
Body Composition Assessment by Air-Displacement Plethysmography Compared to Dual-Energy X-ray Absorptiometry in Full-Term and Preterm Aged Three to Five Years

 , , ,
, , ,
Abstract
:1. Introduction
2. Material and Methods
2.1. Study Setting and Subjects
2.2. Data Collection and Measurements
2.3. Anthropometrics
2.4. Body Composition
C2 = Dfm/(Dffm − Dfm)
FM% = (C1/BD − C2) ∗ 100%
2.5. Statistical Analysis
3. Results
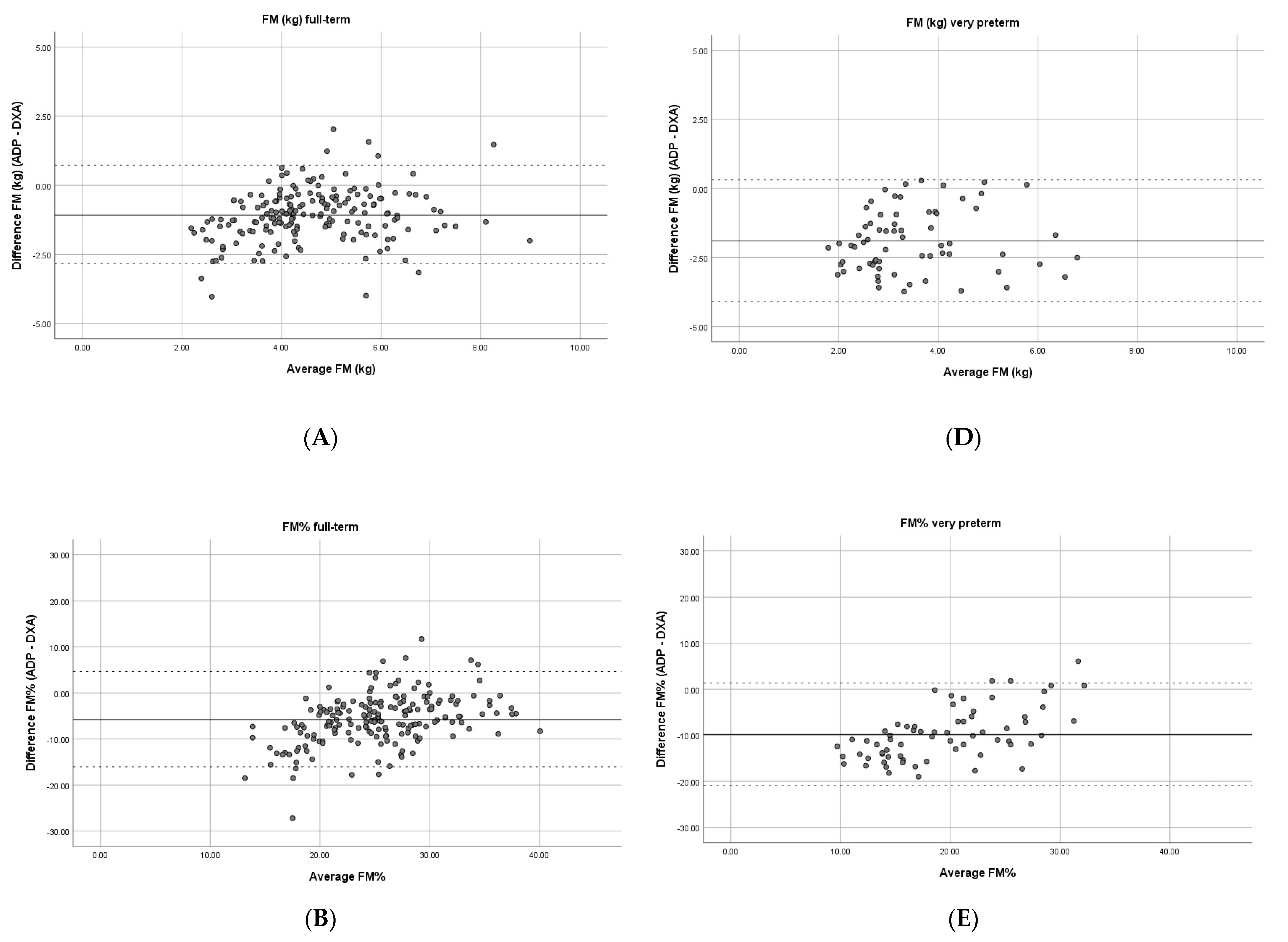
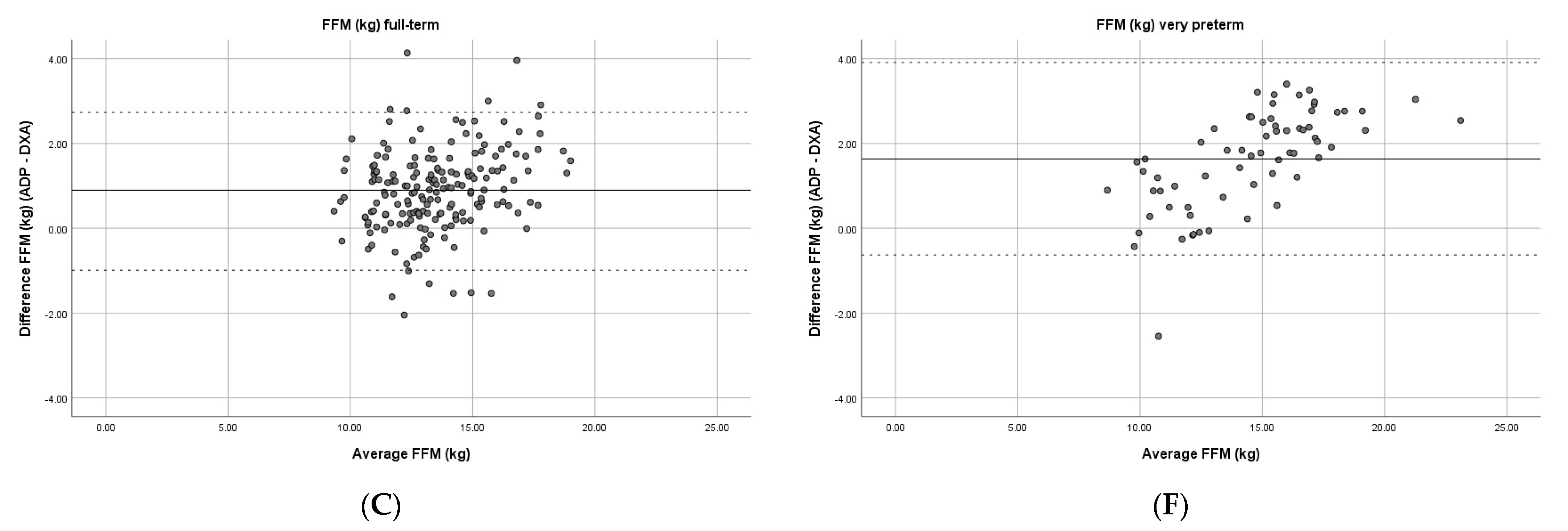
3.1. Comparison between ADP and DXA in Full-Term-Born Children
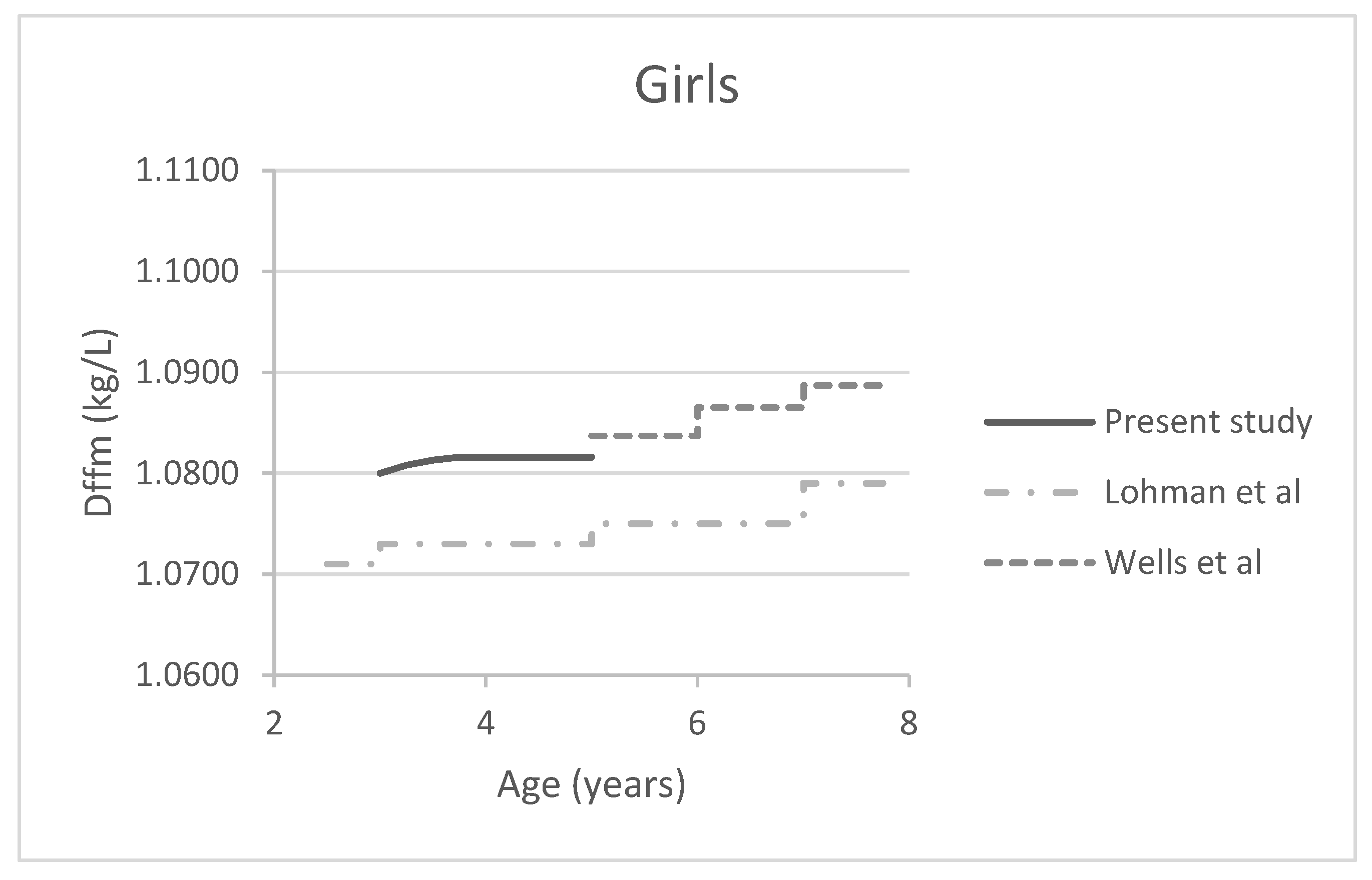
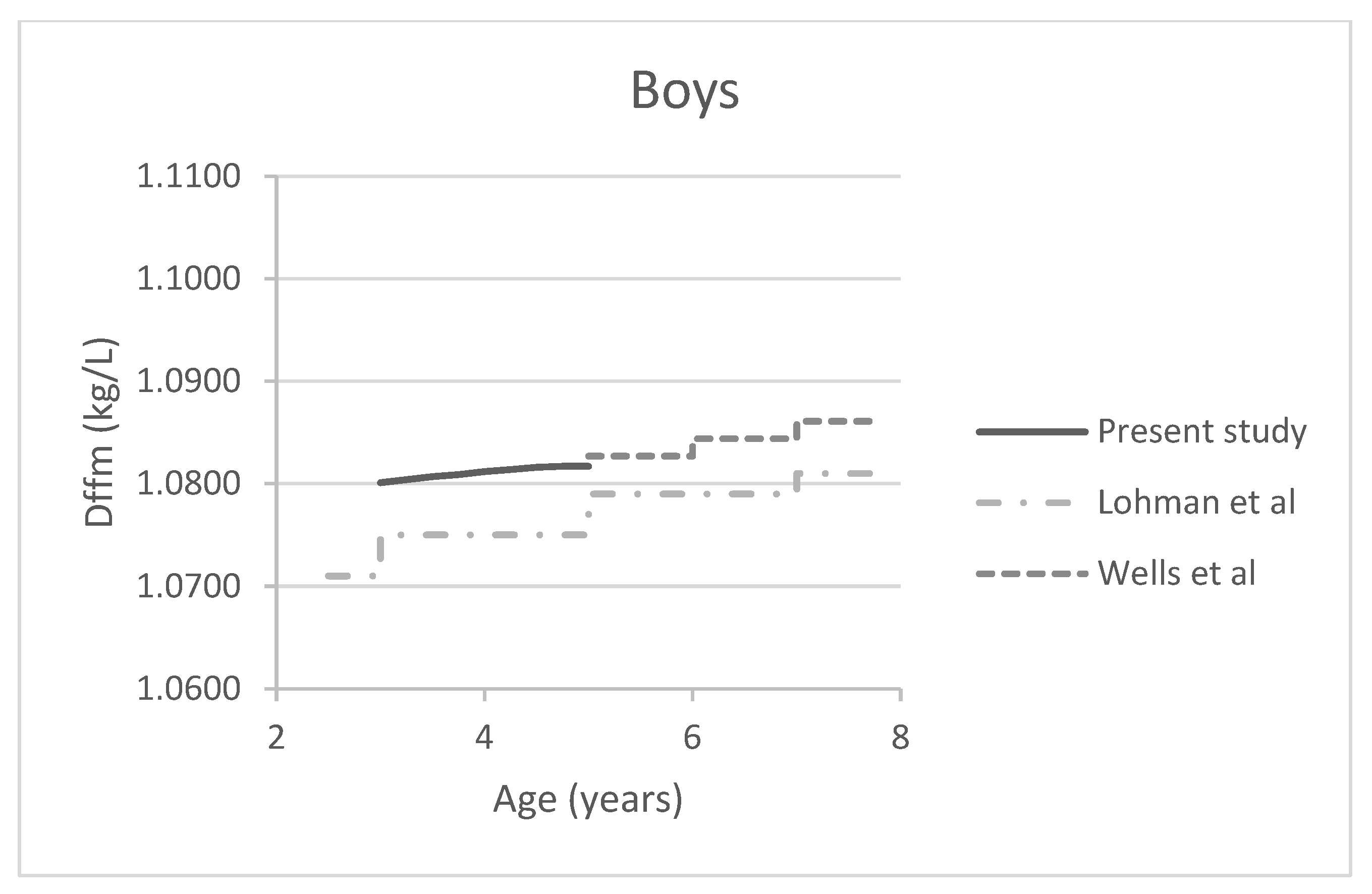
3.2. Revised FFM Density Model
3.3. Comparison between ADP and DXA in Very Preterm-Born Children
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- WHO. Report of the Commission on Ending Childhood Obesity; Report No. 9789241510066; World Health Organization: Geneva, Switzerland, 2016. [Google Scholar]
- Weihrauch-Bluher, S.; Schwarz, P.; Klusmann, J.H. Childhood obesity: Increased risk for cardiometabolic disease and cancer in adulthood. Metabolism. 2019, 92, 147–152. [Google Scholar] [CrossRef] [PubMed]
- Breij, L.M.; Kerkhof, G.F.; De Lucia Rolfe, E.; Ong, K.K.; Abrahamse-Berkeveld, M.; Acton, D.; Hokken-Koelega, A.C.S. Longitudinal fat mass and visceral fat during the first 6 months after birth in healthy infants: Support for a critical window for adiposity in early life. Pediatr. Obes. 2017, 12, 286–294. [Google Scholar] [CrossRef]
- Freedman, D.S.; Sherry, B. The validity of BMI as an indicator of body fatness and risk among children. Pediatrics 2009, 124 (Suppl. 1), S23–S34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Griffin, I.J.; Cooke, R.J. Development of whole body adiposity in preterm infants. Early Hum. Dev. 2012, 88 (Suppl. 1), S19–S24. [Google Scholar] [CrossRef] [PubMed]
- Gallagher, D.; Andres, A.; Fields, D.A.; Evans, W.J.; Kuczmarski, R.; Lowe, W.L., Jr.; Lumeng, J.C.; Oken, E.; Shepherd, J.A.; Sun, S. Body composition measurements from birth through 5 years: Challenges, gaps, and existing & emerging technologies—A National Institutes of Health Workshop. Obes. Rev. 2020, 21, e13033. [Google Scholar]
- Zanini Rde, V.; Santos, I.S.; Chrestani, M.A.; Gigante, D.P. Body fat in children measured by DXA, air-displacement plethysmography, TBW and multicomponent models: A systematic review. Matern. Child Health J. 2015, 19, 1567–1573. [Google Scholar] [CrossRef] [PubMed]
- de Fluiter, K.S.; van Beijsterveldt, I.; Goedegebuure, W.J.; Breij, L.M.; Spaans, A.M.J.; Acton, D.; Hokken-Koelega, A.C.S. Longitudinal body composition assessment in healthy term-born infants until 2 years of age using ADP and DXA with vacuum cushion. Eur. J. Clin. Nutr. 2020, 74, 642–650. [Google Scholar] [CrossRef] [PubMed]
- van Beijsterveldt, I.; van der Steen, M.; de Fluiter, K.S.; Spaans, S.; Hokken-Koelega, A.C.S. Body composition and bone mineral density by Dual Energy X-ray Absorptiometry: Reference values for young children. Clin. Nutr. 2021, 41, 71–79. [Google Scholar] [CrossRef] [PubMed]
- Fields, D.A.; Goran, M.I.; McCrory, M.A. Body-composition assessment via air-displacement plethysmography in adults and children: A review. Am. J. Clin. Nutr. 2002, 75, 453–467. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ma, G.; Yao, M.; Liu, Y.; Lin, A.; Zou, H.; Urlando, A.; Wong, W.W.; Nommsen-Rivers, L.; Dewey, K.G. Validation of a new pediatric air-displacement plethysmograph for assessing body composition in infants. Am. J. Clin. Nutr. 2004, 79, 653–660. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mazahery, H.; von Hurst, P.R.; McKinlay, C.J.D.; Cormack, B.E.; Conlon, C.A. Air displacement plethysmography (pea pod) in full-term and pre-term infants: A comprehensive review of accuracy, reproducibility, and practical challenges. Matern. Health Neonatol. Perinatol. 2018, 4, 12. [Google Scholar] [CrossRef] [PubMed]
- Fields, D.A.; Allison, D.B. Air-displacement plethysmography pediatric option in 2-6 years old using the four-compartment model as a criterion method. Obesity 2012, 20, 1732–1737. [Google Scholar] [CrossRef]
- Lohman, T.G. Assessment of body composition in children. Pediatric Exerc. Sci. 1989, 1, 19–30. [Google Scholar] [CrossRef]
- Fomon, S.J.; Haschke, F.; Ziegler, E.E.; Nelson, S.E. Body composition of reference children from birth to age 10 years. Am. J. Clin. Nutr. 1982, 35 (Suppl. 5), 1169–1175. [Google Scholar] [CrossRef]
- Wells, J.C.; Williams, J.E.; Chomtho, S.; Darch, T.; Grijalva-Eternod, C.; Kennedy, K.; Haroun, D.; Wilson, C.; Cole, T.J.; Fewtrell, M.S. Pediatric reference data for lean tissue properties: Density and hydration from age 5 to 20 y. Am. J. Clin. Nutr. 2010, 91, 610–618. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Delisle Nystrom, C.; Soderstrom, E.; Henriksson, P.; Henriksson, H.; Poortvliet, E.; Lof, M. The paediatric option for BodPod to assess body composition in preschool children: What fat-free mass density values should be used? Br. J. Nutr. 2018, 120, 797–802. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nunez, C.; Kovera, A.J.; Pietrobelli, A.; Heshka, S.; Horlick, M.; Kehayias, J.J.; Wang, Z.; Heymsfield, S.B. Body composition in children and adults by air displacement plethysmography. Eur. J. Clin. Nutr. 1999, 53, 382–387. [Google Scholar] [CrossRef] [Green Version]
- Sardinha, L.B.; Lohman, T.G.; Teixeira, P.J.; Guedes, D.P.; Going, S.B. Comparison of air displacement plethysmography with dual-energy X-ray absorptiometry and 3 field methods for estimating body composition in middle-aged men. Am. J. Clin. Nutr. 1998, 68, 786–793. [Google Scholar] [CrossRef] [PubMed]
- Radley, D.; Gately, P.J.; Cooke, C.B.; Carroll, S.; Oldroyd, B.; Truscott, J.G. Estimates of percentage body fat in young adolescents: A comparison of dual-energy X-ray absorptiometry and air displacement plethysmography. Eur. J. Clin. Nutr. 2003, 57, 1402–1410. [Google Scholar] [CrossRef] [Green Version]
- Breij, L.M.; Steegers-Theunissen, R.P.; Briceno, D.; Hokken-Koelega, A.C. Maternal and Fetal Determinants of Neonatal Body Composition. Horm. Res. Paediatr. 2015, 84, 388–395. [Google Scholar] [CrossRef] [PubMed]
- de Fluiter, K.S.; van Beijsterveldt, I.; Breij, L.M.; Acton, D.; Hokken-Koelega, A.C.S. Association Between Fat Mass in Early Life and Later Fat Mass Trajectories. JAMA Pediatr. 2020, 174, 1141–1148. [Google Scholar] [CrossRef] [PubMed]
- Roelants, J.A.; Joosten, K.F.M.; van der Geest, B.M.A.; Hulst, J.M.; Reiss, I.K.M.; Vermeulen, M.J. First week weight dip and reaching growth targets in early life in preterm infants. Clin. Nutr. 2018, 37, 1526–1533. [Google Scholar] [CrossRef] [PubMed]
- Fenton, T.R.; Kim, J.H. A systematic review and meta-analysis to revise the Fenton growth chart for preterm infants. BMC Pediatr. 2013, 13, 59. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schönbeck, Y.; Talma, H.; van Dommelen, P.; Bakker, B.; Buitendijk, S.E.; HiraSing, R.A.; van Buuren, S. The world’s tallest nation has stopped growing taller: The height of Dutch children from 1955 to 2009. Pediatr. Res. 2013, 73, 371–377. [Google Scholar] [CrossRef] [PubMed]
- Lohman, T.G. Applicability of body composition techniques and constants for children and youths. Exerc. Sport Sci. Rev. 1986, 14, 325–357. [Google Scholar] [CrossRef] [PubMed]
- Rigby, R.A.; Stasinopoulos, D.M. Smooth centile curves for skew and kurtotic data modelled using the Box-Cox power exponential distribution. Stat. Med. 2004, 23, 3053–3076. [Google Scholar] [CrossRef] [PubMed]
- Rigby, R.A.; Stasinopoulos, D.M. Generalized additive models for location, scale and shape. J. R. Stat. Soc. Ser. C 2005, 54, 507–554. [Google Scholar] [CrossRef] [Green Version]
- Fields, D.A.; Demerath, E.W.; Pietrobelli, A.; Chandler-Laney, P.C. Body composition at 6 months of life: Comparison of air displacement plethysmography and dual-energy X-ray absorptiometry. Obesity 2012, 20, 2302–2306. [Google Scholar] [CrossRef] [PubMed]
- Wrottesley, S.V.; Pisa, P.T.; Micklesfield, L.K.; Pettifor, J.M.; Norris, S.A. A comparison of body composition estimates using dual-energy X-ray absorptiometry and air-displacement plethysmography in South African neonates. Eur. J. Clin. Nutr. 2016, 70, 1254–1258. [Google Scholar] [CrossRef] [PubMed]
- Radley, D.; Gately, P.J.; Cooke, C.B.; Carroll, S.; Oldroyd, B.; Truscott, J.G. Percentage fat in overweight and obese children: Comparison of DXA and air displacement plethysmography. Obes. Res. 2005, 13, 75–85. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gutiérrez-Marín, D.; Luque, V.; Ferré, N.; Fewtrell, M.S.; Williams, J.E.; Wells, J.C.K. Associations of age and body mass index with hydration and density of fat-free mass from 4 to 22 years. Eur. J. Clin. Nutr. 2019, 73, 1422–1430. [Google Scholar] [CrossRef] [PubMed]
- Bazzocchi, A.; Ponti, F.; Albisinni, U.; Battista, G.; Guglielmi, G. DXA: Technical aspects and application. Eur. J. Radiol. 2016, 85, 1481–1492. [Google Scholar] [CrossRef] [PubMed]
- Orsso, C.E.; Silva, M.I.B.; Gonzalez, M.C.; Rubin, D.A.; Heymsfield, S.B.; Prado, C.M.; Haqq, A.M. Assessment of body composition in pediatric overweight and obesity: A systematic review of the reliability and validity of common techniques. Obes. Rev. 2020, 21, e13041. [Google Scholar] [CrossRef]
- Testolin, C.G.; Gore, R.; Rivkin, T.; Horlick, M.; Arbo, J.; Wang, Z.; Chiumello, G.; Heymsfield, S.B. Dual-energy X-ray absorptiometry: Analysis of pediatric fat estimate errors due to tissue hydration effects. J. Appl. Physiol. [1985] 2000, 89, 2365–2372. [Google Scholar] [CrossRef]
- Laskey, M.A. Dual-energy X-ray absorptiometry and body composition. Nutrition 1996, 12, 45–51. [Google Scholar] [CrossRef]
- Bergmann, R.L.; Bergmann, K.E.; Richter, R.; Schlaud, M.; Henrich, W.; Weichert, A. Growth attainment in German children born preterm, and cardiovascular risk factors in adolescence. Analysis of the population representative KiGGS data. J. Perinat. Med. 2017, 45, 619–626. [Google Scholar] [CrossRef] [PubMed]
- Engan, M.; Vollsaeter, M.; Oymar, K.; Markestad, T.; Eide, G.E.; Halvorsen, T.; Juliusson, P.; Clemm, H. Comparison of physical activity and body composition in a cohort of children born extremely preterm or with extremely low birth weight to matched term-born controls: A follow-up study. BMJ Paediatr. Open 2019, 3, e000481. [Google Scholar] [CrossRef]
- Lee, J.; Park, H.K.; Kim, J.H.; Choi, Y.Y.; Lee, H.J. Bone Mineral Density According to Dual Energy X-ray Absorptiometry is Associated with Serial Serum Alkaline Phosphatase Level in Extremely Low Birth Weight Infants at Discharge. Pediatr. Neonatol. 2017, 58, 251–257. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Figueras-Aloy, J.; Alvarez-Dominguez, E.; Perez-Fernandez, J.M.; Moretones-Sunol, G.; Vidal-Sicart, S.; Botet-Mussons, F. Metabolic bone disease and bone mineral density in very preterm infants. J. Pediatr. 2014, 164, 499–504. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Simpson, S.J.; Turkovic, L.; Wilson, A.C.; Verheggen, M.; Logie, K.M.; Pillow, J.J.; Hall, G.L. Lung function trajectories throughout childhood in survivors of very preterm birth: A longitudinal cohort study. Lancet Child Adolesc. Health 2018, 2, 350–359. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Full-Term | Very Preterm | p-Value | |||
|---|---|---|---|---|---|
| Boys | Girls | Boys | Girls | ||
| Birth | N = 79 | N = 75 | N = 39 | N = 28 | |
| Gestational age (weeks) | 39.47 (1.29) | 39.77 (1.24) | 27.50 (1.55) | 27.44 (1.55) | <0.001 |
| Birth weight SDS | 0.39 (1.00) | 0.19 (1.09) | 0.27 (0.68) | 0.05 (0.76) | 0.416 |
| BPD (%) | NA | NA | 12 (30.8%) | 5 (17.9%) | |
| Ethnicity (%) | <0.020 | ||||
| White | 54 (68.4%) | 45 (60.0%) | 30 (76.9%) | 23 (82.1%) | |
| Non-white | 25 (31.6%) | 30 (40.0%) | 9 (23.1%) | 5 (17.9%) | |
| All visits, total group | |||||
| Weight-for-height SDS | 0.07 (1.11) | 0.40 (0.91) | −0.55 (1.10) | −0.51 (1.13) | <0.001 |
| Height SDS | −0.26 (0.79) | −0.20 (1.02) | −0.87 (0.76) | −0.70 (1.11) | <0.001 |
| Age 3 years | N = 18 | N = 24 | N = 13 | N = 10 | |
| Age (years) | 3.06 (0.11) | 3.08 (0.10) | 3.44 (0.15) | 3.46 (0.18) | <0.001 |
| Weight-for-height SDS | 0.31 (1.08) | 0.51 (1.02) | −0.43 (0.94) | −0.47 (0.95) | 0.001 |
| Height SDS | −0.13 (0.72) | 0.09 (0.93) | −0.69 (0.65) | −0.58 (1.34) | 0.008 |
| Age 4 years | N = 33 | N = 24 | |||
| Age (years) | 4.11 (0.13) | 4.15 (0.15) | NA | NA | |
| Weight-for-height SDS | −0.13 (1.21) | 0.45 (0.83) | NA | NA | |
| Height SDS | −0.32 (0.89) | 0.02 (1.08) | NA | NA | |
| Age 5 years | N = 46 | N = 41 | N = 26 | N = 18 | |
| Age (years) | 5.11 (0.14) | 5.08 (0.13) | 5.97 (0.17) | 5.94 (0.12) | <0.001 |
| Weight-for-height SDS | 0.13 (1.05) | 0.31 (0.14) | −0.61 (1.18) | −0.53 (1.25) | <0.001 |
| Height SDS | −0.27 (0.75) | −0.51 (0.98) | −0.96 (0.80) | −0.77 (1.00) | 0.002 |
| Full-Term N = 186 | Very Preterm N = 67 | p-Value | |
|---|---|---|---|
| FM (kg) | |||
| DXA | 5.16 (1.26) | 4.43 (1.26) | <0.001 |
| ADP default | 4.09 (1.45) | 2.54 (1.35) | <0.001 |
| ADP revised | 4.47 (1.40) | 2.98 (1.73) | <0.001 |
| Mean difference (LoA) ADP default–DXA | −1.08 * (−2.92; 0.76) | −1.89 * (−4.10; 0.32) | <0.001 |
| Mean difference (LoA) ADP revised–DXA | −0.67 * (−2.38; 1.04) | −1.45 * (−3.53; 0.63) | <0.001 |
| FM% | |||
| DXA | 28.26 (4.88) | 24.39 (4.76) | <0.001 |
| ADP default | 22.47 (6.91) | 14.60 (7.88) | <0.001 |
| ADP revised | 24.90 (6.64) | 17.07 (7.93) | <0.001 |
| Mean difference (LoA) ADP default–DXA | −5.78 * (−16.25; 4.69) | −9.79 * (−20.92; 1.34) | <0.001 |
| Mean difference (LoA) ADP revised–DXA | −3.54 * (−13.44; 6.36) | −7.32 * (−18.26; 3.62) | <0.001 |
| FFM (kg) | |||
| DXA | 13.06 (2.01) | 13.72 (2.59) | 0.064 |
| ADP default | 13.96 (2.25) | 15.36 (3.36) | 0.002 |
| ADP revised | 13.41 (2.13) | 14.91 (3.28) | 0.001 |
| Mean difference (LoA) ADP default–DXA | 0.90 * (−1.00; 2.80) | 1.64 * (−0.63; 3.91) | <0.001 |
| Mean difference (LoA) ADP revised–DXA | 0.50 * (−1.30; 2.30) | 1.20 * (−0.92; 3.32) | <0.001 |
| Age (years) | Boys | Girls | ||||
|---|---|---|---|---|---|---|
| C1 | C2 | Dffm | C1 | C2 | Dffm | |
| 2.75 | 5.432 | 5.031 | 1.0797 | 5.449 | 5.050 | 1.0790 |
| 3 | 5.424 | 5.022 | 1.0801 | 5.426 | 5.025 | 1.0800 |
| 3.25 | 5.416 | 5.013 | 1.0804 | 5.405 | 5.001 | 1.0808 |
| 3.5 | 5.409 | 5.005 | 1.0807 | 5.393 | 4.987 | 1.0813 |
| 3.75 | 5.402 | 4.998 | 1.0809 | 5.386 | 4.980 | 1.0816 |
| 4 | 5.395 | 4.990 | 1.0812 | 5.384 | 4.978 | 1.0816 |
| 4.25 | 5.390 | 4.984 | 1.0814 | 5.384 | 4.978 | 1.0816 |
| 4.5 | 5.386 | 4.980 | 1.0816 | 5.384 | 4.978 | 1.0816 |
| 4.75 | 5.384 | 4.978 | 1.0817 | 5.384 | 4.978 | 1.0816 |
| 5 | 5.384 | 4.977 | 1.0817 | 5.384 | 4.978 | 1.0816 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
van Beijsterveldt, I.A.L.P.; Beunders, V.A.A.; Bijlsma, A.; Vermeulen, M.J.; Joosten, K.F.M.; Hokken-Koelega, A.C.S. Body Composition Assessment by Air-Displacement Plethysmography Compared to Dual-Energy X-ray Absorptiometry in Full-Term and Preterm Aged Three to Five Years. J. Clin. Med. 2022, 11, 1604. https://doi.org/10.3390/jcm11061604
van Beijsterveldt IALP, Beunders VAA, Bijlsma A, Vermeulen MJ, Joosten KFM, Hokken-Koelega ACS. Body Composition Assessment by Air-Displacement Plethysmography Compared to Dual-Energy X-ray Absorptiometry in Full-Term and Preterm Aged Three to Five Years. Journal of Clinical Medicine. 2022; 11(6):1604. https://doi.org/10.3390/jcm11061604
Chicago/Turabian Stylevan Beijsterveldt, Inge A. L. P., Victoria A. A. Beunders, Alja Bijlsma, Marijn J. Vermeulen, Koen F. M. Joosten, and Anita C. S. Hokken-Koelega. 2022. "Body Composition Assessment by Air-Displacement Plethysmography Compared to Dual-Energy X-ray Absorptiometry in Full-Term and Preterm Aged Three to Five Years" Journal of Clinical Medicine 11, no. 6: 1604. https://doi.org/10.3390/jcm11061604