–1.275) | 0.363 |
| p-value | 0.256 | 0.223 | 0.412 | ||
| Model 3 § HR (95% CI) | 1 (reference) | 1.12 (0.949–1.323) | 0.947 (0.764–1.174) | 1.009 (0.741–1.373) | 0.722 |
| p-value | 0.185 | 0.370 | 0.682 | ||
| Subgroup | Crohn’s Disease | Ulcerative Colitis | ||
|---|---|---|---|---|
| Adjusted HR † (95% CI) | p for Interaction | Adjusted HR † (95% CI) | p for Interaction | |
| Age, years | ||||
| 20–64 | 1.732 (1.27–2.361) | 0.828 | 0.903 (0.741–1.101) | 0.068 |
| 65–110 | 1.459 (0.708–3.003) | 1.33 (0.886–1.996) | ||
| Sex | ||||
| Male | 1.515 (1.032–2.224) | 0.099 | 0.984 (0.794–1.221) | 0.489 |
| Female | 2.099 (1.38–3.194) | 0.899 (0.657–1.231) | ||
| eGFR, mL/min/1.73 m2 | ||||
| ≥ 90 | 1.703 (1.063–2.728) | 0.340 | 0.945 (0.693–1.287) | 0.552 |
| 60–90 | 1.46 (0.952–2.238) | 0.923 (0.721–1.181) | ||
| < 60 | 2.217 (1.109–4.431) | 1.303 (0.818–2.078) | ||
| Regular exercise ‡ | ||||
| No | 1.726 (1.162–2.564) | 0.938 | 1.102 (0.869–1.397) | 0.143 |
| Yes | 1.633 (1.083–2.462) | 0.831 (0.635–1.086) | ||
| Obese § | ||||
| No | 1.765 (1.255–2.452) | 0.711 | 0.987 (0.794–1.228) | 0.912 |
| Yes | 1.482 (0.863–2.546) | 0.922 (0.68–1.251) | ||
| Diabetes mellitus | ||||
| No | 1.532 (1.099–2.135) | 0.171 | 0.846 (0.687–1.041) | 0.004 |
| Yes | 2.28 (1.281–4.057) | 1.527(1.073–2.174) | ||
| Hypertension | ||||
| No | 1.617 (1.111–2.355) | 0.572 | 0.936(0.738–1.188) | 0.720 |
| Yes | 1.751 (1.127–2.719) | 0.987(0.755–1.288) | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, S.; Lee, H.J.; Han, K.-D.; Soh, H.; Moon, J.M.; Hong, S.W.; Kang, E.A.; Im, J.P.; Kim, J.S. Proteinuria Is Associated with the Development of Crohn’s Disease: A Nationwide Population-Based Study. J. Clin. Med. 2021, 10, 799. https://doi.org/10.3390/jcm10040799
Park S, Lee HJ, Han K-D, Soh H, Moon JM, Hong SW, Kang EA, Im JP, Kim JS. Proteinuria Is Associated with the Development of Crohn’s Disease: A Nationwide Population-Based Study. Journal of Clinical Medicine. 2021; 10(4):799. https://doi.org/10.3390/jcm10040799
Chicago/Turabian StylePark, Seona, Hyun Jung Lee, Kyung-Do Han, Hosim Soh, Jung Min Moon, Seung Wook Hong, Eun Ae Kang, Jong Pil Im, and Joo Sung Kim. 2021. "Proteinuria Is Associated with the Development of Crohn’s Disease: A Nationwide Population-Based Study" Journal of Clinical Medicine 10, no. 4: 799. https://doi.org/10.3390/jcm10040799