Sarcopenia in Patients with Rheumatic Diseases: Prevalence and Associated Risk Factors

 , , ,
, , ,
Abstract
:1. Introduction
2. Patients and Methods
2.1. Patients Characteristics
2.2. Nutritional Evaluations
2.3. Sarcopenia Evaluation
2.4. Disease Activity Assessment
2.5. Statistical Analysis
3. Results
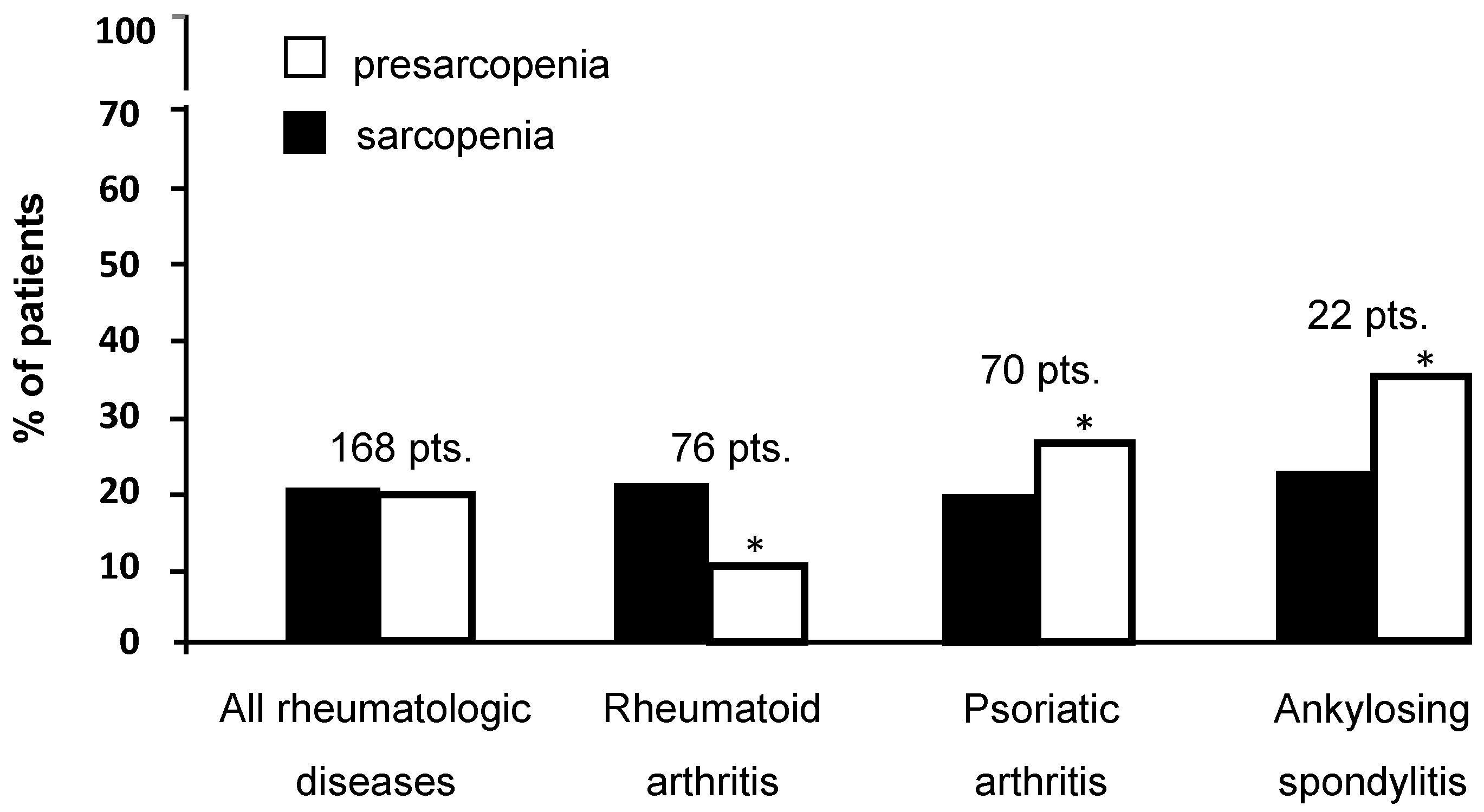
3.1. Prevalence of Sarcopenia and Presarcopenia
3.2. Factors Associated with Sarcopenia in Rheumatologic Diseases
4. Discussion
5. Conclusions
Author Contributions
Conflicts of Interest
References
- Cruz-Jentoft, A.J.; Baeyens, J.P.; Bauer, J.M.; Boirie, Y.; Cederholm, T.; Landi, F.; Martin, F.C.; Michel, J.P.; Rolland, Y.; Schneider, S.M.; et al. Sarcopenia: European consensus on definition and diagnosis: Report of the European Working Group on Sarcopenia in Older People. Age Ageing 2010, 39, 412–423. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barone, M.; Viggiani, M.T.; Avolio, A.W.; Iannone, A.; Rendina, M.; Di Leo, A. Obesity as predictor of postoperative outcomes in liver transplant candidates: Review of the literature and future perspectives. Dig. Liver Dis. 2017, 49, 957–966. [Google Scholar] [CrossRef] [PubMed]
- Baracos, V.; Caserotti, P.; Earthman, C.P.; Fields, D.; Gallagher, D.; Hall, K.D.; Heymsfield, S.B.; Müller, M.J.; Rosen, A.N.; Pichard, C.; et al. Advances in the science and application of body composition measurement. J. Parenter. Enteral Nutr. 2012, 36, 96–107. [Google Scholar] [CrossRef] [PubMed]
- Giles, J.T.; Ling, S.M.; Ferrucci, L.; Bartlett, S.J.; Andersen, R.E.; Towns, M.; Muller, D.; Fontaine, K.R.; Bathon, J.M. Abnormal body composition phenotypes in older rheumatoid arthritis patients: Association with disease characteristics and pharmacotherapies. Arthritis Rheum. 2008, 59, 807–815. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dao, H.H.; Do, Q.T.; Sakamoto, J. Abnormal body composition phenotypes in Vietnamese women with early rheumatoid arthritis. Rheumatology 2011, 50, 1250–1258. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aguiar, R.; Sequeira, J.; Meirinhos, T.; Ambrósio, C.; Barcelos, A. SARCOSPA—Sarcopenia in spondyloarthritis patients. Acta Reumatol. Port. 2014, 39, 322–326. [Google Scholar]
- Doğan, S.C.; Hizmetli, S.; Hayta, E.; Kaptanoğlu, E.; Erselcan, T.; Güler, E. Sarcopenia in women with rheumatoid arthritis. Eur. J. Rheumatol. 2015, 2, 57–61. [Google Scholar] [CrossRef]
- Elkan, A.C.; Engvall, I.L.; Cederholm, T.; Hafström, I. Rheumatoid cachexia, central obesity and malnutrition in patients with low-active rheumatoid arthritis: Feasibility of anthropometry, Mini Nutritional Assessment and body composition techniques. Eur. J. Nutr. 2009, 48, 315–322. [Google Scholar] [CrossRef]
- Ngeuleu, A.; Allali, F.; Medrare, L.; Madhi, A.; Rkain, H.; Hajjaj-Hassouni, N. Sarcopenia in rheumatoid arthritis: Prevalence, influence of disease activity and associated factors. Rheumatol. Int. 2017, 37, 1015–1020. [Google Scholar] [CrossRef]
- Tournadre, A.; Pereira, B.; Dutheil, F.; Giraud, C.; Courteix, D.; Sapin, V.; Frayssac, T.; Mathieu, S.; Malochet-Guinamand, S.; Soubrier, M. Changes in body composition and metabolic profile during interleukin 6 inhibition in rheumatoid arthritis. J. Cachexia Sarcopenia Muscle 2017, 8, 639–646. [Google Scholar] [CrossRef] [Green Version]
- El Maghraoui, A.; Ebo’o, F.B.; Sadni, S.; Majjad, A.; Hamza, T.; Mounach, A. Is there a relation between pre-sarcopenia, sarcopenia, cachexia and osteoporosis in patients with ankylosing spondylitis? BMC Musculoskelet Disord. 2016, 17, 268. [Google Scholar] [CrossRef] [PubMed]
- Krajewska-Włodarczyk, M.; Owczarczyk-Saczonek, A.; Placek, W. Changes in body composition and bone mineral density in postmenopausal women with psoriatic arthritis. Reumatologia 2017, 55, 215–221. [Google Scholar] [CrossRef] [PubMed]
- Torii, M.; Hashimoto, M.; Hanai, A.; Fujii, T.; Furu, M.; Ito, H.; Uozumi, R.; Hamaguchi, M.; Terao, C.; Yamamoto, W.; et al. Prevalence and factors associated with sarcopenia in patients with rheumatoid arthritis. Mod. Rheumatol. 2018, 11, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Lee, R.C.; Wang, Z.; Heo, M.; Ross, R.; Janssen, I.; Heymsfield, S.B. Total-body skeletal muscle mass: Development and cross-validation of anthropometric prediction models. Am. J. Clin. Nutr. 2000, 72, 796–803. [Google Scholar] [CrossRef] [PubMed]
- Barone, M.; Della Valle, N.; Rosania, R.; Facciorusso, A.; Trotta, A.; Cantatore, F.P.; Falco, S.; Pignatiello, S.; Viggiani, M.T.; Amoruso, A.; et al. A comparison of the nutritional status between adult celiac patients on a long-term, strictly gluten-free diet and healthy subjects. Eur. J. Clin. Nutr. 2016, 70, 23–27. [Google Scholar] [CrossRef] [PubMed]
- Human Energy Requirements: Report of a Joint FAO/WHO/UNU Expert Consultation. Available online: http://www.fao.org/3/a-y5686e.pdf (accessed on 5 November 2018).
- Viggiani, M.T.; Lorusso, O.; Natalizio, F.; Principi, M.; Di Leo, A.; Barone, M. Influence of chemotherapy on total energy expenditure in patients with gastrointestinal cancer: A pilot study. Nutrition 2017, 42, 7–11. [Google Scholar] [CrossRef] [PubMed]
- Alkan Melikoğlu, M. Presarcopenia and its impact on disability in female patients with rheumatoid arthritis. Arch. Rheumatol. 2017, 32, 53–59. [Google Scholar] [CrossRef]
- Janssen, I.; Baumgartner, R.N.; Ross, R.; Rosenberg, I.H.; Roubenoff, R. Skeletal muscle cutpoints associated with elevated physical disability risk in older men and women. Am. J. Epidemiol. 2004, 159, 413–421. [Google Scholar] [CrossRef]
- Lauretani, F.; Russo, C.R.; Bandinelli, S.; Bartali, B.; Cavazzini, C.; Di Iorio, A.; Corsi, A.M.; Rantanen, T.; Guralnik, J.M.; Ferrucci, L. Age-associated changes in skeletal muscles and their effect on mobility: An operational diagnosis of sarcopenia. J. Appl. Physiol. 2003, 95, 1851–1860. [Google Scholar] [CrossRef]
- Smolen, J.S.; Breedveld, F.C.; Eberl, G.; Jones, I.; Leeming, M.; Wylie, G.L.; Kirkpatrick, J. Validity and reliability of the twenty-eightjoint count for the assessment of rheumatoid arthritis activity. Arthritis Rheum. 1995, 38, 38–43. [Google Scholar] [CrossRef]
- Prevoo, M.L.; van’t Hof, M.A.; Kuper, H.H.; van Leeuwen, M.A.; van de Putte, L.B.; van Riel, P.L. Modified disease activity scores that include twenty-eight-joint counts. Development and validation in a prospective longitudinal study of patients with rheumatoid arthritis. Arthritis Rheum. 1995, 38, 44–48. [Google Scholar] [CrossRef] [PubMed]
- Smolen, J.S.; Breedveld, F.C.; Schiff, M.H.; Kalden, J.R.; Emery, P.; Eberl, G.; van Riel, P.L.; Tugwell, P. A simplified disease activity index for rheumatoid arthritis for use in clinical practice. Rheumatology 2003, 42, 244–257. [Google Scholar] [CrossRef] [Green Version]
- Aletaha, D.; Smolen, J.S. The definition and measurement of disease modification in inflammatory rheumatic diseases. Rheum. Dis. Clin. N. Am. 2006, 32, 9–44. [Google Scholar] [CrossRef]
- Aletaha, D.; Smolen, J.S. The Simplified Disease Activity Index (SDAI) and Clinical Disease Activity Index (CDAI) to monitor patients in standard clinical care. Best Pract. Res. Clin. Rheumatol. 2007, 21, 663–675. [Google Scholar] [CrossRef] [PubMed]
- Garrett, S.; Jenkinson, T.; Kennedy, L.G.; Whitelock, H.; Gaisford, P.; Calin, A. A new approach to defining disease status in ankylosing spondylitis: The Bath Ankylosing Spondylitis Disease Activity Index. J. Rheumatol. 1994, 21, 2286–2291. [Google Scholar] [PubMed]
- Lukas, C.; Landewé, R.; Sieper, J.; Dougados, M.; Davis, J.; Braun, J.; van der Linden, S.; van der Heijde, D. Development of an ASAS-endorsed disease activity score (ASDAS) in patients with ankylosing spondylitis. Ann. Rheum. Dis. 2009, 68, 18–24. [Google Scholar] [CrossRef] [PubMed]
- Machado, P.; Landewé, R.; Lie, E.; Kvien, T.K.; Braun, J.; Baker, D.; van der Heijde, D. Ankylosing Spondylitis Disease Activity Score (ASDAS): Defining cut-off values for disease activity states and improvement scores. Ann. Rheum. Dis. 2011, 70, 47–53. [Google Scholar] [CrossRef]
- Eberl, G.; Studnicka-Benke, A.; Hitzelhammer, H.; Gschnait, F.; Smolen, J.S. Development of a disease activity index for the assessment of reactive arthritis (DAREA). Rheumatology 2000, 39, 148–155. [Google Scholar] [CrossRef] [Green Version]
- Schoels, M.; Aletaha, D.; Funovits, J.; Kavanaugh, A.; Baker, D.; Smolen, J.S. Application of the DAREA/DAPSA score for assessment of disease activity in psoriatic arthritis. Ann. Rheum. Dis. 2010, 69, 1441–1447. [Google Scholar] [CrossRef]
- Fries, J.F.; Spitz, P.; Kraines, R.G.; Holman, H.R. Measurement of patient outcome in arthritis. Arthritis Rheum. 1980, 23, 137–145. [Google Scholar] [CrossRef] [Green Version]
- Ranza, R.; Marchesoni, A.; Calori, G.; Bianchi, G.; Braga, M.; Canazza, S.; Canesi, B.; Fumagalli, M.; Mastaglio, C.; Mathieu, A.; et al. The Italian version of the Functional Disability Index of the Health Assessment Questionnaire. A reliable instrument for multicenter studies on rheumatoid arthritis. Clin. Exp. Rheumatol. 1993, 11, 123–128. [Google Scholar]
- Santos, M.J.; Vinagre, F.; Canas da Silva, J.; Gil, V.; Fonseca, J.E. Body composition phenotypes in systemic lupus erythematosus and rheumatoid arthritis: A comparative study of Caucasian female patients. Clin. Exp. Rheumatol. 2011, 29, 470–476. [Google Scholar] [PubMed]
- Kim, J.S.; Wilson, J.M.; Lee, S.R. Dietary implications on mechanisms of sarcopenia: Roles of protein, amino acids and antioxidants. J. Nutr. Biochem. 2010, 21, 1–13. [Google Scholar] [CrossRef]
- Verlaan, S.; Aspray, T.J.; Bauer, J.M.; Cederholm, T.; Hemsworth, J.; Hill, T.R.; McPhee, J.S.; Piasecki, M.; Seal, C.; Sieber, C.C.; et al. Nutritional status, body composition, and quality of life in community-dwelling sarcopenic and non-sarcopenic older adults: A case-control study. Clin. Nutr. 2017, 36, 267–274. [Google Scholar] [CrossRef] [PubMed]
- Baker, J.F.; Long, J.; Ibrahim, S.; Leonard, M.B.; Katz, P. Are men at greater risk of lean mass deficits in rheumatoid arthritis? Arthritis Care Res. 2015, 67, 112–119. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Rheumatoid Arthritis | Psoriatic Arthritis | Ankylosing Spondylitis | p | |
|---|---|---|---|---|
| N. of pts | 76 | 70 | 22 | |
| M/F | 10/66 | 32/38 | 14/8 | <0.001 * |
| Age | 56.5 ± 8.8 | 55.3 ± 9.1 | 51.6 ± 8.8 | 0.08 † |
| Body mass index (BMI) (kg/m2) | 24.9 ± 3.2 | 25.6 ± 3.0 | 24.9 ± 2.5 | 0.37 † |
| Caloric intake (Kcal/Kg/die) | 24.8 ± 6.7 | 23.7 ± 6.8 | 24.8 ± 6.5 | 0.54 † |
| Protein intake (g/Kg/die) | 0.9 ± 0.2 | 0.8 ± 0.2 | 0.9 ± 0.2 | 0.39 † |
| Physical activity level | 1.3 ± 0.1 | 1.4 ± 0.2 | 1.4 ± 0.2 | 0.02 † |
| Disease duration (years) | 10.8 ± 8.2 | 11.1 ± 8.1 | 14.5 ± 8.4 | 0.16 † |
| C-reactive protein (CRP) elevated (%) | 39.7 | 7.4 | 5.2 | <0.001 * |
| Erythrocyte sedimentation rate (ESR) elevated (%) | 51.3 | 26.0 | 18.1 | 0.001 * |
| Biologic therapy (%) | 65.7 | 78.5 | 86.3 | 0.07 * |
| Disability (%) | 52.7 | 54.2 | 54.5 | 0.97 * |
| Variable | N. of Patients with Sarcopenia/Tot. (%) | Univariate | Multivariate | ||
|---|---|---|---|---|---|
| OR (95% CI) | p | OR (95% CI) | p | ||
| Rheumatoid arthritis (RA) | 16/76 (21.0) | ref. | ref. | ||
| Psoriatic arthritis (PsA) | 14/70 (20.0) | 0.9 (0.4–2.0) | 0.87 | 1.1 (0.4–2.7) | 0.79 |
| Ankylosing spondylitis (AS) | 5/22 (22.7) | 1.1 (0.3–3.4) | 0.86 | 1.8 (0.5–6.7) | 0.33 |
| Gender | |||||
| Female | 20/112 (17.8) | ref. | |||
| Male | 15/56 (26.7) | 1.6 (0.7–3.6) | 0.18 | ||
| Age (years) | |||||
| <60 | 13/109 (11.9) | ref. | ref. | ||
| ≥60 | 22/59 (37.2) | 4.3 (2.0–9.6) | <0.001 | 3.3 (1.4–7.7) | 0.005 |
| Calorie intake a | - | 1.0 (0.9–1.0) | 0.19 | ||
| Protein intake b | - | 2.1 (0.5–8.9) | 0.28 | ||
| Physical activity level (PAL) c | - | 0.2 (0.02–3.5) | 0.32 | ||
| Disease duration d | - | 1.0 (0.9–1.0) | 0.37 | ||
| C-reactive protein (CRP) * | |||||
| normal | 26/137 (18.9) | ref. | ref. | ||
| elevated | 9/21 (42.8) | 3.2 (1.2–8.3) | 0.01 | 2.6 (0.8–7.8) | 0.07 |
| Erythrocyte sedimentation rate (ESR) ** | |||||
| normal | 18/105 (17.1) | ref. | |||
| elevated | 16/60 (26.6) | 1.7 (0.8–3.7) | 0.14 | ||
| Biologic therapy | |||||
| no | 6/44 (13.6) | ref. | |||
| yes | 29/124 (23.3) | 1.9 (0.7–5.0) | 0.17 | ||
| Disability | |||||
| no | 7/77 (9.0) | ref. | ref. | ||
| yes | 28/89 (31.4) | 4.5 (1.8–11.2) | 0.001 | 3.0 (1.2–7.9) | 0.01 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Barone, M.; Viggiani, M.T.; Anelli, M.G.; Fanizzi, R.; Lorusso, O.; Lopalco, G.; Cantarini, L.; Di Leo, A.; Lapadula, G.; Iannone, F. Sarcopenia in Patients with Rheumatic Diseases: Prevalence and Associated Risk Factors. J. Clin. Med. 2018, 7, 504. https://doi.org/10.3390/jcm7120504
Barone M, Viggiani MT, Anelli MG, Fanizzi R, Lorusso O, Lopalco G, Cantarini L, Di Leo A, Lapadula G, Iannone F. Sarcopenia in Patients with Rheumatic Diseases: Prevalence and Associated Risk Factors. Journal of Clinical Medicine. 2018; 7(12):504. https://doi.org/10.3390/jcm7120504
Chicago/Turabian StyleBarone, Michele, Maria Teresa Viggiani, Maria Grazia Anelli, Rosalinda Fanizzi, Orsola Lorusso, Giuseppe Lopalco, Luca Cantarini, Alfredo Di Leo, Giovanni Lapadula, and Florenzo Iannone. 2018. "Sarcopenia in Patients with Rheumatic Diseases: Prevalence and Associated Risk Factors" Journal of Clinical Medicine 7, no. 12: 504. https://doi.org/10.3390/jcm7120504