Calf Circumference as a Screening Tool for Cognitive Frailty in Community-Dwelling Older Adults: The Korean Frailty and Aging Cohort Study (KFACS)


Abstract
:1. Introduction
2. Materials and Methods
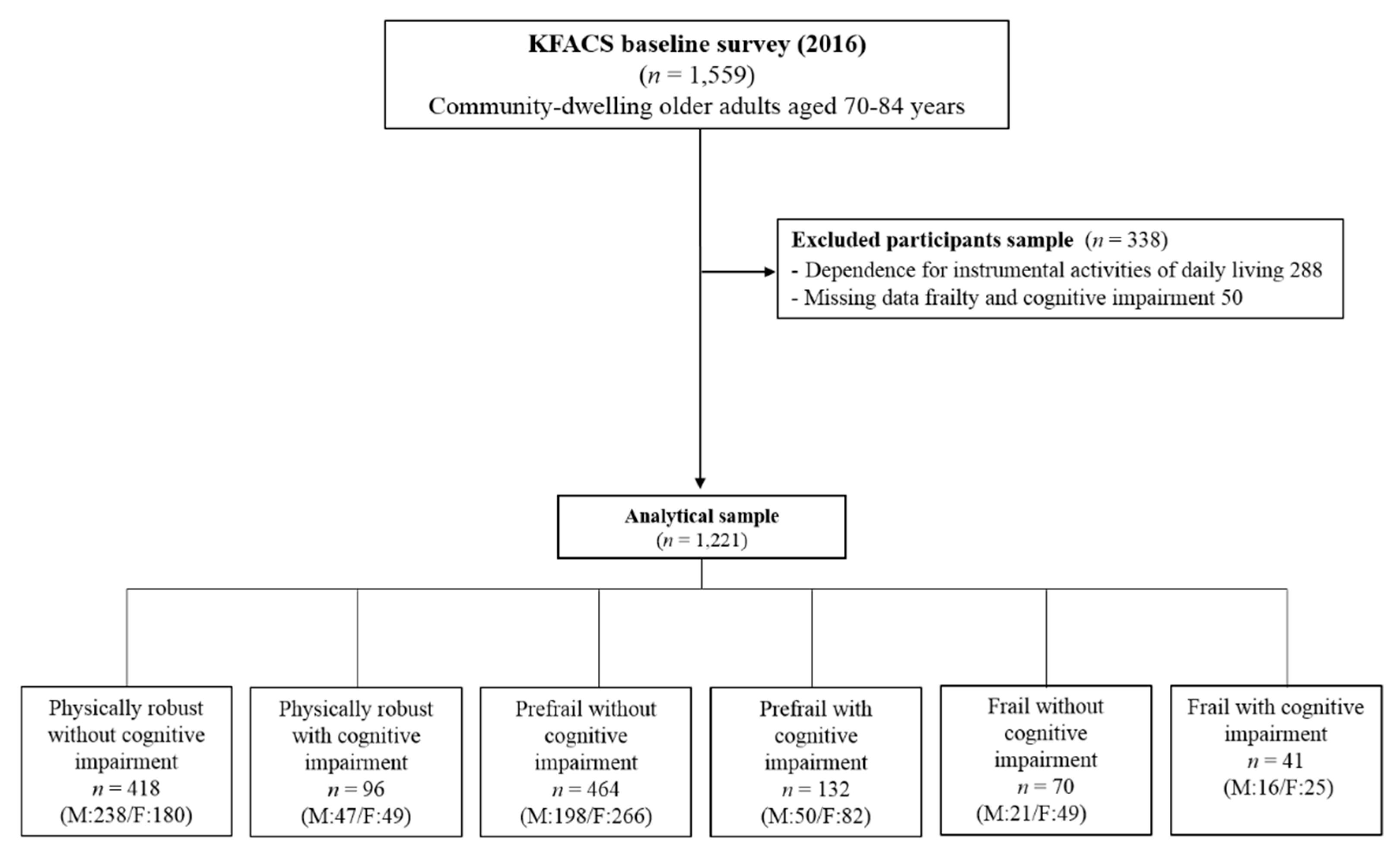
2.1. Study Population
2.2. Physical Frailty, Cognitive Impairment, and Cognitive Frailty
- Unintentional weight loss: responding “yes” to the question: “In the last year, have you lost more than 4.5 kg unintentionally?” or exhibiting unintentional weight loss ≥5% of total body weight in the last year.
- Weakness: maximal grip strength <26 kg for men and <18 kg for women, measured twice for each hand using a digital hand grip dynamometer (T.K.K. 5401; Takei Scientific Instruments Co, Ltd., Tokyo, Japan).
- Self-reported exhaustion: responding “yes” to either of the following statements from the Center for Epidemiological Studies-Depression scale: “I felt that everything I did was an effort” and “I could not get going” on 3 or more days per week.
- Slowness: 4-m gait speed <1.0 m/s, measured using an automatic timer (Gaitspeedometer Ver.1, Dynamicphysiology, Daejeon, Korea), with acceleration and deceleration phases of 1.5 m each. Gait speed was measured twice, and the mean values were used in the analysis.
- Low physical activity: energy expenditure estimates (kcal/week) were calculated for various activities, and metabolic equivalent scores were derived using the International Physical Activity Questionnaire. Low physical activity level was defined as <494.65 kcal for men and <283.50 kcal for women, with these values corresponding to 20% of the total energy consumed in a population-based Korean survey of older adults from among the general population [22].
2.3. Calf Circumference
2.4. Other Measurements
2.5. Ethics
2.6. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Fried, L.P.; Tangen, C.M.; Walston, J.; Newman, A.B.; Hirsch, C.; Gottdiener, J.; Seeman, T.; Tracy, R.; Kop, W.J.; Burke, G.; et al. Frailty in older adults: Evidence for a phenotype. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2001, 56, M146–M156. [Google Scholar] [CrossRef]
- Walston, J.; Hadley, E.C.; Ferrucci, L.; Guralnik, J.M.; Newman, A.B.; Studenski, S.A.; Ershler, W.B.; Harris, T.; Fried, L.P. Research agenda for frailty in older adults: Toward a better understanding of physiology and etiology: Summary from the american geriatrics society/national institute on aging research conference on frailty in older adults. J. Am. Geriatr. Soc. 2006, 54, 991–1001. [Google Scholar] [CrossRef] [PubMed]
- Feng, L.; Zin Nyunt, M.S.; Gao, Q.; Feng, L.; Yap, K.B.; Ng, T.P. Cognitive frailty and adverse health outcomes: Findings from the singapore longitudinal ageing studies (SLAS). J. Am. Med. Dir. Assoc. 2017, 18, 252–258. [Google Scholar] [CrossRef] [PubMed]
- Kelaiditi, E.; Cesari, M.; Canevelli, M.; van Kan, G.A.; Ousset, P.J.; Gillette-Guyonnet, S.; Ritz, P.; Duveau, F.; Soto, M.E.; Provencher, V.; et al. Cognitive frailty: Rational and definition from an (IANA/IAGG) international consensus group. J. Nutr. Health Aging 2013, 17, 726–734. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez-Manas, L.; Feart, C.; Mann, G.; Vina, J.; Chatterji, S.; Chodzko-Zajko, W.; Gonzalez-Colaco Harmand, M.; Bergman, H.; Carcaillon, L.; Nicholson, C.; et al. Searching for an operational definition of frailty: A delphi method based consensus statement: The frailty operative definition-consensus conference project. J. Gerontol. Ser. Biol. Sci. Med. Sci. 2013, 68, 62–67. [Google Scholar] [CrossRef] [PubMed]
- Gross, A.L.; Xue, Q.L.; Bandeen-Roche, K.; Fried, L.P.; Varadhan, R.; McAdams-DeMarco, M.A.; Walston, J.; Carlson, M.C. Declines and impairment in executive function predict onset of physical frailty. J. Gerontol. Ser. Biol. Sci. Med. Sci. 2016, 71, 1624–1630. [Google Scholar] [CrossRef] [PubMed]
- Halil, M.; Cemal Kizilarslanoglu, M.; Emin Kuyumcu, M.; Yesil, Y.; Cruz Jentoft, A.J. Cognitive aspects of frailty: Mechanisms behind the link between frailty and cognitive impairment. J. Nutr. Health Aging 2015, 19, 276–283. [Google Scholar] [CrossRef] [PubMed]
- Feng, L.; Nyunt, M.S.Z.; Gao, Q.; Feng, L.; Lee, T.S.; Tsoi, T.; Chong, M.S.; Lim, W.S.; Collinson, S.; Yap, P.; et al. Physical frailty, cognitive impairment, and the risk of neurocognitive disorder in the Singapore longitudinal ageing studies. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2017, 72, 369–395. [Google Scholar] [CrossRef] [PubMed]
- Solfrizzi, V.; Scafato, E.; Seripa, D.; Lozupone, M.; Imbimbo, B.P.; D’Amato, A.; Tortelli, R.; Schilardi, A.; Galluzzo, L.; Gandin, C.; et al. Reversible cognitive frailty, dementia, and all-cause mortality. The Italian longitudinal study on aging. J. Am. Med. Dir. Assoc. 2017, 18, 89e81–89e88. [Google Scholar] [CrossRef] [PubMed]
- Cruz-Jentoft, A.J.; Baeyens, J.P.; Bauer, J.M.; Boirie, Y.; Cederholm, T.; Landi, F.; Martin, F.C.; Michel, J.P.; Rolland, Y.; Schneider, S.M.; et al. Sarcopenia: European consensus on definition and diagnosis: Report of the european working group on sarcopenia in older people. Age Ageing 2010, 39, 412–423. [Google Scholar] [CrossRef] [PubMed]
- Spauwen, P.J.; Murphy, R.A.; Jonsson, P.V.; Sigurdsson, S.; Garcia, M.E.; Eiriksdottir, G.; van Boxtel, M.P.; Lopez, O.L.; Gudnason, V.; Harris, T.B.; et al. Associations of fat and muscle tissue with cognitive status in older adults: The ages-reykjavik study. Age Ageing 2017, 46, 250–257. [Google Scholar] [CrossRef] [PubMed]
- Chang, K.V.; Hsu, T.H.; Wu, W.T.; Huang, K.C.; Han, D.S. Association between sarcopenia and cognitive impairment: A systematic review and meta-analysis. J. Am. Med. Dir. Assoc. 2016, 17, 1164.e7–1164.e15. [Google Scholar] [CrossRef] [PubMed]
- Cesari, M.; Leeuwenburgh, C.; Lauretani, F.; Onder, G.; Bandinelli, S.; Maraldi, C.; Guralnik, J.M.; Pahor, M.; Ferrucci, L. Frailty syndrome and skeletal muscle: Results from the invecchiare in chianti study. Am. J. Clin. Nutr. 2006, 83, 1142–1148. [Google Scholar] [CrossRef] [PubMed]
- Kawakami, R.; Murakami, H.; Sanada, K.; Tanaka, N.; Sawada, S.S.; Tabata, I.; Higuchi, M.; Miyachi, M. Calf circumference as a surrogate marker of muscle mass for diagnosing sarcopenia in Japanese men and women. Geriatr. Gerontol. Int. 2015, 15, 969–976. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.; Kim, M.; Lee, Y.; Kim, B.; Yoon, T.Y.; Won, C.W. Calf circumference as a simple screening marker for diagnosing sarcopenia in older korean adults: The korean frailty and aging cohort study (KFACS). J. Korean Med. Sci 2018, 33, e151. [Google Scholar] [CrossRef] [PubMed]
- Maeda, K.; Koga, T.; Nasu, T.; Takaki, M.; Akagi, J. Predictive accuracy of calf circumference measurements to detect decreased skeletal muscle mass and European society for clinical nutrition and metabolism-defined malnutrition in hospitalized older patients. Ann. Nutr. Metab. 2017, 71, 10–15. [Google Scholar] [CrossRef] [PubMed]
- Aparecida Leandro-Merhi, V.; Luiz Braga de Aquino, J.; Gonzaga Teixeira de Camargo, J. Agreement between body mass index, calf circumference, arm circumference, habitual energy intake and the mna in hospitalized elderly. J. Nutr. Health Aging 2012, 16, 128–132. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.; Suzuki, T.; Kim, M.; Kojima, N.; Yoshida, Y.; Hirano, H.; Saito, K.; Iwasa, H.; Shimada, H.; Hosoi, E.; et al. Incidence and predictors of sarcopenia onset in community-dwelling elderly japanese women: 4-year follow-up study. J. Am. Med. Dir. Assoc. 2015, 16, 85.e1–85.e8. [Google Scholar] [CrossRef] [PubMed]
- Landi, F.; Onder, G.; Russo, A.; Liperoti, R.; Tosato, M.; Martone, A.M.; Capoluongo, E.; Bernabei, R. Calf circumference, frailty and physical performance among older adults living in the community. Clin. Nutr. 2014, 33, 539–544. [Google Scholar] [CrossRef] [PubMed]
- Won, H.; Abdul Manaf, Z.; Mat Ludin, A.F.; Shahar, S. Wide range of body composition measures are associated with cognitive function in community-dwelling older adults. Geriatr. Gerontol. Int. 2017, 17, 554–560. [Google Scholar] [CrossRef] [PubMed]
- Won, C.W.; Lee, Y.; Choi, J.; Kim, K.W.; Park, Y.; Park, H.; Oh, I.-H.; Ga, H.; Kim, Y.S.; Jang, H.C. Starting construction of frailty cohort for elderly and intervention study. Ann. Geriatr. Med. Res. 2016, 20, 114–117. [Google Scholar] [CrossRef]
- Son, J.H.; Kim, S.Y.; Won, C.W.; Choi, H.R.; Kim, B.S.; Park, M.S. Physical frailty predicts medical expenses in community-dwelling, elderly patients: Three-year prospective findings from living profiles of older people surveys in korea. Eur. Geriatr. Med. 2015, 6, 412–416. [Google Scholar] [CrossRef]
- Won, C.W.; Lee, Y.; Kim, S.; Yoo, J.; Kim, M.; Ng, T.P.; Kim, H.; Son, S.J. Modified criteria for diagnosing “cognitive frailty”. Psychiatry Investig. 2018, 15, 839–842. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.H.; Lee, K.U.; Lee, D.Y.; Kim, K.W.; Jhoo, J.H.; Kim, J.H.; Lee, K.H.; Kim, S.Y.; Han, S.H.; Woo, J.I. Development of the korean version of the consortium to establish a registry for alzheimer’s disease assessment packet (CERAD-K): Clinical and neuropsychological assessment batteries. J. Gerontol. Ser. B Psychol. Sci. Soc. Sci. 2002, 57, P47–P53. [Google Scholar] [CrossRef]
- Lee, D.Y.; Lee, K.U.; Lee, J.H.; Kim, K.W.; Jhoo, J.H.; Kim, S.Y.; Yoon, J.C.; Woo, S.I.; Ha, J.; Woo, J.I. A normative study of the cerad neuropsychological assessment battery in the Korean elderly. J. Int. Neuropsychol. Soc. 2004, 10, 72–81. [Google Scholar] [CrossRef] [PubMed]
- Kim, T.H.; Huh, Y.; Choe, J.Y.; Jeong, J.W.; Park, J.H.; Lee, S.B.; Lee, J.J.; Jhoo, J.H.; Lee, D.Y.; Woo, J.I.; et al. Korean version of frontal assessment battery: Psychometric properties and normative data. Dement. Geriatr. Cognit. Disord. 2010, 29, 363–370. [Google Scholar] [CrossRef] [PubMed]
- Aisen, P.S. Treatment for MCI: Is the evidence sufficient? Neurology 2008, 70, 2020–2021. [Google Scholar] [CrossRef] [PubMed]
- Petersen, R.C.; Smith, G.E.; Waring, S.C.; Ivnik, R.J.; Tangalos, E.G.; Kokmen, E. Mild cognitive impairment: Clinical characterization and outcome. Arch. Neurol. 1999, 56, 303–308. [Google Scholar] [CrossRef] [PubMed]
- Jessen, F.; Amariglio, R.E.; van Boxtel, M.; Breteler, M.; Ceccaldi, M.; Chetelat, G.; Dubois, B.; Dufouil, C.; Ellis, K.A.; van der Flier, W.M.; et al. A conceptual framework for research on subjective cognitive decline in preclinical Alzheimer’s disease. Alzheimer’s Dement. J. Alzheimer’s Assoc. 2014, 10, 844–852. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dubois, B.; Feldman, H.H.; Jacova, C.; Cummings, J.L.; Dekosky, S.T.; Barberger-Gateau, P.; Delacourte, A.; Frisoni, G.; Fox, N.C.; Galasko, D.; et al. Revising the definition of Alzheimer’s disease: A new lexicon. Lancet Neurol. 2010, 9, 1118–1127. [Google Scholar] [CrossRef]
- Lee, W.J.; Peng, L.N.; Liang, C.K.; Loh, C.H.; Chen, L.K. Cognitive frailty predicting all-cause mortality among community-living older adults in Taiwan: A 4-year nationwide population-based cohort study. PLoS ONE 2018, 13, e0200447. [Google Scholar] [CrossRef] [PubMed]
- Shimada, H.; Doi, T.; Lee, S.; Makizako, H.; Chen, L.K.; Arai, H. Cognitive frailty predicts incident dementia among community-dwelling older people. J. Clin. Med. 2018, 7, 250. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.K.; Liu, L.K.; Woo, J.; Assantachai, P.; Auyeung, T.W.; Bahyah, K.S.; Chou, M.Y.; Chen, L.Y.; Hsu, P.S.; Krairit, O.; et al. Sarcopenia in asia: Consensus report of the asian working group for sarcopenia. J. Am. Med. Dir. Assoc. 2014, 15, 95–101. [Google Scholar] [CrossRef] [PubMed]
- Guralnik, J.M.; Simonsick, E.M.; Ferrucci, L.; Glynn, R.J.; Berkman, L.F.; Blazer, D.G.; Scherr, P.A.; Wallace, R.B. A short physical performance battery assessing lower extremity function: Association with self-reported disability and prediction of mortality and nursing home admission. J. Gerontol. 1994, 49, M85–M94. [Google Scholar] [CrossRef] [PubMed]
- Guralnik, J.M.; Ferrucci, L.; Pieper, C.F.; Leveille, S.G.; Markides, K.S.; Ostir, G.V.; Studenski, S.; Berkman, L.F.; Wallace, R.B. Lower extremity function and subsequent disability: Consistency across studies, predictive models, and value of gait speed alone compared with the short physical performance battery. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2000, 55, M221–M231. [Google Scholar] [CrossRef]
- Podsiadlo, D.; Richardson, S. The timed “up & go”: A test of basic functional mobility for frail elderly persons. J.Am. Geriatr. Soc. 1991, 39, 142–148. [Google Scholar] [PubMed]
- Heinze, G.; Schemper, M. A solution to the problem of separation in logistic regression. Stat. Med. 2002, 21, 2409–2419. [Google Scholar] [CrossRef] [PubMed]
- Shimada, H.; Makizako, H.; Doi, T.; Yoshida, D.; Tsutsumimoto, K.; Anan, Y.; Uemura, K.; Ito, T.; Lee, S.; Park, H.; et al. Combined prevalence of frailty and mild cognitive impairment in a population of elderly Japanese people. J. Am. Med. Dir. Assoc. 2013, 14, 518–524. [Google Scholar] [CrossRef] [PubMed]
- Sugimoto, T.; Sakurai, T.; Ono, R.; Kimura, A.; Saji, N.; Niida, S.; Toba, K.; Chen, L.K.; Arai, H. Epidemiological and clinical significance of cognitive frailty: A mini review. Ageing Res. Rev. 2018, 44, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Solfrizzi, V.; Scafato, E.; Lozupone, M.; Seripa, D.; Giannini, M.; Sardone, R.; Bonfiglio, C.; Abbrescia, D.I.; Galluzzo, L.; Gandin, C.; et al. Additive role of a potentially reversible cognitive frailty model and inflammatory state on the risk of disability: The Italian longitudinal study on aging. Am. J. Geriatr. Psychiatry 2017, 25, 1236–1248. [Google Scholar] [CrossRef] [PubMed]
- Shimada, H.; Makizako, H.; Lee, S.; Doi, T.; Lee, S.; Tsutsumimoto, K.; Harada, K.; Hotta, R.; Bae, S.; Nakakubo, S.; et al. Impact of cognitive frailty on daily activities in older persons. J. Nutr. Health Aging 2016, 20, 729–735. [Google Scholar] [CrossRef] [PubMed]
- St John, P.D.; Tyas, S.L.; Griffith, L.E.; Menec, V. The cumulative effect of frailty and cognition on mortality–results of a prospective cohort study. Int. Psychogeriatr. 2017, 29, 535–543. [Google Scholar] [CrossRef] [PubMed]
- Tsai, A.C.; Chang, T.L. The effectiveness of BMI, calf circumference and mid-arm circumference in predicting subsequent mortality risk in elderly taiwanese. Br. J. Nutr. 2011, 105, 275–281. [Google Scholar] [CrossRef] [PubMed]
- Sun, Y.S.; Kao, T.W.; Chang, Y.W.; Fang, W.H.; Wang, C.C.; Wu, L.W.; Yang, H.F.; Liaw, F.Y.; Chen, W.L. Calf circumference as a novel tool for risk of disability of the elderly population. Sci. Rep. 2017, 7, 16359. [Google Scholar] [CrossRef] [PubMed]
- Hsu, W.C.; Tsai, A.C.; Wang, J.Y. Calf circumference is more effective than body mass index in predicting emerging care-need of older adults—Results of a national cohort study. Clin. Nutr. 2016, 35, 735–740. [Google Scholar] [CrossRef] [PubMed]
- Rolland, Y.; Lauwers-Cances, V.; Cournot, M.; Nourhashemi, F.; Reynish, W.; Riviere, D.; Vellas, B.; Grandjean, H. Sarcopenia, calf circumference, and physical function of elderly women: A cross-sectional study. J. Am. Geriatr. Soc. 2003, 51, 1120–1124. [Google Scholar] [CrossRef] [PubMed]
- Walston, J.; Fried, L.P. Frailty and the older man. Med. Clin. N. Am. 1999, 83, 1173–1194. [Google Scholar] [CrossRef]
- Kim, J.; Lee, Y.; Won, C.W.; Lee, K.E.; Chon, D. Nutritional status and frailty in community-dwelling older korean adults: The korean frailty and aging cohort study. J. Nutr. Health Aging 2018, 22, 774–778. [Google Scholar] [CrossRef] [PubMed]
- Portero-McLellan, K.C.; Staudt, C.; Silva, F.R.; Delbue Bernardi, J.L.; Baston Frenhani, P.; Leandro Mehri, V.A. The use of calf circumference measurement as an anthropometric tool to monitor nutritional status in elderly inpatients. J. Nutr. Health Aging 2010, 14, 266–270. [Google Scholar] [CrossRef] [PubMed]
- Nishiguchi, S.; Yamada, M.; Fukutani, N.; Adachi, D.; Tashiro, Y.; Hotta, T.; Morino, S.; Shirooka, H.; Nozaki, Y.; Hirata, H.; et al. Differential association of frailty with cognitive decline and sarcopenia in community-dwelling older adults. J. Am. Med. Dir. Assoc. 2015, 16, 120–124. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abellan van Kan, G.; Cesari, M.; Gillette-Guyonnet, S.; Dupuy, C.; Nourhashemi, F.; Schott, A.M.; Beauchet, O.; Annweiler, C.; Vellas, B.; Rolland, Y. Sarcopenia and cognitive impairment in elderly women: Results from the epidos cohort. Age Ageing 2013, 42, 196–202. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Auyeung, T.W.; Kwok, T.; Lee, J.; Leung, P.C.; Leung, J.; Woo, J. Functional decline in cognitive impairment—The relationship between physical and cognitive function. Neuroepidemiology 2008, 31, 167–173. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variable | Physically Robust without Cog Imp (n = 238) | Physically Robust with Cog Imp (n = 47) | Prefrail without Cog Imp (n = 198) | Prefrail with Cog Imp (n = 50) | Frail without Cog Imp (n = 21) | Frail with Cog Imp (n = 16) | p-Value | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Age (years) | 75.7 | (3.7) | 76.1 | (3.7) | 76.7 | (4.1) | 77.4 | (3.6) | 78.8 | (3.8) | 78.3 | (3.6) | <0.001 |
| BMI (kg/m2) | 24.0 | (2.7) | 25.0 | (2.4) | 23.9 | (3.1) | 23.9 | (3.1) | 23.2 | (3.6) | 21.2 | (2.5) | 0.001 |
| Smoking status | |||||||||||||
| Never | 50 | (21.0) | 15 | (31.9) | 37 | (18.7) | 10 | (20.0) | 6 | (28.6) | 2 | (12.5) | 0.363 |
| Ever | 188 | (79.0) | 32 | (68.1) | 161 | (81.3) | 40 | (80.0) | 15 | (71.4) | 14 | (87.5) | |
| Alcohol (servings per week) a | |||||||||||||
| Never | 62 | (26.1) | 15 | (32.6) | 68 | (34.3) | 25 | (50.0) | 9 | (42.9) | 7 | (43.8) | 0.018 |
| Ever | 176 | (74.0) | 31 | (67.4) | 130 | (65.7) | 25 | (50.0) | 12 | (57.1) | 9 | (56.2) | |
| Education (years) | |||||||||||||
| 0–6 | 56 | (23.5) | 11 | (23.4) | 62 | (31.3) | 16 | (32.0) | 11 | (52.4) | 8 | (50.0) | 0.016 |
| ≥7 | 182 | (76.5) | 36 | (76.6) | 136 | (68.7) | 34 | (68.0) | 10 | (47.6) | 8 | (50.0) | |
| Marital status | |||||||||||||
| Married | 218 | (91.6) | 40 | (85.1) | 172 | (86.9) | 42 | (84.0) | 18 | (85.7) | 11 | (68.8) | 0.077 |
| Unmarried, divorced, widowed, or separated | 20 | (8.4) | 7 | (14.9) | 26 | (13.1) | 8 | (16.0) | 3 | (14.3) | 5 | (31.2) | |
| SPPB score a | 11.4 | (0.9) | 11.1 | (1.3) | 11.0 | (1.2) | 10.6 | (1.5) | 10.0 | (2.3) | 9.1 | (2.2) | <0.001 |
| Timed Up and Go test | |||||||||||||
| ≤10 s | 165 | (69.3) | 25 | (53.2) | 96 | (48.5) | 17 | (34.0) | 2 | (9.5) | 1 | (6.2) | <0.001 |
| >10 s | 73 | (30.7) | 22 | (46.8) | 102 | (51.5) | 33 | (66.0) | 19 | (90.5) | 15 | (93.8) | |
| ASM/height2 (kg/m2) a | 7.2 | (0.9) | 7.4 | (0.8) | 7.1 | (1.0) | 7.2 | (0.9) | 7.1 | (1.0) | 6.2 | (0.7) | <0.001 |
| Normal muscle mass | 139 | (58.9) | 34 | (72.3) | 98 | (49.8) | 27 | (54.0) | 13 | (61.9) | 2 | (12.5) | 0.001 |
| Low muscle mass | 97 | (41.1) | 13 | (27.7) | 99 | (50.2) | 23 | (46.0) | 8 | (38.1) | 14 | (87.5) | |
| Number of comorbidities | |||||||||||||
| 0 | 160 | (67.2) | 36 | (76.6) | 103 | (52.0) | 28 | (56.0) | 6 | (28.6) | 9 | (56.2) | <0.001 |
| ≥1 | 78 | (32.8) | 11 | (23.4) | 95 | (48.0) | 22 | (44.0) | 15 | (71.4) | 7 | (43.8) | |
| Number of medications a | |||||||||||||
| 0 | 54 | (22.7) | 12 | (25.5) | 31 | (15.7) | 4 | (8.0) | 0 | (0.0) | 1 | (6.2) | <0.001 |
| 1–4 | 112 | (47.1) | 26 | (55.3) | 88 | (44.4) | 20 | (40.0) | 7 | (33.3) | 7 | (43.8) | |
| ≥5 | 72 | (30.2) | 9 | (19.2) | 79 | (39.9) | 26 | (52.0) | 14 | (66.7) | 8 | (50.0) | |
| Calf circumference (cm) | 34.8 | (2.4) | 34.7 | (2.8) | 33.8 | (2.8) | 33.6 | (2.8) | 32.6 | (3.4) | 30.5 | (2.4) | <0.001 |
| Variable | Physically Robust without Cog Imp (n = 180) | Physically Robust with Cog Imp (n = 49) | Prefrail without Cog Imp (n = 266) | Prefrail with Cog Imp (n = 82) | Frail without Cog Imp (n = 49) | Frail with Cog Imp (n = 25) | p-Value | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Age (years) | 74.5 | (3.4) | 75.2 | (3.6) | 75.7 | (4.0) | 76.0 | (3.3) | 78.1 | (4.3) | 78.5 | (3.2) | <0.001 |
| BMI (kg/m2) | 24.9 | (3.0) | 24.0 | (2.2) | 24.5 | (2.9) | 25.0 | (2.7) | 24.3 | (3.3) | 24.9 | (3.9) | 0.704 |
| Smoking status | |||||||||||||
| Never | 177 | (98.3) | 46 | (93.9) | 259 | (97.4) | 81 | (98.8) | 47 | (95.9) | 24 | (96.0) | 0.360 |
| Ever | 3 | (1.7) | 3 | (6.1) | 7 | (2.6) | 1 | (1.2) | 2 | (4.1) | 1 | (4.0) | |
| Alcohol (servings per week) a | |||||||||||||
| Never | 103 | (58.2) | 34 | (69.4) | 165 | (62.3) | 47 | (58.8) | 38 | (77.6) | 15 | (60.0) | 0.176 |
| Ever | 74 | (41.8) | 15 | (30.6) | 100 | (37.7) | 33 | (41.3) | 11 | (22.4) | 10 | (40.0) | |
| Education (years) | |||||||||||||
| 0–6 | 84 | (46.7) | 29 | (59.2) | 150 | (56.4) | 62 | (75.6) | 43 | (87.8) | 21 | (84.0) | <0.001 |
| ≥7 | 96 | (53.3) | 20 | (40.8) | 116 | (43.6) | 20 | (24.4) | 6 | (12.2) | 4 | (16.0) | |
| Marital status | |||||||||||||
| Married | 85 | (47.2) | 20 | (40.8) | 123 | (46.2) | 30 | (36.6) | 21 | (42.9) | 8 | (32.0) | 0.439 |
| Unmarried, divorced, widowed, or separated | 95 | (52.8) | 29 | (59.2) | 143 | (53.8) | 52 | (63.4) | 28 | (57.1) | 17 | (68.0) | |
| SPPB score a | 11.3 | (1.0) | 11.2 | (1.1) | 10.8 | (1.2) | 10.3 | (1.5) | 9.4 | (1.8) | 9.0 | (1.6) | <0.001 |
| Timed Up and Go test | |||||||||||||
| ≤10 s | 125 | (69.4) | 34 | (69.4) | 134 | (50.4) | 25 | (30.5) | 3 | (6.1) | 0 | (0.0) | <0.001 |
| >10 s | 55 | (30.6) | 15 | (30.6) | 132 | (49.6) | 57 | (69.5) | 46 | (93.9) | 25 | (100.0) | |
| ASM/height2 (kg/m2) a | 6.1 | (0.9) | 6.2 | (0.9) | 6.0 | (0.9) | 5.9 | (0.8) | 6.0 | (0.9) | 6.0 | (1.1) | 0.704 |
| Normal muscle mass | 141 | (78.3) | 43 | (87.8) | 206 | (77.4) | 54 | (65.9) | 33 | (67.4) | 17 | (68.0) | 0.034 |
| Low muscle mass | 39 | (21.7) | 6 | (12.2) | 60 | (22.6) | 28 | (34.1) | 16 | (32.7) | 8 | (32.0) | |
| Number of comorbidities | |||||||||||||
| 0 | 124 | (68.9) | 39 | (79.6) | 179 | (67.3) | 48 | (58.5) | 27 | (55.1) | 18 | (72.0) | 0.079 |
| ≥1 | 56 | (31.1) | 10 | (20.4) | 87 | (32.7) | 34 | (41.5) | 22 | (44.9) | 7 | (28.0) | |
| Number of medications a | |||||||||||||
| 0 | 33 | (18.3) | 11 | (22.5) | 29 | (10.9) | 14 | (17.1) | 1 | (2.0) | 6 | (24.0) | <0.001 |
| 1–4 | 107 | (59.4) | 28 | (57.1) | 162 | (60.9) | 35 | (42.7) | 19 | (38.8) | 12 | (48.0) | |
| ≥5 | 40 | (22.2) | 10 | (20.4) | 75 | (28.2) | 33 | (40.2) | 29 | (59.2) | 7 | (28.0) | |
| Calf circumference (cm) | 33.1 | (2.7) | 32.7 | (2.1) | 32.6 | (2.6) | 32.3 | (2.9) | 31.1 | (3.2) | 31.7 | (3.0) | <0.001 |
| Variable | Unadjusted | Model 1 | Model 2 | Model 3 | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Estimate | 95% CI | p-Value | Estimate | 95% CI | p-Value | Estimate | 95% CI | p-Value | Estimate | 95% CI | p-Value | |
| Cognitive frailty status | ||||||||||||
| Physically robust without Cog Imp | Ref. | Ref. | Ref. | Ref. | ||||||||
| Physically robust with Cog Imp | −0.139 | −0.982, 0.703 | 0.746 | −0.109 | −0.947, 0.729 | 0.789 | −1.116 | −0.956, 0.723 | 0.786 | −0.682 | −1.352, −0.013 | 0.046 |
| Prefrail without Cog Imp | −0.946 | −1.472, −0.457 | 0.000 | −0.885 | −1.393, −0.377 | 0.001 | −0.803 | −1.310, −0.296 | 0.002 | −0.745 | −1.150, −0.340 | <0.001 |
| Prefrail with Cog Imp | −1.243 | −2.064, −0.422 | 0.003 | −1.107 | −1.930, −0.285 | 0.008 | −0.959 | −1.783, −1.134 | 0.023 | −0.932 | −1.589, −0.275 | 0.005 |
| Frail without Cog Imp | −2.182 | −3.383, −0.980 | 0.000 | −1.945 | −3.152, −0.738 | 0.002 | −1.697 | −2.905, −0.488 | 0.006 | −1.299 | −2.274, −0.324 | 0.009 |
| Frail with Cog Imp | −4.301 | −5.664, −2.938 | 0.000 | −4.098 | −5.462, −2.735 | 0.000 | −3.862 | −5.224, −2.501 | 0.000 | −2.471 | −3.566, −1.377 | <0.001 |
| Variable | Unadjusted | Model 1 | Model 2 | Model 3 | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Estimate | 95% CI | p-Value | Estimate | 95% CI | p-Value | Estimate | 95% CI | p-Value | Estimate | 95% CI | p-Value | |
| Cognitive frailty status | Ref. | |||||||||||
| Physically robust without Cog Imp | Ref. | Ref. | Ref. | |||||||||
| Physically robust with Cog Imp | −0.370 | −1.216, 0.476 | 0.391 | −0.282 | −1.116, 0.551 | 0.507 | −0.232 | −1.071, 0.606 | 0.587 | 0.021 | −1.636, 0.677 | 0.951 |
| Prefrail without Cog Imp | −0.493 | −1.000, 0.013 | 0.056 | −0.331 | −0.835, 0.172 | 0.197 | −0.301 | −0.809, 0.280 | 0.246 | −0.408 | −1.806, −0.011 | 0.044 |
| Prefrail with Cog Imp | −0.842 | −1.542, −0.143 | 0.018 | −0.642 | −1.336, 0.052 | 0.070 | −0.515 | −1.229, 0.198 | 0.157 | −0.681 | −1.241, −0.121 | 0.017 |
| Frail without Cog Imp | −2.001 | −2.847, −1.115 | 0.000 | −1.535 | −2.391, −0.679 | 0.000 | −1.362 | −2.240, −0.484 | 0.002 | −1.104 | −1.799, −0.409 | 0.002 |
| Frail with Cog Imp | −1.378 | −2.499, −0.258 | 0.016 | −0.859 | −1.984, 0.266 | 0.135 | −0.712 | −1.849, 0.425 | 0.220 | −0.509 | −1.397, 0.379 | 0.261 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, M.; Jeong, M.J.; Yoo, J.; Song, D.Y.; Won, C.W. Calf Circumference as a Screening Tool for Cognitive Frailty in Community-Dwelling Older Adults: The Korean Frailty and Aging Cohort Study (KFACS). J. Clin. Med. 2018, 7, 332. https://doi.org/10.3390/jcm7100332
Kim M, Jeong MJ, Yoo J, Song DY, Won CW. Calf Circumference as a Screening Tool for Cognitive Frailty in Community-Dwelling Older Adults: The Korean Frailty and Aging Cohort Study (KFACS). Journal of Clinical Medicine. 2018; 7(10):332. https://doi.org/10.3390/jcm7100332
Chicago/Turabian StyleKim, Miji, Min Jeong Jeong, Jinho Yoo, Da Young Song, and Chang Won Won. 2018. "Calf Circumference as a Screening Tool for Cognitive Frailty in Community-Dwelling Older Adults: The Korean Frailty and Aging Cohort Study (KFACS)" Journal of Clinical Medicine 7, no. 10: 332. https://doi.org/10.3390/jcm7100332