Incidence and Mortality of Renal Cell Carcinoma after Kidney Transplantation: A Meta-Analysis

 , ,
, ,  , ,
, , 
Abstract
:1. Introduction
2. Methods
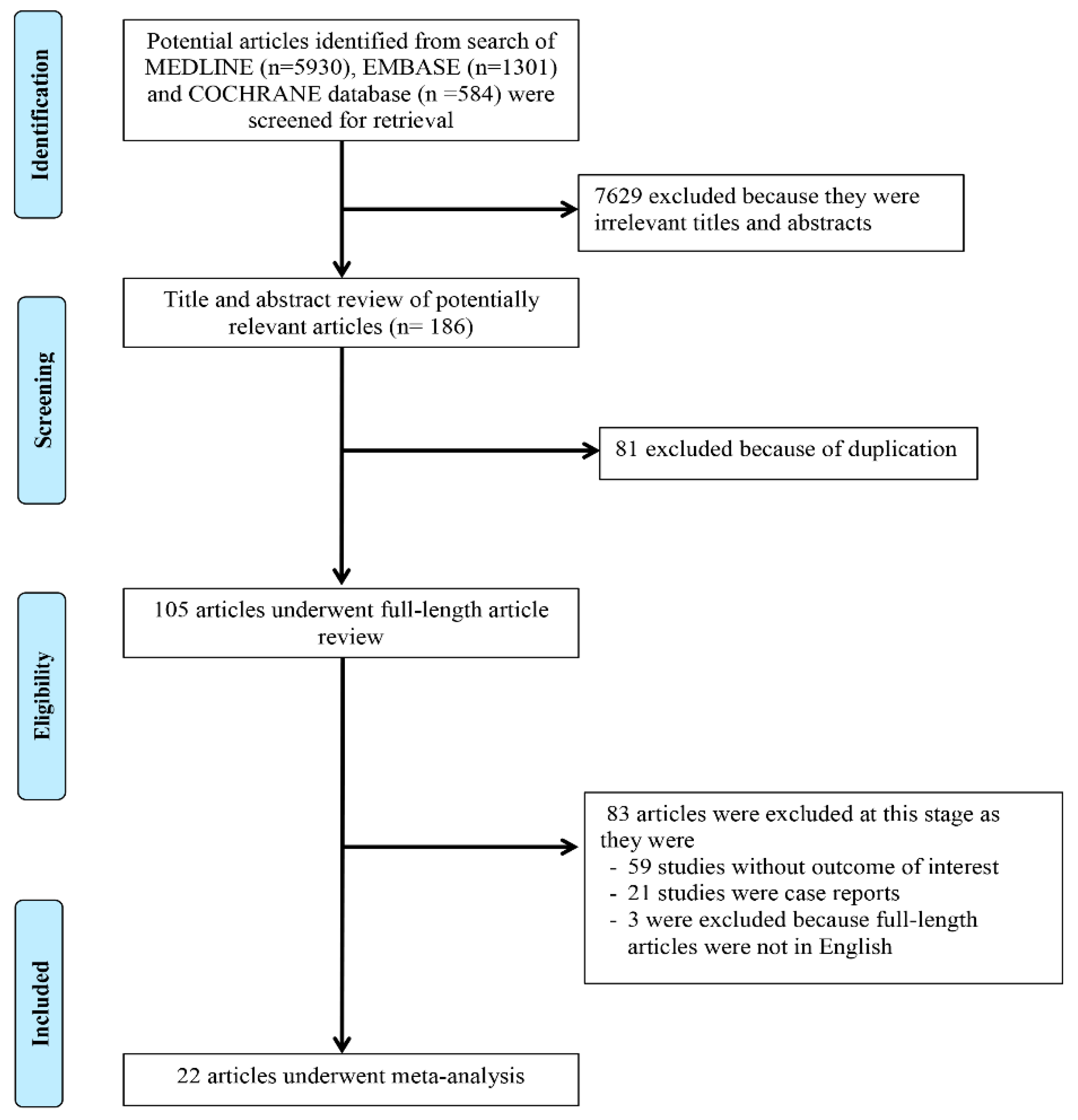
2.1. Search Strategy and Literature Review
2.2. Selection Criteria
2.3. Data Abstraction
2.4. Statistical Analysis
3. Results
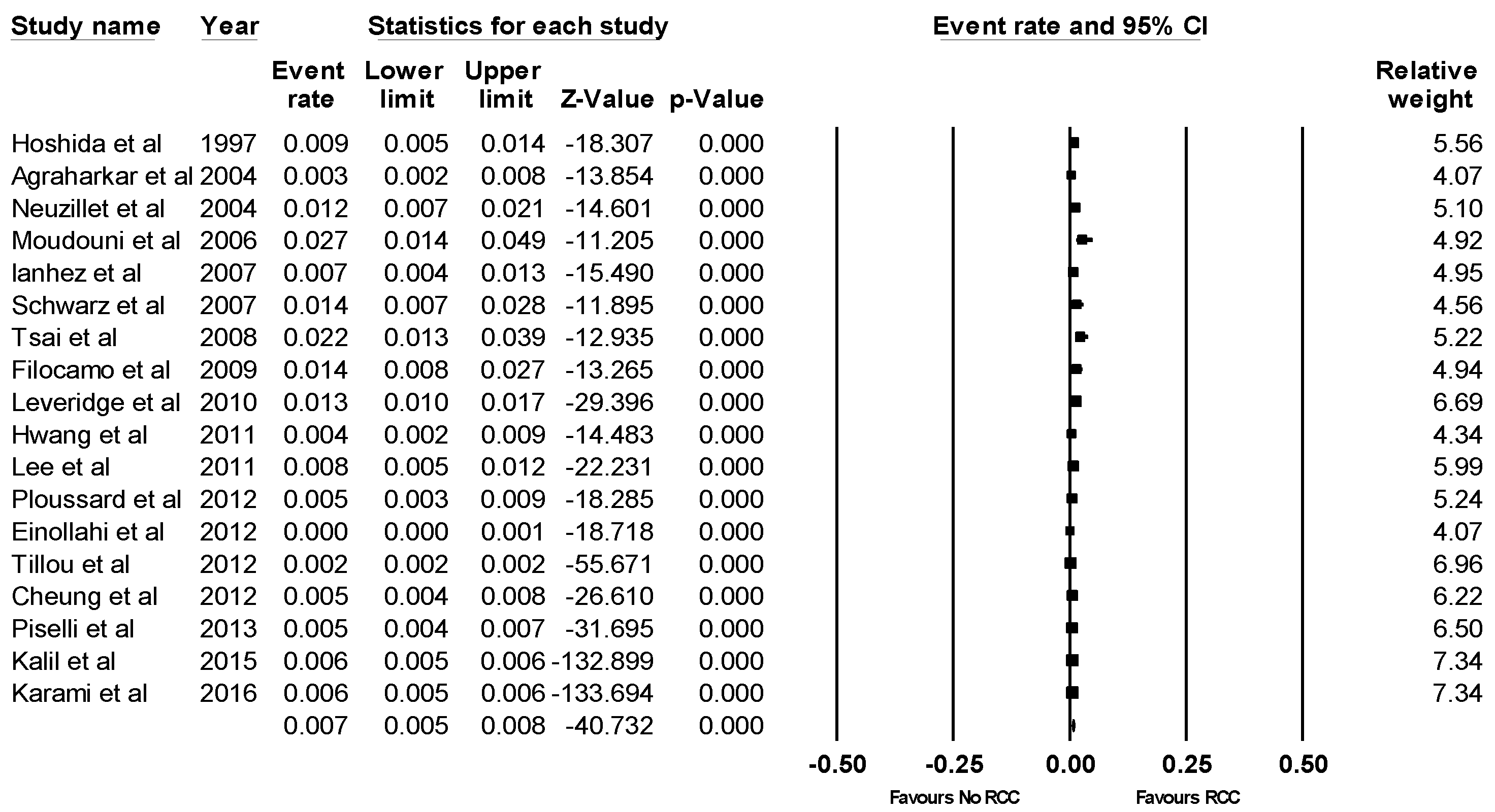
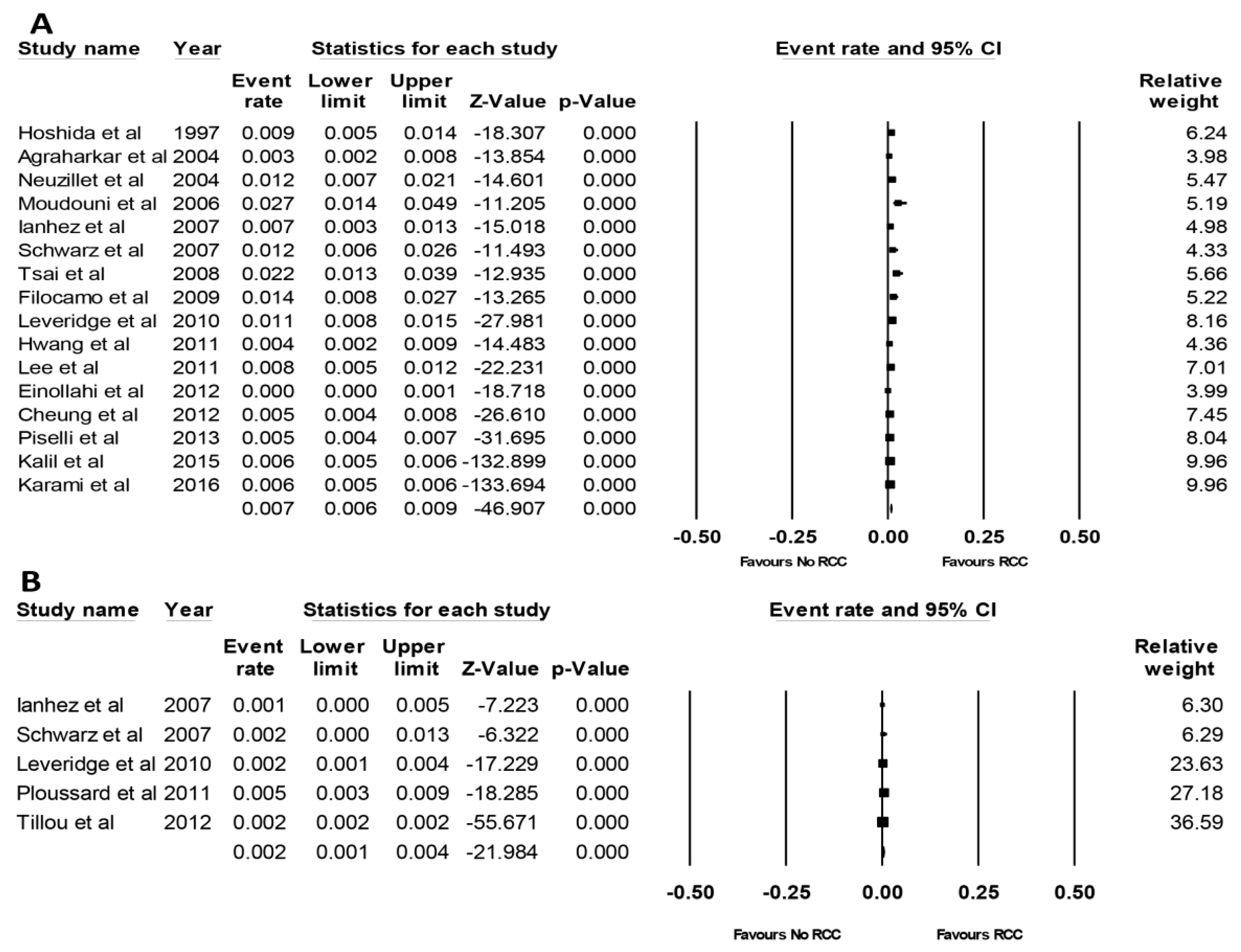
3.1. Incidence of RCC after KTx
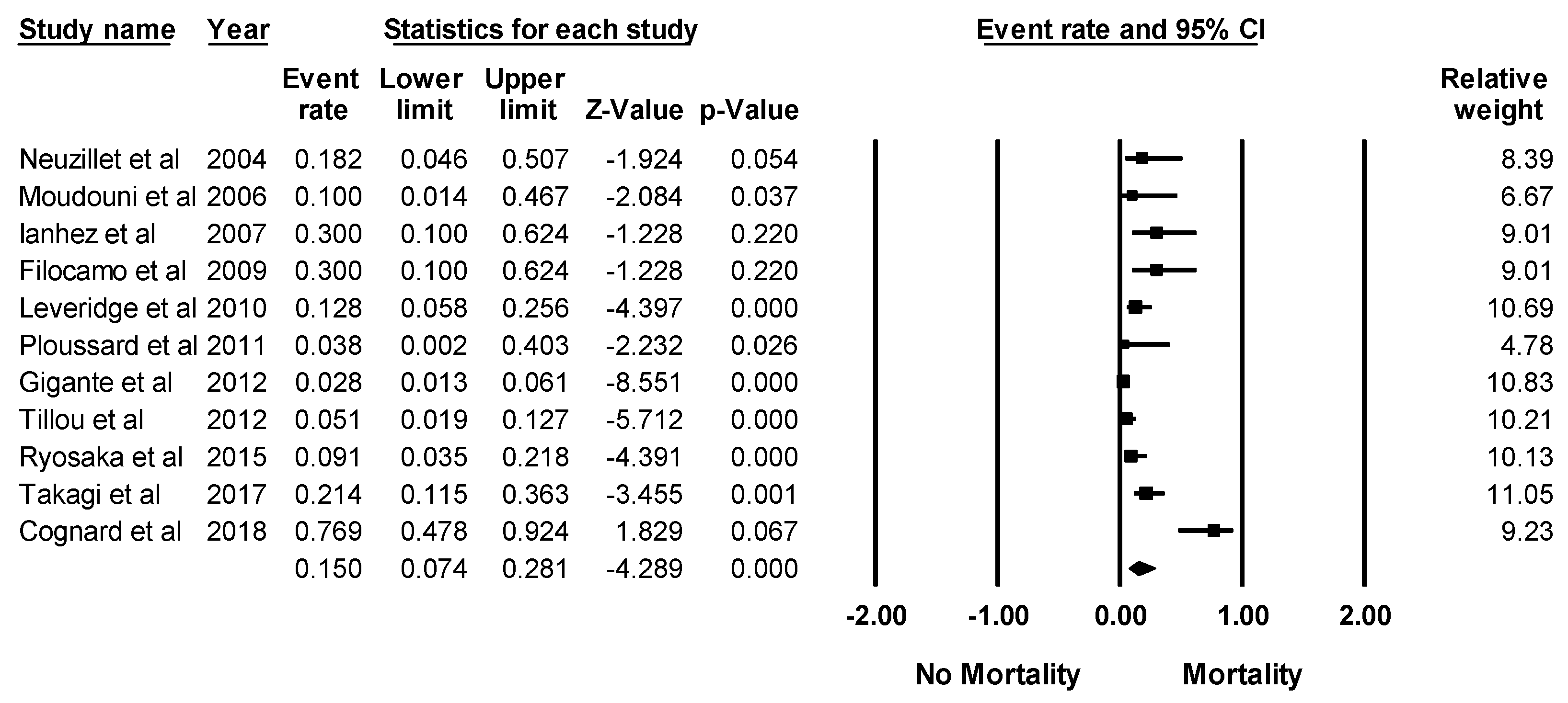
3.2. Mortality Rate in KTx Recipients with RCC
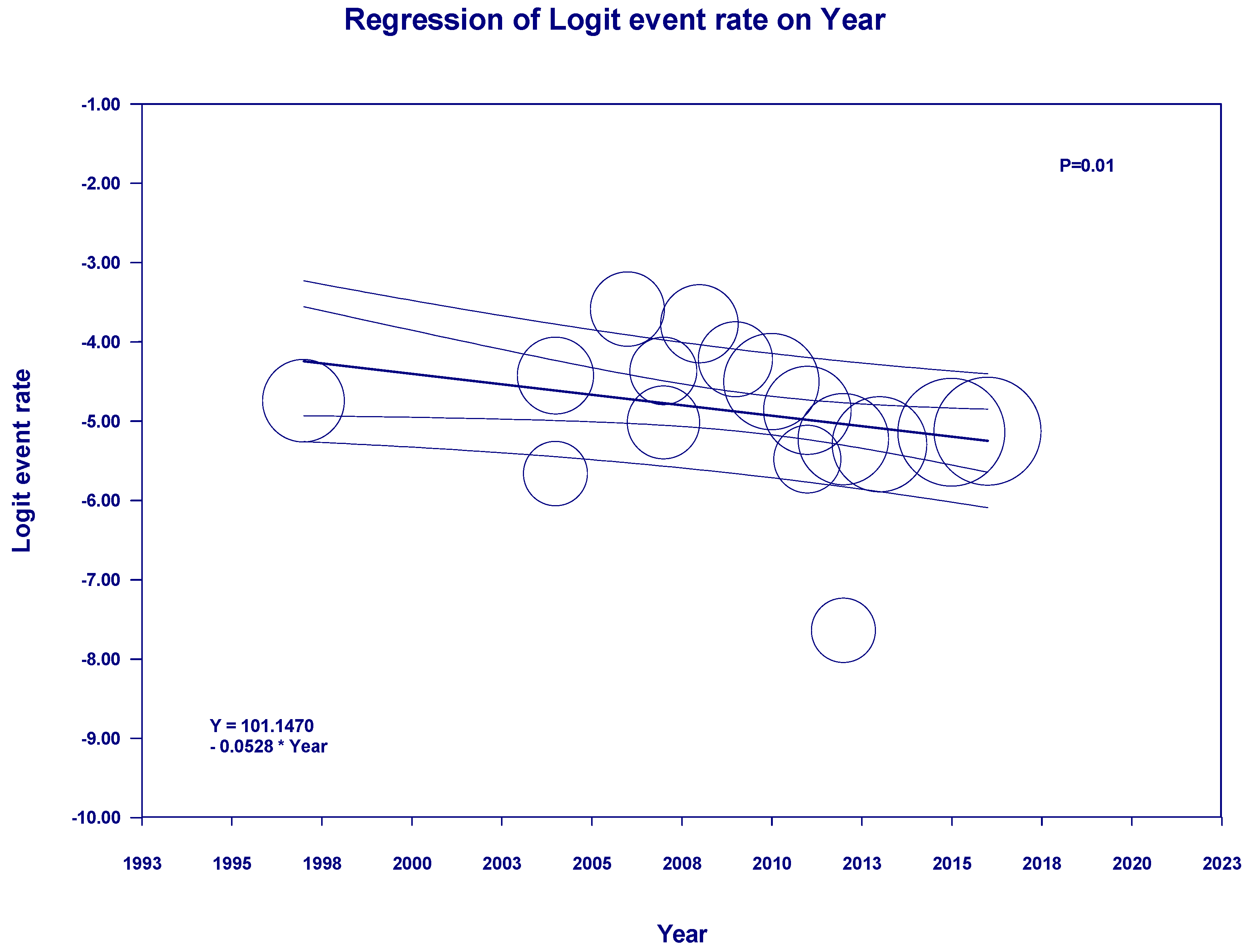
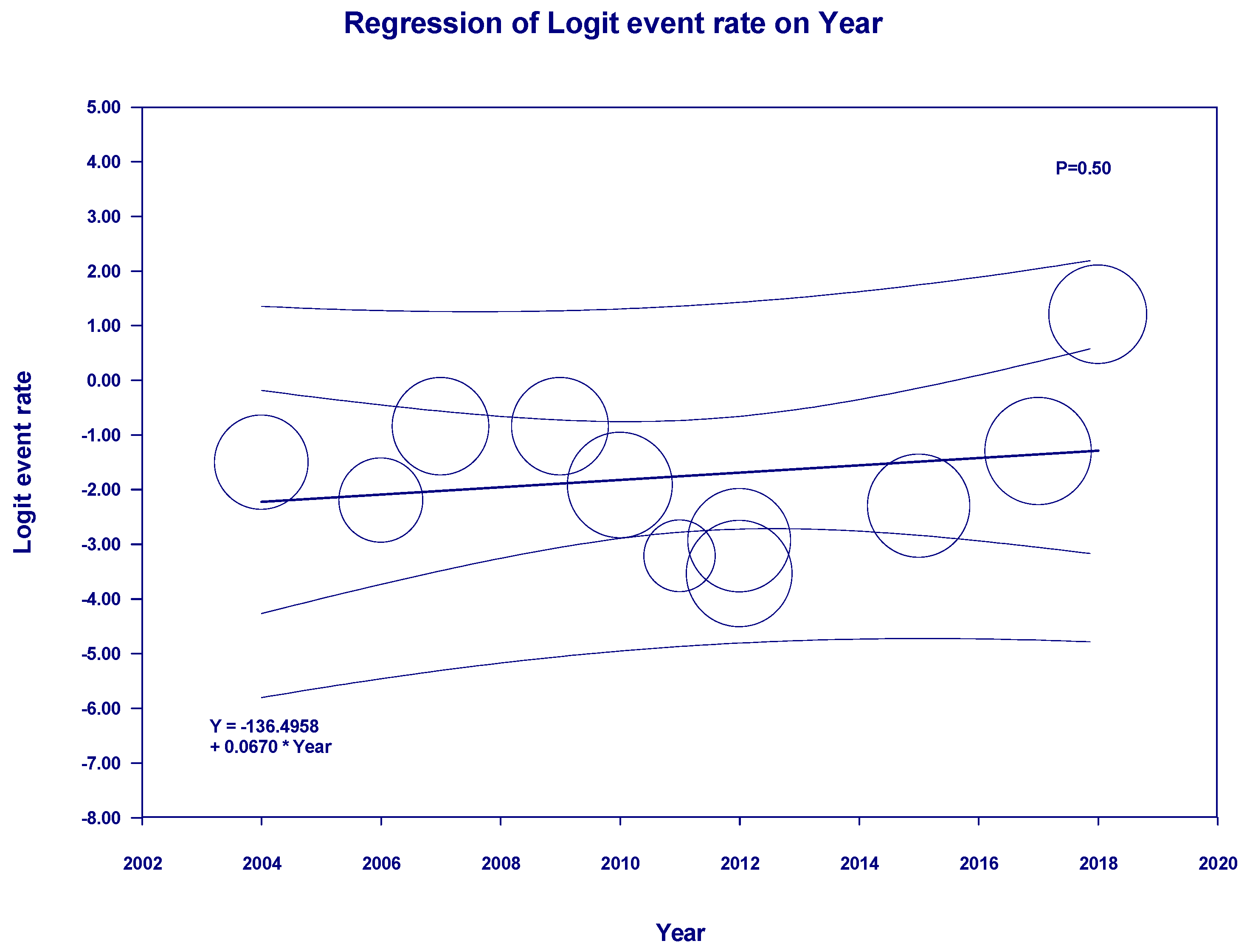
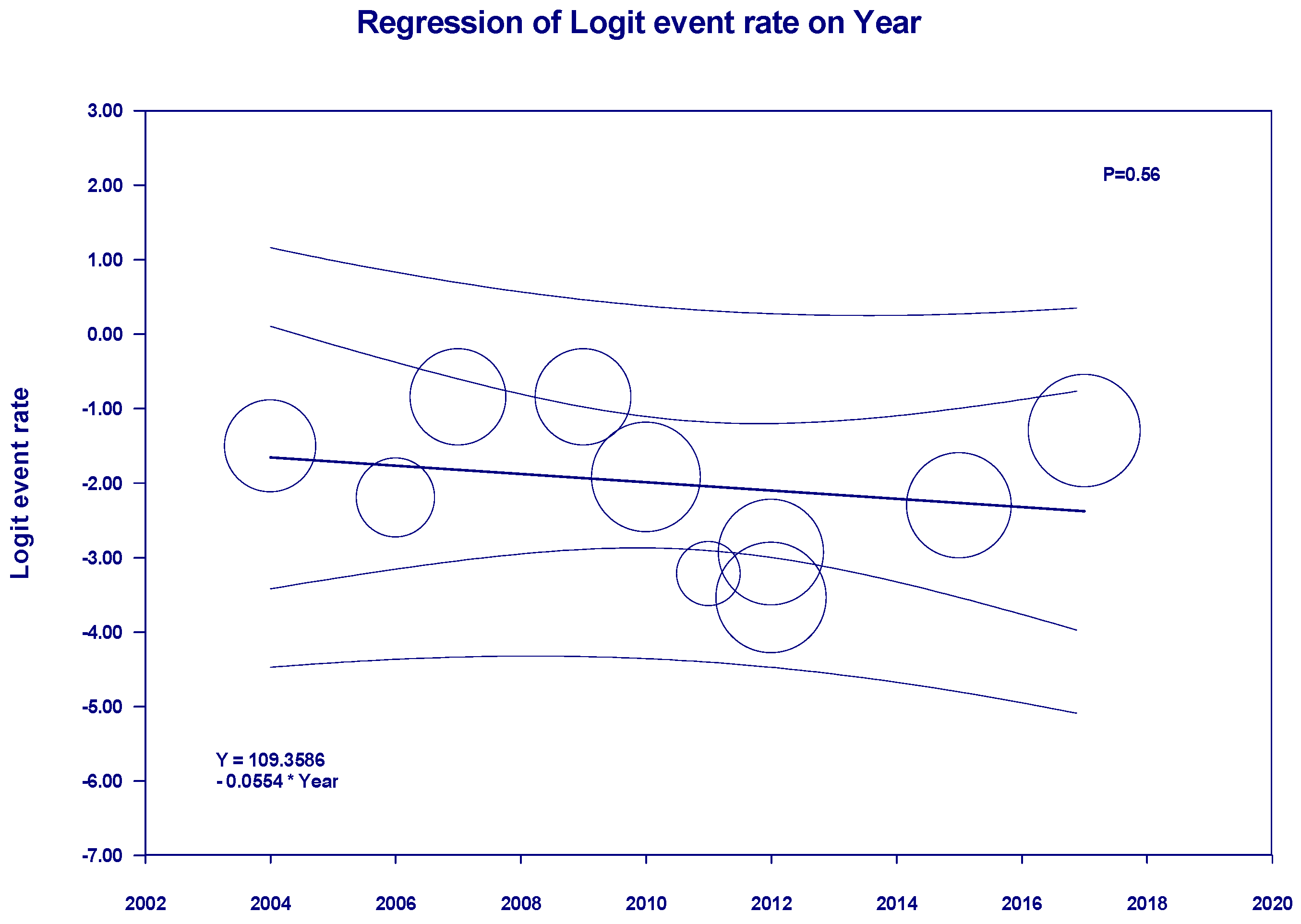
3.3. Evaluation for Publication Bias
4. Discussion
Supplementary Materials
Author Contributions
Conflicts of Interest
References
- Kaballo, M.A.; Canney, M.; O’Kelly, P.; Williams, Y.; O’Seaghdha, C.M.; Conlon, P.J. A comparative analysis of survival of patients on dialysis and after kidney transplantation. Clin. Kidney J. 2018, 11, 389–393. [Google Scholar] [CrossRef] [PubMed]
- Wolfe, R.A.; Ashby, V.B.; Milford, E.L.; Ojo, A.O.; Ettenger, R.E.; Agodoa, L.Y.; Held, P.J.; Port, F.K. Comparison of mortality in all patients on dialysis, patients on dialysis awaiting transplantation, and recipients of a first cadaveric transplant. N. Engl. J. Med. 1999, 341, 1725–1730. [Google Scholar] [CrossRef] [PubMed]
- Hickman, L.A.; Sawinski, D.; Guzzo, T.; Locke, J.E. Urologic malignancies in kidney transplantation. Am. J. Transpl. 2018, 18, 13–22. [Google Scholar] [CrossRef] [PubMed]
- Engels, E.A.; Pfeiffer, R.M.; Fraumeni, J.F.; Jr Kasiske, B.L.; Israni, A.K.; Snyder, J.J.; Wolfe, R.A.; Goodrich, N.P.; Bayakly, A.R.; Clarke, C.A.; et al. Spectrum of cancer risk among US solid organ transplant recipients. JAMA 2011, 306, 1891–1901. [Google Scholar] [CrossRef] [PubMed]
- Bennett, W.M.; Simonich, E.L.; Garre, A.M.; McEvoy, K.M.; Farinola, M.A.; Batiuk, T.D. Renal Cell Carcinoma in Renal Transplantation: The Case for Surveillance. Transpl. Proc. 2017, 49, 1779–1782. [Google Scholar] [CrossRef]
- Briggs, J.D. Causes of death after renal transplantation. Nephrol Dial. Transpl. 2001, 16, 1545–1549. [Google Scholar] [CrossRef]
- Dy, G.W.; Gore, J.L.; Forouzanfar, M.H.; Naghavi, M.; Fitzmaurice, C. Global Burden of Urologic Cancers, 1990. Eur. Urol. 2017, 71, 437–446. [Google Scholar] [CrossRef] [PubMed]
- Kompotiatis, P.; Thongprayoon, C.; Manohar, S.; Cheungpasitporn, W.; Gonzalez Suarez, M.L.; Craici, I.M.; Mao, M.A.; Herrmann, S.M. Association between urologic malignancies and end-stage renal disease: A meta-analysis. Nephrology 2019, 24, 65–73. [Google Scholar] [CrossRef] [PubMed]
- Kasiske, B.L.; Cangro, C.B.; Hariharan, S.; Hricik, D.E.; Kerman, R.H.; Roth, D.; Rush, D.N.; Vazquez, M.A.; Weir, M.R. The evaluation of renal transplantation candidates: Clinical practice guidelines. Am. J. Transplant. 2001, 1 (Suppl. 2), 3–95. [Google Scholar]
- Holley, J.L. Screening, diagnosis, and treatment of cancer in long-term dialysis patients. Clin. J. Am. Soc. Nephrol. 2007, 2, 604–610. [Google Scholar] [CrossRef] [PubMed]
- Hoshida, Y.; Tsukuma, H.; Yasunaga, Y.; Xu, N.; Fujita, M.Q.; Satoh, T.; Ichikawa, Y.; Kurihara, K.; Imanishi, M.; Matsuno, T.; et al. Cancer risk after renal transplantation in Japan. Int. J. Cancer 1997, 71, 517–520. [Google Scholar] [CrossRef]
- Agraharkar, M.L.; Cinclair, R.D.; Kuo, Y.F.; Daller, J.A.; Shahinian, V.B. Risk of malignancy with long-term immunosuppression in renal transplant recipients. Kidney Int. 2004, 66, 383–389. [Google Scholar] [CrossRef] [PubMed]
- Neuzillet, Y.; Lay, F.; Luccioni, A.; Daniel, L.; Berland, Y.; Coulange, C.; Lechevallier, E. De novo renal cell carcinoma of native kidney in renal transplant recipients. Cancer 2005, 103, 251–257. [Google Scholar] [CrossRef] [PubMed]
- Moudouni, S.M.; Lakmichi, A.; Tligui, M.; Rafii, A.; Tchala, K.; Haab, F.; Gattegno, B.; Thibault, P.; Doublet, J.D. Renal cell carcinoma of native kidney in renal transplant recipients. BJU Int. 2006, 98, 298–302. [Google Scholar] [CrossRef]
- Tsai, M.K.; Yang, C.Y.; Lee, C.Y.; Yeh, C.C.; Hu, R.H.; Lee, P.H. De novo malignancy is associated with renal transplant tourism. Kidney Int. 2011, 79, 908–913. [Google Scholar] [CrossRef]
- Filocamo, M.T.; Zanazzi, M.; Li Marzi, V.; Guidoni, L.; Villari, D.; Dattolo, E.; Nicita, G. Renal cell carcinoma of native kidney after renal transplantation: Clinical relevance of early detection. Transpl. Proc. 2009, 41, 4197–4201. [Google Scholar] [CrossRef] [PubMed]
- Leveridge, M.; Musquera, M.; Evans, A.; Cardella, C.; Pei, Y.; Jewett, M.; Robinette, M.; Finelli, A. Renal cell carcinoma in the native and allograft kidneys of renal transplant recipients. J. Urol. 2011, 186, 219–223. [Google Scholar] [CrossRef]
- Hwang, J.K.; Moon, I.S.; Kim, J.I. Malignancies after kidney transplantation: A 40-year single-center experience in Korea. Transpl. Int. 2011, 24, 716–721. [Google Scholar] [CrossRef] [PubMed]
- Tillou, X.; Doerfler, A.; Collon, S.; Kleinclauss, F.; Patard, J.J.; Badet, L.; Barrou, B.; Audet, M.; Bensadoun, H.; Berthoux, E.; et al. De novo kidney graft tumors: Results from a multicentric retrospective national study. Am. J. Transpl. 2012, 12, 3308–3315. [Google Scholar] [CrossRef]
- Ploussard, G.; Chambade, D.; Meria, P.; Gaudez, F.; Tariel, E.; Verine, J.; De Bazelaire, C.; Peraldi, M.N.; Glotz, D.; Desgrandchamps, F.; et al. Biopsy-confirmed de novo renal cell carcinoma (RCC) in renal grafts: A single-centre management experience in a 2396 recipient cohort. BJU Int. 2012, 109, 195–199. [Google Scholar] [CrossRef]
- Scandling, J.D. Acquired cystic kidney disease and renal cell cancer after transplantation: Time to rethink screening? Clin. J. Am. Soc. Nephrol. 2007, 2, 621–622. [Google Scholar] [CrossRef]
- Kasiske, B.L.; Vazquez, M.A.; Harmon, W.E.; Brown, R.S.; Danovitch, G.M.; Gaston, R.S.; Roth, D.; Scandling, J.D.; Singer, G.G. Recommendations for the outpatient surveillance of renal transplant recipients. American Society of Transplantation. J. Am. Soc. Nephrol 2000, 11 (Suppl. 15), S1–S86. [Google Scholar] [PubMed]
- Cognard, N.; Anglicheau, D.; Gatault, P.; Girerd, S.; Essig, M.; Hurault de Ligny, B.; Le Meur, Y.; Le Roy, F.; Garrouste, C.; Thierry, A.; et al. Recurrence of Renal Cell Cancer After Renal Transplantation in a Multicenter French Cohort. Transplantation 2018, 102, 860–867. [Google Scholar] [CrossRef] [PubMed]
- EBPG Expert Group on Renal Transplantation. European best practice guidelines for renal transplantation. Section IV: Long-term management of the transplant recipient. IV.6. Cancer risk after renal transplantation. Solid organ cancers: Prevention and treatment. Nephrol Dial. Transplant. 2002, 17 (Suppl. 4), 34–36. [Google Scholar]
- Wiesel, M.; Carl, S.; Drehmer, I.; Hofmann, W.J.; Zeier, M.; Staehler, G. [The clinical significance of renal cell carcinoma in dialysis dependent patients in comparison with kidney transplant recipients]. Urol. A 1997, 36, 126–129. [Google Scholar] [CrossRef]
- Gulanikar, A.C.; Daily, P.P.; Kilambi, N.K.; Hamrick-Turner, J.E.; Butkus, D.E. Prospective pretransplant ultrasound screening in 206 patients for acquired renal cysts and renal cell carcinoma. Transplantation 1998, 66, 1669–1672. [Google Scholar] [CrossRef]
- Brunner, F.P.; Landais, P.; Selwood, N.H. Malignancies after renal transplantation: The EDTA-ERA registry experience. European Dialysis and Transplantation Association-European Renal Association. Nephrol. Dial. Transplant. 1995, 10 (Suppl. 1), 74–80. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.H.; Choi, K.H.; Yang, S.C.; Han, W.K. Renal cell carcinoma in kidney transplant recipients and dialysis patients. Korean J. Urol. 2012, 53, 229–233. [Google Scholar] [CrossRef] [PubMed]
- Einollahi, B.; Rostami, Z.; Nourbala, M.H.; Lessan-Pezeshki, M.; Simforoosh, N.; Nemati, E.; Pourfarziani, V.; Beiraghdar, F.; Nafar, M.; Pour-Reza-Gholi, F.; et al. Incidence of malignancy after living kidney transplantation: A multicenter study from iran. J. Cancer 2012, 3, 246–256. [Google Scholar] [CrossRef] [PubMed]
- Gigante, M.; Neuzillet, Y.; Patard, J.J.; Tillou, X.; Thuret, R.; Branchereau, J.; Timsit, M.O.; Terrier, N.; Boutin, J.M.; Sallusto, F.; et al. Renal cell carcinoma (RCC) arising in native kidneys of dialyzed and transplant patients: Are they different entities? BJU Int. 2012, 110, E570–E573. [Google Scholar] [CrossRef] [PubMed]
- Cheung, C.Y.; Lam, M.F.; Chu, K.H.; Chow, K.M.; Tsang, K.Y.; Yuen, S.K.; Wong, P.N.; Chan, S.K.; Leung, K.T.; Chan, C.K.; et al. Malignancies after kidney transplantation: Hong Kong renal registry. Am. J. Transpl. 2012, 12, 3039–3046. [Google Scholar] [CrossRef]
- Piselli, P.; Busnach, G.; Citterio, F.; Richiardi, L.; Cimaglia, C.; Angeletti, C.; Doringhet, P.V.; Pozzetto, U.; Perrino, M.L.; Serraino, D. [Kidney transplant and cancer risk: An epidemiological study in Northern and Central Italy]. Epidemiol. Prev. 2008, 32, 205–211. [Google Scholar]
- Ryosaka, M.; Ishida, H.; Takagi, T.; Shimizu, T.; Tanabe, K.; Kondo, T. Solid-type RCC originating from native kidneys in renal transplant recipients should be monitored cautiously. Transpl. Int. 2015, 28, 813–819. [Google Scholar] [CrossRef]
- Kalil, R.S.; Lynch, C.F.; Engels, E.A. Risk of cancer in retransplants compared to primary kidney transplants in the United States. Clin. Transpl. 2015, 29, 944–950. [Google Scholar] [CrossRef]
- Karami, S.; Yanik, E.L.; Moore, L.E.; Pfeiffer, R.M.; Copeland, G.; Gonsalves, L.; Hernandez, B.Y.; Lynch, C.F.; Pawlish, K.; Engels, E.A. Risk of Renal Cell Carcinoma Among Kidney Transplant Recipients in the United States. Am. J. Transpl. 2016, 16, 3479–3489. [Google Scholar] [CrossRef]
- Takagi, T.; Kondo, T.; Okumi, M.; Ishida, H.; Tanabe, K. Differences in Clinical and Pathological Features of Renal Cell Carcinoma Between Japanese Patients After Kidney Transplantation and Those on Hemodialysis. Ther. Apher. Dial. 2017, 21, 133–138. [Google Scholar] [CrossRef]
- Olsson, C.A. Renal cell carcinoma (RCC) arising in native kidneys of dialyzed and transplant patients: Are they different entities? BJU Int. 2012, 110, E574. [Google Scholar] [CrossRef]
- Schwarz, A.; Vatandaslar, S.; Merkel, S.; Haller, H. Renal cell carcinoma in transplant recipients with acquired cystic kidney disease. Clin. J. Am. Soc. Nephrol. 2007, 2, 750–756. [Google Scholar] [CrossRef] [PubMed]
- Ianhez, L.E.; Lucon, M.; Nahas, W.C.; Sabbaga, E.; Saldanha, L.B.; Lucon, A.M.; Srougi, M. Renal cell carcinoma in renal transplant patients. Urology 2007, 69, 462–464. [Google Scholar] [CrossRef] [PubMed]
- Levine, E. Renal cell carcinoma in uremic acquired renal cystic disease: Incidence, detection, and management. Urol Radiol 1992, 13, 203–210. [Google Scholar] [CrossRef] [PubMed]
- Doublet, J.D.; Peraldi, M.N.; Gattegno, B.; Thibault, P.; Sraer, J.D. Renal cell carcinoma of native kidneys: Prospective study of 129 renal transplant patients. J. Urol. 1997, 158, 42–44. [Google Scholar] [CrossRef]
- Nie, H.; Wang, W.; Zhao, Y.; Zhang, X.; Xiao, Y.; Zeng, Q.; Zhang, C.; Zhang, L. New-Onset Diabetes After Renal Transplantation (NODAT): Is It a Risk Factor for Renal Cell Carcinoma or Renal Failure? Ann. Transpl. 2019, 24, 62–69. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef]
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials. Controll. Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef]
- Easterbrook, P.J.; Berlin, J.A.; Gopalan, R.; Matthews, D.R. Publication bias in clinical research. Lancet 1991, 337, 867–872. [Google Scholar] [CrossRef]
- Penn, I. Primary kidney tumors before and after renal transplantation. Transplantation 1995, 59, 480–485. [Google Scholar] [CrossRef]
- Kasiske, B.L.; Snyder, J.J.; Gilbertson, D.T.; Wang, C. Cancer after kidney transplantation in the United States. Am. J. Transplant. 2004, 4, 905–913. [Google Scholar] [CrossRef]
- Pedotti, P.; Cardillo, M.; Rossini, G.; Arcuri, V.; Boschiero, L.; Caldara, R.; Cannella, G.; Dissegna, D.; Gotti, E.; Marchini, F.; et al. Incidence of cancer after kidney transplant: Results from the North Italy transplant program. Transplantation 2003, 76, 1448–1451. [Google Scholar] [CrossRef]
- Bellini, M.I.; Gopal, J.P.; Hill, P.; Nicol, D.; Gibbons, N. Urothelial Carcinoma arising from the transplanted kidney: A single centre experience and literature review. Clin. Transplant. 2019. [Google Scholar] [CrossRef]
- Benoni, H.; Eloranta, S.; Ekbom, A.; Wilczek, H.; Smedby, K.E. Survival among solid organ transplant recipients diagnosed with cancer compared to nontransplanted cancer patients-A nationwide study. Int. J. Cancer 2019. [Google Scholar] [CrossRef] [PubMed]
- Vajdic, C.M.; McDonald, S.P.; McCredie, M.R.; van Leeuwen, M.T.; Stewart, J.H.; Law, M.; Chapman, J.R.; Webster, A.C.; Kaldor, J.M.; Grulich, A.E. Cancer incidence before and after kidney transplantation. JAMA 2006, 296, 2823–2831. [Google Scholar] [CrossRef] [PubMed]
- Birkeland, S.A.; Lokkegaard, H.; Storm, H.H. Cancer risk in patients on dialysis and after renal transplantation. Lancet 2000, 355, 1886–1887. [Google Scholar] [CrossRef]
- Knoll, G.; Cockfield, S.; Blydt-Hansen, T.; Baran, D.; Kiberd, B.; Landsberg, D.; Rush, D.; Cole, E. Canadian Society of Transplantation: Consensus guidelines on eligibility for kidney transplantation. CMAJ 2005, 173, S1–S25. [Google Scholar] [CrossRef] [PubMed]
- Knoll, G.; Cockfield, S.; Blydt-Hansen, T.; Baran, D.; Kiberd, B.; Landsberg, D.; Rush, D.; Cole, E. Canadian Society of Transplantation consensus guidelines on eligibility for kidney transplantation. CMAJ 2005, 173, 1181–1184. [Google Scholar] [CrossRef] [PubMed]
- Butler, A.M.; Olshan, A.F.; Kshirsagar, A.V.; Edwards, J.K.; Nielsen, M.E.; Wheeler, S.B.; Brookhart, M.A. Cancer incidence among US Medicare ESRD patients receiving hemodialysis, 1996–2009. Am. J. Kidney Dis. 2015, 65, 763–772. [Google Scholar] [CrossRef]
- Zorbas, K.A.; Karhadkar, S.S.; Lau, K.N.; Di Carlo, A. Renal Cell Carcinoma in Kidney Transplant Candidates. Transpl. Proc. 2017, 49, 1312–1317. [Google Scholar] [CrossRef]
- Tillou, X.; Guleryuz, K.; Doerfler, A.; Bensadoun, H.; Chambade, D.; Codas, R.; Devonec, M.; Dugardin, F.; Erauso, A.; Hubert, J.; et al. Nephron sparing surgery for De Novo kidney graft tumor: Results from a multicenter national study. Am. J. Transpl. 2014, 14, 2120–2125. [Google Scholar] [CrossRef]
- Krisl, J.C.; Doan, V.P. Chemotherapy and Transplantation: The Role of Immunosuppression in Malignancy and a Review of Antineoplastic Agents in Solid Organ Transplant Recipients. Am. J. Transpl. 2017, 17, 1974–1991. [Google Scholar] [CrossRef] [PubMed]
- Purdue, M.P.; Moore, L.E.; Merino, M.J.; Boffetta, P.; Colt, J.S.; Schwartz, K.L.; Bencko, V.; Davis, F.G.; Graubard, B.I.; Janout, V.; et al. An investigation of risk factors for renal cell carcinoma by histologic subtype in two case-control studies. Int. J. Cancer 2013, 132, 2640–2647. [Google Scholar] [CrossRef]
- Ishikawa, I. Uremic acquired renal cystic disease. Natural history and complications. Nephron 1991, 58, 257–267. [Google Scholar] [CrossRef] [PubMed]
- Ishikawa, I. Uremic acquired cystic disease of kidney. Urology 1985, 26, 101–108. [Google Scholar] [CrossRef]
- Levine, E.; Slusher, S.L.; Grantham, J.J.; Wetzel, L.H. Natural history of acquired renal cystic disease in dialysis patients: A prospective longitudinal CT study. Am. J. Roentgenol. 1991, 156, 501–506. [Google Scholar] [CrossRef] [PubMed]
- Matson, M.A.; Cohen, E.P. Acquired cystic kidney disease: Occurrence, prevalence, and renal cancers. Medicine 1990, 69, 217–226. [Google Scholar] [CrossRef] [PubMed]
- Goh, A.; Vathsala, A. Native renal cysts and dialysis duration are risk factors for renal cell carcinoma in renal transplant recipients. Am. J. Transplant. Off. J. Am. Soc. Transplant. Am. Soc. Transpl. Surg. 2011, 11, 86–92. [Google Scholar] [CrossRef] [PubMed]
- Moris, D.; Kakavia, K.; Argyrou, C.; Garmpis, N.; Bokos, J.; Vernadakis, S.; Diles, K.; Sotirchos, G.; Boletis, J.; Zavos, G. De Novo Renal Cell Carcinoma of Native Kidneys in Renal Transplant Recipients: A Single-center Experience. Anticancer Res. 2017, 37, 773–779. [Google Scholar] [CrossRef]
- Chow, W.H.; Devesa, S.S. Contemporary epidemiology of renal cell cancer. Cancer J. 2008, 14, 288–301. [Google Scholar] [CrossRef]
- Dhakal, P.; Giri, S.; Siwakoti, K.; Rayamajhi, S.; Bhatt, V.R. Renal Cancer in Recipients of Kidney Transplant. Rare Tumors 2017, 9, 6550. [Google Scholar] [CrossRef] [PubMed]
- Kidney Disease: Improving Global Outcomes (KDIGO) Transplant Work Group. KDIGO clinical practice guideline for the care of kidney transplant recipients. Am. J. Transplant. 2009, 9 (Suppl. 3), S1–S155. [Google Scholar] [CrossRef]
- Bia, M.; Adey, D.B.; Bloom, R.D.; Chan, L.; Kulkarni, S.; Tomlanovich, S. KDOQI US commentary on the 2009 KDIGO clinical practice guideline for the care of kidney transplant recipients. Am. J. Kidney Dis. 2010, 56, 189–218. [Google Scholar] [CrossRef]
- European Renal Best Practice Transplantation Guideline Development Group. ERBP Guideline on the Management and Evaluation of the Kidney Donor and Recipient. Nephrol. Dial. Transplant. 2013, 28 (Suppl. 2), ii1–ii71. [Google Scholar]
- Kalble, T.; Lucan, M.; Nicita, G.; Sells, R.; Burgos Revilla, F.J.; Wiesel, M. EAU guidelines on renal transplantation. Eur. Urol. 2005, 47, 156–166. [Google Scholar] [CrossRef]
- Fuiano, G.; Zoccali, C.; Bertoni, E.; Bartolomeo, F.; Cambareri, F.; Salvadori, M.; Altieri, P.; Ponticelli, C.; Sandrini, S.; Schena, F.P.; et al. [Guidelines for ambulatory monitoring of kidney transplant patients. Adaptation of the Guidelines of the American Society of Transplantation (J Am Soc Nephrol 2000; 11 (S1): 86)]. Giornale italiano di nefrologia Organo ufficiale della Societa italiana di nefrologia 2004, 21 (Suppl. 28), S11–S50. [Google Scholar]
- Marinella, M.A. Hematologic abnormalities following renal transplantation. Int. Urol. Nephrol. 2010, 42, 151–164. [Google Scholar] [CrossRef] [PubMed]
- Park, P.; Kim, W.Y.; Lee, J.B.; Choi, S.B.; Kim, W.B.; Choi, S.Y. Incidental renal cell carcinoma originating from a native kidney after en-bloc resection for adrenal carcinoma in a kidney transplant recipient. Transpl. Proc. 2014, 46, 637–639. [Google Scholar] [CrossRef] [PubMed]
- Brennan, J.F.; Stilmant, M.M.; Babayan, R.K.; Siroky, M.B. Acquired renal cystic disease: Implications for the urologist. Br. J. Urol. 1991, 67, 342–348. [Google Scholar] [CrossRef]
- Klatte, T.; Seitz, C.; Waldert, M.; de Martino, M.; Kikic, Z.; Bohmig, G.A.; Haitel, A.; Schmidbauer, J.; Marberger, M.; Remzi, M. Features and outcomes of renal cell carcinoma of native kidneys in renal transplant recipients. BJU Int. 2010, 105, 1260–1265. [Google Scholar] [CrossRef] [PubMed]
- Muruve, N.A.; Shoskes, D.A. Genitourinary malignancies in solid organ transplant recipients. Transplantation 2005, 80, 709–716. [Google Scholar] [CrossRef]
- Ljungberg, B.; Cowan, N.C.; Hanbury, D.C.; Hora, M.; Kuczyk, M.A.; Merseburger, A.S.; Patard, J.J.; Mulders, P.F.; Sinescu, I.C. EAU guidelines on renal cell carcinoma: The 2010 update. Eur. Urol. 2010, 58, 398–406. [Google Scholar] [CrossRef] [PubMed]
- Israel, G.M.; Bosniak, M.A. An update of the Bosniak renal cyst classification system. Urology 2005, 66, 484–488. [Google Scholar] [CrossRef]
- Kauffman, H.M.; Cherikh, W.S.; McBride, M.A.; Cheng, Y.; Hanto, D.W. Post-transplant de novo malignancies in renal transplant recipients: The past and present. Transpl. Int. Off. J. Eur. Soc. Organ. Transplant. 2006, 19, 607–620. [Google Scholar] [CrossRef] [PubMed]
- Taylor, A.L.; Marcus, R.; Bradley, J.A. Post-transplant lymphoproliferative disorders (PTLD) after solid organ transplantation. Crit. Rev. Oncol. Hematol. 2005, 56, 155–167. [Google Scholar] [CrossRef]
- Barrett, W.L.; First, M.R.; Aron, B.S.; Penn, I. Clinical course of malignancies in renal transplant recipients. Cancer 1993, 72, 2186–2189. [Google Scholar] [CrossRef]
- Kliem, V.; Kolditz, M.; Behrend, M.; Ehlerding, G.; Pichlmayr, R.; Koch, K.M.; Brunkhorst, R. Risk of renal cell carcinoma after kidney transplantation. Clin. Transplant. 1997, 11, 255–258. [Google Scholar]
- Sandock, D.S.; Seftel, A.D.; Resnick, M.I. A new protocol for the followup of renal cell carcinoma based on pathological stage. J. Urol. 1995, 154, 28–31. [Google Scholar] [CrossRef]
- Kapoor, A. Malignancy in kidney transplant recipients. Drugs 2008, 68 (Suppl. 1), 11–19. [Google Scholar] [CrossRef]
- Opelz, G.; Unterrainer, C.; Susal, C.; Dohler, B. Immunosuppression with mammalian target of rapamycin inhibitor and incidence of post-transplant cancer in kidney transplant recipients. Nephrol. Dial. Transpl. 2016, 31, 1360–1367. [Google Scholar] [CrossRef] [PubMed]
- Kao, C.C.; Liu, J.S.; Lin, M.H.; Hsu, C.Y.; Chang, F.C.; Lin, Y.C.; Chen, H.H.; Chen, T.W.; Hsu, C.C.; Wu, M.S. Impact of mTOR Inhibitors on Cancer Development in Kidney Transplantation Recipients: A Population-Based Study. Transpl. Proc. 2016, 48, 900–904. [Google Scholar] [CrossRef]
- Karpe, K.M.; Talaulikar, G.S.; Walters, G.D. Calcineurin inhibitor withdrawal or tapering for kidney transplant recipients. Cochrane Database Syst. Rev. 2017, 7, CD006750. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Year | Type of Study | Number of Patients | Incidence of RCC | Follow-Up Time after Transplant | Time from Transplant to Cancer Diagnosis | Mortality of RCC | Quality Assessment |
|---|---|---|---|---|---|---|---|---|
| Hoshida et al. [11] | 1997 | Cohort | 1744 | 15/1744 | N/A | N/A | N/A | S4 C0 O3 |
| Agraharkar et al. [12] | 2004 | Cohort | 1739 | 6/1739 | Mean 6.1 years | N/A | N/A | S4 C1 O3 |
| Neuzillet et al. [13] | 2004 | Cohort | 933 | 11/933 | N/A | Mean 70.9 ± 49.4 (range 8–156) months | 2/11 (1 died due to cancer) | S4 C0 O2 |
| Moudouni et al. [14] | 2006 | Cohort | 373 | 10/373 | N/A | Mean 12.8 years Median 127 in patients treated with cyclosporine A and 114 months in patients not treated with cyclosporine A | 1/10 (1 died due to cancer) | S4 C0 O3 |
| Ianhez et al. [39] | 2007 | Cohort | 1375 | 10/1375 9 in native kidney 1 in allograft kidney | N/A | N/A | 3/10 (2 died due to myocardial infarction and one due to penile cancer) | S4 C0 O2 |
| Schwarz et al. [38] | 2007 | Cohort | 561 | 8/561 7 de novo in native kidney 1 de novo in allograft kidney | N/A | 105.2 ± 62.39 months | N/A | S4C2O3 |
| Tsai et al. [15] | 2008 | Cohort | 3259 | Touring group 15/215 kidney cancer Domestic group 4/321 kidney cancer | Touring group Mean 76.2 ± 48.1 months Domestic group Mean 81.5 ± 53.4 months | N/A | N/A | S4 C1 O3 |
| Filocamo et al. [16] | 2009 | cohort | 694 | Native de novo 10/694 | N/A | 61.8 months (12–156 months) | 3/10 (3 died due to cancer other than RCC) | S4 C1 O3 |
| Leveridge et al. [17] | 2010 | cohort | 3568 | 39/3568 native kidney 8/3568 allograft kidney | 6.6 years | Native 10.6 years allograft 12.1 years | 5 native died (not RCC cause), 1 allograft died due to cardiac cause | S4 C0 O3 |
| Hwang et al. [18] | 2011 | Cohort | 1695 | 7/1695 | 9.1 ± 6.9 years | Mean 11.8 ± 6.0 years | N/A | S4 C0 O3 |
| Lee et al. [28] | 2011 | Cohort | 2757 | 21/2757 | N/A | Mean 119 (range 0–264) months | N/A | S4 C1 O2 |
| Ploussard et al. [20] | 2012 | Cohort | 2396 | Allograft kidney 12/2396 | N/A | Mean 13 (range 4–20) years | 0/12 | S4 C0 O3 |
| Einollahi et al. [29] | 2012 | Cohort | 12,525 | 6/12,525 | N/A | Median 16 months | N/A | S4 C0 O3 |
| Gigante et al. [30] | 2012 | Cohort | 213 | N/A | N/A | Mean 91 ± 82 months | 6/213 due to RCC | S4 C0 O2 |
| Tillou et al. [19] | 2012 | Cohort | 41,806 | Allograft kidney 79/41,806 | N/A | Mean 131.7 (0.9–244) months | 4/79 | S4 C0 O3 |
| Cheung et al. [31] | 2012 | Cohort | 4895 | 26/4895 | N/A | Median 4 (0.2–16.5) years | N/A | S4 C1 O3 |
| Piselli et al. [32] | 2013 | Cohort | 7217 | 31/7217 | Median 5.2 years (2.9–7.8) | N/A | N/A | S4 C1 O3 |
| Ryosaka et al. [33] | 2015 | Cohort | 202 | N/A | N/A | N/A | Solid-type renal cell carcinoma 2/17 Cystic-type renal cell carcinoma 2/27 | S4 C0 O3 |
| Kalil et al. [34] | 2015 | Cohort | 115,845 | Primary kidney transplant 514/109,224 Retransplant 43/6621 | Mean 1st–4.6 years 2nd–3.7 years 3rd–2.9 years 4th–3.4 years | N/A | N/A | S4 C2 O3 |
| Karami et al. [35] | 2016 | Cohort | 116,208 | 683/116,208 | Median 4.2 years (range 0.003–23.1) | N/A | N/A | S4 C0 O2 |
| Takagi et al. [36] | 2017 | Cohort | 42 | N/A | N/A | Mean 86 ± 69 months | 9/42 (5 died due to cancer) | S4 C0 O3 |
| Cognard et al. [23] | 2018 | Cohort | 143 with history of pre-transplant kidney cancer | 13/143 | Mean 5.6 ± 3.2 years | Mean 3 ± 2.3 years (range 45 days–7 years) | 10/13 (9 died due to cancer) | S4 C0 O3 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chewcharat, A.; Thongprayoon, C.; Bathini, T.; Aeddula, N.R.; Boonpheng, B.; Kaewput, W.; Watthanasuntorn, K.; Lertjitbanjong, P.; Sharma, K.; Torres-Ortiz, A.; et al. Incidence and Mortality of Renal Cell Carcinoma after Kidney Transplantation: A Meta-Analysis. J. Clin. Med. 2019, 8, 530. https://doi.org/10.3390/jcm8040530
Chewcharat A, Thongprayoon C, Bathini T, Aeddula NR, Boonpheng B, Kaewput W, Watthanasuntorn K, Lertjitbanjong P, Sharma K, Torres-Ortiz A, et al. Incidence and Mortality of Renal Cell Carcinoma after Kidney Transplantation: A Meta-Analysis. Journal of Clinical Medicine. 2019; 8(4):530. https://doi.org/10.3390/jcm8040530
Chicago/Turabian StyleChewcharat, Api, Charat Thongprayoon, Tarun Bathini, Narothama Reddy Aeddula, Boonphiphop Boonpheng, Wisit Kaewput, Kanramon Watthanasuntorn, Ploypin Lertjitbanjong, Konika Sharma, Aldo Torres-Ortiz, and et al. 2019. "Incidence and Mortality of Renal Cell Carcinoma after Kidney Transplantation: A Meta-Analysis" Journal of Clinical Medicine 8, no. 4: 530. https://doi.org/10.3390/jcm8040530