
Validation and Classification of the 9-Item Voice Handicap Index (VHI-9i)
by
 ,
,
Felix Caffier
1,†, 
Tadeus Nawka
1,†,
Konrad Neumann
2,
Matthias Seipelt
3 and
Philipp P. Caffier
1,*,† 1
Department of Audiology and Phoniatrics, Charité-Universitätsmedizin Berlin, Charitéplatz 1, D-10117 Berlin, Germany
2
Institute of Biometry and Clinical Epidemiology, Charité-Universitätsmedizin Berlin, Campus Charité Mitte, Charitéplatz 1, D-10117 Berlin, Germany
3
Department of Otorhinolaryngology, Ernst von Bergmann Klinikum Potsdam, Charlottenstr. 72, D-14467 Potsdam, Germany
*
Author to whom correspondence should be addressed.
†
Corporate Member of Freie Universität Berlin and Humboldt-Universität zu Berlin, Campus Charité Mitte.
J. Clin. Med. 2021, 10(15), 3325; https://doi.org/10.3390/jcm10153325
Submission received: 31 May 2021
/
Revised: 24 July 2021
/
Accepted: 25 July 2021
/
Published: 28 July 2021
(This article belongs to the Special Issue Advances in Management of Voice and Swallowing Disorders)
Abstract
:The international nine-item Voice Handicap Index (VHI-9i) is a clinically established short-scale version of the original VHI, quantifying the patients’ self-assessed vocal handicap. However, the current vocal impairment classification is based on percentiles. The main goals of this study were to establish test–retest reliability and a sound statistical basis for VHI-9i severity levels. Between 2009 and 2021, 17,660 consecutive cases were documented. A total of 416 test–retest pairs and 3661 unique cases with complete multidimensional voice diagnostics were statistically analyzed. Classification candidates were the overall self-assessed vocal impairment (VHIs) on a four-point Likert scale, the dysphonia severity index (DSI), the vocal extent measure (VEM), and the auditory–perceptual evaluation (GRB scale). The test–retest correlation of VHI-9i total scores was very high (r = 0.919, p < 0.01). Reliability was excellent regardless of gender or professional voice use, with negligible dependency on age. The VHIs correlated best with the VHI-9i, whereas statistical calculations proved that DSI, VEM, and GRB are unsuitable classification criteria. Based on ROC analysis, we suggest modifying the former VHI-9i severity categories as follows: 0 (healthy): 0 ≤ 7; 1 (mild): 8 ≤ 16; 2 (moderate): 17 ≤ 26; and 3 (severe): 27 ≤ 36.
1. Introduction
A patient’s self-assessment of his or her own voice is an important tool for diagnosing voice disorders and vocal treatment outcomes [1,2]. Only the patients themselves can quantify how much a voice disorder impacts their daily lives. For instance, mild hoarseness affects professional voice users such as opera singers in a different way than non-professional voice users such as office workers [3,4].
The Voice Handicap Index (VHI) was developed and validated as a statistically robust method to measure the subjective impact of voice disorders [5]. The original questionnaire consists of 30 items (VHI-30) addressing functional, physical and emotional impairments in the context of dysphonia according to the patient’s own experience. Each question is answered on a scale from 0 (never) to 4 (always), resulting in an overall score ranging from 0 to 120. The VHI-30 was translated and validated cross-culturally to form international variants (e.g., [6,7,8,9,10,11]) which were proven to be equivalent with each other [12,13].
From our own clinical experience, many patients and medical staff perceive the original 30-item questionnaire as rather time-consuming. To increase overall acceptance and practicability, shortened versions with fewer items were developed. A 12-item questionnaire [14,15] was soon followed by another reduction to 10 items [16,17]. Since 2009, the commonly used variant at the Charité-Universitätsmedizin Berlin is the VHI-9i international questionnaire [14]. It consists of only nine items, after item reduction based on the original VHI-30 and European translations. A detailed discussion of the item and scale development can be found in the original VHI-9i publication [14]. In everyday diagnostic practice, the German translation of the VHI-9i is widely used by laryngologists and phoniatricians in German-speaking countries (e.g., [18,19,20,21,22]). Despite its clinical adoption, the reliability and validity of this VHI short scale as well as its classification have not yet been statistically verified. Instead, the current classification scale is based on the 25th, 50th, and 75th percentiles, dividing the scores into four severity classes. Thus far, clinical experience seems to plausibly reflect the self-perceived voice impairment. However, to overcome this arbitrary percentile-based exploration, we looked for a sound statistical basis for VHI-9i severity levels by revising the current cut-off points. In the context of expert opinion, thorough classifications of vocal parameters are essential for the assessment of dysphonia. In addition, a reliable and valid VHI-9i severity classification is needed to improve clinician-rated evaluations of treatment outcomes (e.g., better characterization of the quantified extent of subjective vocal impairment, more comprehensible assessment of individual pre- vs. post-therapeutic comparisons).
This study aims to address these shortcomings. Initially, we investigated whether the VHI-9i produces reliable results independent of age, gender or professional voice use. Next, the questionnaire validity was examined. For this purpose, the relationship between VHI-9i total scores and other established vocal parameters was statistically analyzed to establish cut-off values for healthy voices and mild to severe dysphonia. For external criteria, we intended to use objective acoustic–aerodynamic voice function diagnostics including voice range profile (VRP) measurements, dysphonia severity index (DSI) and vocal extent measure (VEM) calculations, as well as the subjective auditory–perceptual evaluation of voices by experienced examiners (GRB scale). Furthermore, the overall self-assessed vocal impairment (VHIs) served as an internal criterion.
2. Materials and Methods
2.1. Study Design and Patients
This study was conducted in accordance with the Declaration of Helsinki and approved by the local ethical review board. Selection criteria involved informed consent and the completion of the standard phoniatric examination procedures. After taking the medical history, all patients presenting in the Department of Audiology and Phoniatrics, Charité-Universitätsmedizin Berlin, Germany, received a digital videolaryngostroboscopy to assess the laryngeal findings and to establish a medical diagnosis. Subsequently, multidimensional voice function diagnostics were carried out as recommended by the European Laryngological Society (ELS) [1], starting with subjective evaluations (GRB, VHI-9i) and followed by objective voice function diagnostics (VRP, DSI, VEM). For subjective vocal self-assessment, patients completed the VHI-9i questionnaire. To estimate the voice use of every study participant, we also asked about their occupation and categorized them according to Koufman and Isaacson [23]: elite vocal performers (Level 1; e.g., actors, singers, voice artists), professional voice users (Level 2; e.g., teachers, politicians, moderators), non-vocal professionals (Level 3; e.g., lawyers, medical personnel, civil service employees), and non-vocal non-professionals (Level 4; e.g., IT staff, office workers, mechanics).
Between May 2009 and March 2021, a total of 17,660 consecutive cases were documented in the clinical database. To analyze the reliability of the VHI-9i, 718 patients were asked to complete the same questionnaire for a second time, without therapeutical intervention. The retest form had to be returned within one week to study the differences between the original answers and the retest. The second VHI-9i questionnaire was returned by 517 patients, corresponding to a response rate of 72%. Some questionnaires containing unanswered items or ambiguous checkmarks (e.g., between items) had to be excluded, resulting in 416 test–retest pairs.
The remaining 16,942 consecutive cases were analyzed to establish the validity of the questionnaire and to calculate statistically valid classification ranges. Since the VHI-9i should be compared with other established vocal parameters, only 7766 cases with complete multi-dimensional diagnostic assessment were considered. Cases with unreliable perturbation measures (jitter > 5%) were excluded, as recommended in the literature [1,24], resulting in a sample size of 6882. After another exclusion of follow-up visits, 3661 complete and unique cases were left for statistical analysis.
2.2. Subjective Examination Instruments
The VHI-9i represents an item-reduced short scale of the established VHI-30 [14], available in several languages (i.e., Dutch, English, French, German, Italian, Portuguese and Swedish). In this study, the German translation of the questionnaire was used (see Appendix A). Study participants were asked to answer all 9 items on a scale from 0 to 4 (0: never, 1: almost never, 2: sometimes, 3: almost always, 4: always), resulting in a total score between 0 and 36. The total score was then assigned to one of four dysphonia severity categories, ranging from 0 (healthy; 0 ≤ 5), 1 (mild; 6 ≤ 13), 2 (moderate; 14 ≤ 22), to 3 (severe; 23 ≤ 36). However, these categories correspond to a classification proposed by Nawka et al., based on the percentiles of a representative investigation of 716 patients [25]. Since these classification ranges have not yet been validated, statistical calculation of potential cut-off values for the VHI-9i classification was a main goal of this study.
Additionally, participants were asked to rate their overall voice impairment at present on a scale from 0 to 3 (0: normal, 1: mild, 2: moderate, 3: severe), the VHI summary assessment (VHIs). This index allows patients to assess how they feel about their voice with only one number. The relationship between VHI-9i and VHIs scores was examined to determine whether patients would rate themselves differently when asked about specific situations in their lives (VHI-9i items) or directly about their overall impairment (VHIs).
Apart from self-assessment, voices were also evaluated by auditory–perceptual assessment using the GRB system [26,27,28]. Based on the GRBAS scale, our department developed the modified GRB classification [29,30]. Only the first three criteria are used, focusing on the overall grade of hoarseness (G) and both main pathophysiological hoarseness components: roughness (R) and breathiness (B). The assessment of voice quality can be carried out more quickly and easily. Therefore, this system has become established in German-speaking countries and is also recommended in the ELS protocol [1]. Patients were asked to read the standardized text “The north wind and the sun” (German version), while the perceived G, R and B were scored on a scale from 0 to 3. To increase objectivity, each voice recording was rated independently by one experienced phoniatric physician and one senior speech–language therapist. The means were used for further exploration. While the degree of G serves as the overall indicator of dysphonia in the original GRBAS scale, it is regarded as gold standard for hoarseness evaluation in the GRB system presented here [31].
2.3. Objective Acoustic Assessment
For objective external validation criteria, we applied acoustic–aerodynamic voice function diagnostics. Voice recordings of all participants were conducted at the voice lab of our outpatient department, which is a sound-treated room with a background noise <40 dB(A). Study participants were asked to wear a head-mounted microphone with a stable mouth–microphone distance of 30 cm [32]. The equipment used for this purpose was the XION microphone headset (model number 352,009,010; XION GmbH, Berlin, Germany), which enables the realization of speech and singing VRP measurements and voice analyses under reproducible conditions. Technical microphone specifications include a frequency response of 70 Hz–20 kHz and a dynamic range of 40–120 dB(A). The microphone headset incorporates a calibrated audio interface that transmits digitized data to the PC via USB. The built-in electronics ensure the automatic calibration of the microphone connection without additional adjustments. The audio was processed via the DiVAS 2.8 software using the Singing Voice Analysis module (product number 350,020,013) and the Speaking Voice Analysis module (product number 350,020,024; XION GmbH, Berlin, Germany). VRP measurements were performed to show the functional interactions of different components of voice generation regarding vocal frequency and intensity [33,34]. The detailed procedure of VRP recordings is described in previous publications [35,36].
The established parameter DSI was automatically calculated as a weighted combination of the highest possible fundamental frequency, the lowest phonation intensity, maximum phonation time and jitter [37]. Regarding jitter, the waveform matching method was used for fundamental frequency extraction as it meets the high-precision criterion of being able to extract a 1% frequency change per cycle with a 1% accuracy, as long as the signal-to-noise ratio is greater than about 40 dB and concomitant amplitude modulations are below about 5% [24]. Measurements were conducted in a standing position. Subjects were asked to produce a sustained vowel (/na/ or /a/) for about 3 seconds at comfortable pitch and loudness. The most stable recording out of 3 trials was chosen for DSI calculation. Based on Gonnermann’s investigation of 495 subjects [38], the DSI scores were sorted into 4 severity categories, discriminating healthy voices (≥4.2) from mildly (<4.2 to ≥1.8), moderately (<1.8 to ≥−1.2), or severely (<−1.2) dysphonic voices. Since the DSI quantifies dysphonia as a negative criterion and involves the risk of imprecise results due to its multidimensional data acquisition, the one-dimensional parameter VEM was recently developed [35].
VEM calculation was performed automatically after VRP recording via the proprietary AVA software [39,40]. The VEM quantifies a subject’s dynamic performance and frequency range. It is calculated as a relation of the area and perimeter of the VRP and describes the vocal function by an interval-scaled value without unit, usually between 0 and 120. These limits may be exceeded at both ends by either severely impaired or exceptionally capable voices with a large ambitus and dynamic range. A small vocal capacity is described by a low VEM, a large VRP by a high VEM. The VEM emphasizes the vocal abilities and enables a classification of voice performance as a positive criterion [21,31,41]. Based on Müller’s investigation of 994 subjects [36], the resulting VEM scores were divided into percentiles, distinguishing a normal vocal capacity (≥108) from mildly reduced (<108 to ≥93), moderately (<93 to ≥69) and severely reduced (<69) vocal capacities.
Table 1 summarizes the severity classification of different objective and subjective vocal parameters by reference range. In contrast to the ordinally scaled GRB and VHIs, the classifications of metrically scaled parameters (VEM, VHI-30, VHI-9i) are based on the percentiles of the respective study cohorts (Level 0: 100th percentile/4th quartile; Level 1: 75th percentile/3rd quartile; Level 2: 50th percentile/2nd quartile; Level 3: 25th percentile/1st quartile).
3. Data Analysis
Statistical analysis was performed using IBM SPSS version 26.0.0.1. To establish the questionnaire as reliable, the absolute differences in total VHI-9i scores between test and retest were compared. An analysis of the differences of every single item in the questionnaire is individually important, but only the total scores are relevant in diagnostic practice. Paired-sample t-tests were used to check for biases, and correlations were established through Pearson’s r. To test the dependency of the VHI-9i total score on age, a regression analysis was performed. Gender differences were analyzed through independent sample t-tests. We checked for a dependency on voice use by means of the nonparametric Kruskal–Wallis H-test.
Before the cut-off points for the VHI-9i severity categories could be validated, the correlations between the VHI-9i and the severity classifications for VHIs, DSI, VEM, G, R and B had to be determined using Spearman’s rho (ϱ), in order to choose which of them was best suited for classification. These vocal parameters had to be balanced in terms of sensitivity (i.e., true positive rate, TPR) and specificity (i.e., true negative rate, TNR) when applied to the VHI-9i scores. Receiver operator characteristic (ROC) curves were used, which plot the TPR against the false positive rate (FPR = 1 − TNR). Since ROC is a binary classifier, the curves had to be plotted three times to establish possible cut-off points for every severity level (0 vs. 1–3, 0–1 vs. 2–3, 0–2 vs. 3). The area under the curve (AUC) was used to rank the performance of every curve to distinguish between two severity classes. Values between 0.8 and 0.9 are considered excellent, 0.7 to 0.8 acceptable, 0.5 to 0.7 poor.
Several methods exist to determine good class boundaries from ROC curves. As a starting point, we used Youden’s index (J) [42]. The highest J (Max J) is achieved when sensitivity and specificity are at optimal balance (J = TPR − FPR = TPR + TNR − 1). As a second possible class boundary, we determined the point where the number of correctly classified cases (CCCs) was the highest. The CCC is calculated as follows:
| CCC | = TPR | * (n cases of classifying index above class boundary) |
| + TNR | * (n cases of classifying index below class boundary) |
To find plausible cut-off values or categories of reasonable size, we selected a value between the two suggested class boundaries based on the median between Max J and Max CCC, also taking into account well over a decade of clinical experience with the VHI-9i.
4. Results
4.1. Test–Retest Reliability
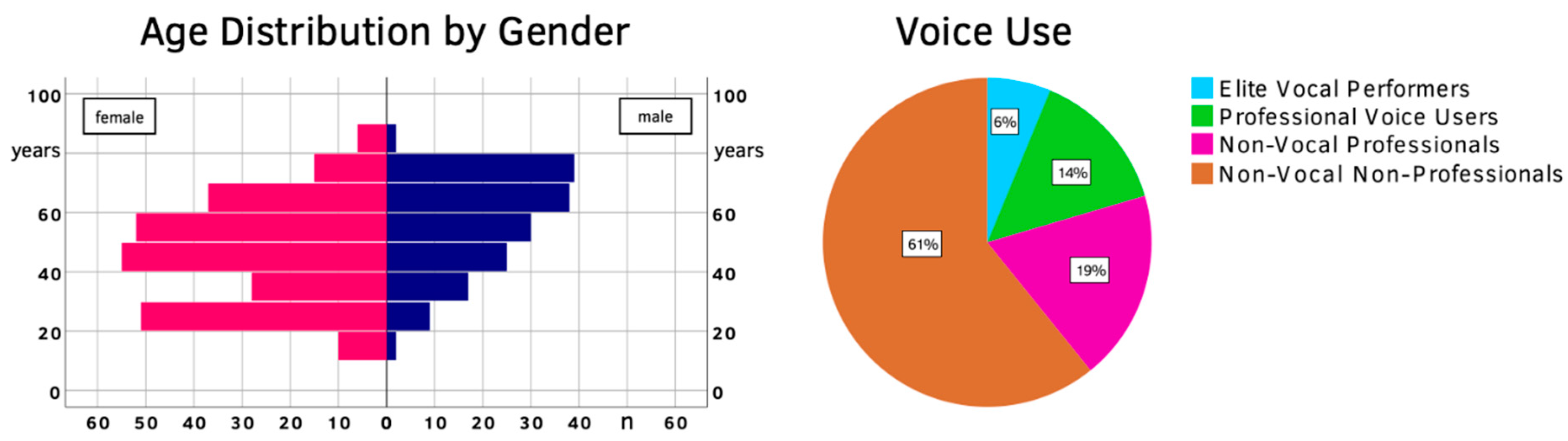
After eliminating all incomplete questionnaires, 416 test–retest pairs were left. The mean age (±SD) was 50 (±17), with males skewing generally older at 56 (±16) compared to female patients at 46 (±17) years of age. A total of 26 participants (6.3%) were classified as elite vocal performers, 59 as professional voice users (14.2%), 78 as non-vocal professionals (18.7%) and 253 as non-vocal non-professionals (60.8%). An overview of the test–retest population is given in Figure 1 and Table 2.
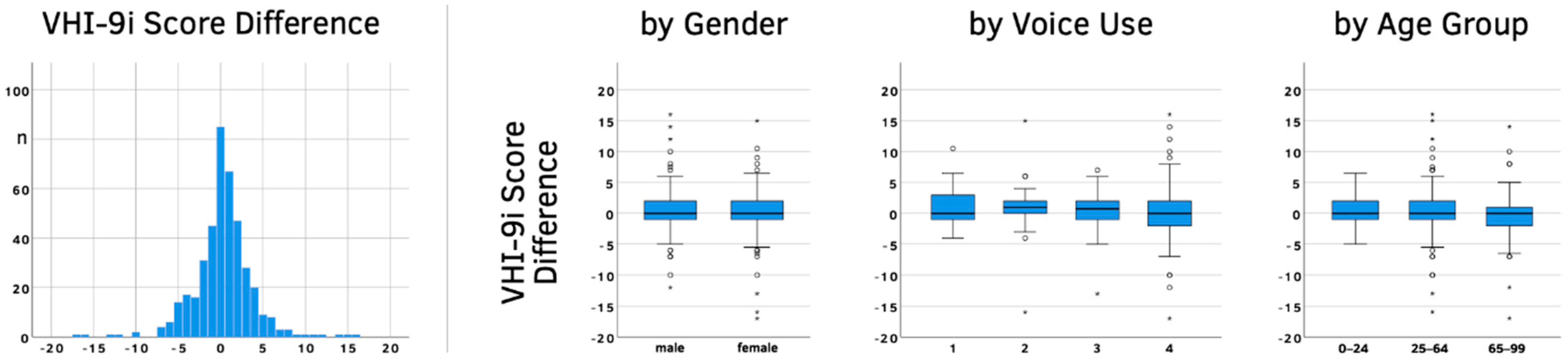
The median gap between test and retest was 2 days, with a mean of 3.3 days. The overall mean difference between VHI-9i scores (± SD) was very small at 0.25 (±3.52). Gender, voice use or age showed similarly minor differences (see Figure 2 and Table 2).
A paired-sample t-test between the VHI-9i total scores showed no significant differences (p = 0.146). Test and retest scores also correlated very well (r = 0.919, p < 0.01), indicating a highly reliable questionnaire. Only 5% of the population had a difference larger than 7 points. Gender had no impact on the reliability of the questionnaire. The independent sample t-test for the absolute VHI-9i score difference between males and females was not significant (p = 0.589). The level of voice use did also not affect reliability. The Kruskal–Wallis H-test showed no significance between the four voice use classifications (p = 0.701). The absolute score differences lightly depended on age. For every year of life, the difference rose by 0.016 points (p = 0.028).
4.2. Validation
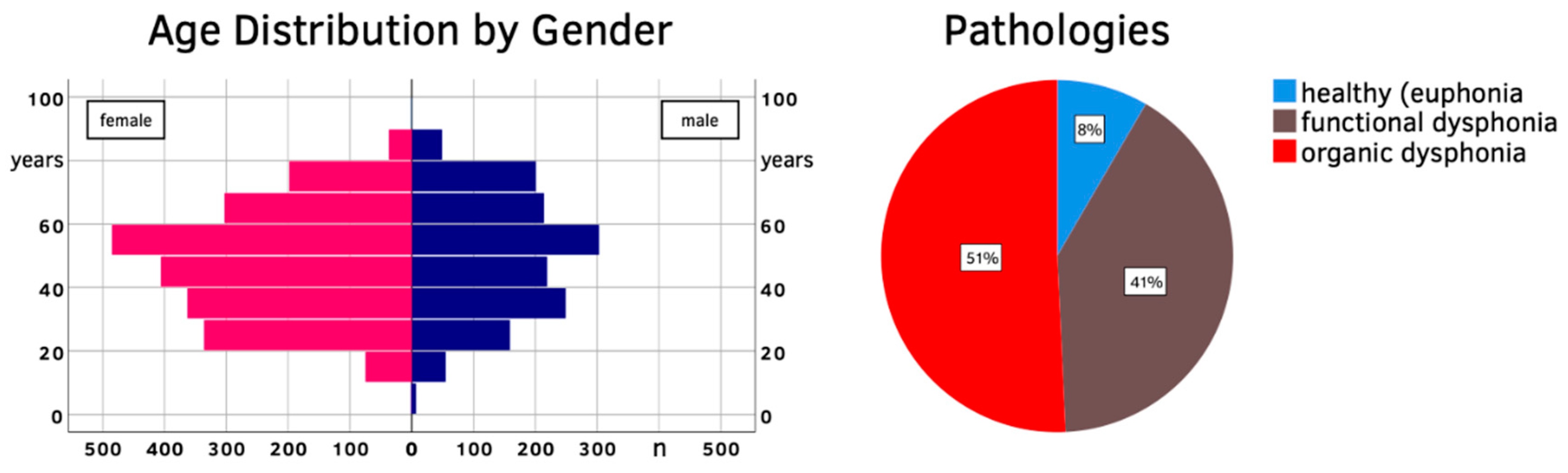
Of the 3661 participants remaining for VHI-9i validation, 1456 were male (39.8%) and 2205 were female (60.2%). The mean age (±SD) was 48 (±17), with males being on average slightly older at 50 (±18) years compared to females at 47 (±17) years of age. Vocal impairment was caused by functional dysphonia in 40.8% of the study population. Patients with organic dysphonia (50.8%) showed various pathologies: mostly lesions of the lamina propria (e.g., vocal fold nodules, polyps, cysts, Reinke’s edema), followed by benign and malignant changes of the epithelium (e.g., leukoplakia, papillomatosis, carcinoma), as well as neurogenic voice disorders (e.g., unilateral paralyses of the recurrent laryngeal nerve, spasmodic dysphonia). The remaining 8.4% were healthy subjects without dysphonia, mainly college applicants who presented to receive a vocal fitness examination, or prior to starting a profession associated with high vocal demands (e.g., teachers, singers, lecturers). The population pyramid and pathology classification are shown in Figure 3.
As the test–retest examinations demonstrated, the reliability of VHI-9i scores is not affected by gender or voice use. Although statistically significant, the age dependency is so small that it can be neglected in clinical practice. Therefore, all further observations and calculations were conducted for the entire population of 3661 participants. Using the old VHI-9i classification scale based on percentiles [25], 15.5% of our participants had healthy voices (total score 0 ≤ 5), 25.7% mild dysphonia (6 ≤ 13), 32.3% moderate (14 ≤ 22) and 26.5% severe dysphonia (23 ≤ 36). Applying the same method to the current database, 25% of patients had a score between 0 and 9, 50% up to 16, and 75% up to 22 points. The severity distribution for the other vocal parameters can be found in Table 3. Regarding VHIs, 63 cases had to be excluded (n = 3598 instead of 3661), because these test subjects had marked this question outside or in-between the provided options for the severity levels, rendering them invalid.
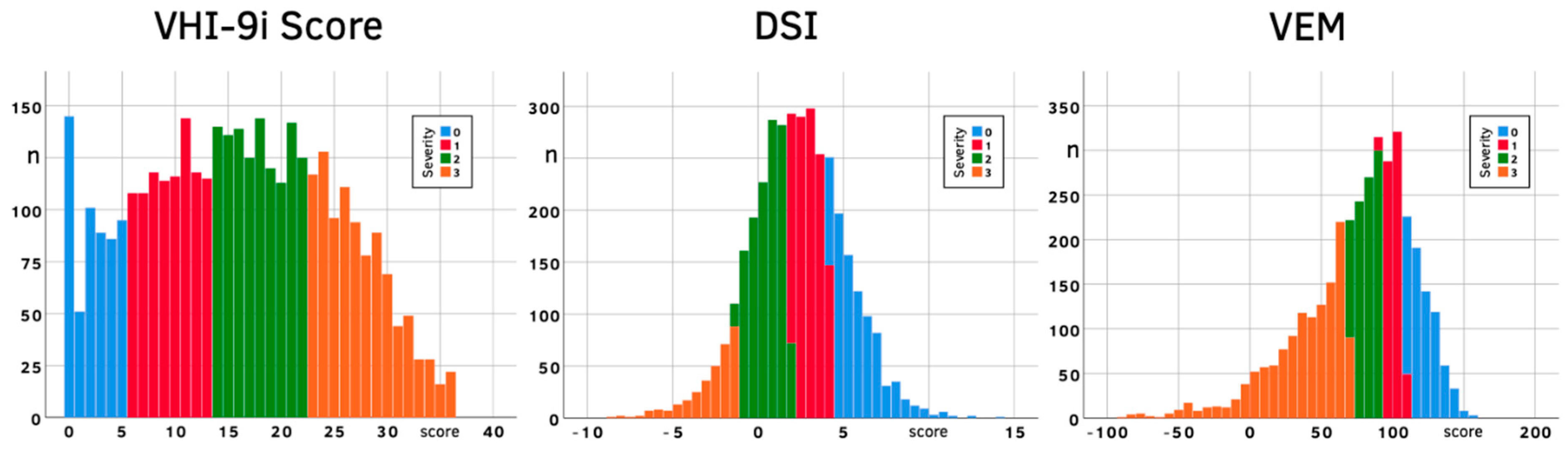
The size and mean of each severity category as well as the distribution of scores were notably different between parameters. The VHI-9i histogram shows a centered flat curve (skewness 0.063, kurtosis −0.90), the DSI is still centered but steeper (skewness −0.04, kurtosis 0.48) and the VEM is even steeper and skewed towards lower VEM values (skewness −1.08, kurtosis 1.94), with most patients falling into severity category 3 (Figure 4).
The VHI-9i total scores correlated the most with the VHIs, even though ϱ was only moderate (ϱ = 0.592; see Table 4). All other parameters correlated notably weaker with the VHI-9i. The objective DSI and VEM were also moderately correlated to each other at ϱ = 0.663. The distribution of subjects into G and R severity levels was rather similar, while B showed a different result with over 50% of all cases falling into the “healthy” category. G and R also had the strongest correlation among each other (ϱ = 0.871), reinforcing clinical experience that G serves as the gold standard for hoarseness evaluations via the GRB scale.
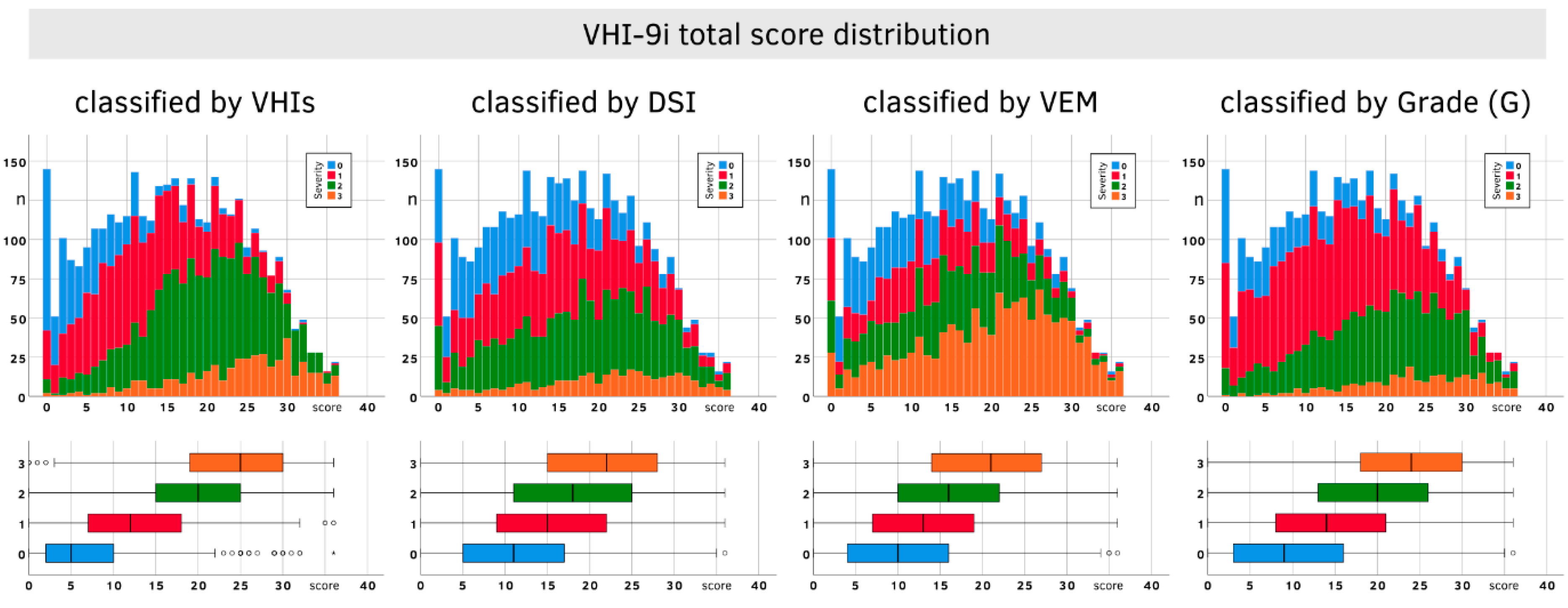
Figure 5 shows the distribution of VHI-9i total scores using the classifications for VHIs, DSI, VEM and G. The boxplots reveal a clear tendency: the higher the severity level, the higher the associated median. However, there is also a lot of overlap between the quartiles of different severity levels. This especially applies to DSI and VEM, which makes these parameters less suitable for VHI-9i classification.
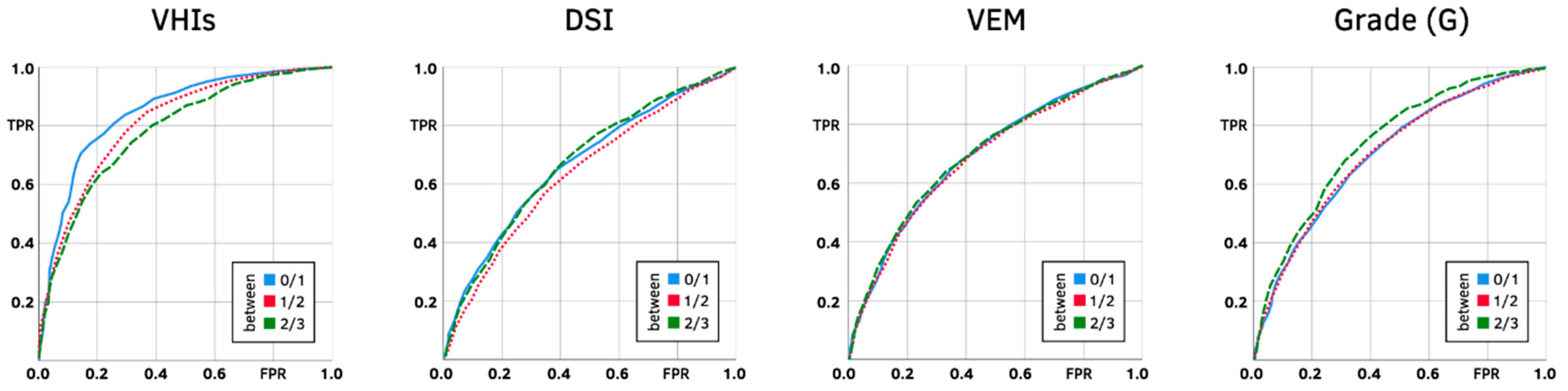
The ROC plots (Figure 6) also favor the VHIs as the best classifying index. DSI, VEM and G are visibly less suitable classifiers, because their curves are closer to the hypothetical diagonal through the ROC plot, signifying weaker discriminating performance.
The AUC results (Table 5) mirror the correlations of vocal parameters (compare Table 4). The best performance was achieved by the VHIs with excellent AUCs, followed by acceptable values for G. The parameters DSI and VEM turned out to be poor discriminators, with AUCs below 0.7.
As shown by our reliability analysis, severity categories must be at least 7 points in size to account for significant changes and minimize the possibility of retest artifacts. Neither optimizing for sensitivity and specificity (Max J) nor correctly classified cases (Max CCC) alone produced classes that were all wide enough (>7 points). Apart from the VHIs, Max CCC even produced cut-off recommendations that would eliminate the lowest (VEM) or lowest and highest (DSI, G) severity categories (highlighted in Table 5). Since both methods did not produce plausible cut-off values or categories of reasonable size, medians between the Max J and Max CCC measurements had to be calculated.
However, both median calculations did not always return the exact same result, which is why the J–CCC–Median cut-off values are expressed as ranges in Table 5. In general, the difference between both medians was below 0.25 points most of the time and very rarely exceeded 0.5 points. The medians for all vocal parameters agreed on the first boundary (i.e., between severity levels 0 and 1) at 7 or 8. Between “mild” and “moderate” (severity levels 1 and 2), the median recommendations ranged from 14 to 20. Except for the VEM, the medians led to a cut-off point between 26 and 28 for the boundary distinguishing “moderate” from “severe” impairment (i.e., severity levels 2 and 3).
5. Discussion
The VHI-9i short scale has proven to be a valuable diagnostic tool in our clinical practice for well over a decade. The total number of 17,660 consecutively completed questionnaires documented in our database confirms its high acceptance among patients and medical staff. In our test–retest analysis, the VHI-9i questionnaire demonstrated very high reliability independent of gender or voice use. Age had a minor influence, which we do not consider clinically relevant: For every year of life, the absolute score difference between test and retest increased by 0.016. If we applied that difference to the entire age range of our study population, the VHI-9i total score of an adolescent compared to a senior person would differ by about 1. The reliability analysis also showed that the severity classes for the VHI-9i need to be at least 7 points in size (2*SD of paired sample t-test), since only differences of 7 points and above account for significant changes and minimize the possibility of retest artifacts. Our interpretation of the ROC analysis had to consider this requirement. Unfortunately, neither optimizing for Max J nor Max CCC resulted in categories that were all large enough. Calculating the median between them for each cut-off point, however, yielded satisfactory results for clinical use.
All classification ranges are listed in Table 6. The Median J method strikes a good balance between sensitivity, specificity and the minimum class width of 7 points. The new boundary of a score of 7 corresponds directly with the VHIs Median J result for healthy voices (class 0). Finding a reasonable upper boundary for severity level 1 is more difficult: using VHIs Median J (a score of 14) would result in a category that is too small. The median for the expert auditory–perceptual assessment (G) points towards an even higher boundary (a score of 19). Since we were trying to find a mid-point for our severity classes, we decided to use the upper boundary of the 50% quartile (a score of 16). The upper boundary for severity level 2 (moderate impairment) can be taken once again from the VHIs Median J row, placing class 2 between 17 ≤ 26 and class 3 between 27 ≤ 36.
Compared to the old VHI-9i classification scale based on percentiles [25], the revised severity ranges classify more patients towards the lower categories. Severity level 3 is reduced by 4 points and is no longer the largest category. Level 1 and 2 start at higher class boundaries due to the size increase in level 0.
The best correlation was observed between VHI-9i and VHIs, making the overall self-assessed vocal impairment the best candidate for the validation process. However, the VHI-9i did not correlate well with the two objective parameters DSI and VEM, and had only slightly higher correlations with GRB. This supports recent studies that all these vocal parameters measure different aspects of a patient’s voice and are neither mutually interchangeable nor redundant [31,36,41,43]. Due to the weak correlations, poor discriminating performance and sometimes impossible cut-off points, DSI, VEM and G ultimately had no part in our recommendation for the revised VHI-9i cut-off points. It is important to remember that the VHI-9i does not measure objective voice impairment (DSI) or vocal capacity (VEM), but personal suffering due to a subjectively perceived vocal handicap. None of the parameters allow conclusions to be drawn about the diagnoses or underlying causes of the voice disorder.
Study Limitations
Over 60% of our test–retest population were categorized as non-vocal non-professionals. Ideally, the study would have included more subjects with professional backgrounds in singing, acting or teaching, especially since establishing independence from voice use was one of our goals during the rest-retest analysis. A bigger population of elite vocal performers and professional voice users would have been preferrable, but does not represent the actual proportions of our clinic clientele.
Furthermore, males are underrepresented in our study, so there may be participation bias. Despite the limited number of male subjects, we concluded that the VHI-9i was independent of gender, but a more balanced gender involvement would have been more representative. However, our clinical experience shows that women are generally more likely to see a doctor for voice problems.
In addition, signal-to-noise ratio (SNR) analysis and signal typing are considered to be important for valid and reliable perturbation measurements [44,45,46]. Unfortunately, this functionality is not included in the DiVAS software, which was specified in our study design as the main tool for objective voice analysis. One of the fundamental limitations of the DSI is the inclusion of jitter without sufficient evaluation of the signal type. In general, only type 1 and 2 are considered viable for perturbation analysis. The 5% jitter cut-off applied in our study was established to exclude type 4 signals only [46]. However, the categorization of a small test sample (n = 40) revealed signal type 1 and 2 exclusively, even for patients with low DSI and high jitter values. Furthermore, the majority of SNR results were between 42 and 50 dB (“recommended”), with a smaller number between 30 and 42 dB (“acceptable”) [45]. Therefore, we believe that our exclusion criteria were sufficient to eliminate voices which are not suitable for perturbation analysis. We recognize that this estimate cannot be taken as proof for the entire dataset and plan to include SNR and signal typing analyses in our future studies from the outset. It should also be noted that jitter was only used for DSI calculation, which proved to be irrelevant for the main goal of our study, i.e., a revised VHI-9i classification. Therefore, our recommendations regarding VHI-9i severity categories should not have been distorted.
Moreover, our initial ROC analysis produced boundary recommendations that were not feasible for diagnostic purposes. The resulting severity categories would have been either too small (<7 points) or would even not exist at all. Calculating the median between Max J and Max CCC is not a commonly used method for solving these problems. However, based on the frequent use of the VHI-9i in clinical investigations [18,19,20,21,22,31,36,41], it appears that the new classification will be a practical option for clinical settings.
In general, the auditory-perceptual assessment of voices via GRB was conducted only by two experienced examiners. Safer larger group judgments were not made. Due to the enormous number of cases (n = 17,660) and over a decade of diagnostic voice recordings, a retrospective blinded voice evaluation with 4-5 raters was not an option.
6. Conclusions
The VHI-9i is a reliable questionnaire which is independent of gender and professional voice use. Its dependency on age is negligible. Based on many years of clinical experience, it also has high acceptance among patients and medical staff, making it a valuable diagnostic tool.
The old cut-off values for the VHI-9i severity categories based on percentiles had to be adjusted. We recommend setting class 0 (healthy) between 0 ≤ 7, class 1 (mild impairment) between 8 ≤ 16, class 2 (moderate impairment) between 17 ≤ 26 and class 3 (severe impairment) between 27 ≤ 36.
The subjective VHI-9i does not correlate well with objective vocal parameters (DSI, VEM) or subjective auditory–perceptual assessment (GRB), reinforcing the notion that all these parameters measure different dimensions of a patient’s voice and are neither mutually interchangeable nor redundant.
Author Contributions
Conceptualization, T.N., M.S. and P.P.C.; Methodology, F.C., T.N. and P.P.C.; Literature Review, F.C. and P.P.C.; Investigation, T.N., M.S. and P.P.C.; Data Analysis, F.C. and K.N.; Original Draft Writing, F.C. and P.P.C.; Draft Review and Editing, F.C., T.N., K.N. and P.P.C.; Visualization, F.C. and K.N.; Supervision, T.N. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the Ethics Committee of Charité-Universitätsmedizin Berlin, Berlin, Germany (reference number: EA4/140/10).
Informed Consent Statement
Informed consent was obtained from all study participants.
Data Availability Statement
All data of the study are available in the Department of Audiology and Phoniatrics, Charité-Universitätsmedizin Berlin, Berlin, Germany.
Acknowledgments
The authors wish to thank Tatiana Ermakova for the statistical advice.
Conflicts of Interest
The authors declare no conflict of interest.
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table A1.
VHI-9i questionnaire items (German translation) as used in the study.
| Item Text | Score | ||||
|---|---|---|---|---|---|
| My voice makes it difficult for people to hear me. (Man hört mich wegen meiner Stimme schlecht.) | 0 | 1 | 2 | 3 | 4 |
| People have difficulty understanding me in a noisy room. (Anderen fällt es schwer, mich in einem lauten Raum zu verstehen.) | 0 | 1 | 2 | 3 | 4 |
| The sound of my voice varies throughout the day. (Der Klang meiner Stimme ändert sich im Laufe des Tages.) | 0 | 1 | 2 | 3 | 4 |
| My family has difficulty hearing me when I call them throughout the house. (Meine Familie hört mich kaum, wenn ich zuhause nach ihnen rufe.) | 0 | 1 | 2 | 3 | 4 |
| My voice difficulties restrict my personal and social life. (Meine Stimmschwierigkeiten schränken mich in meinem Privatleben ein.) | 0 | 1 | 2 | 3 | 4 |
| The clarity of my voice is unpredictable. (Bevor ich spreche, weiß ich nicht, wie klar meine Stimme klingen wird.) | 0 | 1 | 2 | 3 | 4 |
| My voice is worse in the evening. (Abends ist meine Stimme schlechter.) | 0 | 1 | 2 | 3 | 4 |
| I am less outgoing because of my voice problem. (Ich bin weniger kontaktfreudig wegen meines Stimmproblems.) | 0 | 1 | 2 | 3 | 4 |
| My voice makes me feel incompetent. (Wegen meiner Stimme fühle ich mich unfähig.) | 0 | 1 | 2 | 3 | 4 |
Scoring: 0 = never (nie), 1 = almost never (selten), 2 = sometimes (manchmal), 3 = almost always (oft), 4 = always (immer).
Table A2.
Global VHIs question added to the study questionnaire.
| Question | Score | |||
|---|---|---|---|---|
| How do you rate your voice today? (Wie schätzen Sie Ihre Stimme heute ein?) | 0 | 1 | 2 | 3 |
Scoring: 0 = normal (normal), 1 = mildly (leicht), 2 = moderately (mittelgradig), 3 = severely disturbed (hochgradig gestört).
References
- Dejonckere, P.H.; Bradley, P.; Clemente, P.; Cornut, G.; Crevier-Buchman, L.; Friedrich, G.; Van de Heyning, P.; Remacle, M.; Woisard, V. A basic protocol for functional assessment of voice pathology, especially for investigating the efficacy of (phonosurgical) treatments and evaluating new assessment techniques. Guideline elaborated by the Committee on Phoniatrics of the European Laryngological Society (ELS). Eur. Arch. Oto-Rhino-Laryngol. 2001, 258, 77–82. [Google Scholar] [CrossRef]
- Carding, P.N.; Wilson, J.; MacKenzie, K.; Deary, I.J. Measuring voice outcomes: State of the science review. J. Laryngol. Otol. 2009, 123, 823–829. [Google Scholar] [CrossRef]
- Sataloff, R.T. Professional voice users: The evaluation of voice disorders. Occup. Med. 2001, 16, 633–647. [Google Scholar]
- Mori, M.C.; Francis, D.O.; Song, P.C. Identifying Occupations at Risk for Laryngeal Disorders Requiring Specialty Voice Care. Otolaryngol. Neck Surg. 2017, 157, 670–675. [Google Scholar] [CrossRef] [PubMed]
- Jacobson, B.H.; Johnson, A.; Grywalski, C.; Silbergleit, A.; Jacobson, G.; Benninger, M.S.; Newman, C.W. The Voice Handicap Index (VHI): Development and Validation. Am. J. Speech Lang. Pathol. 1997, 6, 66–70. [Google Scholar] [CrossRef]
- Frajkova, Z.; Krizekova, A.; Missikova, V.; Tedla, M. Translation, Cross-Cultural Validation of the Voice Handicap Index (VHI-30) in Slovak Language. J. Voice 2020. [Google Scholar] [CrossRef]
- Sakaguchi, Y.; Kanazawa, T.; Okui, A.; Hirosaki, M.; Konomi, U.; Sotome, T.; Tashiro, N.; Kurihara, M.; Omae, T.; Nakayama, Y.; et al. Assessment of Dysphonia Using the Japanese Version of the Voice Handicap Index and Determination of Cutoff Points for Screening. J. Voice 2020. [Google Scholar] [CrossRef] [PubMed]
- Sotirović, J.; Grgurević, A.; Mumović, G.; Grgurević, U.; Pavićević, L.; Perić, A.; Erdoglija, M.; Milojević, M. Adaptation and Validation of the Voice Handicap Index (VHI)-30 into Serbian. J. Voice 2016, 30, 758.e1–758.e6. [Google Scholar] [CrossRef] [PubMed]
- Jaruchinda, P.; Suwanwarangkool, T. Cross-Cultural Adaptation and Validation of the Voice Handicap Index into Thai. J. Med. Assoc. Thail. 2015, 98, 1199–1208. [Google Scholar]
- Trinite, B.; Sokolovs, J. Adaptation and Validation of the Voice Handicap Index in Latvian. J. Voice 2014, 28, 452–457. [Google Scholar] [CrossRef]
- Nawka, T.; Wiesmann, U.; Gonnermann, U. Validation of the German version of the Voice Handicap Index (VHI). Hno 2003, 51, 921–929. [Google Scholar] [CrossRef] [PubMed]
- Leeuw, I.V.-D.; Kuik, D.; De Bodt, M.; Guimarães, I.; Holmberg, E.; Nawka, T.; Rosen, C.; Schindler, A.; Whurr, R.; Woisard, V. Validation of the Voice Handicap Index by Assessing Equivalence of European Translations. Folia Phoniatr. Logop. 2008, 60, 173–178. [Google Scholar] [CrossRef] [PubMed]
- Seifpanahi, S.; Jalaie, S.; Nikoo, M.R.; Sobhani-Rad, D. Translated Versions of Voice Handicap Index (VHI)-30 across Languages: A Systematic Review. Iran. J. Public Health 2015, 44, 458–469. [Google Scholar]
- Nawka, T.; Leeuw, I.V.-D.; De Bodt, M.; Guimarães, I.; Holmberg, E.; Rosen, C.; Schindler, A.; Woisard, V.; Whurr, R.; Konerding, U. Item Reduction of the Voice Handicap Index Based on the Original Version and on European Translations. Folia Phoniatr. Logop. 2009, 61, 37–48. [Google Scholar] [CrossRef]
- Hanschmann, H.; Lohmann, A.; Berger, R. Comparison of Subjective Assessment of Voice Disorders and Objective Voice Measurement. Folia Phoniatr. Logop. 2011, 63, 83–87. [Google Scholar] [CrossRef]
- Gilbert, M.R.; Gartner-Schmidt, J.L.; Rosen, C.A. The VHI-10 and VHI Item Reduction Translations—Are we all Speaking the Same Language? J. Voice 2017, 31, 250.e1–250.e7. [Google Scholar] [CrossRef] [PubMed]
- Rosen, C.A.; Lee, A.S.; Osborne, J.; Zullo, T.; Murry, T. Development and validation of the voice handicap index-10. Laryngoscope 2004, 114, 1549–1556. [Google Scholar] [CrossRef]
- Song, W.; Caffier, F.; Nawka, T.; Ermakova, T.; Martin, A.; Mürbe, D.; Caffier, P. T1a Glottic Cancer: Advances in Vocal Outcome Assessment after Transoral CO2-Laser Microsurgery Using the VEM. J. Clin. Med. 2021, 10, 1250. [Google Scholar] [CrossRef]
- Langenfeld, A.; Bohlender, J.E.; Swanenburg, J.; Brockmann-Bauser, M. Cervical Spine Disability in Correlation with Subjective Voice Handicap in Patients with Voice Disorders: A Retrospective Analysis. J. Voice 2020, 34, 371–379. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reetz, S.; Bohlender, J.E.; Brockmann-Bauser, M. Do Standard Instrumental Acoustic, Perceptual, and Subjective Voice Outcomes Indicate Therapy Success in Patients With Functional Dysphonia? J. Voice 2019, 33, 317–324. [Google Scholar] [CrossRef]
- Salmen, T.; Ermakova, T.; Schindler, A.; Ko, S.-R.; Göktas, O.; Gross, M.; Nawka, T.; Caffier, P. Efficacy of microsurgery in Reinke’s oedema evaluated by traditional voice assessment integrated with the Vocal Extent Measure (VEM). Acta Otorhinolaryngol. Ital. 2018, 38, 194–203. [Google Scholar] [CrossRef]
- Caffier, P.P.; Salmen, T.; Ermakova, T.; Forbes, E.; Ko, S.-R.; Song, W.; Gross, M.; Nawka, T. Phonomicrosurgery in Vocal Fold Nodules: Quantification of Outcomes in Professional and Non-Professional Voice Users. Med Probl. Perform. Artist. 2017, 32, 187–194. [Google Scholar] [CrossRef] [PubMed]
- Koufman, J.A.; Isaacson, G. The spectrum of vocal dysfunction. Otolaryngol. Clin. N. Am. 1991, 24, 985–988. [Google Scholar] [CrossRef]
- Titze, I.R.; Liang, H. Comparison of F o Extraction Methods for High-Precision Voice Perturbation Measurements. J. Speech Lang. Heart Res. 1993, 36, 1120–1133. [Google Scholar] [CrossRef] [PubMed]
- Nawka, T.; Rosanowski, F.; Gross, M. How to render an expert opinion on dysphonia. Laryngorhinootologie 2014, 93, 591–598. [Google Scholar]
- Hanschmann, H.; Berger, R. Perceptual and acoustic evaluation of hoarseness. Laryngorhinootologie 2011, 90, 68–70. [Google Scholar]
- Ptok, M.; Schwemmle, C.; Iven, C.; Jessen, M.; Nawka, T. On the auditory evaluation of voice quality. Hno 2006, 54, 793–802. [Google Scholar] [CrossRef]
- Schönweiler, R.; Wübbelt, P.; Hess, M.; Ptok, M. Psychoacoustic scaling of acoustic voice parameters by multicenter voice ratings. Laryngorhinootologie 2001, 80, 117–122. [Google Scholar] [CrossRef]
- Wendler, J.; Rauhut, A.; Krüger, H. Classification of voice qualities. J. Phon. 1986, 14, 483–488. [Google Scholar] [CrossRef]
- Anders, L.; Hollien, H.; Hurme, P.; Sonninen, A.; Wendler, J. Perception of Hoarseness by Several Classes of Listeners. Folia Phoniatr. Logop. 1988, 40, 91–100. [Google Scholar] [CrossRef] [PubMed]
- Seipelt, M.; Möller, A.; Nawka, T.; Gonnermann, U.; Caffier, F.; Caffier, P.P. Monitoring the Outcome of Phonosurgery and Vocal Exercises with Established and New Diagnostic Tools. BioMed Res. Int. 2020, 2020, 4208189. [Google Scholar] [CrossRef] [Green Version]
- Schutte, H.; Seidner, W. Recommendation by the Union of European Phoniatricians (UEP): Standardizing Voice Area Measurement/Phonetography. Folia Phoniatr. Logop. 1983, 35, 286–288. [Google Scholar] [CrossRef]
- Ternström, S.; Pabon, P.; Södersten, M.; Peter, P.; Maria, S. The Voice Range Profile: Its Function, Applications, Pitfalls and Potential. Acta Acust. United Acust. 2016, 102, 268–283. [Google Scholar] [CrossRef]
- Printz, T.; Godballe, C.; Grøntved, Å.M. The Dual-Microphone Voice Range Profile Assessment—Interrater Reliability. J. Voice 2020. [Google Scholar] [CrossRef] [PubMed]
- Caffier, P.P.; Möller, A.; Forbes, E.; Müller, C.; Freymann, M.-L.; Nawka, T. The Vocal Extent Measure: Development of a Novel Parameter in Voice Diagnostics and Initial Clinical Experience. BioMed Res. Int. 2018, 2018, 3836714. [Google Scholar] [CrossRef] [PubMed]
- Müller, C.; Caffier, F.; Nawka, T.; Müller, M.; Caffier, P.P. Pathology-Related Influences on the VEM: Three Years’ Experience since Implementation of a New Parameter in Phoniatric Voice Diagnostics. BioMed Res. Int. 2020, 2020, 5309508. [Google Scholar] [CrossRef] [PubMed]
- Wuyts, F.L.; Bodt, M.S.D.; Molenberghs, G.; Remacle, M.; Heylen, L.; Millet, B.; Lierde, K.V.; Raes, J.; Heyning, P.H.V.D. The dysphonia severity index: An objective measure of vocal quality based on a multiparameter approach. J. Speech Lang. Heart Res. 2000, 43, 796–809. [Google Scholar] [CrossRef]
- Gonnermann, U. Quantifizierbare Verfahren zur Bewertung von Dysphonien [Quantifiable Techniques for Evaluation of Dysphonia]; Peter Lang: Frankfurt/Main, Germany, 2007. [Google Scholar]
- Möller, A. Vocal Extent Measure as a New Parameter in Instrumental Voice Diagnostics. Unpublished. Bachelor Thesis, Fachhochschule Stralsund—University of Applied Sciences, Stralsund, Germany, 2010. [Google Scholar]
- Caffier, P.P.; Möller, A. Das Stimmumfangsmaß SUM als neuer Parameter in der objektiven Stimmdiagnostik. Sprache · Stimme · Gehör 2016, 40, 183–187. [Google Scholar] [CrossRef]
- Salmen, T.; Ermakova, T.; Möller, A.; Seipelt, M.; Weikert, S.; Rummich, J.; Gross, M.; Nawka, T.; Caffier, P.P. The Value of Vocal Extent Measure (VEM) Assessing Phonomicrosurgical Outcomes in Vocal Fold Polyps. J. Voice 2017, 31, 114.e7–114.e15. [Google Scholar] [CrossRef]
- Youden, W.J. Index for rating diagnostic tests. Cancer 1950, 3, 32–35. [Google Scholar] [CrossRef]
- Woisard, V.; Bodin, S.; Yardeni, E.; Puech, M. The Voice Handicap Index: Correlation Between Subjective Patient Response and Quantitative Assessment of Voice. J. Voice 2007, 21, 623–631. [Google Scholar] [CrossRef] [PubMed]
- Titze, I.R. Workshop on Acoustic Voice Analysis: Summary Statement; National Center for Voice and Speech: Iowa City, IA, USA, 1995. [Google Scholar]
- Deliyski, D.D.; Shaw, H.S.; Evans, M.K. Adverse Effects of Environmental Noise on Acoustic Voice Quality Measurements. J. Voice 2005, 19, 15–28. [Google Scholar] [CrossRef] [PubMed]
- Sprecher, A.; Olszewski, A.; Jiang, J.J.; Zhang, Y. Updating signal typing in voice: Addition of type 4 signals. J. Acoust. Soc. Am. 2010, 127, 3710–3716. [Google Scholar] [CrossRef] [PubMed] [Green Version]
Figure 1.
Overview of the test–retest population (age, gender, voice use classification).

Figure 2.
VHI-9i score difference between test and retest (total differences, by gender, by voice use, by age group). Age dependency was analyzed using discrete age values; age groups were only used in the diagram to improve the graphical representation. Circles (○) mark outliers (3rd quartile + 1.5*interquartile range; 1st quartile − 1.5*interquartile range) and asterisks (*) mark far outliers (3rd quartile + 3*interquartile range; 1st quartile − 3*interquartile range).
Figure 2.
VHI-9i score difference between test and retest (total differences, by gender, by voice use, by age group). Age dependency was analyzed using discrete age values; age groups were only used in the diagram to improve the graphical representation. Circles (○) mark outliers (3rd quartile + 1.5*interquartile range; 1st quartile − 1.5*interquartile range) and asterisks (*) mark far outliers (3rd quartile + 3*interquartile range; 1st quartile − 3*interquartile range).

Figure 3.
Overview of the validation population (age, gender, pathology classification).

Figure 4.
Observed VHI-9i, DSI and VEM scores with their associated severities.

Figure 5.
Distribution of VHI-9i total scores classified by VHIs, DSI, VEM and G severity levels. Upper row: stacked bar chart showing the number of subjects with their VHI-9i scores. Lower row: boxplots showing the percentiles of patients’ VHI-9i scores by severity level. Circles (○) and asterisks (*) mark outliers and far outliers.
Figure 5.
Distribution of VHI-9i total scores classified by VHIs, DSI, VEM and G severity levels. Upper row: stacked bar chart showing the number of subjects with their VHI-9i scores. Lower row: boxplots showing the percentiles of patients’ VHI-9i scores by severity level. Circles (○) and asterisks (*) mark outliers and far outliers.

Figure 6.
Combined ROC plots to determine cut-off points between severity categories 0 and 1 (blue), 1 and 2 (red), 2 and 3 (green).
Figure 6.
Combined ROC plots to determine cut-off points between severity categories 0 and 1 (blue), 1 and 2 (red), 2 and 3 (green).

Table 1.
Severity classification of different vocal parameters, assessed by study participants (VHI-30, VHI-9i, VHIs), experienced clinicians (GRB), and acoustic–aerodynamic analysis (VEM, DSI). Although all parameters share the same classification scale (0–3), equal levels of severity among different parameters do not imply equivalence (* classification ranges based on percentiles).
Table 1.
Severity classification of different vocal parameters, assessed by study participants (VHI-30, VHI-9i, VHIs), experienced clinicians (GRB), and acoustic–aerodynamic analysis (VEM, DSI). Although all parameters share the same classification scale (0–3), equal levels of severity among different parameters do not imply equivalence (* classification ranges based on percentiles).
| Level of Severity | VHI-30 *[25] | VHI-9i *[25] | VHIs | Grade (G) | VEM *[36] | DSI [38] |
|---|---|---|---|---|---|---|
| 0: healthy | 0 ≤ 14 | 0 ≤ 5 | 0 | 0 | ≥108 | ≥4.2 |
| 1: mild | 15 ≤ 28 | 6 ≤ 13 | 1 | 1 | 93 < 108 | 1.8 < 4.2 |
| 2: moderate | 29 ≤ 50 | 14 ≤ 22 | 2 | 2 | 69 < 93 | −1.2 < 1.8 |
| 3: severe | 51 ≤ 120 | 23 ≤ 36 | 3 | 3 | <69 | <−1.2 |
Table 2.
Study participant distribution and VHI-9i score differences between test and retest.
| Number n (%) | Mean Total Score Difference (±SD) | |
|---|---|---|
| Male | 162 (38.9%) | 0.38 (±3.68) |
| Female | 254 (61.1%) | 0.17 (±3.42) |
| Voice Use Level 1 | 26 (6.3%) | 0.75 (±3.45) |
| Voice Use Level 2 | 59 (14.2%) | 0.82 (±3.48) |
| Voice Use Level 3 | 78 (18.7%) | 0.40 (±2.91) |
| Voice Use Level 4 | 253 (60.8%) | 0.02 (±3.70) |
| Age Group 0–24 years | 46 (11.1%) | 0.41 (±2.17) |
| Age Group 25–64 years | 267 (64.2%) | 0.45 (±3.47) |
| Age Group 65–99 years | 103 (24.7%) | −0.33 (±4.06) |
Table 3.
Collected voice data by vocal parameter, classified according to the associated level of severity as shown in Table 1.
Table 3.
Collected voice data by vocal parameter, classified according to the associated level of severity as shown in Table 1.
| Vocal Parameter | Level of Severity | ||||
|---|---|---|---|---|---|
| 0: Healthy | 1: Mild | 2: Moderate | 3: Severe | ||
| VHIs | number (%) mean VHI-9i score (±SD) | 559 (15.5%) 6.6 (±6.8) | 1170 (32.5%) 12.8 (±7.2) | 1425 (39.6%) 19.5 (±7.4) | 444 (12.4%) 23.9 (±7.8) |
| DSI | number (%) mean VHI-9i score (±SD) | 879 (24.0%) 11.9 (±8.1) | 1210 (33.0%) 15.5 (±8.8) | 1244 (34.0%) 17.7 (±8.9) | 328 (9.0%) 21.0 (±8.5) |
| VEM | number (%) mean VHI-9i score (±SD) | 732 (20.0%) 11.1 (±8.0) | 673 (18.4%) 13.5 (±8.2) | 945 (25.8%) 15.7 (±8.3) | 1311 (35.8%) 19.9 (±8.8) |
| G | number (%) mean VHI-9i score (±SD) | 537 (14.7%) 10.4 (±8.3) | 1693 (46.2%) 14.2 (±8.4) | 1169 (31.9%) 19.1 (±8.4) | 262 (7.2%) 23.3 (±7.8) |
| R | number (%) mean VHI-9i score (±SD) | 602 (16.4%) 11.7 (±8.9) | 1864 (50.9%) 15.0 (±8.7) | 1031 (28.2%) 18.9 (±8.4) | 164 (4.5%) 21.8 (±8.2) |
| B | number (%) mean VHI-9i score (±SD) | 1865 (50.9%) 12.8 (±8.4) | 1205 (32.9%) 17.3 (±8.4) | 446 (12.2%) 21.8 (±8.1) | 145 (4.0%) 25.6 (±6.7) |
Table 4.
Results of correlation analysis between vocal parameters (Spearman’s rho). All correlation coefficients were significant (p < 0.001).
Table 4.
Results of correlation analysis between vocal parameters (Spearman’s rho). All correlation coefficients were significant (p < 0.001).
| VHIs (0–3) | DSI (0–3) | VEM (0–3) | G (0–3) | R (0–3) | B (0–3) | |
|---|---|---|---|---|---|---|
| VHI-9i | 0.592 | 0.292 | 0.373 | 0.393 | 0.299 | 0.386 |
| VHIs (0–3) | 0.229 | 0.261 | 0.328 | 0.263 | 0.287 | |
| DSI (0–3) | 0.663 | 0.525 | 0.454 | 0.494 | ||
| VEM (0–3) | 0.494 | 0.390 | 0.501 | |||
| G (0–3) | 0.871 | 0.665 | ||||
| R (0–3) | 0.449 |
Table 5.
ROC results for potential cut-offs between severity categories (0–1, 1–2, 2–3) using Max J, Max CCC and Median calculations. Yellow cells mark impossible cut-offs. Median calculations for every ROC parameter (TPR, FPR, J, CCC) resulted in slightly different class boundaries, which were specified by the ranges of cut-off values.
Table 5.
ROC results for potential cut-offs between severity categories (0–1, 1–2, 2–3) using Max J, Max CCC and Median calculations. Yellow cells mark impossible cut-offs. Median calculations for every ROC parameter (TPR, FPR, J, CCC) resulted in slightly different class boundaries, which were specified by the ranges of cut-off values.
| VHIs | G | ||||||
| Cut 0–1 | Cut 1–2 | Cut 2–3 | Cut 0–1 | Cut 1–2 | Cut 2–3 | ||
| AUC | 0.846 | 0.811 | 0.783 | 0.704 | 0.709 | 0.748 | |
| Max J | TPR | 0.737 | 0.781 | 0.743 | 0.633 | 0.664 | 0.683 |
| FPR | 0.174 | 0.298 | 0.316 | 0.33 | 0.352 | 0.311 | |
| J | 0.564 | 0.483 | 0.427 | 0.303 | 0.311 | 0.372 | |
| CCC | 2702 | 2674 | 2486 | 2336 | 2394 | 2521 | |
| cut-off | 11.5 | 14.75 | 19.5 | 13.5 | 16.75 | 20.5 | |
| Max CCC | TPR | 0.966 | 0.818 | 0.115 | 1 | 0.464 | 0 |
| FPR | 0.651 | 0.337 | 0.014 | 1 | 0.193 | 0 | |
| J | 0.315 | 0.481 | 0.101 | 0 | 0.271 | 0 | |
| CCC | 3132 | 2675 | 3162 | 3124 | 2464 | 3399 | |
| cut-off | 2.5 | 13.5 | 32.5 | 0 | 21.25 | 36 | |
| J–CCC–Median | TPR | 0.86 | 0.78 | 0.43 | 0.83 | 0.59 | 0.32 |
| FPR | 0.35 | 0.3 | 0.1 | 0.56 | 0.28 | 0.09 | |
| J | 0.51 | 0.48 | 0.33 | 0.27 | 0.31 | 0.23 | |
| CCC | 2988 | 2674 | 3026 | 2813 | 2443 | 3182 | |
| cut-off | 7–8 | 14–15 | 26–27 | 7–8 | 19 | 28 | |
| DSI | VEM | ||||||
| Cut 0–1 | Cut 1–2 | Cut 2–3 | Cut 0–1 | Cut 1–2 | Cut 2–3 | ||
| AUC | 0.667 | 0.64 | 0.674 | 0.692 | 0.689 | 0.699 | |
| Max J | TPR | 0.651 | 0.569 | 0.683 | 0.648 | 0.585 | 0.639 |
| FPR | 0.39 | 0.344 | 0.416 | 0.35 | 0.296 | 0.329 | |
| J | 0.26 | 0.226 | 0.267 | 0.298 | 0.289 | 0.31 | |
| CCC | 2346 | 2266 | 2170 | 2373 | 2309 | 2415 | |
| cut-off | 13.5 | 17.25 | 17.75 | 13.5 | 16.75 | 17.75 | |
| Max CCC | TPR | 1 | 0.408 | 0 | 1 | 0.786 | 0.44 |
| FPR | 1 | 0.216 | 0 | 1 | 0.537 | 0.167 | |
| J | 0 | 0.193 | 0 | 0 | 0.25 | 0.273 | |
| CCC | 2782 | 2280 | 3333 | 2929 | 2425 | 2535 | |
| cut-off | 0 | 21.75 | 36 | 0 | 10.75 | 22.5 | |
| J–CCC–Median | TPR | 0.83 | 0.48 | 0.3 | 0.83 | 0.66 | 0.53 |
| FPR | 0.66 | 0.28 | 0.13 | 0.61 | 0.38 | 0.23 | |
| J | 0.17 | 0.2 | 0.17 | 0.22 | 0.28 | 0.3 | |
| CCC | 2604 | 2266 | 3012 | 2718 | 2360 | 2512 | |
| cut-off | 7–8 | 18–20 | 26–27 | 7–8 | 14 | 20–21 | |
Table 6.
Sizes of severity classes based on Max J, Max CCC and Median calculations. Green cells serve as the basis for our proposed new VHI-9i severity classification.
Table 6.
Sizes of severity classes based on Max J, Max CCC and Median calculations. Green cells serve as the basis for our proposed new VHI-9i severity classification.
| Classifying Method | Level of Severity | |||
|---|---|---|---|---|
| 0: Healthy | 1: Mild | 2: Moderate | 3: Severe | |
| VHIs (Max J) | 0 ≤ 12 | 13 ≤ 15 | 16 ≤ 20 | 21 ≤ 36 |
| VHIs (Max CCC) | 0 ≤ 3 | 4 ≤ 14 | 15 ≤ 33 | 34 ≤ 36 |
| VHIs (Median J) | 0 ≤ 7 | 8 ≤ 14 | 15 ≤ 26 | 27 ≤ 36 |
| VHIs (Median CCC) | 0 ≤ 8 | 9 ≤ 15 | 16 ≤ 27 | 28 ≤ 36 |
| G (Max J) | 0 ≤ 14 | 15 ≤ 17 | 18 ≤ 21 | 22 ≤ 36 |
| G (Max CCC) | - | 0 ≤ 21 | 22 ≤ 36 | - |
| G (Median J) | 0 ≤ 7 | 8 ≤ 19 | 20 ≤ 28 | 29 ≤ 36 |
| G (Median CCC) | 0 ≤ 8 | 9 ≤ 19 | 20 ≤ 28 | 29 ≤ 36 |
| DSI (Max J) | 0 ≤ 14 | 15 ≤ 17 | 18 | 19 ≤ 36 |
| DSI (Max CCC) | - | 0 ≤ 22 | 23 ≤ 36 | - |
| DSI (Median J) | 0 ≤ 8 | 9 ≤ 20 | 21 ≤ 27 | 28 ≤ 36 |
| DSI (Median CCC) | 0 ≤ 8 | 9 ≤ 18 | 19 ≤ 26 | 27 ≤ 36 |
| VEM (Max J) | 0 ≤ 14 | 15 ≤ 17 | 18 | 19 ≤ 36 |
| VEM (Max CCC) | - | 0 ≤ 11 | 12 ≤ 23 | 24 ≤ 36 |
| VEM (Median J) | 0 ≤ 8 | 9 ≤ 14 | 15 ≤ 20 | 21 ≤ 36 |
| VEM (Median CCC) | 0 ≤ 7 | 8 ≤ 14 | 15 ≤ 21 | 22 ≤ 36 |
| VHI-9i quartiles | 0 ≤ 9 | 10 ≤ 16 | 17 ≤ 22 | 23 ≤ 36 |
| Proposed new classification | 0 ≤ 7 | 8 ≤ 16 | 17 ≤ 26 | 27 ≤ 36 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Caffier, F.; Nawka, T.; Neumann, K.; Seipelt, M.; Caffier, P.P. Validation and Classification of the 9-Item Voice Handicap Index (VHI-9i). J. Clin. Med. 2021, 10, 3325. https://doi.org/10.3390/jcm10153325
AMA Style
Caffier F, Nawka T, Neumann K, Seipelt M, Caffier PP. Validation and Classification of the 9-Item Voice Handicap Index (VHI-9i). Journal of Clinical Medicine. 2021; 10(15):3325. https://doi.org/10.3390/jcm10153325
Chicago/Turabian StyleCaffier, Felix, Tadeus Nawka, Konrad Neumann, Matthias Seipelt, and Philipp P. Caffier. 2021. "Validation and Classification of the 9-Item Voice Handicap Index (VHI-9i)" Journal of Clinical Medicine 10, no. 15: 3325. https://doi.org/10.3390/jcm10153325
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.