4. Discussion
Ischemia reperfusion injury (IRI) and subsequent early graft dysfunction play a central role for early as well as long-term outcome and graft function, not only in pancreas transplantation [
1,
2]. Well-considered monitoring of specific serological biomarkers could be a helpful tool for early detection and diagnosis, treatment choice and induction as well as outcome prediction after transplantation with the final goal of predicting the individual’s risk of allograft injury and ischemic damage, resulting in individualized treatment approaches and outcome improvement after solid organ transplantation [
30,
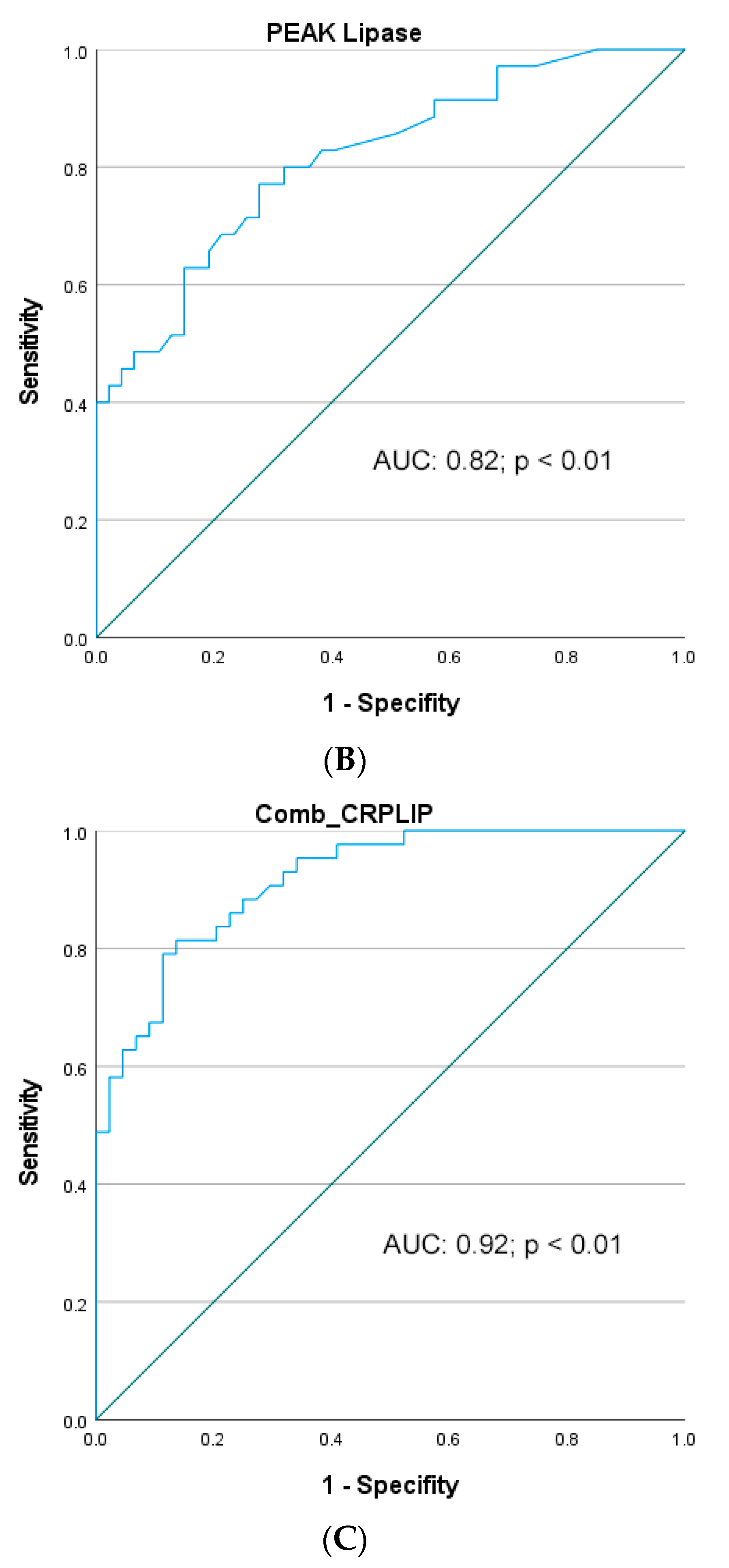
31]. Our study provides a comprehensive summary of the predictive values of a panel of widely used global serum biomarkers for the detection of early graft dysfunction for both the pancreas and the kidney graft, respectively, in patients after simultaneous pancreas–kidney transplantation (SPKT). Hereby, peak serum lipase and peak serum CRP as well as their combination showed the most consistent results with good and excellent predictive values (AUCs > 0.8 und > 0.9, respectively), demonstrating a high predictive accuracy in the prediction of ePGD of all analyzed biomarkers in our current study. In contrast, with regard to the prediction of early renal graft dysfunction, the predictive value and diagnostic accuracy of all analyzed serological markers had lower sensitivity and were only assessed as fair to moderate (all AUC < 0.8). According to the findings of our study, the assessment of specific laboratory biomarkers combined with other pre-, intra- and postoperative donor- and recipient-related clinical factors (e.g., donor age and BMI, CIT of the pancreas) may present helpful insights, in order to identify patients at a high risk of ePGD and to predict long-term graft function and outcome, especially of the pancreas graft.
Despite constant improvement in the field of SPKT, the pancreas graft especially remains highly prone to IRI and early graft dysfunction, which leads to early graft damage and consecutively severe patient morbidity and mortality. Due to the high susceptibility of the pancreas graft, unavoidable procedural and surgical steps during the process of transplantation may lead to considerable damage of the graft and impaired outcome [
1,
31,
32].
In this context, the pancreatic allograft is particularly susceptible to injuries in the early reperfusion period with damaging effects on the grafts’ microvasculature resulting in early and severe post-transplant pancreatitis as well as the formation of thromboses in the pancreas vein, in some cases within a few hours after transplantation [
14,
15,
33]. These complications not only significantly impair graft function and survival but are additionally associated with severe surgical complications such as enteric leakage of the anastomosis, profound hemorrhage due to disintegration of vascular anastomosis and profound pancreatitis with fatal outcome for the affected patient [
19,
34].
Monitoring of serum biomarkers, repeated imaging studies and implementation of clinical scoring systems are widely used for the assessment of mortality and severity of acute pancreatitis in the non-transplant setting [
14,
16,
35,
36,
37,
38]. However, little is known about the usefulness and value of different serum biomarkers for the prediction of specific pancreas graft-related outcomes and early graft dysfunction (mainly ischemia reperfusion injury) after clinical SPKT. In this context, the majority of the implemented scores for non-transplant pancreatitis are impractical for immediate use after transplantation due to various reasons, including but not limited to, a natural increase in used serum biomarkers such as serum lipase and amylase concentrations after transplantation, not necessarily associated with disease severity. Therefore, current research focusses on the detection and verification of new rapid-onset serum biomarkers to predict early pancreatic graft dysfunction as well as ischemia reperfusion injury and following complications after SPKT accurately and promptly, in order to assess the severity of post-transplant pancreatitis as soon as possible, which again may be important for prudent and yet speedy clinical decision making in choice and induction of treatment.
In the past, serum CRP and interleukin levels have been well evaluated for the assessment of the severity and prognosis of acute pancreatitis in “non-transplant” patients [
14,
16,
38]. Recently, a meta-analysis carried out by van den Berg and colleagues showed a superiority of serum IL- 6 within the first 72 h for the early prediction of severity of acute pancreatitis, followed by increased serum CRP levels with adequate predictive values [
14]. Another systematic review and meta-analysis could show that serum CRP levels on POD 4 were highly effective (AUC of 0.86, sensitivity and specificity of 86% and 69%, respectively) in predicting pancreas-related complications following pancreas surgery [
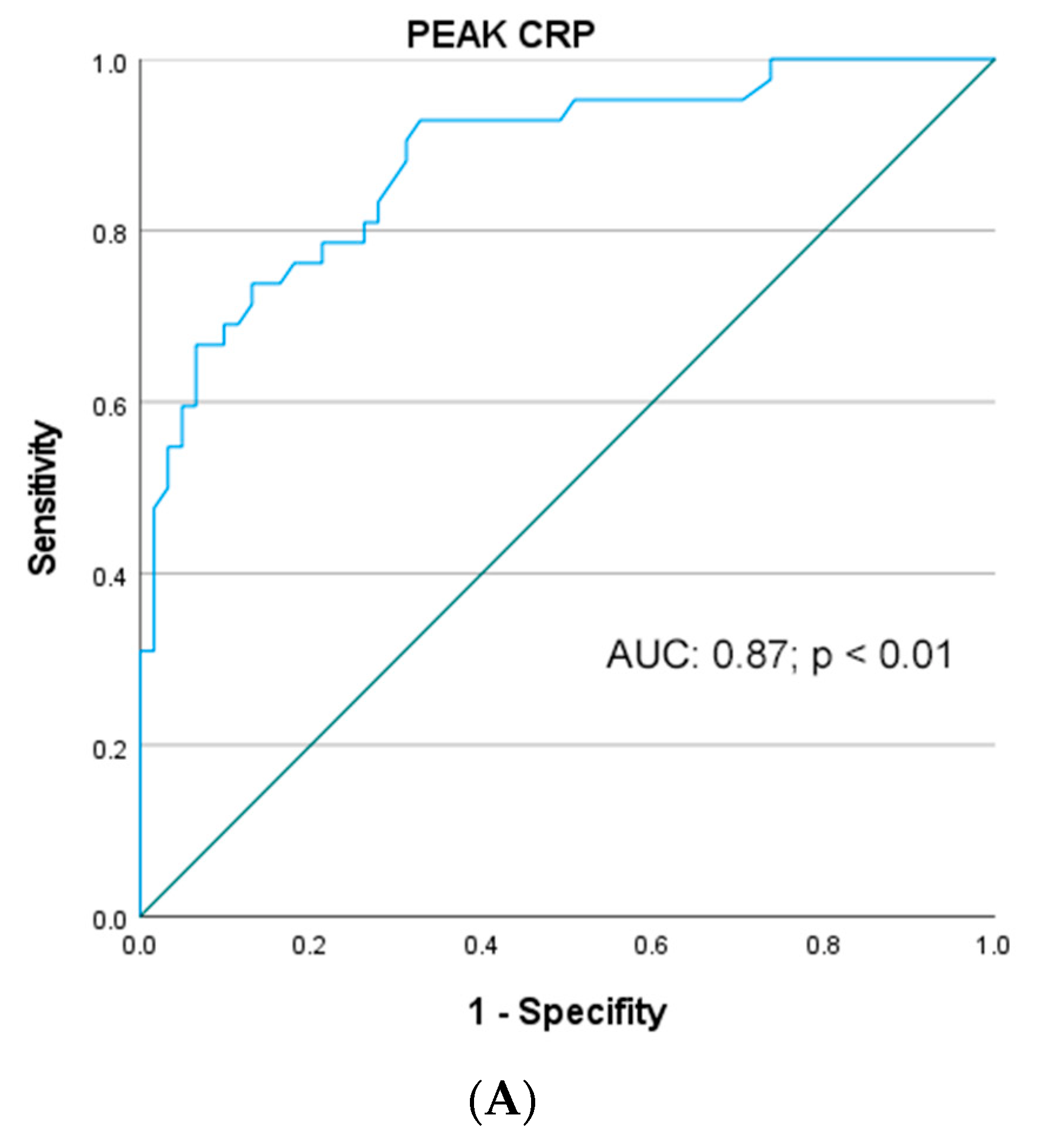
39]. Intriguingly, our current study of patients after SPKT could reveal that serum CRP levels—especially peak serum CRP levels during the first 3 days after transplantation—are a robust predictive marker with good AUCs > 0.8 for predicting the degree and severity of ePGD. Our findings are consistent with a previous publication, which could demonstrate that peak serum CRP levels correlate well with ePGD and IRI and the consecutive impairment of microcirculation in the early reperfusion period after SPKT, and that an elevation of serum CRP in the early phase after transplantation is associated with increased pancreas graft-associated complications [
3]. However, one may argue that the exclusive monitoring of serum CRP levels after SPKT may not be sufficiently organ-specific in monitoring for ePGD and IRI complications due to the rather unspecific nature of serum CRP, which is also increased in the case of any other reason of inflammation, systemical infection and/or renal graft injury after transplantation. Nonetheless, systemical infections, such as pneumonia, blood stream or wound infections, are not very common in the early phase (POD 1–3) after solid organ transplantation and mostly become relevant on POD 4 and later in the case of a prolonged ICU stay. In contrast, ePGD and other pancreatic IRI-associated complications, such as post-transplantation pancreatitis usually develop during the first few days after SPKT, being accountable for early increases in serum CRP levels [
34,
35]. Therefore, according to the expected time frame of serum CRP rise and in the absence of other clinical signs of early post-transplant infection, elevated CRP levels within the first 72 h after SPKT represent a fairly specific marker for pancreatic tissue injury due to ePGD- and IRI-related complications. Of interest, the results of our ROC analysis concerning CRP course and peak of CRP were less sensitive (all AUC < 0.8) for the prediction of eRGD following SPKT.
Transient elevation of serum pancreatic enzymes in the early postoperative period after SPKT is more common and generally caused by IRI and ePGD, which could reflect the degree of graft-related complications including pancreatitis [
36,
40,
41]. In the non-transplant setting, most previous studies could demonstrate that elevated serum pancreatic enzymes (particularly on POD 1 and 3) as well increased drain fluid pancreatic amylase activity (on POD 1 and 2) are highly predictive parameters for pancreas-related complications following pancreatic surgery [
42,
43,
44,
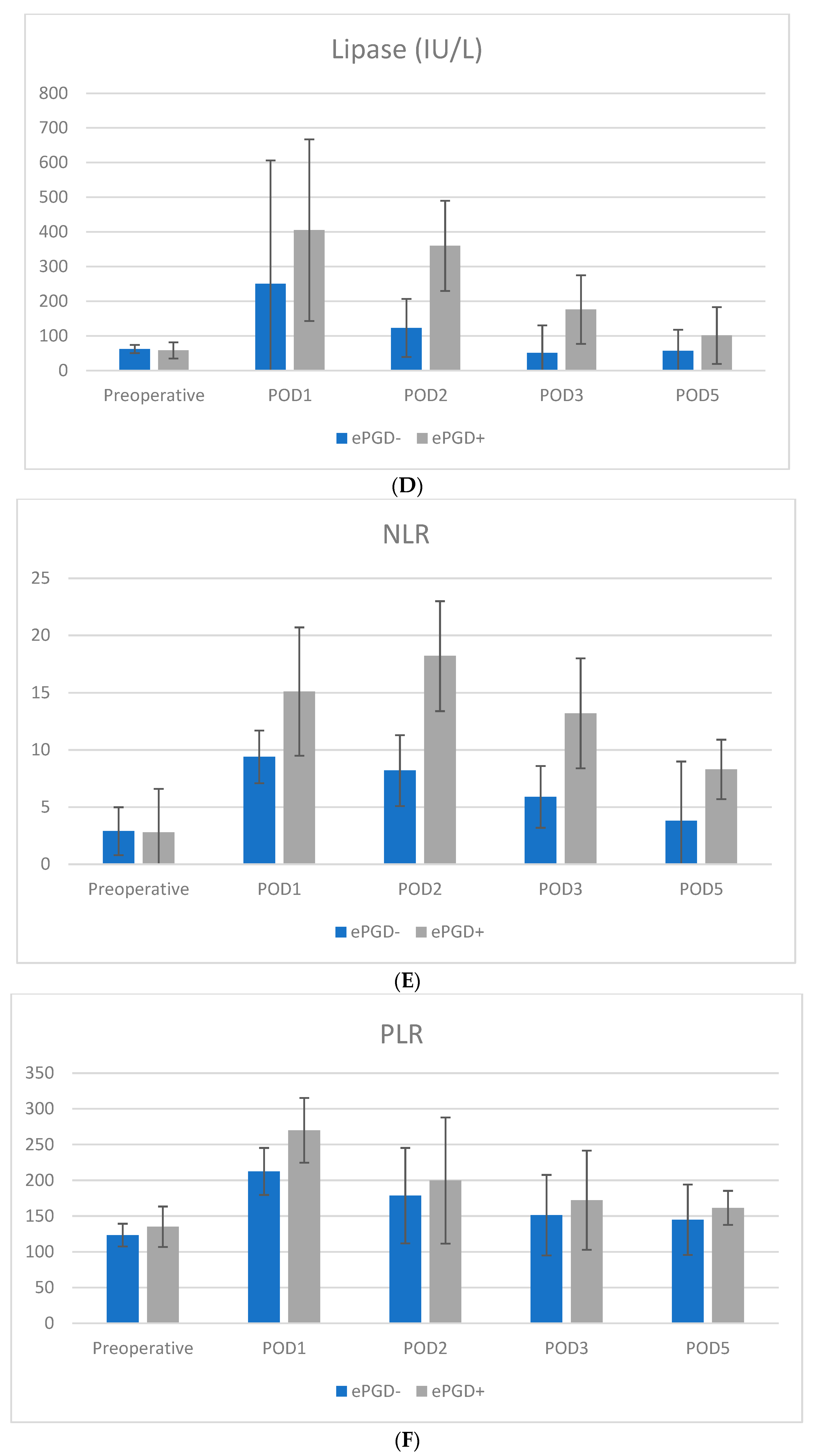
45]. Consistently, the results of our current study show that a serum lipase value of >150 IU/L on POD 2 is an independent prognostic parameter in multivariate logistic regression analysis for ePGD following SPKT. Interestingly, the peak of serum lipase values with a cut-off value >168 IU/L shows excellent predictive correlations (>0.8 AUC) for ePGD and pancreatic graft-related complications after SPKT. On the other hand, the serum lipase values on POD 1 and 2 only had acceptable predictive accuracy (<0.8 AUC) for predicting ePGD.
Based on these former findings and particularly with regard to the results of our ROC analyses, we believe that the combination of monitoring peak serum CRP and serum lipase levels during the first three to five days after SPKT may be very useful for the monitoring of ePGD-associated complications as well as in the prediction of early graft function and long-term outcome in SPKT recipients.
In contrast, the ability of WBC as well as PLR and NLR to predict ePGD and pancreas graft-associated complications as well as early renal graft dysfunction in our patient cohort was assessed as fair. Our current findings are consistent with previous studies in the non-transplant setting, showing weak or acceptable predictive values of PLR and/or NLR for prediction of postoperative pancreas-related complications following pancreatic surgery as well as a reduced ability for the prediction of the severity of the disease in acute pancreatitis [
9,
14,
16,
37,
43,
46]. However, after liver and kidney transplantation alone, preoperative NLR and PLR levels as well as their distinct postoperative course could be identified as independent predictors of early graft dysfunction and decreased graft survival in the long-term follow up [
47,
48,
49,
50].
In question of our results concerning serum PCT values, this marker is widely reported as a useful biomarker to differentiate sepsis- and non-sepsis-related inflammatory response and to predict severe bacterial infection as well as to guide discontinuation of antibiotic treatment. The role of PCT and its ability to predict disease severity as well as reliable prognosis in acute pancreatitis in the non-transplant setting, is a matter of dispute [
38]. So far, previous studies showed a low predictive accuracy for the severity of disease, prognostic stratification as well as (pancreas related) complications following pancreatic surgery in the setting of acute pancreatitis [
9,
14,
16,
37,
38,
39]. These previous findings are in accordance with our current results in patients after SPKT, only showing a weak correlation and a low predictive accuracy of serum PCT levels in predicting ePGD- and pancreas-related complications after SPKT. Therefore, our data do not support serum PCT as useful in postoperative monitoring of ePGD-associated complications; however, we highly recommend the monitoring of this marker for the early detection of postoperative bacteria-derived infectious complications after SPKT.
Current literature provides only sparce evidence for organ-specific biomarkers for the discrimination between IRI and early graft dysfunction of the pancreas and kidney graft, respectively. Due to the unique characteristic of SPKT, two organs of a very different kind and nature are transplanted simultaneously, of which the pancreas graft is by far the most susceptible for postoperative early graft dysfunction and failure. The kidney graft on the other hand is in comparison much more robust and much less susceptive to ischemia reperfusion injury and postoperative graft failure compared to the delicate pancreas graft. Concerning SPKT and pancreas transplantation alone, only two studies exist which examined this question in detail [
51,
52]. Glazunova et al., focused on kidney specific serum markers (such as Cystatin C, NGAL, podocin and OPN) after SPKT, which, however, were not found to be specific for IRI, but only for unspecific acute kidney injury [
51]. Fernstad et al., could show that pancreatic-specific protein (PASP) is a good marker for early pancreatic graft dysfunction and IRI-associated pancreatitis following SPKT [
52]. In a recent review by Prudhomme et al., the findings of preclinical studies with regard to machine perfusion showed promising approaches for the evaluation of pancreas-specific markers in the sense of metabolic assessment of perfusate solutions (Insulin, ATP, LDH, multiple metabolomics) or cell death activity (e.g., caspase, cell-free DNA) during pancreas preservation, which might be implemented for clinical use after successful evaluation in prospective clinical studies in the [
1]. Newer approaches, such as the evaluation of non-invasive liquid biopsy and liquid biopsy-based biomarkers, e.g., different protein-panels and extracellular vesicles (EVs), miRNA and cell-free DNA, have shown promising results concerning diagnostic insight in various disorders, not only in malignancies and autoimmune diseases, but also in the evaluation of graft dysfunction after solid organ transplantation as well [
53,
54,
55]. Since the introduction of multi-omics techniques, which are shedding light on discrete genomic, transcriptomic, proteomic and metabolomic signatures, new biomarkers have been the focus of interest in the prediction of allograft outcomes [
56]. In this proactive approach, the focus lies on the prediction and prevention of pathological processes by providing earlier and more extensive information than traditional ones [
54,
57]. In the case of kidney transplantation alone, some metabolic- and protein-associated markers (namely KIM-1, Cystatin C, NAG, NAGL, chemokine (CXCL 9 and 10) or L-FAB) have recently been identified in some clinical studies as potential and “organ-specific” markers for monitoring graft function and detecting early graft dysfunction and IRI-associated complications and outcome after KTA [
54]. Furthermore, few current convincing studies identified cell-free DNA (circulating/donor-derived) as well as EVs, specifically kidney-specific parameters (aquaporin, CD133, clusterin, PODXL, SYT17 as well as multiple mRNA signatures), as promising markers for early graft dysfunction in several clinical KTA settings [
54,
55]. Notably, in the field of genomic and transcriptomic profiling, the assessment of DNA methylation seems to become a potential new and sensitive clinical biomarker in the detection of early graft dysfunction during KTA and consecutively targeting therapy for the future [
58]. However, further research is needed to evaluate the significance of these new approaches for early graft dysfunction in SPKT, with the pancreas-specific lipase and alterations of CRP being by far the most specific IRI and graft dysfunction markers for the pancreas graft yet.
Apart from the diagnostical pathway for the detection of early graft dysfunction and IRI-associated complications, for instance by the screening and monitoring of serological biomarkers in combination with clinical risk-factor-dependent prediction scoring systems, therapeutical approaches are the key pathways for reducing IRI-associated damages with encouraging early and long-term success following solid organ transplantation [
2]. In this context, conditioning is a broad term generally used to describe strategies to attenuate IRI and early graft dysfunction by inducing biochemical changes within the recipient and transplant allograft. Depending on timing and application, it can be referred to as pre-, peri- and post-conditioning [
32,
59]. Herein, ischemic preconditioning and remote ischemic preconditioning have previously been shown to induce beneficial effects in solid organ transplantation including SPKT [
60]. Insights into the molecular pathophysiology of IRI and subsequent early graft dysfunction have opened the door to new therapeutic targets and novel interventions, such as succinate removal, ferroptosis inhibitors, regulation of complement cascade and manipulation of regulatory cells, such as myeloid-derived suppressor cells (MDSC) and hematopoietic stem cells (HSC), which may play an important role in reducing early graft dysfunction after transplantation [
2]. As long-term preservation technologies of the graft, such as machine perfusion, become more and more accessible, the possibility of pharmacological organ conditioning as well as recipient conditioning (e.g., anesthetic conditioning, pharmacological (such as α-Lipoic Acid substitution) and manipulation with novel strategies such as RNA interferences, become more attractive [
1,
2,
8,
11,
61]. In this regard, differential regulation of early graft dysfunction and IRI-related miRNAs may lead to improved graft function and survival as well as an expansion of the donor organ pool [
2].
Although our current study shows promising results, several limitations are important to discuss.
Firstly, the low number of patients in each group and the retrospective, non-randomized design of our current study must be considered, before extrapolating our results to common clinical practice. Therefore, as a future study approach, a detailed multiple logistic regression analysis within a larger cohort should be investigated.
Secondly, although this study represents the results of a big German pancreas transplant center with equivalent surgical procedure and compact and robust follow-up data, the long investigation period as well as different anesthesiologic and operative teams and styles may have had an impact on diagnostical and therapeutical decision.
Thirdly, although in our analysis a variety of the most commonly used global serologic markers of inflammation (CRP, WBC, PCT, NLR, PLR) were evaluated, these—except perhaps for pancreatic-specific lipase—cannot distinguish by laboratory chemistry alone between the source of IRI, hence between pancreas- and kidney-specific injury. Therefore, future large prospective multi-center studies are needed to introduce new and reliable sets of graft-specific serological markers (e.g., miRNAs, cell-free DNA, EVs, etc.), which may identify which organ is affected by IRI and to assess internal/external validity and reliability of the presented data.


 ,
, 




{kind=link}
{kind=link}
{kind=link}
{kind=link}