
Robot-Assisted Tubal Reanastomosis after Sterilization: A Choice for Family Planning

 ,
,  , ,
, ,
Abstract
:1. Introduction
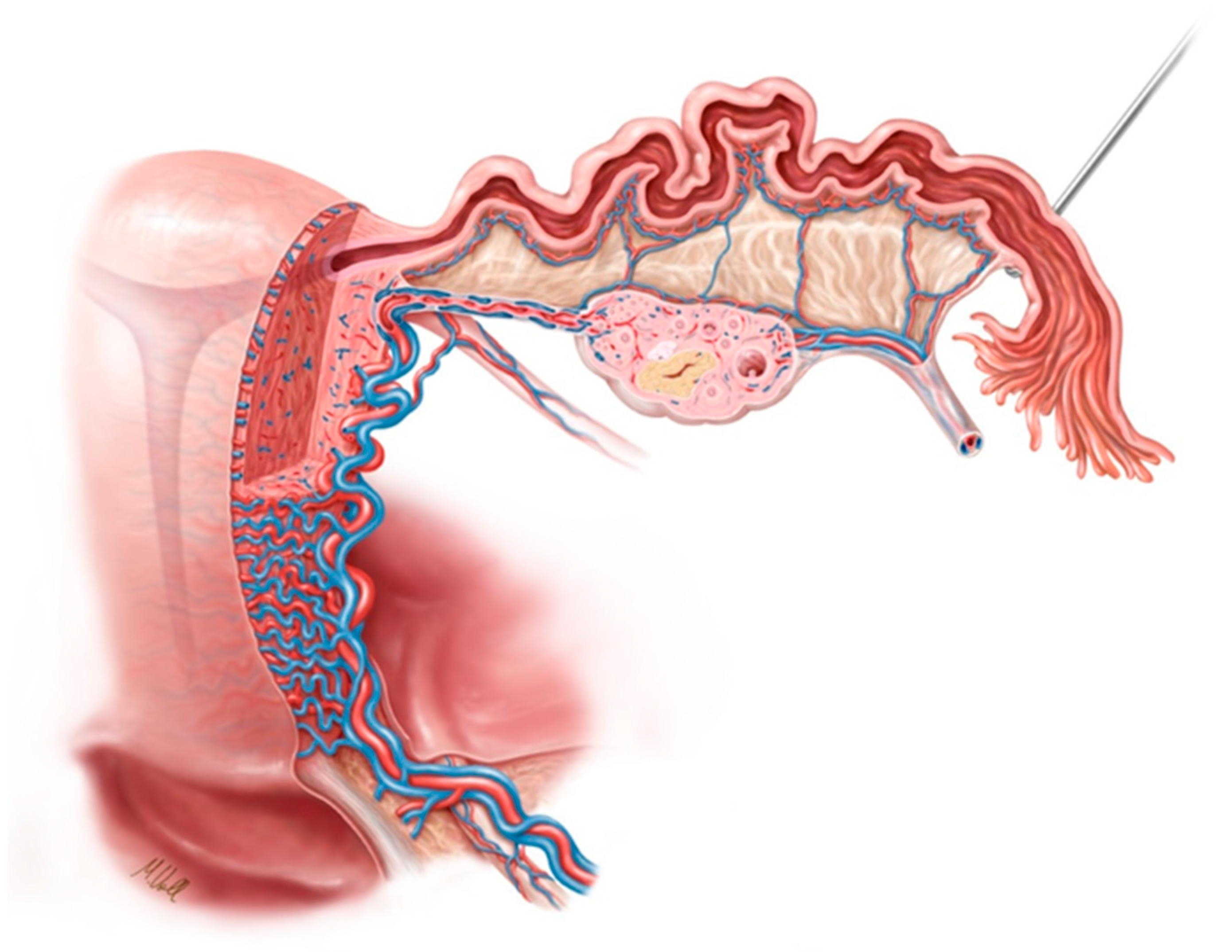
2. Anatomy of the Fallopian Tube
3. Blood Supply and Lymphatics
4. Nerves
5. Muscles
6. Family Planning
7. Reasons for Performing Sterilization
8. Index of Sterilization
9. Types of Sterilization
10. Methods of Sterilization
11. Post-Sterilization Regret and Symptoms of Depression
12. Sterilization Reversal versus IVF
13. Prognostic Factors for Reversal of Sterilization
14. Description of the Procedure
14.1. Docking and Instrumentation
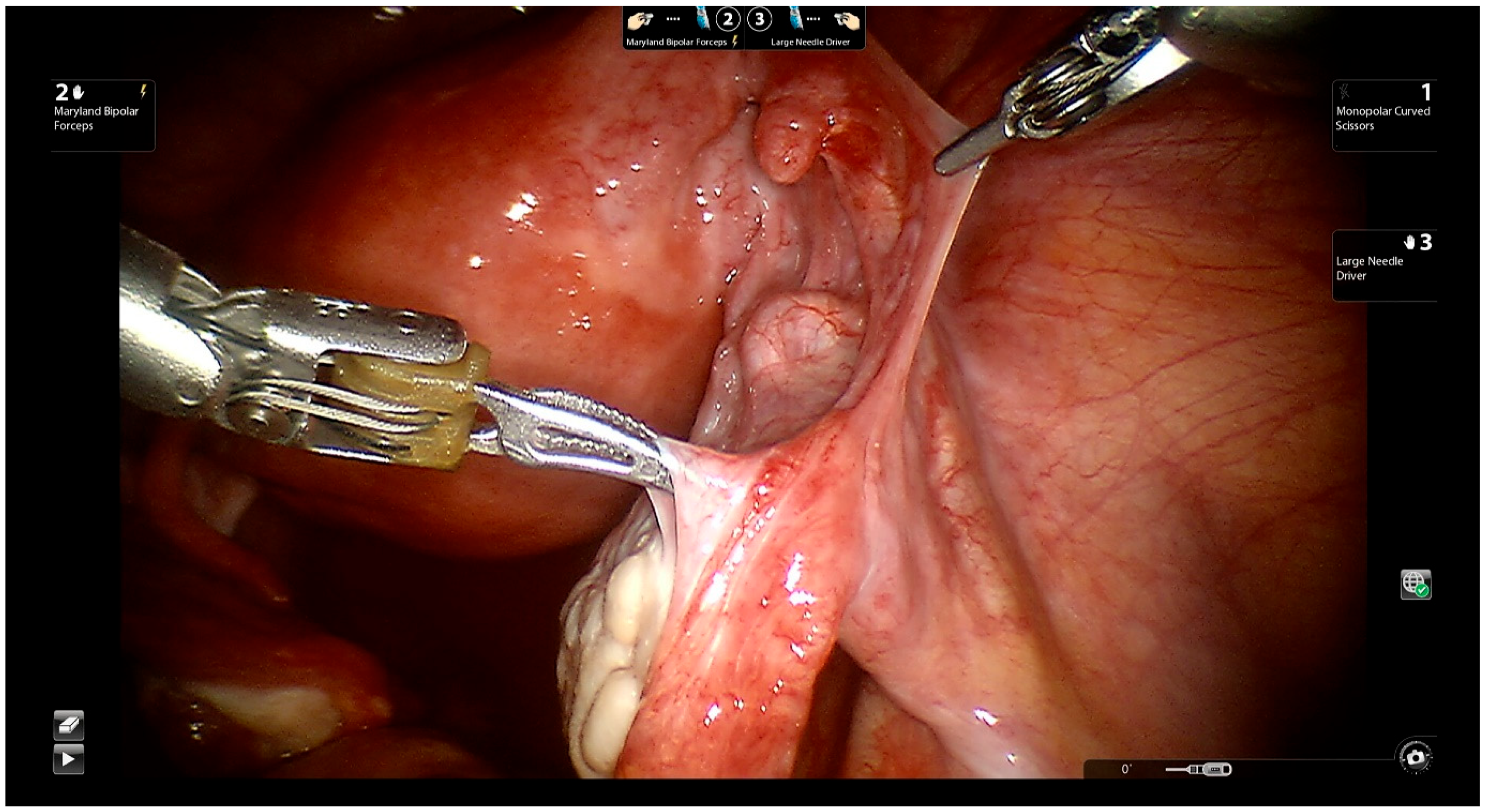
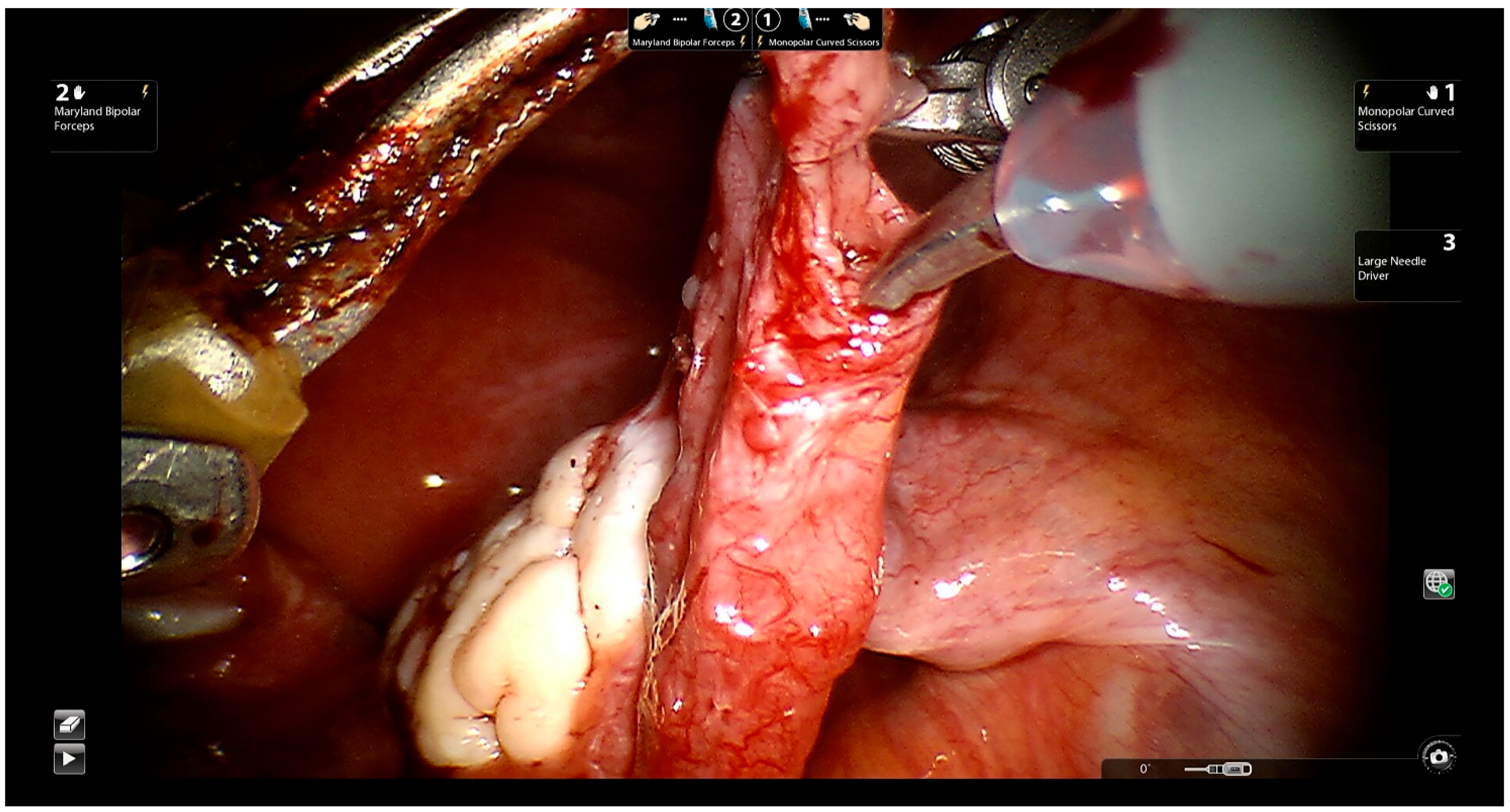
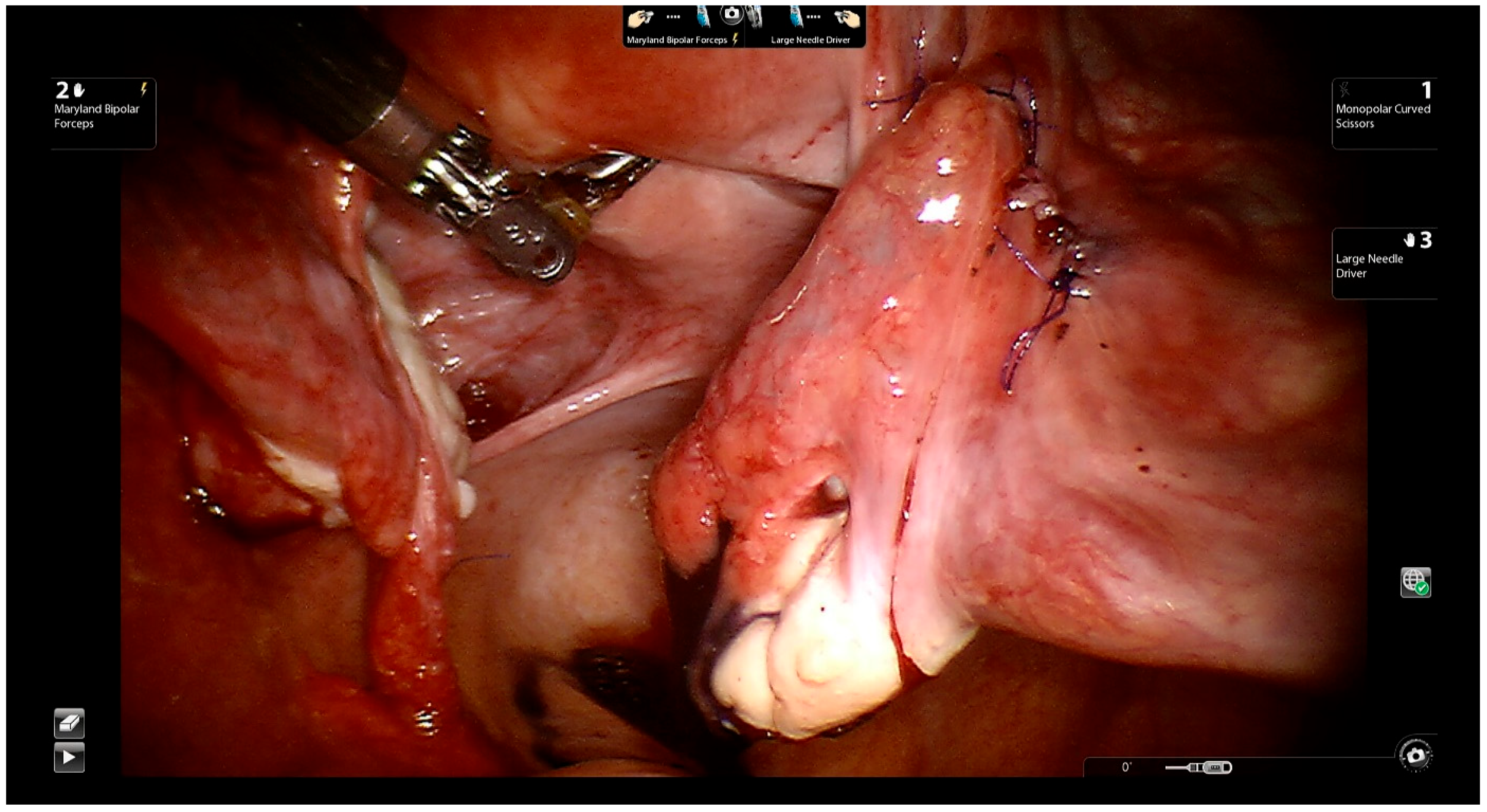
14.2. Surgical Technique
15. Robot-Assisted Tubal Anastomosis with the One-Stitch Technique
16. Comparing Robot-Assisted Laparoscopic Surgery versus Conventional Laparoscopic Surgery
17. Pregnancy Rates in the First 12 Months after Tubal Anastomoses
18. Future Perspectives, Tubal Grafting
19. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Van Seeters, J.A.; Chua, S.J.; Mol, B.W.J.; Koks, C.A. Tubal anastomosis after previous sterilization: A systematic review. Hum. Reprod. Update 2017, 23, 358–370. [Google Scholar] [CrossRef] [PubMed]
- Hillis, S.D.; Marchbanks, P.A.; Tylor, L.R.; Peterson, H.B. Poststerilization regret: Findings from the United States Collaborative Review of Sterilization. Obstet. Gynecol. 1999, 93, 889–895. [Google Scholar] [CrossRef] [PubMed]
- Alkatout, I. Communicative and ethical aspects of physician-patient relationship in extreme situations. Wien. Med. Wochenschr. 2015, 165, 491–498. [Google Scholar] [CrossRef] [PubMed]
- Williams, G.F. Fallopian tube surgery for reversal of sterilization. Br. Med. J. 1973, 1, 599–601. [Google Scholar] [PubMed] [Green Version]
- Siegler, A.M.; Perez, R.J. Reconstruction of fallopian tubes in previously sterilized patients. Fertil. Steril. 1975, 26, 383–392. [Google Scholar] [CrossRef]
- Bedaiwy, M.A.; Barakat, E.M.; Falcone, T. Robotic tubal anastomosis: Technical aspects. JSLS J. Soc. Laparoendosc. Surg. 2011, 15, 10. [Google Scholar] [CrossRef] [Green Version]
- Alkatout, I. Complications of laparoscopy in connection with entry techniques. J. Gynecol. Surg. 2017, 33, 81–91. [Google Scholar]
- Alkatout, I.; Mettler, L.; Maass, N.; Noé, G.-K.; Elessawy, M. Abdominal anatomy in the context of port placement and trocars. J. Turk. Ger. Gynecol. Assoc. 2015, 16, 241. [Google Scholar]
- Han, J.; Sadiq, N.M. Anatomy, Abdomen and Pelvis, Fallopian Tube; StatPearls Publishing: Treasure Island, FL, USA, 2019. [Google Scholar]
- Cahill, E.P.; Kaur, S. Advances in contraception research and development. Curr. Opin. Obstet. Gynecol. 2020, 32, 393–398. [Google Scholar] [CrossRef]
- Bahamondes, L.; Fernandes, A.; Monteiro, I.; Bahamondes, M.V. Long-acting reversible contraceptive (LARCs) methods. Best Pract. Res. Clin. Obstet. Gynaecol. 2020, 66, 28–40. [Google Scholar]
- Wolman, I. Berek and Novak’s Gynecology 15th Edition. J. Obstet. Gynaecol. India 2014, 64, 150–151. [Google Scholar] [CrossRef] [Green Version]
- Cates, W., Jr.; Stone, K.M. Family planning, sexually transmitted diseases and contraceptive choice: A literature update—Part I. Fam. Plan. Perspect. 1992, 24, 75–84. [Google Scholar] [CrossRef]
- Mosher, W.D.; Jones, J. Use of contraception in the United States: 1982–2008. Vital Health Stat. Ser. 23 Data Natl. Surv. Fam. Growth 2010, 29, 1–44. [Google Scholar]
- Burkman, R.T. Berek & Novak’s gynecology. JAMA 2012, 308, 516–517. [Google Scholar]
- Hatcher, R.A.; Stewart, F.; Trussell, J.; Kowal, D.; Guest, F.; Stewart, G.K.; Kowal, D. Contraceptive Technology 1990–1992; Irvington Publishers, Inc.: New York, NY, USA, 1990. [Google Scholar]
- Sedgh, G.; Singh, S.; Hussain, R. Intended and unintended pregnancies worldwide in 2012 and recent trends. Stud. Fam. Plan. 2014, 45, 301–314. [Google Scholar] [CrossRef] [Green Version]
- Shreffler, K.M.; Greil, A.L.; McQuillan, J.; Gallus, K.L. Reasons for tubal sterilisation, regret and depressive symptoms. J. Reprod. Infant Psychol. 2016, 34, 304–313. [Google Scholar] [CrossRef] [Green Version]
- Uchida, H. Uchida tubal sterilization. Am. J. Obstet. Gynecol. 1975, 121, 153–158. [Google Scholar] [CrossRef]
- Filshie, G.; Casey, D.; Pogmore, J.; Dutton, A.; Symonds, E.; Peake, A. The titanium/silicone rubber clip for female sterilization. BJOG Int. J. Obstet. Gynaecol. 1981, 88, 655–662. [Google Scholar] [CrossRef]
- Penfield, A.J. The Filshie clip for female sterilization: A review of world experience. Am. J. Obstet. Gynecol. 2000, 182, 485–489. [Google Scholar] [CrossRef]
- Borrero, S.B.; Reeves, M.; Schwarz, E.B.; Bost, J.E.; Creinin, M.D.; Ibrahim, S.A. Race, insurance status, and desire for tubal sterilization reversal. Fertil. Steril. 2008, 90, 272–277. [Google Scholar] [CrossRef] [Green Version]
- Kariminia, A.; Saunders, D.M.; Chamberlain, M. Risk factors for strong regret and subsequent IVF request after having tubal ligation. Aust. New Zealand J. Obstet. Gynaecol. 2002, 42, 526–529. [Google Scholar] [CrossRef]
- Moseman, C.P.; Robinson, R.D.; Bates, G.W., Jr.; Propst, A.M. Identifying women who will request sterilization reversal in a military population. Contraception 2006, 73, 512–515. [Google Scholar] [CrossRef]
- Kelekçi, S.; Erdemoglu, E.; Kutluk, S.; Yılmaz, B.; Savan, K. Risk factors for tubal ligation: Regret and psychological effects impact of Beck Depression Inventory. Contraception 2005, 71, 417–420. [Google Scholar] [CrossRef]
- Berger, G.S.; Thorp, J.M., Jr.; Weaver, M.A. Effectiveness of bilateral tubotubal anastomosis in a large outpatient population. Hum. Reprod. 2016, 31, 1120–1125. [Google Scholar] [CrossRef] [Green Version]
- Sreshthaputra, O.; Sreshthaputra, R.A.; Vutyavanich, T. Factors affecting pregnancy rates after microsurgical reversal of tubal sterilization. J. Reconstr. Microsurg. 2013, 29, 189–194. [Google Scholar] [CrossRef]
- Boeckxstaens, A.; Devroey, P.; Collins, J.; Tournaye, H. Getting pregnant after tubal sterilization: Surgical reversal or IVF? Hum. Reprod. 2007, 22, 2660–2664. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hanafi, M.M. Factors affecting the pregnancy rate after microsurgical reversal of tubal ligation. Fertil. Steril. 2003, 80, 434–440. [Google Scholar] [CrossRef]
- Schepens, J.J.; Mol, B.W.; Wiegerinck, M.A.; Houterman, S.; Koks, C.A. Pregnancy outcomes and prognostic factors from tubal sterilization reversal by sutureless laparoscopical re-anastomosis: A retrospective cohort study. Hum. Reprod. 2011, 26, 354–359. [Google Scholar] [CrossRef] [Green Version]
- Gordts, S.; Campo, R.; Puttemans, P.; Gordts, S. Clinical factors determining pregnancy outcome after microsurgical tubal reanastomosis. Fertil. Steril. 2009, 92, 1198–1202. [Google Scholar] [CrossRef]
- Yoon, T.K.; Sung, H.R.; Kang, H.G.; Cha, S.H.; Lee, C.N.; Cha, K.Y. Laparoscopic tubal anastomosis: Fertility outcome in 202 cases. Fertil. Steril. 1999, 72, 1121–1126. [Google Scholar] [CrossRef]
- Kim, S.H.; Shin, C.J.; Kim, J.G.; Moon, S.Y.; Lee, J.Y.; Chang, Y.S. Microsurgical reversal of tubal sterilization: A report on 1,118 cases. Fertil. Steril. 1997, 68, 865–870. [Google Scholar] [CrossRef]
- Alkatout, I. An atraumatic retractor for interdisciplinary use in conventional laparoscopy and robotic surgery. Minim. Invasive Ther. Allied Technol. 2018, 27, 265–271. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alkatout, I.; Mettler, L.; Maass, N.; Ackermann, J. Robotic surgery in gynecology. J. Turk. Ger. Gynecol. Assoc. 2016, 17, 224. [Google Scholar] [CrossRef] [PubMed]
- Madison, A.; Alamri, L.; Schwartz, A.; Brolinson, M.; DeCherney, A. Conventional Laparoscopy Is the Better Option for Tubal Sterilization Reversal: A Closer Look at Tubal Reanastomosis. Women's Health Rep. 2021, 2, 375–380. [Google Scholar] [CrossRef] [PubMed]
- Kavoussi, S.K.; Kavoussi, K.; Lebovic, D.I. Robotic-assisted tubal anastomosis with one-stitch technique. J. Robot. Surg. 2014, 8, 133–136. [Google Scholar] [CrossRef] [Green Version]
- Jayakumaran, J.; Patel, S.D.; Gangrade, B.K.; Narasimhulu, D.M.; Pandian, S.R.; Silva, C. Robotic-assisted laparoscopy in reproductive surgery: A contemporary review. J. Robot. Surg. 2017, 11, 97–109. [Google Scholar] [CrossRef]
- Roh, H.F.; Nam, S.H.; Kim, J.M. Robot-assisted laparoscopic surgery versus conventional laparoscopic surgery in randomized controlled trials: A systematic review and meta-analysis. PLoS ONE 2018, 13, e0191628. [Google Scholar] [CrossRef] [Green Version]
- Barbash, G.I.; Glied, S.A. New technology and health care costs—The case of robot-assisted surgery. N. Engl. J. Med. 2010, 363, 701–704. [Google Scholar] [CrossRef] [Green Version]
- Patel, S.P.D.; Steinkampf, M.P.; Whitten, S.J.; Malizia, B.A. Robotic tubal anastomosis: Surgical technique and cost effectiveness. Fertil. Steril. 2008, 90, 1175–1179. [Google Scholar] [CrossRef]
- Ghomi, A.; Nolan, W.; Rodgers, B. Robotic-assisted laparoscopic tubal anastomosis: Single institution analysis. Int. J. Med. Robot. Comput. Assist. Surg. MRCAS 2020, 16, 1–5. [Google Scholar] [CrossRef]
- Goldberg, J.M.; Falcone, T. Laparoscopic microsurgical tubal anastomosis with and without robotic assistance. Hum. Reprod. 2003, 18, 145–147. [Google Scholar] [CrossRef] [Green Version]
- Hirth, R.; Zbella, E.; Sanchez, M.; Prieto, J. Microtubal reanastomosis: Success rates as compared to in vitro fertilization. J. Reprod. Med. 2010, 55, 161–165. [Google Scholar]
- Practice Committee of the American Society for Reproductive Medicine. Role of tubal surgery in the era of assisted reproductive technology: A committee opinion. Fertil. Steril. 2015, 103, e37–e43. [Google Scholar] [CrossRef]
- Caillet, M.; Vandromme, J.; Rozenberg, S.; Paesmans, M.; Germay, O.; Degueldre, M. Robotically assisted laparoscopic microsurgical tubal reanastomosis: A retrospective study. Fertil. Steril. 2010, 94, 1844–1847. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Method | Advantage | Disadvantage | Risks | Non Contraceptive Benefits |
|---|---|---|---|---|
| Coitus interruptus | Available, free | Depends on male control | Pregnancy | Reduces risk of HIV |
| Lactation | Available, free | Duration of effect is unreliable | Pregnancy | Reduces breast cancer |
| Periodic abstinence | Available, free | Complex method, motivation is essential | pregnancy | None |
| Condom | Available, no prescription needed | Motivation is essential, must be used each time, depends on the man, skin irritation, allergic reaction | Pregnancy | Proven to reduce STDs and cervical cancer |
| Spermicide and sponge | Available, no prescription needed | Must be used each time, skin irritation, allergic reaction | Pregnancy | None |
| Diaphragm, cap | Non-hormonal | Must be used each time, fitting required | Pregnancy, cystitis | Proven to reduce STDs and cervical cancer |
| Copper spiral (ParaGard® IUD) | Highest efficacy, unrelated to coitus | Initial cost, skilled insertion, pain and bleeding, uterine perforation, expulsion | Initial mild risk of PID and septic abortion if pregnancy occurs | None |
| Levonorgestrel-releasing intrauterine system (Mirena®, Kyleena® IUS) | Highest efficiency, unrelated to coitus. non-contraceptive benefits: prevention of endometrial hyperplasia during menopausal hormonal therapy, endometrial protection in breast cancer patients treated with tamoxifen | Initial cost, skilled insertion, amenorrhea for some women, functional ovarian cysts, irregular bleeding (first 3–6 months), uterine perforation, expulsion | Initial mild risk of PID and septic abortion if pregnancy occurs | Reduces menstrual bleeding, can be used to treat menorrhagia |
| Oral contraception, patch, vaginal ring (Nuvaring®) | High efficacy | Must be taken/or changed regularly, costs | Thrombosis, risk of MI and stroke for older smokers | Can be used to treat symptoms of endometriosis and benign ovarian cyst |
| Emergency contraception (levonorgestrel, ulipristal acetate) | Moderate efficacy | Frequent use disrupts menses | None | Unknown |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Salehjawich, A.; Günther, V.; Ruchay, Z.; Al Zoubi, M.S.; Dhanawat, J.; Maass, N.; Ackermann, J.; Pape, J.; Alkatout, I. Robot-Assisted Tubal Reanastomosis after Sterilization: A Choice for Family Planning. J. Clin. Med. 2022, 11, 4385. https://doi.org/10.3390/jcm11154385
Salehjawich A, Günther V, Ruchay Z, Al Zoubi MS, Dhanawat J, Maass N, Ackermann J, Pape J, Alkatout I. Robot-Assisted Tubal Reanastomosis after Sterilization: A Choice for Family Planning. Journal of Clinical Medicine. 2022; 11(15):4385. https://doi.org/10.3390/jcm11154385
Chicago/Turabian StyleSalehjawich, Arwa, Veronika Günther, Zino Ruchay, Mazhar Salim Al Zoubi, Juhi Dhanawat, Nicolai Maass, Johannes Ackermann, Julian Pape, and Ibrahim Alkatout. 2022. "Robot-Assisted Tubal Reanastomosis after Sterilization: A Choice for Family Planning" Journal of Clinical Medicine 11, no. 15: 4385. https://doi.org/10.3390/jcm11154385