
Arthroscopy-Assisted Reduction and Internal Fixation versus Open Reduction and Internal Fixation for Glenoid Fracture with Scapular Involvement: A Retrospective Cohort Study

 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
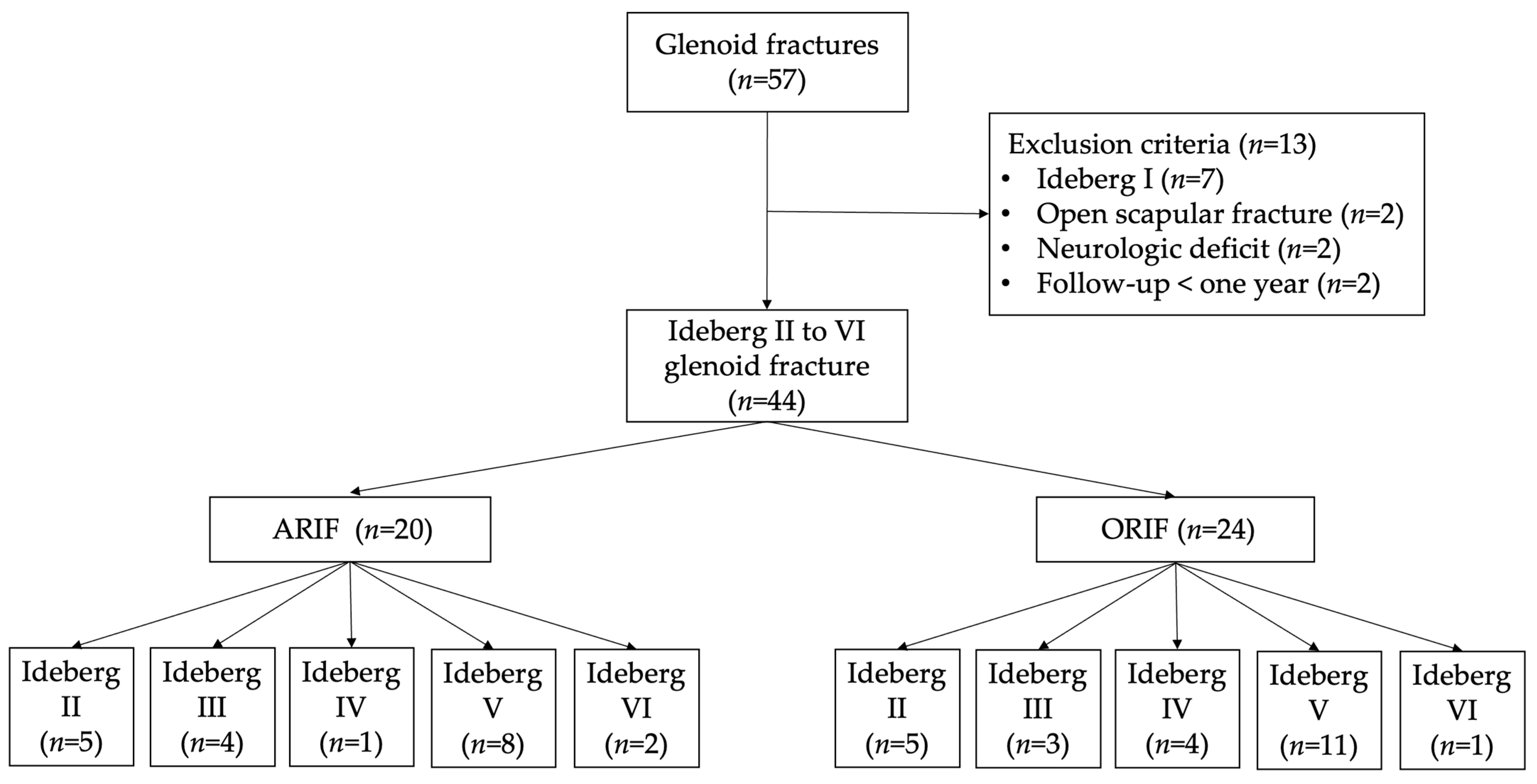
2.1. Patients
2.2. Preoperative Evaluation
2.3. Surgical Technique
2.4. Postoperative Protocol
2.5. Evaluation
2.6. Statistical Analysis
3. Results
3.1. Data Presentation and Population Comparison
3.2. Outcome Comparison
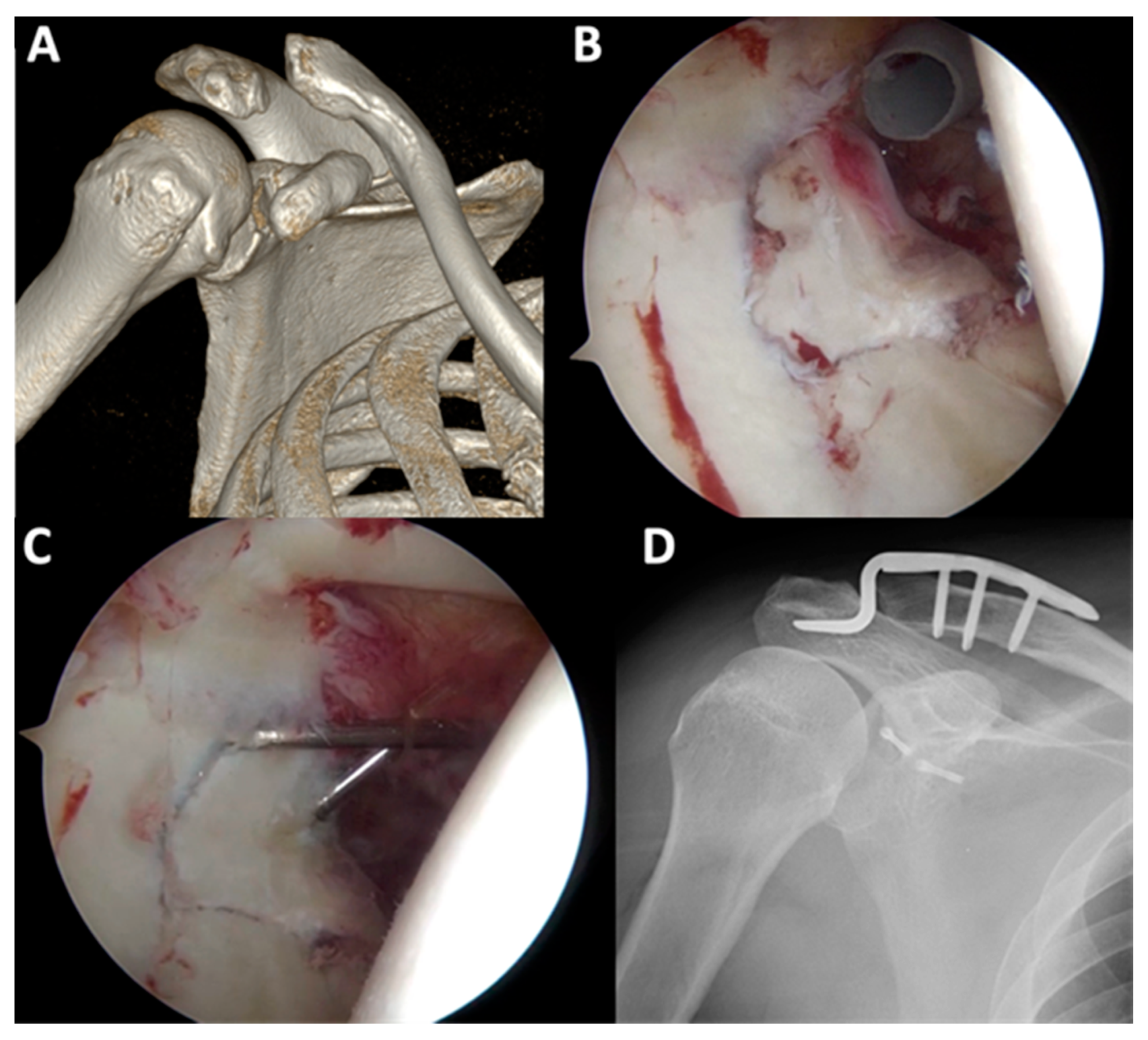
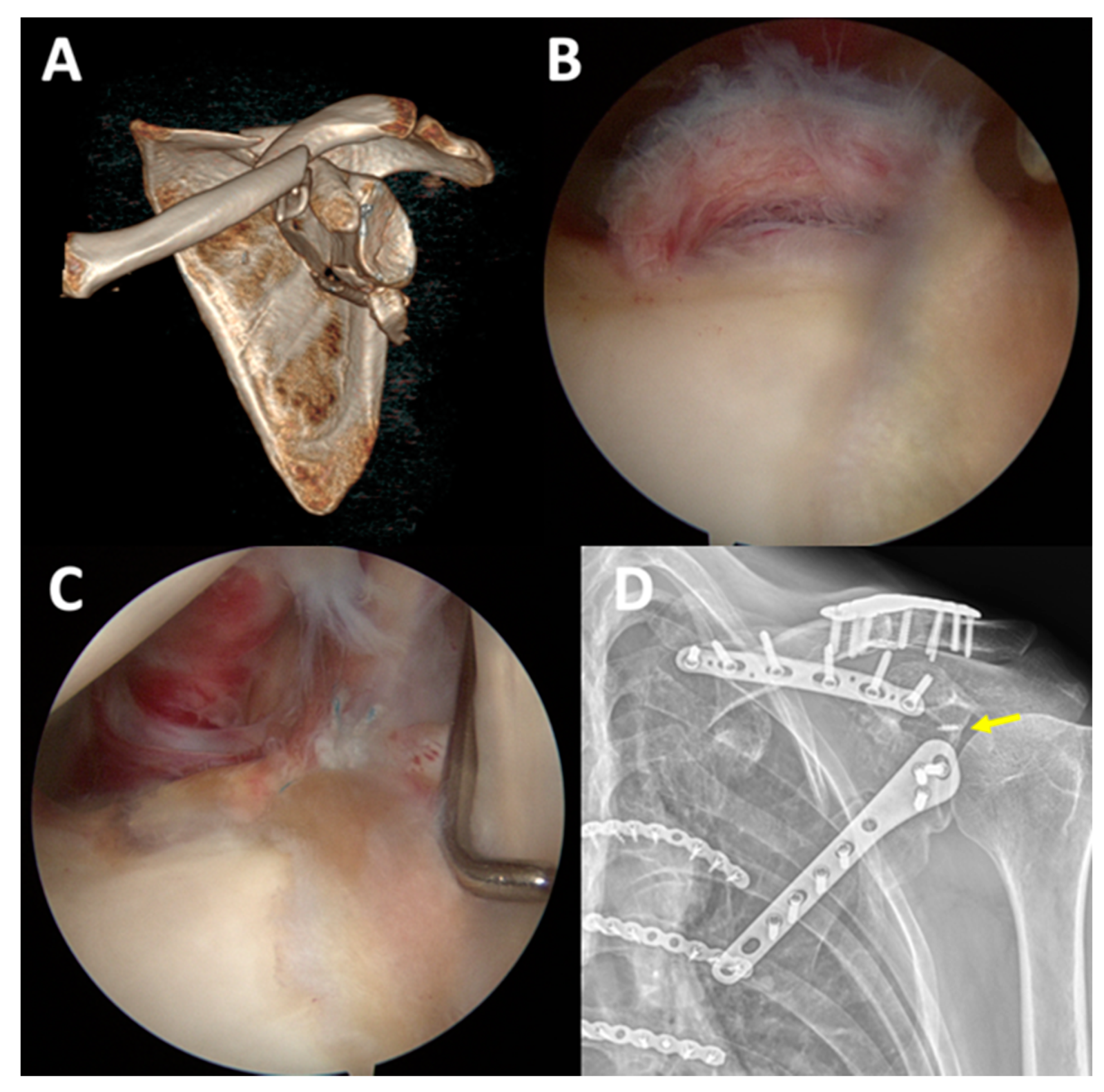
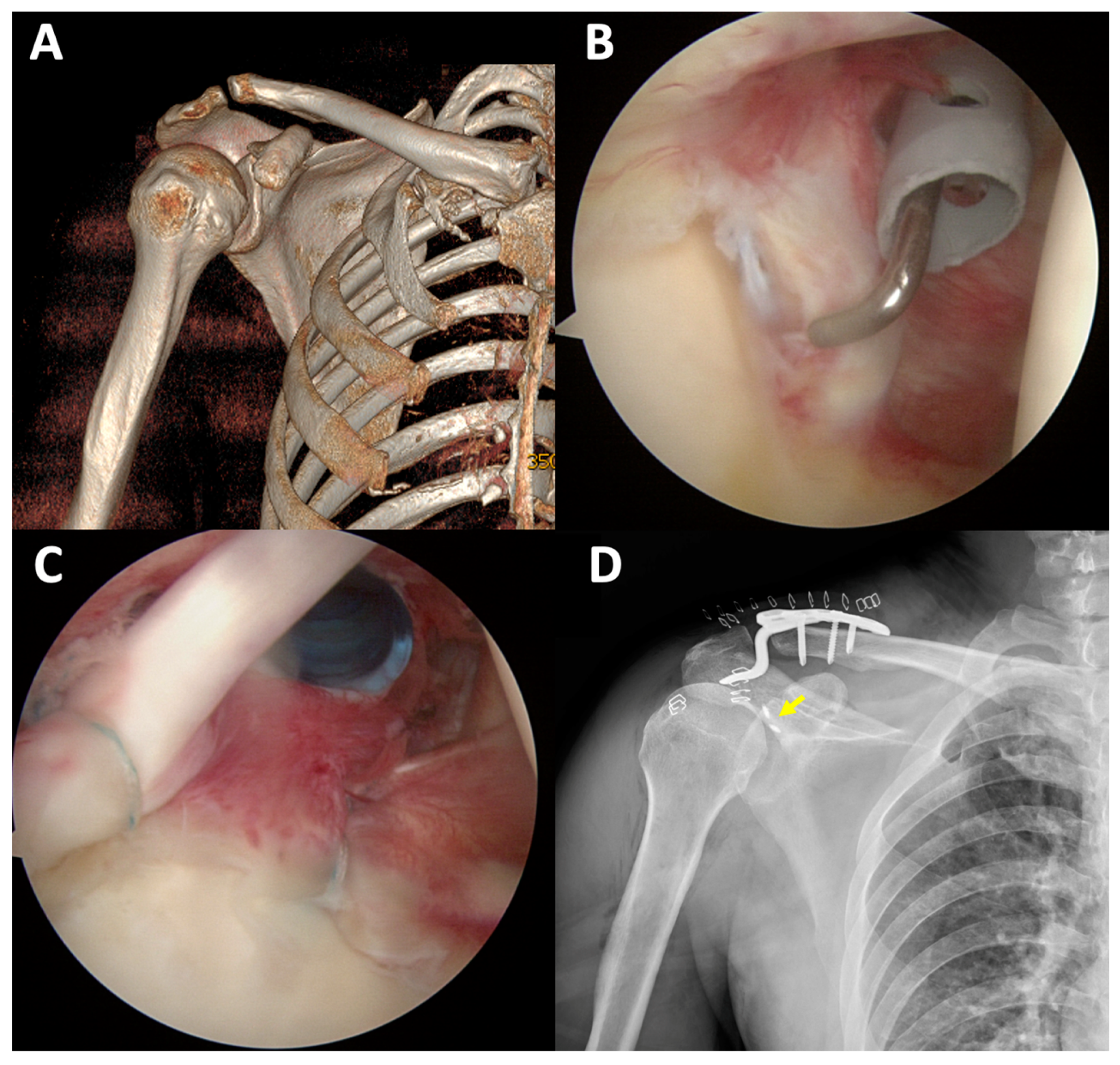
3.3. Arthroscopic Finding in ARIF and Case Presentation
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Armitage, B.M.; Wijdicks, C.A.; Tarkin, I.S.; Schroder, L.K.; Marek, D.J.; Zlowodzki, M.; Cole, P.A. Mapping of scapular fractures with three-dimensional computed tomography. J. Bone Jt. Surg. Am. 2009, 91, 2222–2228. [Google Scholar] [CrossRef]
- Ideberg, R.; Grevsten, S.; Larsson, S. Epidemiology of scapular fractures. Incidence and classification of 338 fractures. Acta Orthop. Scand. 1995, 66, 395–397. [Google Scholar] [CrossRef] [PubMed]
- Bahk, M.S.; Kuhn, J.E.; Galatz, L.M.; Connor, P.M.; Williams, G.R., Jr. Acromioclavicular and sternoclavicular injuries and clavicular, glenoid, and scapular fractures. J. Bone Jt. Surg. Am. 2009, 91, 2492–2510. [Google Scholar]
- Bucholz, R.W.; Heckman, J.D.; Court-Brown, C.M.; Tornetta, P., III; McQueen, M.; Ricci, W.M. Scapular fractures. In Rockwood and Green's Fractures in Adults, 7th ed.; Wolters Kluwer: Philadelphia, PA, USA, 2010; pp. 1144–1164. [Google Scholar]
- Frich, L.H.; Larsen, M.S. How to deal with a glenoid fracture. EFORT Open Rev. 2017, 2, 151–157. [Google Scholar] [CrossRef] [Green Version]
- Goss, T.P. Fractures of the glenoid cavity. J. Bone Jt. Surg. Am. 1992, 74, 299–305. [Google Scholar] [CrossRef]
- Van Oostveen, D.P.; Temmerman, O.P.; Burger, B.J.; van Noort, A.; Robinson, M. Glenoid fractures: A review of pathology, classification, treatment and results. Acta Orthop. Belg. 2014, 80, 88–98. [Google Scholar]
- Cole, P.A. Scapula fractures: Open reduction internal fixation. In Fractures, 2nd ed.; Wiss, D.A., Ed.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2006; pp. 15–36. [Google Scholar]
- Gauger, E.M.; Cole, P.A. Surgical technique: A minimally invasive approach to scapula neck and body fractures. Clin. Orthop. Relat. Res. 2011, 469, 3390–3399. [Google Scholar] [CrossRef] [Green Version]
- Obremskey, W.T.; Lyman, J.R. A modified judet approach to the scapula. J. Orthop. Trauma 2004, 18, 696–699. [Google Scholar] [CrossRef] [Green Version]
- Cameron, S.E. Arthroscopic reduction and internal fixation of an anterior glenoid fracture. Arthroscopy 1998, 14, 743–746. [Google Scholar] [CrossRef]
- Tauber, M.; Moursy, M.; Eppel, M.; Koller, H.; Resch, H. Arthroscopic screw fixation of large anterior glenoid fractures. Knee Surg. Sports Traumatol. Arthrosc. 2008, 16, 326–332. [Google Scholar] [CrossRef] [PubMed]
- Yang, H.B.; Wang, D.; He, X.J. Arthroscopic-assisted reduction and percutaneous cannulated screw fixation for Ideberg type III glenoid fractures: A minimum 2-year follow-up of 18 cases. Am. J. Sports Med. 2011, 39, 1923–1928. [Google Scholar] [CrossRef] [PubMed]
- Bauer, T.; Abadie, O.; Hardy, P. Arthroscopic treatment of glenoid fractures. Arthroscopy 2006, 22, 569.e1–569.e6. [Google Scholar] [CrossRef]
- Bonnevialle, N.; Clavert, P.; Arboucalot, M.; Bahlau, D.; Bauer, T.; Ehlinger, M. Contribution of arthroscopy in the treatment of anterior glenoid rim fractures: A comparison with open surgery. J. Shoulder Elb. Surg. 2019, 28, 42–47. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bauer, G.; Fleischmann, W.; Dussler, E. Displaced scapular fractures: Indication and long-term results of open reduction and internal fixation. Arch. Orthop. Trauma Surg. 1995, 114, 215–219. [Google Scholar] [CrossRef] [PubMed]
- Jones, C.B.; Cornelius, J.P.; Sietsema, D.L.; Ringler, J.R.; Endres, T.J. Modified Judet approach and minifragment fixation of scapular body and glenoid neck fractures. J. Orthop. Trauma 2009, 23, 558–564. [Google Scholar] [CrossRef]
- Owens, B.; Goss, T. Surgical approaches for glenoid fractures. Tech. Shoulder Elb. Surg. 2004, 5, 103–115. [Google Scholar] [CrossRef]
- Ao, R.; Yu, B.; Shi, J.; Li, Z.; Zhu, Y. Acromial approach for treating glenoid fractures: A report of two cases and a literature review. Exp. Ther. Med. 2015, 10, 1653–1656. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cole, P.A.; Gauger, E.M.; Schroder, L.K. Management of scapular fractures. J. Am. Acad. Orthop. Surg. 2012, 20, 130–141. [Google Scholar] [CrossRef] [Green Version]
- Bonnevialle, N.; Mansat, P.; Bellumore, Y.; Mansat, M.; Bonnevialle, P. Selective capsular repair for the treatment of anterior-inferior shoulder instability: Review of seventy-nine shoulders with seven years' average follow-up. J. Shoulder Elb. Surg. 2009, 18, 251–259. [Google Scholar] [CrossRef] [PubMed]
- Samilson, R.L.; Prieto, V. Dislocation arthropathy of the shoulder. J. Bone Jt. Surg. Am. 1983, 65, 456–460. [Google Scholar] [CrossRef]
- Sato, E.J.; Killian, M.L.; Choi, A.J.; Lin, E.; Choo, A.D.; Rodriguez-Soto, A.E.; Lim, C.T.; Thomopoulos, S.; Galatz, L.M.; Ward, S.R. Architectural and biochemical adaptations in skeletal muscle and bone following rotator cuff injury in a rat model. J. Bone Jt. Surg. Am. 2015, 97, 565–573. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ao, R.; Jian, Z.; Zhou, J.; Jiang, X.; Yu, B. A comparison of deltopectoral versus Judet approach for glenoid exposure. J. Shoulder Elb. Surg. 2020, 29, 370–373. [Google Scholar] [CrossRef]
- Scheibel, M.; Hug, K.; Gerhardt, C.; Krueger, D. Arthroscopic reduction and fixation of large solitary and multifragmented anterior glenoid rim fractures. J. Shoulder Elb. Surg. 2016, 25, 781–790. [Google Scholar] [CrossRef] [PubMed]
- Schandelmaier, P.; Blauth, M.; Schneider, C.; Krettek, C. Fractures of the glenoid treated by operation. A 5- to 23-year follow-up of 22 cases. J. Bone Jt. Surg. Br. 2002, 84, 173–177. [Google Scholar] [CrossRef]
- Adam, F.F. Surgical treatment of displaced fractures of the glenoid cavity. Int. Orthop. 2002, 26, 150–153. [Google Scholar] [CrossRef] [Green Version]
- Anavian, J.; Gauger, E.M.; Schroder, L.K.; Wijdicks, C.A.; Cole, P.A. Surgical and functional outcomes after operative management of complex and displaced intra-articular glenoid fractures. J. Bone Jt. Surg. Am. 2012, 94, 645–653. [Google Scholar] [CrossRef]
- Mayo, K.A.; Benirschke, S.K.; Mast, J.W. Displaced fractures of the glenoid fossa. Results of open reduction and internal fixation. Clin. Orthop. Relat. Res. 1998, 347, 122–130. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Surgery Type | |||
|---|---|---|---|
| Variables | ARIF (n = 20) | ORIF (n = 24) | p Value |
| Age, years (95% CI) | 41.15 (25–61) | 43.12 (21–65) | 0.667 |
| Gender in female, n (%) | 15 (75.0) | 19 (79.2) | 0.743 |
| Motor vehicle accidents, n (%) | 16 (80.0) | 22 (91.7) | 0.129 |
| Right laterality, n (%) | 8 (40.0) | 10 (41.7) | 0.563 |
| Dominant hand in right, n (%) | 20 (100.0) | 23 (95.8) | 0.890 |
| Ideberg classification | |||
| II, n (%) | 5 (25.0) | 5 (20.8) | 0.617 |
| III, n (%) | 4 (20.0) | 3 (12.5) | 0.774 |
| IV, n (%) | 1 (5.0) | 4 (16.7) | 0.128 |
| V, n (%) | 8 (40.0) | 11 (45.8) | 0.694 |
| VI, n (%) | 2 (10.0) | 1 (4.2) | 0.826 |
| Combined injury | |||
| Clavicle fracture, n (%) | 7 (35.0) | 7 (29.2) | 0.633 |
| Acromion fracture, n (%) | 2 (10.0) | 2 (8.3) | 0.704 |
| Coracoid fracture, n (%) | 1 (5.0) | 1 (4.2) | 0.896 |
| Acromioclavicular injury, n (%) | 4 (20.0) | 3 (12.5) | 0.741 |
| Nil, n (%) | 6 (30.0) | 11 (45.8) | 0.287 |
| Concomitant injury other than shoulder | |||
| Head injury, n (%) | 2 (10.0) | 2 (8.3) | 0.712 |
| Hemopneumothorax, n (%) | 4 (20.0) | 3 (12.5) | 0.807 |
| Upper extremity fracture, n (%) | 3 (15.0) | 2 (8.3) | 0.760 |
| Pelvic fracture, n (%) | 1 (5.0) | 1 (4.2) | 0.729 |
| Lower extremity fracture, n (%) | 2 (10.0) | 2 (8.3) | 0.761 |
| Nil, n (%) | 8 (40.0) | 14 (58.4) | 0.288 |
| Range of Motion | ARIF | ORIF | p Value |
|---|---|---|---|
| Forward elevation, ° (mean) | 175.5 ± 10.9 | 166.25 ± 33.0 | 0.239 |
| Lateral elevation, ° (mean) | 168 ± 20.4 | 165 ± 31.8 | 0.719 |
| External rotation, ° (mean) | 83.25 ± 7.6 | 80.41 ± 16.7 | 0.489 |
| Internal rotation (spine level) | T10±2 | T11±3 | 0.099 |
| ARIF | ORIF | p Value | |
|---|---|---|---|
| VAS | 1.5 ± 0.6 | 2.75 ± 1.45 | 0.001 |
| Constant score | 90.95 ± 9.2 | 86.62 ± 18.2 | 0.341 |
| DASH score | 6.84 ± 9.5 | 9.37 ± 21.3 | 0.626 |
| Patient No. | Arthroscopic Finding | Arthroscopic Procedure |
|---|---|---|
| 1 | Articular surface depressed | ARIF with 3.0 mm cannulated screw |
| 2 | Articular surface depressed | ARIF with 3.0 mm cannulated screw |
| 3 | Articular surface depressed | Chondral shaving |
| 4 | Articular surface depressed | ARIF with 3.0 mm cannulated screw |
| 5 | Articular surface depressed | ARIF with 2.4 mm headless screws |
| 6 | Articular surface depressed | ARIF with 3.0 mm cannulated screw |
| 7 | Articular surface depressed | ARIF with 3.0 mm cannulated screw |
| 8 | Articular surface depressed | ARIF with 3.0 mm cannulated screw |
| 9 | Articular surface depressed | ARIF with 3.0 mm cannulated screw |
| 10 | Articular surface depressed | Chondral shaving |
| 11 | Articular surface depressed, labrum tear | Chondral shaving |
| 12 | Articular surface depressed, labrum tear | Labrum repair with 2.8 mm suture anchor |
| 13 | Articular surface depressed, labrum tear | Labrum repair with 2.8 mm suture anchor |
| 14 | Articular surface depressed, labrum tear | ARIF with 3.0 mm cannulated screw |
| 15 | Articular surface depressed, labrum tear | ARIF with headless screws, labrum repair with 2.8 suture anchor |
| 16 | Articular surface depressed, labrum tear | labrum repair with 2.8 suture anchor |
| 17 | SLAP lesion | SLAP repair with Y-Knot® RC anchors |
| 18 | SLAP lesion | SLAP repair with Y-Knot® RC anchors |
| 19 | SLAP lesion | SLAP repair with Smith & Nephew TWINFIX anchors |
| 20 | SLAP lesion | SLAP repair with Y-Knot® RC anchors |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lin, I.-H.; Lin, T.-L.; Chang, H.-W.; Lin, C.-Y.; Tsai, C.-H.; Lo, C.-S.; Chen, H.-Y.; Chen, Y.-W.; Hsu, C.-J. Arthroscopy-Assisted Reduction and Internal Fixation versus Open Reduction and Internal Fixation for Glenoid Fracture with Scapular Involvement: A Retrospective Cohort Study. J. Clin. Med. 2022, 11, 1131. https://doi.org/10.3390/jcm11041131
Lin I-H, Lin T-L, Chang H-W, Lin C-Y, Tsai C-H, Lo C-S, Chen H-Y, Chen Y-W, Hsu C-J. Arthroscopy-Assisted Reduction and Internal Fixation versus Open Reduction and Internal Fixation for Glenoid Fracture with Scapular Involvement: A Retrospective Cohort Study. Journal of Clinical Medicine. 2022; 11(4):1131. https://doi.org/10.3390/jcm11041131
Chicago/Turabian StyleLin, I-Hao, Tsung-Li Lin, Hao-Wei Chang, Chia-Yu Lin, Chun-Hao Tsai, Chien-Sheng Lo, Hui-Yi Chen, Yi-Wen Chen, and Chin-Jung Hsu. 2022. "Arthroscopy-Assisted Reduction and Internal Fixation versus Open Reduction and Internal Fixation for Glenoid Fracture with Scapular Involvement: A Retrospective Cohort Study" Journal of Clinical Medicine 11, no. 4: 1131. https://doi.org/10.3390/jcm11041131